
Notes
Article history
The research reported in this issue of the journal was commissioned by the HTA programme as project number 01/70/05. The contractual start date was in September 2003. The draft report began editorial review in May 2008 and was accepted for publication in November 2008. As the funder, by devising a commissioning brief, the HTA programme specified the research question and study design. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HTA editors and publisher have tried to ensure the accuracy of the authors’ report and would like to thank the referees for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Tony Kendrick has received fees for presenting at educational meetings and/or research funding from Lilly, Lundbeck, Servier and Wyeth pharmaceuticals, and has also received HTA funding for research into psychological treatments. Christopher Dowrick has received research funding from Lilly, Lundbeck, Servier and Wyeth pharmaceuticals, and MRC and EU research funding for research into psychological treatments, and has written about the limited value of antidepressants. André Tylee has received fees for presenting at educational meetings and/or research funding from Lilly, Lundbeck, Servier, Wyeth and GlaxoSmithKline pharmaceuticals. Richard Morriss has received fees for presenting at educational meetings from Lilly and AstraZeneca pharmaceuticals, and MRC funding for research into psychological treatments. Robert Peveler has received fees for presenting at educational meetings and/or consultancy from Lilly, GlaxoSmithKline, Pfizer, Lundbeck, Wyeth, AstraZeneca, Bristol Myers Squibb, Servier and Organon pharmaceuticals. Richard Byng has received fees for speaking at an educational meeting from Lilly pharmaceuticals and has written about the limited value of antidepressants. Paul McCrone has received fees for speaking at educational meetings and/or consultancy from Lilly, Lundbeck, Organon, Servier and Janssen-Cilag pharmaceuticals. Tirril Harris and George Brown have published articles on the importance of social factors in determining the course and outcome of depression. The remaining authors have declared no competing interests.
Permissions
Copyright statement
© 2009 Queen’s Printer and Controller of HMSO. This monograph may be freely reproduced for the purposes of private research and study and may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NETSCC, Health Technology Assessment, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2009 Queen’s Printer and Controller of HMSO
Chapter 1 Introduction
Depression is a very common and costly condition, both in terms of the personal suffering of those it affects, and in terms of the costs to the nation through absence from work and treatment costs. Most of the treatment of depression takes place in primary care, which in the UK means general practice, rather than in the secondary care setting of specialised psychiatric practice. The most common general practice treatment for depression is the prescription of antidepressant drugs, and there is a clear need for good research evidence on the cost-effectiveness of these drug treatments to inform decisions about treating patients.
The increasing use of antidepressants in general practice
Antidepressant prescribing rates in the UK have been rising year on year since the early 1990s. This is costly and may not be appropriate. Expenditure on antidepressants in England rose from £147 million to £279 million between 1995 and 1998, with the bulk of the increase being due to increased prescribing in general practice. 1 Prescribing of antidepressants has continued to increase annually since the turn of the century. The National Health Service (NHS) Prescription Pricing Authority reported a 36% increase between 2000 and 2005, to 7.3 million items, costing £91 million, in the quarter to June 2005 (www.nhsbsa.nhs.uk/PrescriptionServices/Documents/PrescriptionServices/imPACTjan2006.pdf). Prescription numbers have continued to rise since then, to more than 9.6 million items in the last quarter of 2007 (Alison Bowes, Prescription Analysis Service, NHSBSA Prescription Pricing Division, personal communication).
The Defeat Depression Campaign, mounted by the Royal Colleges of Psychiatrists and General Practitioners in the 1990s, was a promotional campaign designed specifically to increase both doctor and patient awareness of depressive disorders. 2 The message has been caricatured as ‘see more, treat more’3 and was probably part of the reason for the increase in antidepressant prescribing in general practice starting in the early 1990s. Another likely reason was the introduction of the selective serotonin reuptake inhibitors (SSRIs), starting with fluoxetine in 1990, as they were perceived to be better tolerated by patients than the older tricyclic antidepressants. 4 However, much of this increased prescribing probably falls outside current guideline recommendations and may not be appropriate. This is because antidepressants are frequently being prescribed for relatively mild depression, for which they are not recommended in the guidelines. Guidelines recommend drug treatment only for ‘major depression’ of a minimum level of severity.
Depression and its classification
Depressive symptoms range along a continuous spectrum from everyday sadness to suicidal ideas, and any cut-off between ‘normal’ and ‘depressed’ patients is, to an extent, arbitrary, but categorical classifications are necessary in order to make decisions about intervening in clinical practice. Depression is classified in two ways: categorically, in descriptive diagnostic classification systems; and dimensionally, in terms of scores on continuous self-rating questionnaire measures.
Categorical classification
Major depression
According to antidepressant treatment guidelines, the category of ‘major depression’ predicts the need for active treatment, irrespective of environmental factors except for bereavement. 5 The World Health Organization’s International Classification of Diseases, 10th edition (ICD-10) criteria for major depressive disorder state that at least five of nine symptoms (depressed mood, loss of interest or pleasure in activities, weight change, change in sleep pattern, agitation or retardation, fatigue, feelings of worthlessness or guilt, impaired concentration and suicidal thoughts) must be present most of the day, nearly daily, for a minimum of 2 weeks, accompanied by significant impairment of functioning. 6 The American Psychiatric Association’s Diagnostic and Statistical Manual, 4th edition (DSM-IV) classification of major depression also requires five out of nine symptoms, one of which must be depressed mood or loss of interest and pleasure in usual activities. 7
The World Health Organization’s multicountry survey of 2000–1 found that major depression affected around 5% of women and 3% of men per year. 8 Major depression was identified as the fourth leading cause of global health burden among all diseases, responsible for 4.4% of total disability-adjusted life-years lost on average,8 and is predicted to be second after ischaemic heart disease by 2020. 9
‘Mild depression’, ‘minor depression’ and ‘dysthymia’
In addition to the 3–5% of people with major depression, three to four times as many have depressive symptoms below the cut-off for the diagnosis. In UK general practice, roughly 5% of attenders are found to be suffering from major depression, 5% from mild depression and around 15% from some depressive symptoms. 10 Mild (or ‘minor’) depression is diagnosed if low mood or loss of pleasure is accompanied by up to three other symptoms of depression. 11 Dysthymia is mild depression which has persisted for 2 years or more. Despite its name, mild depression and dysthymia can be associated with significant distress and impairment of social functioning,12,13 and overall depression of all levels of severity is the second- (for women) or third- (for men) biggest cause of long-term sickness certification in the UK. 14 It is therefore not surprising that general practitioners (GPs) frequently decide to prescribe antidepressants for patients with mild depression, but the routine treatment of mild depression is not recommended in the guidelines.
The threshold for drug treatment
In common with other depression guidelines, the UK’s National Institute for Health and Clinical Excellence (NICE) clinical guidelines for the management of depression recommend antidepressant medication as first-line treatment for depression in primary care only for major depression, with at least five of the symptoms as listed above, and of at least moderate severity in terms of impairment of functioning. 5,11 The NICE guidelines recommend that antidepressants should not normally be prescribed for mild depression, which is defined in terms of a maximum of four symptoms, although it should not be ignored, but should be monitored for a period of 2 weeks or more (‘watchful waiting’), in case the patient goes on to develop more severe symptoms. 11 During this period, a variety of self-help measures are recommended, including advice on sleep hygiene and anxiety management, regular exercise, and the provision of books (‘bibliotherapy’) or interactive computer programs based on the principles of cognitive–behavioural therapy (computerised CBT),15 which encourage patients to identify and tackle their depressive thoughts, and to become more active.
Despite the guideline recommendations, however, antidepressants are frequently prescribed for depressive symptoms below the threshold for major depression, perhaps as a result of the perceived pressure to treat more patients, in the context of a severe lack of availability of alternative treatments, particularly psychological therapies. 16–18 Another reason is that the recommendations on the threshold for treatment are not supported by a great deal of good research evidence. Previous research on antidepressant treatment has mostly been carried out in secondary, specialist care settings, with patients with relatively severe depression, and there has been comparatively little research in primary care on patients with mild depression to guide GPs on the threshold at which antidepressants should be offered.
Previous research on the treatment threshold
Several placebo-controlled trials have been conducted to determine the efficacy of antidepressants in treating depression in primary care. These trials often classify the patients they include in terms of the DSM or ICD diagnostic systems, but they tend to measure outcome using continuous measures of depressive symptoms, rather than the more descriptive DSM and ICD classifications. The outcome measure most commonly used is the Hamilton Depression Rating Scale (HDRS). 19
Major depression
A general practice-based placebo-controlled trial of the tricyclic antidepressant amitriptyline found that patients with ‘probable major depressive disorder’ benefited from drug treatment, but those with ‘minor depression’ did no better on the antidepressant than on placebo. 20 These findings resulted from a post hoc subgroup analysis dividing the patients into those who did or did not fulfil research diagnostic criteria for a diagnosis of probable major depression, and the study was not set up a priori specifically to assess the relationship between severity and response to treatment. In this study, patients with ‘probable major depression’ had HDRS scores ranging from 16 to 19 and those in the ‘minor depression’ category had HDRS scores of 12–15. Despite the fact that this analysis was post hoc, the threshold of ‘major depression’ formed the basis for early guidelines on drug treatment. 10
Supportive evidence for the usefulness of the category of major depression as a treatment threshold also came from two other studies which were not randomised controlled trials of drug treatment. One was a US trial of collaborative management to achieve greater adherence to guidelines21 and the other was a UK trial of nurse intervention to improve compliance with antidepressants. 22 Both studies found that outcome was improved only among patients with major depression, although, again, these were post hoc subgroup analyses, and these studies were not set up to assess the relationship between severity and response to treatment. A subsequent systematic review and meta-analysis of 15 trials, mostly of tricyclic antidepressants, confirmed modest benefit from drug treatment over placebo for major depression in primary care. 23
Mild depression
A placebo-controlled trial of the SSRI paroxetine, versus problem solving, versus watchful waiting, for mild depression in a primary care population, was undertaken in the US. 24 Patients were selected on the basis of diagnostic criteria for minor depression or dysthymia, and an HDRS score of at least 10. The results were mixed: among patients aged 18–59 years with dysthymia, paroxetine improved remission (to a score of 6 or less on the HDRS) at 11 weeks follow-up compared with placebo plus non-specific clinical management, while for minor depression the two treatments were equally effective. 25 Among patients aged 60 and over, paroxetine was beneficial in dysthymia and among more severely impaired patients with minor depression. 26 This study suggested that ‘watchful waiting’, i.e. supportive care but without the prescription of antidepressants, might be an appropriate treatment option for minor depression, at least in adults and elderly patients with mild impairment.
This study also supported the use of antidepressants for dysthymia, suggesting that a longer duration of depression may be an important predictor of likely benefit from treatment. A previous systematic review and meta-analysis of secondary care studies had suggested that antidepressant drug treatment was effective in the management of dysthymia, although most of the research studies analysed were of relatively poor quality. 27
A randomised placebo-controlled trial of fluoxetine carried out among 162 patients with ‘minor depressive disorder’ found that fluoxetine was better in terms of clinical effectiveness when measured using the HDRS. 28 However, the mean difference between intervention and control groups at follow-up was only 1 point on the HDRS scale, and it is debatable whether such a small difference is clinically significant. 29 In addition, one-third of the patients had a past history of major depressive disorder, and their HDRS scores at baseline ranged from 6 to 21 on the 17-item scale, which means they included people with major depression as well as those with mild depression. 29,30
Most recently, a study of the newer dual-action serotonin and noradrenaline reuptake inhibitor duloxetine found that it was more effective than placebo in 159 patients with ‘milder major depressive disorder’ (scores on the HDRS between 15 and 18). 31 The mean difference was 2.9 points on the HDRS, which is more significant clinically, but it should be noted that this study was a post hoc subgroup analysis of pooled data from two trials.
Predictors of response to treatment
Adverse life events and difficulties
The placebo-controlled trial of amitriptyline in general practice referred to above found no difference between those categorised as having endogenous and those having non-endogenous (or ‘reactive’) depression. The authors recommended drug treatment for major depression, regardless of demographic characteristics, a past history of depression or the presence or absence of endogenous features. 20 These findings led to the guideline recommendations to prescribe drug treatment for depression if symptoms are severe enough and functioning is impaired, even if there seems to be an understandable cause for depression such as adverse events or continuing difficulties in the patient’s life (apart from bereavement). 20,20,32,33
However, the importance of social factors in depression is undeniable, and there is substantial evidence to suggest that both onset and recovery are related to life events and difficulties. Depression is strongly associated with lower socioeconomic status,34,35 poverty,36 unemployment,35,37 separation or divorce34,38 and poor housing. 39 Predisposing factors among women include demanding child care,40 lone motherhood and poor social support. 41
Adverse events have been shown to lead to depression by research using the Life Events and Difficulties Schedule (LEDS). 41,42 A lower severity of premorbid life difficulties has also been shown to be associated with a reduced time to remission, at least among patients with high self-esteem and better coping strategies. 43 Recovery from depression is related to positive social support and life events which can be perceived as ‘fresh starts’, which may or may not be related to the original adverse events and difficulties associated with onset. 44 A reduction in marked social difficulties has been found to predict recovery from depression among patients in primary care,45 whereas recognition and drug treatment by the general practitioner has not. 46,47
Currently, there is a limited evidence base to guide treatment choices for individual patients in primary care. Preliminary analysis of data from the Outcomes of Depression International Network (ODIN) study of problem-solving therapy versus group psychoeducation48 showed that recent adverse life events had an adverse effect on outcome for women, but not for men. The outcome was also worse with increasing duration of depression prior to baseline assessment, but no different between episodes which were reported as first or recurrent. Contact with the GP and use of antidepressants were not related to outcome. These results may not apply, however, to patients randomised to drug treatment.
Research into psychosocial predictors of response carried out in secondary care suggested that greater emotional support and a relative lack of experience of adversity, particularly in domains of the patient’s life invested with greater commitment, were more strongly related to recovery than was drug treatment. 49 As findings in secondary care may not generalise to primary care, however, it remains uncertain whether such social factors would predict response to drug treatment in a primary care setting.
Comorbid physical disorder
Another possible predictor of response to antidepressant treatment is comorbid physical disorder. This may be especially important in primary care, where depressed patients often present with somatic symptoms. 50,51 In general, somatic presentations of depressive disorder are associated with a lower severity of depressive symptoms but similar impairments in function and a similar prognosis. 52 However, depression is less likely to be diagnosed in the presence of physical symptoms or physical illness. 50 Little is known about whether comorbid physical illness affects the response to antidepressant treatment because patients with comorbid illness are often excluded from trials. 53 Patients with alcohol misuse are also often excluded too, yet primary care practitioners frequently have to decide whether or not to treat depression in someone with significant alcohol use.
Research in secondary care settings suggests that antidepressants can work for patients with coexisting medical illnesses. 54 Evidence about the effectiveness of antidepressants for patients presenting with pain or other somatic symptoms, which is very common in primary care, is mixed. 55 A distinction needs to be drawn between somatic symptoms, which may be caused by physical illness and just happen to coincide with depression on the one hand, and somatic presentation of underlying mental disorder (‘somatisation’) on the other. 56 Illness beliefs are important and are related to outcome. Reattribution for somatised mental disorder was found to lead to recovery in patients with minor depression and to improved function in those with partly psychologising attributions, but not in patients with totally somatising attributions where improvements were confined only to major depression. 57
The need for a new study
A new study was needed for several reasons. First, we considered that the findings from the US that SSRIs may benefit some patients with ‘minor’ depression or dysthymia25 might not generalise to primary care in the UK, as the type of supportive care usually provided in the UK may differ in quality or quantity from the ‘watchful waiting’ provided in the US study.
Second, we considered that, even if SSRI treatment is efficacious compared with placebo in mild depression, its effectiveness and cost-effectiveness in practice need to be established. All the studies referred to above were placebo-controlled studies aimed at determining the efficacy of antidepressants. To establish effectiveness and cost-effectiveness, a pragmatic open-label trial is necessary, comparing active drug treatment plus supportive care with supportive care without prescription of a drug, as opposed to a placebo-controlled trial, as placebos are not used in practice and cannot be costed as part of usual health care. Cost-effectiveness also needed to be established within the UK health-care system, which is quite different from the US system. For example, GPs in the UK act as gatekeepers to secondary care, whereas in the US patients commonly self-refer to specialists.
Third, another issue that needed to be addressed was whether predictors of response to antidepressant treatment could be identified, to help GPs decide which patients should be offered such treatment. Important predictors to include were sociodemographic factors, the presence of recent adverse life events and ongoing life difficulties, the duration of depression, previous depression and previous experience of using antidepressants, the presence of somatic symptoms, symptom attribution to a physical cause rather than a psychological cause and level of alcohol use.
Our research questions were, therefore:
-
Is treatment with an SSRI plus supportive care more effective and cost-effective than supportive care alone?
-
If it is more effective, does this apply across the whole range of severity of symptoms of mild to moderate depression?
-
What patient factors might predict the need for antidepressant treatment and a beneficial response?
To answer these questions, we designed a randomised controlled trial of SSRI treatment plus supportive care versus supportive care alone, measuring a number of possible predictors of response.
Objectives and hypothesis
The research objectives were:
-
To determine the clinical effectiveness and cost-effectiveness of SSRI treatment plus supportive care versus supportive care alone, for mild to moderate depression in patients with somatic symptoms in primary care. Our first hypothesis was that SSRI treatment plus supportive care would be more effective and cost-effective than supportive care alone.
-
To determine the impact of the initial severity of depression on the effectiveness and relative costs of these two approaches. Our second hypothesis was that SSRI treatment plus supportive care would be relatively more effective and cost-effective than supportive care alone among patients scoring 16–19 on the HDRS, compared with those scoring 12–15.
-
To carry out exploratory analyses of the impact of the following factors on the effectiveness of these two approaches:
-
demographic and social variables including age, gender, and employment status
-
life events and difficulties
-
the patient’s self-reported duration of depressive symptoms
-
the patient’s previous experience of antidepressant use
-
the number of physical symptoms
-
the patient’s self-rating of the cause of his or her illness (physical versus psychological)
-
alcohol consumption.
-
Chapter 2 Methods
Trial design
The study design was a randomised controlled trial comparing treatment by means of an SSRI plus GP supportive care with GP supportive care alone, over 26 weeks of follow-up. The aim was to establish the clinical effectiveness and cost-effectiveness of SSRI antidepressants prescribed by the GP over and above supportive care (defined below) in normal clinical practice conditions.
Setting
Patients were recruited in general practice surgeries around three academic centres: the University of Southampton; the University of Liverpool; and the Institute of Psychiatry, King’s College London.
Ethical approval and Primary Care Trust Research Management and Governance approval
Ethical approval was awarded by the West Midlands Multi-Centre Research Committee (MREC): reference number 02/7/091. Research Management and Governance approval was obtained from 57 primary care trusts (PCTs) during the course of the study: 21 around Southampton, 27 around Liverpool and nine around London.
Practice and general practitioner recruitment
Initially, practices in each centre known to the research teams from previous research studies were approached and asked to take part. However, only a small proportion of practices approached were willing to participate. It soon became apparent, therefore, that referrals from these practices would be insufficient to meet the required target, so all practices in neighbouring PCTs were systematically approached with a letter which had been previously approved by the MREC (see Appendix 1). This was then followed up with a telephone call to the practice manager to ascertain any interest in participating among the GPs within each practice. Where the response was positive, one or more members of the research team (including one of the medical team members where possible) arranged to visit the practice to explain the study in detail and to answer questions about it. Interested GPs were informed verbally and in writing of the patient inclusion and exclusion criteria (see Appendix 2), how to refer patients into the study, the consent procedure involving both the GPs and the researchers, the randomisation procedure and the details of interventions to be offered in each arm of the trial.
No financial incentive was offered to the GPs for taking part but they were advised that they would be reimbursed for their involvement at the rate of £49 per patient referred to the study. This money was provided through the ad hoc NHS Research and Development (R&D) funding arrangement for service support costs, and was calculated to cover the cost of an extra hour of GP time for referring and monitoring study patients, based on the prevailing cost of employing locum tenens doctors at the rate of £45 per hour, plus 20 minutes of clerical time based on the prevailing average rate of £12 per hour.
Over the 41 months during which patients were recruited, various strategies were adopted to keep the study in the GPs’ minds when seeing potential participants in their surgeries. They included sending emails about the study approximately once a month; visiting them face to face whenever possible and appropriate; sending quarterly study newsletters by both post and email; sending Christmas cards; delivering desktop reminders in the form of THREAD-branded computer screen stickers (furry worms) and notepads; and sending letters at intervals, pointing out items on depression in the popular or medical press. The researchers also attempted to make contact with the GPs when visiting the surgery to collect medical record data after participating patients had completed the study, and took the opportunity to request further referrals.
Clinical support officers of the Mental Health Research Network were also helpful in contacting practices to promote the study, particularly in the London and Liverpool centres.
Patient recruitment
Inclusion criteria
Patients were eligible for inclusion if:
-
they were aged 18 and above
-
they were diagnosed as depressed by their GP
-
they were potentially in need of treatment
-
they had had symptoms for at least 8 weeks
-
they had received no antidepressant treatment within the previous 12 months
-
they were not in receipt of counselling or psychological therapies at baseline
-
they agreed to discuss, with the research team, being allocated either to antidepressant treatment plus support from their GP or to GP support without drug treatment
-
at the baseline assessment, they scored between 12 and 19 on the HDRS19 (see below)
-
at the baseline assessment, they had at least one symptom on the Bradford Somatic Inventory (BSI). 51
It was stressed to the GPs that we were asking for patients to be referred into the study who had been diagnosed as depressed in the course of their usual consultations. We did not ask them to identify, by searching their practice records, patients who had been previously diagnosed, as we wanted only incident cases of depression where no antidepressant treatment had already been tried, rather than prevalent cases who had already had treatment, so they must not have received drug treatment for depression within the previous 12 months. This exclusion criterion was designed to limit the sample to patients presenting with new bouts of depression, as we aimed to determine the effectiveness and cost-effectiveness in new episodes and wanted to be clear we were not dealing with relapsing or chronic depression. To avoid including patients with more transient depression, for whom treatment might be unnecessary, patients needed to have had symptoms for at least 8 weeks. They also had to have at least one somatic symptom, as the Health Technology Assessment (HTA) commissioning brief for the study was the treatment of depression in patients with somatic symptoms.
We asked for referral of only those patients for whom the likely benefit of treatment was uncertain in the mind of the GP, as it was essential that the GP was in equipoise about the likely outcome. In addition, we asked for only those patients who were themselves in reasonable equipoise about the need for treatment, such that they would be prepared to be allocated to drug treatment or no drug treatment by the allocation process.
Exclusion criteria
Patients were excluded from the study if:
-
they did not have the spoken or written language skills necessary to take part
-
they expressed suicidal intent
-
at the baseline assessment, they were found to have HDRS scores of less than 12 or greater than 19
-
at the baseline assessment, they reported significant substance misuse, determined by screening questions (this was an addition to the original protocol)
-
at the baseline assessment, they scored more than 12 on the Alcohol Use Disorders Identification Test (AUDIT) questionnaire (this was an addition to the original protocol, see below). 58
The GPs were advised that patients expressing suicidal intent, and those scoring above 19 on the HDRS, would be considered to be suffering from severe depression and would therefore be ineligible for randomisation to treatments designed for mild to moderate depression. Those with scores of less than 12 were considered to be suffering from subthreshold symptoms, for which possible randomisation to drug treatment would be inappropriate given the risks of adverse effects. Patients with significant substance or alcohol misuse were excluded because of the risk of adverse interactions with antidepressants.
Patient consent
The task of referral of patients into the study was kept as simple as possible for the participating GPs, who were asked only to give a brief verbal explanation of the study to eligible patients and to obtain their consent for the research team to contact them. In the original proposal, only verbal consent was envisaged, but early in the course of the study, in July 2004, it was decided to change this to written consent, as some of the referring GPs were not happy to pass on patient details without such consent. The change was approved by the MREC and a form (see Appendix 3) was provided to the GPs to use for this purpose. The form was sent by fax to the research team, who then contacted the patient to arrange a visit to explain in detail what the study involved, prior to obtaining informed consent to take part. The patient was given a study information sheet (see Appendix 4) by the referring GP to read before the first visit from the researcher, which was usually within a few days of referral into the study, at which point the researcher dealt with any questions the patient had about the study. The patient was then given a further week to consider whether or not they wanted to take part and if they were happy to do so, the researcher returned to obtain written consent (see Appendix 5), before establishing the patient’s eligibility for the study and conducting the baseline assessment. This procedure, involving two researcher visits to obtain consent, was stipulated by the MREC, in order to give potential participants at least a week to consider joining the study.
In the original design, referred patients were given only two choices when asked for their written consent to participate: ‘yes’ or ‘no’. However, it was apparent early in the study that some patients remained undecided about taking part despite having had more than a week to consider it. Under the terms of the original protocol they were forced to make a decision at that point, and the default for those still undecided was to decline. As a relatively large number of possible participants who accepted referral to the study subsequently declined to take part at the point of obtaining written consent (see Chapter 4), it was decided, in July 2004, to give them a third option in order not to lose those who needed longer to decide whether or not to take part. In addition to an immediate ‘yes’ or ‘no’, they were offered a third option of ‘undecided’ which, it was explained, meant that they could be approached again 4 weeks later to reconsider participation. This change was approved by the MREC (see Appendix 6).
Piloting of partial patient preference design
Another strategy designed to tackle the issue of the large number of potential participants referred to the study who subsequently declined to take part was suggested by the Chair of the Data Monitoring and Ethics Committee (DMEC), Professor Michael King. He pointed out that a considerable number of patients declared that the reason they declined was because they could not accept possible randomisation to antidepressant drug treatment. He suggested adding a third, patient preference arm, in which patients could take part but have the treatment of their choice. Early in the course of the study, in December 2004, approval was gained from both the sponsor and the MREC to pilot a partial preference design. This was piloted in two of the three centres (Southampton and Liverpool) between January and April 2005. At the end of the pilot, the results were reviewed by the Study Group and Trial Steering Committee (TSC), and it was agreed not to change over to a partial preference design, as it was apparent that, while the total number of patients referred into the study did not increase significantly during the pilot, some patients who would have been prepared to be randomised had the choice of treatment not been offered, were deciding to enter the preference arm instead. So, although more patients in total could have been enrolled into the study by including a preference arm, this would have been at the expense of reduced numbers in the two randomised arms. The results of the partial preference pilot are shown in Chapter 4.
Randomisation and concealment of allocation
Block randomisation with random block sizes, stratified by severity subgroup (HDRS scores 12–15 and 16–19 respectively) and by recruiting centre, was carried out independently of the research team by the Institute of Psychiatry Mental Health and Neuroscience Clinical Trials Unit. Following completion of the baseline assessment, if the patient was eligible for randomisation, the researcher faxed the patient’s details to the study co-ordinator, who either emailed or telephoned the remote randomisation service. The study co-ordinator then faxed the allocation details to the GP (see Appendix 7) and informed the patient by telephone. If the patient was unsuitable, the GP received a fax explaining why the patient was not able to be entered into the study (see Appendix 8). The researcher who had visited and carried out the baseline assessment, therefore, remained blind to the treatment allocation. Wherever possible, the researchers were kept blind to the treatment arm while carrying out the follow-up interviews. Participating patients were asked, when contacted prior to the follow-up interviews, not to reveal whether or not they had been prescribed antidepressants. All instances where researchers became aware of the patient’s allocation to treatment arm were recorded.
Interventions
GP supportive care alone
The GPs were asked to arrange to see and provide support to the patients randomised to supportive care alone in follow-up consultations 2, 4, 8 and 12 weeks after the baseline assessment. They were not asked to provide any specific intervention during their consultations but were asked to refrain from prescribing antidepressants during this 12-week period. However, if the patients’ depression worsened during the 12 weeks and the GPs felt that they were in need of antidepressants then they were advised that they could initiate drug treatment. If this did occur, then the patients remained in the study and were followed up as planned, in the supportive care alone arm, on an intention-to-treat basis.
SSRI antidepressant plus GP supportive care
The GPs were asked to prescribe an SSRI antidepressant of their choice to those patients randomised to the drug arm of the trial, and to arrange to see them in consultations 2, 4, 8 and 12 weeks after randomisation, as above. In the original proposal, fluoxetine was identified as the drug of choice for the study, but it became apparent early in the recruitment of GPs, by July 2004, that restricting them to prescribing only one SSRI would preclude many of them from taking part. Therefore, the choice of antidepressant was extended to include all currently used SSRIs (fluvoxamine, sertraline, paroxetine, citalopram and escitalopram) rather than just fluoxetine. The GPs were also advised that they could switch antidepressants should the first choice prove unsuitable for the patient; initially switching to another SSRI if possible, but switching to a different class if that became necessary. The GPs were advised to continue treatment for 4 months after recovery (in line with antidepressant guidelines), but it was stressed to them that this was a pragmatic study, meant to be as close as possible to usual practice, and that they should use their clinical judgement in relation to the duration of treatment, in discussion with the patient.
Other treatments
After completion of the baseline assessment and randomisation, the GPs were free to refer patients in either arm for counselling, psychological therapy, exercise schemes, or other interventions for depression if this was appropriate in their judgement, but waiting times for counselling and psychological treatment were such that patients would not usually receive this before the 12-week follow-up assessment. All treatments received were recorded (see section on use of services, below).
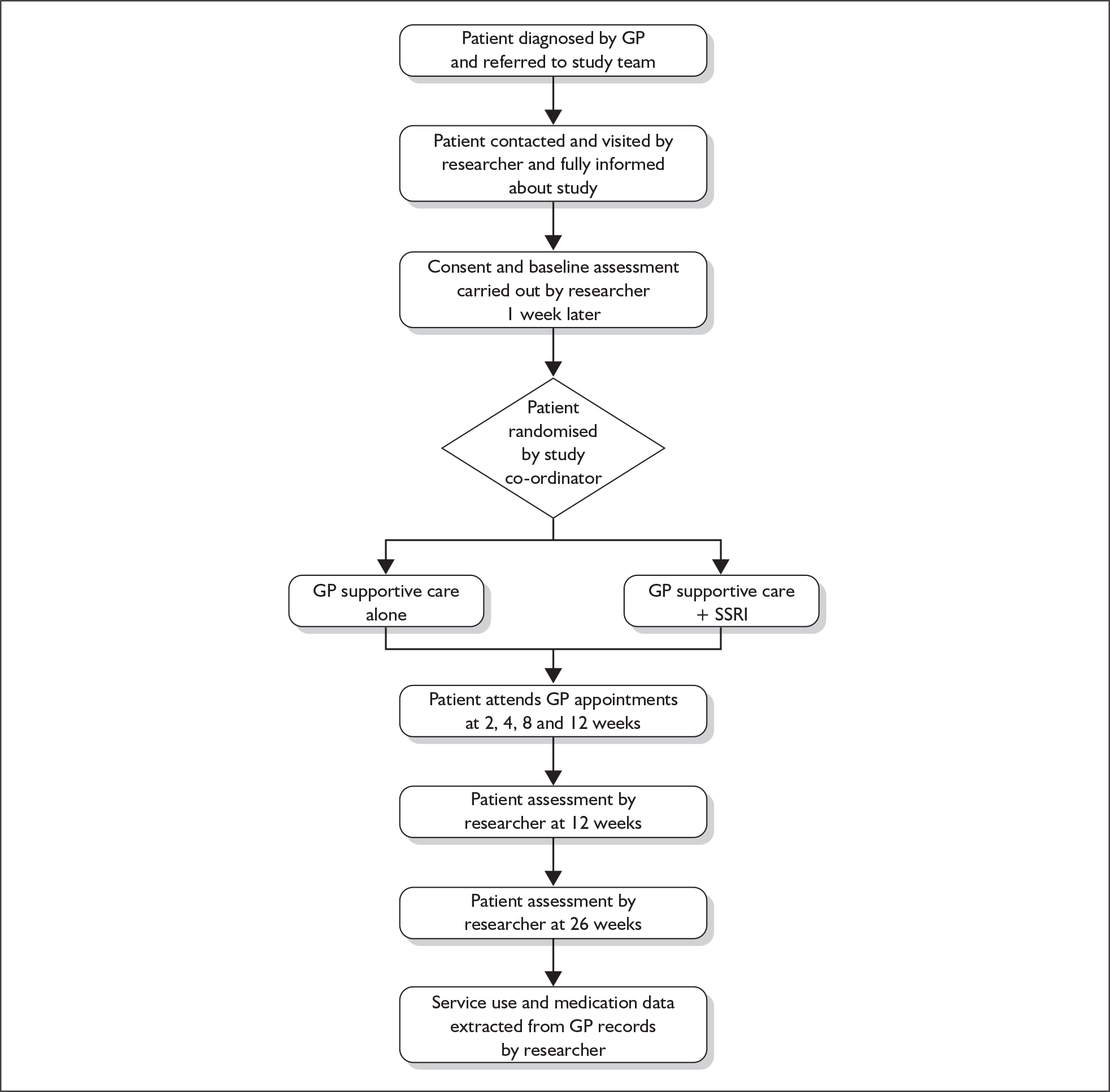
Patient assessments
The baseline assessment took place immediately after consent was obtained from the patient and follow-up interviews were carried out as close as possible to dates 12 and 26 weeks after randomisation. After 26 weeks, whether or not the patient had been assessed in follow-up interviews as planned, the researcher visited the patient’s practice and extracted data from their medical records, on health service contacts (including practice, community, and hospital contacts with GPs, nurses, hospital staff and community mental health professionals) and treatments received, including numbers of antidepressants prescribed. Figure 1 shows the flow of patients through the study.
FIGURE 1.
Flow of patients through the study.
Outcome measures
Depressive symptoms
The primary outcome measure was the score on the17-item HDRS at 12 weeks (see Appendix 9). 19 A large number of studies have shown the HDRS to be a valid and reliable measure of depression,59 and it has been shown to be sensitive to changes in response to drug treatment in a general practice setting. 60 All the researchers involved in assessing patients using the HDRS received extensive initial and follow-up training in the measure. 30
Initial training was carried out by a psychiatrist with long-standing experience of training investigators in the use of the HDRS for the purposes of clinical research, Dr David Baldwin of the Mental Health Group at the University of Southampton. Training included the use of three videotaped patients from psychiatry outpatients followed by observed live interviews with two patients, again from secondary care, all over the course of 1 day. Each case was discussed in detail to ensure that the interviewers were clear on the interpretation of each item. Following this structured training, the initial interviews carried out for the study were audiotaped, the patients having given their written informed consent, and rated jointly by the researchers and RM. RM provided feedback individually to the interviewers, then the three researchers and RM met to define issues of uncertainty, and to refine the interview and its scoring.
This was followed up 3 months later by RM who listened to audiotapes of the initial interviews carried out by the researchers, then met with them to provide further training to ensure uniformity of ratings. The inter-rater reliability of the HDRS ratings was assessed at four points during the 47 months of recruitment and follow-up: at 14, 17, 32 and 39 months. Each researcher was asked to audiotape all their HDRS interviews, as long as the patients gave consent, and to pass a random sample of them to a second researcher, who listened to the tape and independently rated all the items except those relating to non-verbal cues for ‘agitation’ and ‘retardation’. Three tapes were selected at random at 14, 17 and 32 months, and five at 39 months. We used audiotaping because it is more acceptable and less intrusive to patients than videotaping. Patients selected for inclusion in the inter-rater reliability testing included some just below the range of severity for inclusion in the study, some within the inclusion severity range, and some just above the severity for inclusion in the study. Patient interviews were included from both baseline and 12-week follow-ups. In this way, the inter-rater reliability across the whole range of scores from mild depressive symptoms to moderately severe depression was ascertained to check that patients were appropriately included into THREAD on the basis of severity and that they were reliably assessed at follow-up.
The Beck Depression Inventory (BDI) was used as a complementary measure of depressive symptoms (see Appendix 10). 61 This is a 21-item self-report inventory measuring characteristic attitudes and symptoms of depression, which has been validated for use in primary care. 62 As this is self-completed, it was considered that it should be free of observer bias and would enable a check to be carried out to ensure that there was no systematic bias in the HDRS ratings arising from possible unblinding of the researchers to treatment arm.
Quality of life
The Medical Outcomes Study Short Form 36-item (SF-36) questionnaire was used to measure health-related quality of life. 63 The responses to the 36 items can be condensed into scores in eight domains: physical functioning, role – physical, role – emotional, social functioning, bodily pain, vitality, mental health and general health (see Appendix 11). The SF-36 was also used to calculate quality-adjusted life-years (QALYs) to be used in the cost-effectiveness or cost–utility analysis.
Satisfaction with services received
Patient satisfaction was measured using the Medical Interview Satisfaction Scale (MISS),64 a 29-item self-completed scale developed to assess the patient’s satisfaction with the consultation. The scale was developed in the US but has been used previously in UK primary care practice. 65–68 Studies have compared it with other instruments,66 have demonstrated that it has similar properties in the UK to those reported from the US and have linked scores with both patient-centredness68 and enablement. 65 The scale consists of 29 items rated from 1 to 7 on a Likert range (very strongly disagree = 1 to very strongly agree = 7). The maximum score is therefore 7 × 29, i.e. 203. The 29 items include the patient’s ratings of: the doctor’s explanation of the illness and its seriousness; whether the doctor told the patient what they wanted to know; the doctor’s interest in the person; the doctor’s warmth; the doctor’s friendliness; treatment of the patient as an equal; the doctor’s understanding; relief of problems; relief of worries; and whether the patient felt they understood how to follow the doctor’s advice (see Appendix 12).
Use of health services
To ascertain health-care costs in each arm, health services use was measured comprehensively using a modified version of the Client Service Receipt Inventory (CSRI)69 at baseline and 26 weeks, asking about the previous 26 weeks at each point. Services measured included all contacts with GPs, other primary care professionals, psychiatrists, psychologists, community mental health nurses, counsellors, social care professionals and complementary therapists (see Appendices 13 and 14).
However, because patient recollection may not include all the services received over a 26-week period,70 the patient’s general practice medical record was also reviewed after the 26-week follow-up assessment. All GP consultations and other contacts with clinical practice staff were collected from the computerised records, along with outpatient and inpatient hospital contacts, referrals to counselling and psychological services, and any other treatment recorded at the practice. The dose and duration of any prescribed medications were also recorded. These data were collected for a period of 6 months before the date the patient entered the study as well as for the 6 months of participation in the study.
Costs of services used
The service use and medication data collected from the GP records were pooled with the CSRI data to maximise completeness (see Chapter 4 for which sources of data were used for which items of service use). Items of service use were multiplied by standard unit cost data to generate service costs for each patient.
Potential predictors
Sociodemographic questionnaire
A bespoke sociodemographic questionnaire was designed for the study, derived from previous trial instruments that have worked successfully. It included questions covering age, gender, ethnicity, marital status, accommodation, occupation and employment status (see Appendix 15), in order to determine whether these factors were associated with a differential response to treatment.
Previous experience of depression and antidepressants
In the original proposal, we planned to use questions from the PSE-SCAN psychiatric interview71 to determine the duration of depression and any past history of depression, in order to explore whether these factors were associated with a differential response to treatment. However, these questions would have significantly lengthened an already lengthy interview and so it was decided to replace them with a shorter bespoke questionnaire on the duration of the current episode of depression (asking when the patient last felt well, and how long they had felt this bad), previous episodes of depression (none, one, or more than one episode) and previous antidepressant treatment (yes or no, and how successful it was perceived to be). This change was approved by the MREC in July 2004. (The full questionnaire is reproduced in Appendix 16).
Life events and difficulties
The Life Events and Difficulties Schedule (LEDS) is usually used to collect information about stressful experiences over a 1-year period before onset/relapse of disorder. It differs from many other stress measures by distinguishing acute from ongoing stressors (events from difficulties), and by contrasting short- and long-term, and contextual and subjective ratings of these experiences. Specific qualitative aspects of stress such as losses, dangers, humiliations, entrapments, challenges and goal frustrations are also deliberately contrasted. 39 The shortened version of the LEDS (S-LEDS) was used in this study (see Appendix 17); essentially, this is rated using the same interview process, but the ratings concentrate on those events that are considered severe, with marked or moderate threat to the individual (and not on those that are deemed to carry only some or little threat), plus ‘fresh start’ experiences of the type found to predict depressive remission.
The three original researchers, a fourth researcher recruited later to replace one of the researchers who left, and the trial co-ordinator, all completed a week-long training course in London on the full LEDS with TH. She continued to support the researchers and regular consensus meetings were held to clarify any ambiguities that may have occurred with regard to the ratings of individual items.
Alcohol consumption
In a change to the original protocol, approved by the MREC, the AUDIT was added to measure alcohol consumption at baseline. This is a 10-item questionnaire, developed for the World Health Organization to screen for hazardous alcohol intake in primary health-care settings. It has high sensitivity and specificity and can be self-completed or administered in 2–4 minutes (see Appendix 18). 58
Somatic symptoms
The BSI was used to measure somatic symptoms at baseline. This is a 46-item questionnaire about symptoms experienced in the last month, which was designed to detect physical symptoms that are commonly found in depressed patients (see Appendix 19). 51
Symptom attribution
We considered it important to assess patients’ attributions of their symptoms to physical or psychological causes, as a patient with a physical attribution might be more likely to respond to a physical treatment in the form of antidepressants. In the original proposal, we planned to use questions from the revised Illness Perception Questionnaire to assess symptom attribution at baseline. However, these questions would have significantly lengthened an already lengthy interview and so we decided instead to use a single question to determine the patient’s broad attribution of their symptoms to one of three categories: physical cause; stress or emotional cause; or unknown cause (see Appendix 20). This change was approved by the MREC in July 2004.
Patient preference
Participating patients were asked to indicate, prior to randomisation, whether, if they had had a choice of treatments, they had a preference for supportive care without antidepressants, supportive care with antidepressants or no preference, in order to determine whether getting their choice of treatment was associated with a better outcome. The questions used are reproduced as Appendix 21.
Care received questionnaire
At both the 12- and 26-week follow-ups, the care received by participating patients in consultations was measured using a self-reported questionnaire designed specifically for the study (this was an addition to the original protocol). This included a range of depression-specific components of GP consultations, the Psycho-Socially Active Consultation (PSAC) questionnaire, in order to determine whether the support provided by the GPs was comparable in both arms in terms of potentially psychologically helpful consultation techniques. The components included discussion or advice on: tackling practical problems; taking more exercise; relaxation exercises; finding more leisure time; identifying enjoyable activities; addressing personal relationships; changing work patterns; and changing thought patterns. The questionnaire also included a question about patients’ use of antidepressants and four questions devised by Morisky et al. 72 to measure patient adherence to the medication for those prescribed antidepressants, in either arm of the trial. (Appendix 22 shows the full questionnaire). In order to avoid unblinding the researchers, this questionnaire was completed while the researcher was out of the room and was placed in an envelope for direct transportation to the study co-ordinator, so that the researchers did not see any information on patients’ use of antidepressants.
Data entry
The data arising from each baseline or follow-up interview were entered by each of the researchers as the study proceeded. A proportion of the data was double entered by the study co-ordinator JC (12 baseline interviews, ten 12-week interviews and ten 26-week interviews). Comparison of the two sets of data for these interviews confirmed the accuracy of the researchers’ data entry. Table 1 summarises the measures that were used at each point.
| Measures | Baseline | 12-week follow-up | 26-week follow-up |
|---|---|---|---|
| Outcomes | |||
| 17-item Hamilton Depression Rating Scale (HDRS) interview | ✓ | ✓ | ✓ |
| Beck Depression Inventory (BDI) | ✓ | ✓ | ✓ |
| Medical Outcomes Study Short Form 36-item (SF-36) questionnaire | ✓ | ✓ | ✓ |
| Medical Interview Satisfaction Scale (MISS) | ✓ | ✓ | |
| Client Service Receipt Inventory (CSRI) | ✓ | ✓ | |
| Predictors | |||
| Sociodemographic questionnaire | ✓ | ||
| Previous experience of depression questionnaire | ✓ | ||
| Short Life Events and Difficulties Schedule (S-LEDS) | ✓ | ✓ | |
| Alcohol Use Disorders Identification Test (AUDIT) | ✓ | ||
| Bradford Somatic Inventory (BSI) | ✓ | ||
| Symptom attribution questionnaire | ✓ | ||
| Patient treatment preference questionnaire | ✓ | ||
| Psycho-Socially Active Consultation (PSAC) questionnaire | ✓ | ✓ | |
Sample size calculation
The sample size calculation was based on a planned analysis of the HDRS score as the primary outcome for two severity subgroups, corresponding to mild and moderate depression (with HDRS scores of 12–15 and 16–19 respectively). Hollyman et al. 73 found the standard deviation (SD) of the HDRS to be around 3.5, and reported roughly similar numbers of patients in these two severity ranges. We assumed this SD, equal numbers in the two subgroups and a pre–post correlation of 0.5.
Using analysis of covariance controlling for baseline values, we calculated that 49 patients at follow-up in each treatment/severity combination would allow the following effects to be detected at a significance level of 0.05 (standard effect sizes in brackets): an overall average difference in HDRS scores between the two treatment arms of 1.4 (0.4) with 90% power; an interaction (difference between effects in the two severity subgroups) of 2.5 (0.7) with 80% power; and a difference between treatment arms within the more severe group of 2.0 (0.6) with 90% power. The last two calculations were conservative (tending to underestimate the power) because we considered that the SDs could turn out to be lower within the severity subgroups. A difference of 1.4 on the HDRS is relatively small (SD 0.4) and any difference smaller than this we regarded as clinically insignificant. In the trial of amitriptyline by Hollyman et al. 73 the HDRS scores fell by a mean of around 10 points in the mildly depressed group and around 13 in the more severely affected group. Therefore, we calculated that the sample size should be sufficient to detect clinically significant differences.
We therefore needed to follow up 196 patients to detect these differences (98 in each of the two arms). To allow for up to 25% loss to follow-up at 12 weeks, we calculated that 261 (87 at each of the three sites) would be needed. The agreed initial aim was to recruit even more than that number, 300 patients in all, aiming for 100 at each recruitment site (Southampton, Liverpool and London).
Statistical analysis
The primary analysis was by intention to treat (all available data analysed in the groups as randomised) using double-sided significance tests. We used analysis of covariance, controlling for baseline value and recruitment site, to estimate the overall treatment effectiveness (difference between arms in HDRS score) at both follow-ups separately (with 12-week outcome as the primary outcome). Longitudinal analysis, in which 12-week and 26-week outcomes were modelled simultaneously, was also performed. Time point, and time point × treatment interaction effects were tested in these models. Baseline predictors of a lack of follow-up data (‘missingness’) at either follow-up were investigated by means of logistic regression, and the models of predictors of 12- and 26-week outcomes were refitted including these variables. In all models, the patient’s GP was included as a random effect and, as a sensitivity analysis, the overall (longitudinal model) was also fitted including GP practice as an alternative random effect. The interaction between severity subgroup and treatment was also tested, and further exploratory analyses assessed the impact of other potential predictors.
The main aim of the economic analysis was to compare the two treatment groups in terms of mean costs and cost-effectiveness. A secondary aim was to examine differences between the subgroups defined by severity, if differences in effectiveness were found for the severity subgroups. Given that cost data are frequently skewed, which can cause a violation of the assumptions of standard significance tests, bootstrapped estimates (multiple resampling within treatment arms) were planned, so that mean costs could still be compared while imposing no prior assumptions regarding the data distribution.
Cost-effectiveness was expressed in terms of incremental cost-effectiveness ratios (ICERs) and cost–utility ratios. In addition, cost-effectiveness acceptability curves (CEACs) were generated, synthesising data on costs and outcomes, for varying levels of acceptability of costs.
Chapter 3 Recruitment, follow-up rates and inter-rater reliability
Recruitment of practices and GPs
Prior to commencement of the study, NHS R&D approval was sought from those PCTs closest to the study centres and most accessible for the research teams. Very early on in the process of recruitment, it became apparent that progress was going to prove challenging, and therefore it was essential to recruit new practices further afield. A rolling plan of seeking NHS R&D approval from additional PCTs was therefore introduced across all three centres, and throughout 2004, 2005 and 2006 the team wrote to successive groups of GPs, in practices progressively further away from the centres, asking for their interest in participating.
Table 2 shows that, around the three centres, 6015 GPs in1787 practices were approached, and 576 GPs (9.6% of those approached) were inducted into the study from 212 (11.8%) of the practices approached. It should be noted that the number of GPs agreeing to participate is an approximation. If a practice agreed to participate, and all the GPs were present when the research team visited to discuss the study, it was assumed that they were all interested in taking part but it was not possible to be certain that all doctors within any one practice had, in fact, agreed.
| Centre | Number of practices approached | Number of GPs approached | Number of participating practices | Number of participating GPs |
|---|---|---|---|---|
| Southampton | 496 | 2181 | 92 | 218 |
| London | 471 | 1244 | 42 | 136 |
| Liverpool | 820 | 2590 | 78 | 222 |
| Total | 1787 | 6015 | 212 (11.8%) | 576 (9.6%) |
The Royal College of General Practitioners (RCGP)74 estimated that there were 8451 practices in England in 2006, which means that during the course of the study approximately one in five of all practices in England were approached from the three centres.
Tables 3–5 show the number of GPs, by PCT, who were approached to assess their interest. Table 3 shows that agreement to take part was secured from 10% of the GPs approached from 18.5% of the practices in PCTs around the Southampton centre. Table 4 shows that the corresponding figures for the London centre were 10.9% of GPs from 8.9% of practices approached. Table 5 shows that the figures for the Liverpool centre were 8.6% of GPs from 9.5% of practices approached.
| Primary care trust | Number of practices approached | Number of GPs approached | Number of participating practices | Number of participating GPs |
|---|---|---|---|---|
| Blackwater Valley | 21 | 94 | 6 | 10 |
| Bournemouth | 26 | 106 | 5 | 16 |
| East Hampshire | 30 | 125 | 5 | 22 |
| Eastleigh & Test Valley | 20 | 103 | 6 | 9 |
| Fareham & Gosport | 20 | 99 | 5 | 7 |
| Guildford & Waverley | 29 | 155 | 3 | 12 |
| Isle of Wight | 12 | 65 | 4 | 9 |
| Kennet & North Wiltshire | 22 | 93 | 0 | 0 |
| Mid Hampshire | 22 | 110 | 4 | 16 |
| New Forest | 24 | 114 | 4 | 5 |
| Newbury & Community | 11 | 61 | 1 | 4 |
| North Dorset | 15 | 56 | 4 | 8 |
| North Hampshire | 28 | 113 | 10 | 21 |
| Poole | 24 | 107 | 2 | 3 |
| Portsmouth | 29 | 107 | 6 | 16 |
| Reading | 29 | 117 | 1 | 1 |
| South & East Dorset | 23 | 107 | 3 | 7 |
| South Wiltshire | 22 | 81 | 8 | 19 |
| Southampton City | 38 | 173 | 11 | 22 |
| Swindon | 29 | 104 | 3 | 8 |
| West Sussex | 22 | 90 | 2 | 3 |
| Total | 496 | 2180 | 93 (18.7%) | 218 (10%) |
| Primary care trust | Number of practices approached | Number of GPs approached | Number of participating practices | Number of participating GPs |
|---|---|---|---|---|
| Bromley | 57 | 27 | 0 | 0 |
| Croydon | 65 | 88 | 9 | 30 |
| Kingston | 35 | 99 | 1 | 1 |
| Lambeth | 52 | 206 | 7 | 23 |
| Lewisham | 50 | 185 | 8 | 28 |
| Richmond | 34 | 97 | 1 | 2 |
| Southwark | 51 | 150 | 8 | 28 |
| Sutton | 65 | 221 | 3 | 11 |
| Wandsworth | 62 | 171 | 5 | 13 |
| Total | 471 | 1244 | 42 (8.9%) | 136 (10.9%) |
| Primary care trust | Number of practices approached | Number of GPs approached | Number of participating practices | Number of participating GPs |
|---|---|---|---|---|
| Ashton, Wigan & Leigh | 54 | 164 | 1 | 5 |
| Bebington & West Wirral | 17 | 63 | 2 | 2 |
| Birkenhead & Wallasey | 37 | 120 | 7 | 23 |
| Bolton | 58 | 176 | 5 | 13 |
| Bury | 33 | 104 | 1 | 4 |
| Central Cheshire | 31 | 167 | 5 | 34 |
| Central Liverpool | 61 | 150 | 12 | 38 |
| Cheshire West | 26 | 103 | 5 | 10 |
| Chorley & South Ribble | 37 | 109 | 0 | 0 |
| Eastern Cheshire | 23 | 114 | 3 | 13 |
| Ellesmere Port & Neston | 13 | 53 | 1 | 4 |
| Halton | 16 | 63 | 1 | 1 |
| Heywood & Middleton | 14 | 41 | 0 | 0 |
| Knowsley | 31 | 90 | 4 | 3 |
| North Liverpool | 22 | 63 | 4 | 18 |
| Oldham | 43 | 113 | 2 | 4 |
| Preston | 29 | 81 | 2 | 2 |
| Rochdale | 21 | 74 | 1 | 1 |
| Salford | 49 | 124 | 6 | 12 |
| South Liverpool | 17 | 51 | 4 | 12 |
| Southport & Formby | 20 | 72 | 0 | 0 |
| South Sefton | 33 | 85 | 4 | 8 |
| St Helens | 35 | 109 | 3 | 5 |
| Trafford North | 18 | 53 | 1 | 1 |
| Trafford South | 26 | 70 | 1 | 1 |
| Warrington | 31 | 123 | 1 | 1 |
| West Lancashire | 25 | 55 | 2 | 7 |
| Total | 820 | 2590 | 78 (9.5%) | 222 (8.6%) |
Table 6 shows that, compared with the RCGP figures for England as a whole, the participating GPs were broadly representative in terms of gender and whether they were part time or full time. However, the study practices were larger on average than practices in England generally.
| Female (%) | Part time (%) | Average list size of practice | |
|---|---|---|---|
| THREAD GPs | 38 | 29 | 7516 |
| RCGP figures | 40 | 25 | 6250 |
Table 7 shows the range of locations of participating practices by recruitment centre. In 30 cases (14%) no information was received from the practice manager or GPs about practice location.
| Location | Southampton | London | Liverpool | Total |
|---|---|---|---|---|
| Rural [n (%)] | 15 (16) | 0 | 5 (6) | 20 (9) |
| Semi-rural [n (%)] | 16 (17) | 0 | 9 (12) | 25 (12) |
| Suburban [n (%)] | 39 (43) | 11 (26) | 23 (29) | 73 (34) |
| City [n (%)] | 20 (22) | 19 (45) | 25 (32) | 64 (30) |
| Missing [n (%)] | 2 (2) | 12 (29) | 16 (21) | 30 (14) |
| Total | 92 | 42 | 78 | 212 |
Table 8 shows the number of practices and GPs who referred patients into the study by centre and the number of practices and GPs who had patients randomised into the study. Overall, only around half of the practices agreeing to participate actually referred patients into the study. Of those practices who did refer patients, only 37% overall had patients randomised into the study. The lowest ratio of randomised patients to referred patients was found in Liverpool. Reasons for this are considered in Recruitment of patients, below.
| Southampton | London | Liverpool | Total | |
|---|---|---|---|---|
| Number of practices agreeing to participate | 92 | 42 | 78 | 212 |
| Number of practices (%) who referred patients | 57 (61.9) | 21 (50.0) | 37 (47.4) | 115 (54.2) |
| Number of practices (%) who had patients randomised into the study | 46 (50.0) | 17 (40.4) | 20 (25.6) | 83 (39.1) |
| Number of GPs agreeing to participate | 218 | 136 | 222 | 576 |
| Number of GPs (%) who referred patients | 93 (42.6) | 26 (19.1) | 58 (26.1) | 177 (30.7) |
| Number of GPs (%) who had patients randomised into the study | 62 (28.4) | 19 (13.9) | 27 (12.1) | 98 (17) |
The mean and range of referrals per practice was 5.23 (1–32) and the mean and range of patients randomised was 2.68 (1–15).
Recruitment of patients
During the recruitment phase of the study, between December 2003 and May 2007 (42 months), 602 patients in total were referred to the study team across the three centres. However, only 220 of these were actually randomised into the study. Table 9 shows the reasons why the remaining 382 patients were either excluded or declined to participate having had the study explained to them in more detail.
| Southampton | London | Liverpool | Total | |
|---|---|---|---|---|
| Number of patients referred into study | 292 | 108 | 202 | 602 |
| Reasons for exclusion | ||||
| Hamilton (HDRS) score > 19 | 19 | 8 | 13 | 40 |
| Hamilton (HDRS) score < 12 | 31 | 9 | 7 | 47 |
| Antidepressants received in last 12 months | 17 | 7 | 26 | 50 |
| Alcohol consumption too high | 2 | 1 | 5 | 8 |
| Personally known to the researcher | 1 | 0 | 0 | 1 |
| Currently receiving counselling | 1 | 0 | 4 | 5 |
| Drug misuse | 0 | 1 | 0 | 1 |
| Under 18 | 0 | 1 | 0 | 1 |
| Suicide risk | 2 | 2 | 5 | 9 |
| Breastfeeding | 0 | 0 | 1 | 1 |
| Entered partial preference pilot | 6 | 0 | 3 | 9 |
| Total number (%) excluded | 79 (27) | 29 (27) | 64 (32) | 172 (29) |
| Reasons for declining to participate | ||||
| Strong preference against antidepressants | 29 | 11 | 37 | 77 |
| Strong preference for antidepressants | 4 | 0 | 2 | 6 |
| Unable to contact or failed to attend | 20 | 6 | 16 | 42 |
| Problem with the study arrangements | 22 | 7 | 11 | 40 |
| No longer feeling depressed or did not consider self depressed | 11 | 3 | 6 | 20 |
| Too unwell or distressed | 0 | 0 | 1 | 1 |
| No reason given | 8 | 1 | 15 | 24 |
| Total number (%) who declined | 94 (32) | 28 (26) | 88 (44) | 210 (35) |
| Total number (%) of patients randomised | 119 (41) | 51 (47) | 50 (25) | 220 (37) |
Table 9 shows that more patients declined to take part in Liverpool, which was due mainly to a greater proportion having a strong preference against taking antidepressants (18%, versus 10% in Southampton and 10% in London), as well as a greater proportion declining to participate but giving no reason for their decision (7%, versus 3% in Southampton and 1% in London). Discussion with the Liverpool team about the reasons for this identified as a possible factor the apparently much greater availability of counselling in Liverpool than in London and Southampton. It seemed likely that patients in Liverpool had more options for treatment besides drug treatment and more support from the GP, because the waiting list for counselling was only a matter of days, compared with months in London and Southampton.
Partial preference pilot
A partial preference design was piloted in two of the three centres (Southampton and Liverpool) between January and April 2005, to explore whether this would increase the rate of referral into the study. (It was not piloted in London as the researcher there was on leave for January 2005.) The results of the partial preference pilot are shown in Table 10. This shows that, despite patients having the freedom to choose which treatment they would receive, the total number of patients referred into the study did not increase significantly during the preference pilot. Nor was there any reduction in the number of patients declining to take part (there was a reduction in the number of patients excluded, but this could not have been related to patient preference and so must have arisen by chance). Furthermore, the researchers reported that three of the nine patients who entered the preference arms informed the researchers that they would have agreed to be randomised if choosing which arm they entered had not been an option. Therefore it was decided not to change over to a partial preference design, as it was apparent that, although more patients in total could have been enrolled into the study by including a preference arm, this seemed likely to be at the expense of reduced numbers in the two randomised arms. Maximising the numbers agreeing to be randomised was most important in order to fulfil the aims of the study.
| September–December 2004 | January–April 2005 | |
|---|---|---|
| Number of patients referred | 85 | 87 |
| Number of patients excluded | 35 | 22 |
| Number of patients who declined to take part | 23 | 24 |
| Number of patients who entered preference arms | – | 9 |
| Number of patients randomised | 27 | 32 |
Representativeness of patients randomised into the study
Table 11 shows the gender and age profiles of patients referred into the study, those randomised and those not randomised. This shows that those patients who were randomised were generally representative in terms of gender and age of the total number of patients referred into the study. Two-thirds of the patients were female, and 90% were of working age.
| Male [n (%)] | Female [n (%)] | Age < 65 [n (%)] | Age ≥ 65 [n (%)] | Age missing [n (%)] | Total (n) | |
|---|---|---|---|---|---|---|
| Patients referred into study | 194 (32) | 408 (68) | 550 (91) | 39 (6) | 13 (2) | 602 |
| Patients randomised | 67 (31) | 153 (69) | 208 (94) | 12 (6) | 0 (0) | 220 |
It was clear during the first 6 months of the study that the rate of referral of depressed patients into the study was very much lower than the rate of patients presenting with new episodes of depression to GPs in their surgeries. To explore reasons for this, those members of the Study Group who were practising GPs agreed to complete a tally of patients with depression seen in their surgeries, and to ask GP colleagues in their practices to do the same. Tallies were kept over four periods during patient recruitment, and each time the data collection evolved in the light of experience from the previous exercise, so that the later tallies included more information on why patients presenting with depression were not referred into the study. Table 12 summarises the findings of the four periods.
| Tally period | Recording dates | Number of surgery sessions | Number of consultations | Number of patients already taking anti-depressants | Number of new cases | Number of patients referred (%) | Number of patients randomised (%) |
|---|---|---|---|---|---|---|---|
| 1 | 20.5.04–24.11.04 | 167 | 2385 | 304 | 92 | 9 (10) | 2 (2) |
| 2 | 15.2.05–1.7.05 | 168 | 2126 | 244 | 41 | 6 (15) | 1 (2) |
| 3 | 4.10.05–10.2.06 | 182 | 2547 | 313 | 56 | 0 | 0 |
| 4 | 2.10.06–5.12.06 | 249 | 3613 | Not recorded | 76 | 7 (9) | 3 (4) |
Table 12 shows that new episodes of depression were uncommon, occurring in only 2.5% of consultations, and only around 1 in 10 eligible patients were referred into the study. Table 13 shows the age and gender profiles of patients presenting with depression in the third tally period (October 2005 to February 2006) compared with those referred into the study over the whole recruitment period. There was no significant difference in terms of age between eligible patients presenting in surgery and patients referred into the study (χ2 = 0.14, df = 1, p = 0.709), but a lower proportion of male patients were referred into the study than presented in surgery (χ2 = 20.58, df = 1, p < 0.001).
| Male [n (%)] | Female [n (%)] | Gender missing [n (%)] | Age < 65 [n (%)] | Age ≥ 65 [n (%)] | Age missing [n (%)] | Total (n) | |
|---|---|---|---|---|---|---|---|
| Eligible patients presenting in surgery | 32 (57) | 18 (32) | 6 (11) | 46 (82) | 4 (7) | 6 (11) | 56 |
| Patients referred into study | 194 (32) | 408 (68) | 0 (0) | 550 (91) | 39 (6) | 13 (2) | 602 |
More detail from the last of the four tallies is shown in Table 14, which gives the reasons why potentially eligible patients were not referred into the study. For this tally period, a total of 25 GPs returned forms (19 from Southampton and six from Liverpool), including information recorded during 249 surgeries involving 3613 consultations over a 2-month period between 2 October and 5 December 2006.
| Reason | Number of patients |
|---|---|
| Total number presenting with a new episode of depression | 76 |
| Number of patients referred into study | 7 |
| Reason for not referring patient | |
| GP or patient has a preference for antidepressants | 16 |
| GP or patient has a preference against antidepressants | 11 |
| GP perceived level of severity to be too high | 11 |
| GP perceived level of severity to be too low | 4 |
| Patient received antidepressants in last year | 5 |
| Patient has been told about study and is thinking about it | 4 |
| Not asked about study | 3 |
| Declined to take part in study | 3 |
| Already having counselling or psychological treatment | 2 |
| Does not accept diagnosis of depression | 1 |
| Drug or alcohol misuse problem | 2 |
| Under 18 years of age | 1 |
| Result of HADS questionnaire pending | 1 |
| Has multiple physical pathology | 1 |
| Does not speak English | 1 |
| Has terminal disease | 1 |
| Postnatal | 1 |
| Not using contraception | 1 |
Follow-up assessments
The first follow-up assessments were scheduled for as close as possible to 12 weeks (84 days) after the baseline assessment and the second for as close as possible to 26 weeks (182 days). Table 15 shows the range of timing of the follow-up assessments.
| 12 weeks (84 days) | 26 weeks (182 days) | |
|---|---|---|
| Number of patients | 186 | 167 |
| Mean days from baseline | 91 | 191 |
| Range | 73–131 | 157–245 |
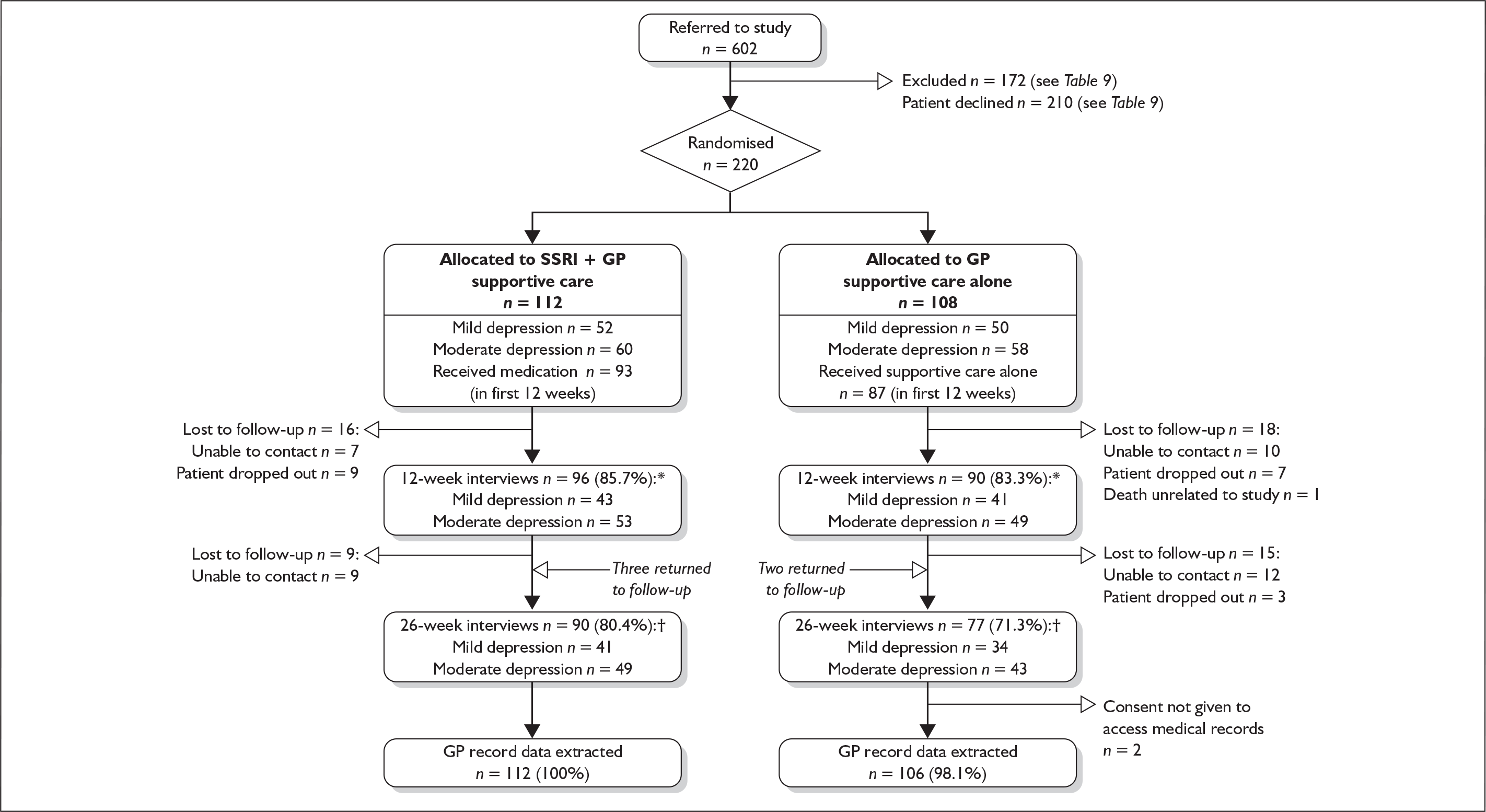
The follow-up rates for each of the time points remained consistent throughout the study. Figure 2 shows that a total of 186 patients were interviewed at the 12-week follow-up and 167 at the 26-week follow-up. Table 16 shows the follow-up rates for each of the three recruiting centres.
FIGURE 2.
CONSORT diagram. * 84.5% follow-up at 12 weeks; † 75.9% follow-up at 26 weeks.
| Centre | Number randomised | 12-week follow-up completed [n (%)] | 26-week follow-up completed [n (%)] |
|---|---|---|---|
| Southampton | 119 | 105 (88.2) | 98 (82.3) |
| London | 51 | 39 (76.4) | 29 (56.8) |
| Liverpool | 50 | 42 (84) | 40 (80) |
| Total | 220 | 186 (84.5) | 167 (75.9) |
Patients were encouraged to make appointments for the next follow-up assessment by the researchers at the baseline or 12-week interview, but this was not always possible. If they did, letters were sent out 2 weeks prior to the appointment to remind them and the researcher would carry out the visit as planned. Sometimes the patient did not attend, in which case repeated attempts were made, if necessary, to contact the patient by means of telephone calls and letters to reschedule the follow-up visit. If no contact was made within 4 weeks, it was considered inappropriate to continue to pursue the patient at that time point, but patients unobtainable at 12 weeks were contacted again when the 26-week time point was reached. Figure 2 shows that in five cases it was possible to collect data at the 26-week time point for patients who had not been followed-up at the 12-week time point.
Figure 2 also shows that there was a slight difference in rate of follow-up between the SSRI plus supportive care group and the supportive care alone group at the 12-week follow-up point (86% versus 83%), which became greater at the 26-week follow-up (80% versus 71%).
Blindness of researchers to allocation of patients
Remote telephone randomisation of the patients was carried out by the study co-ordinator after the baseline assessment, in order to keep the researchers blind to patient allocation. In addition, it was stressed to the patients at the start of the assessments that when the researchers went back to visit them, they must not tell the researchers to which arm they had been randomised. However, it proved impossible to maintain blindness in a number of cases, as shown in Table 17. Overall, at the 12-week interviews, failure of blinding occurred in 46 (25%) cases and at 26 weeks this rose to 53 (32%).
| Number of interviews | Supportive care alone | SSRI plus supportive care | Total |
|---|---|---|---|
| 12-week follow-up | n = 90 | n = 96 | n = 186 |
| Southampton (n = 105) | 12 | 11 | 23 (22%) |
| London (n = 39) | 3 | 9 | 12 (31%) |
| Liverpool (n = 42) | 4 | 7 | 11 (26%) |
| Total | 17 (21%) | 29 (28%) | 46 (25%) |
| 26-week follow-up | n = 77 | n = 90 | n = 167 |
| Southampton (n = 98) | 9 | 16 | 25 (26%) |
| London (n = 29) | 3 | 10 | 13 (45%) |
| Liverpool (n = 40) | 8 | 7 | 15 (37%) |
| Total | 20 (26%) | 33 (37%) | 53 (32%) |
Inter-rater reliability
The inter-rater reliability of the HDRS ratings was assessed at 3 months, as described in Chapter 2, and again at four points during the 47 months of recruitment and follow-up: at 14, 17, 32 and 39 months (October 2004, January 2005, April 2006 and November 2006). Data from all possible pairs of the four raters were obtained in each of the four inter-rater reliability sessions. Within a session, each researcher took the role of primary rater (having taped the interview) an equal number of times, and everyone re-rated each other’s tapes, so that raters and modes of rating were balanced within sessions. Each patient provided two sets of ratings, apart from one, who was assessed by two pairs of raters. A total of 84 ratings from 10 different pairs of raters for 42 patients were available. The patients included in the inter-rater reliability exercise had a mean age of 43.7 years (SD 17.1, range 18–78); 31 (87%) were female; and patients had a mean total score on the 17-item HDRS of 14.9 (SD 4.8, range 5–27). Sixty-six per cent of the total HDRS scores were in the 12–19 range used for inclusion in the THREAD study.
For individual items, the distribution of scores for the primary rater was examined, and overall percentage agreement and both weighted and unweighted kappa statistics were calculated. Weights were lower for disagreements that were further apart (Table 18).
| Item | Responses of primary interviewer (%) (n = 42) | Unweighted | Weighteda | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | Agreement (%) | Kappa | Agreement (%) | Kappa | ||
| 1 | Depressed mood | 11 | 25 | 51 | 13 | 67 | 0.49 | 88 | 0.59 |
| 2 | Guilt | 21 | 24 | 55 | – | 86 | 0.77 | 95 | 0.83 |
| 3 | Suicidality | 69 | 17 | 12 | 2 | 74 | 0.47 | 90 | 0.59 |
| 4 | Initial sleep | 45 | 19 | 36 | – | 88 | 0.81 | 94 | 0.88 |
| 5 | Middle sleep | 24 | 24 | 52 | – | 86 | 0.76 | 93 | 0.83 |
| 6 | Delayed sleep | 29 | 38 | 33 | – | 81 | 0.71 | 90 | 0.78 |
| 7 | Work and interests | 12 | 24 | 59 | 5 | 76 | 0.60 | 92 | 0.70 |
| 10 | Psychic anxiety | 5 | 26 | 67 | 2 | 88 | 0.75 | 96 | 0.78 |
| 11 | Somatic anxiety | 14 | 45 | 38 | 2 | 76 | 0.63 | 92 | 0.71 |
| 12 | Gastrointestinal | 59 | 36 | 5 | – | 83 | 0.69 | 92 | 0.73 |
| 13 | Somatic, general | 9 | 31 | 60 | – | 74 | 0.54 | 87 | 0.61 |
| 14 | Genital symptoms | 48 | 19 | 33 | – | 90 | 0.85 | 93 | 0.85 |
| 15 | Hypochondriasis | 93 | 7 | – | – | 95 | 0.48 | 95 | 0.48 |
| 16 | Weight | 76 | 7 | 17 | – | 95 | 0.88 | 96 | 0.90 |
| 17 | Insight | 76 | 24 | – | – | 74 | 0.30 | 74 | 0.30 |
Most weighted kappa coefficients were above 0.6, indicating good agreement; the items for depressed mood and suicidal tendencies were just below this level. The kappa for hypochondriasis was relatively low, but this item had a very skewed distribution, with only 7% having a positive rating. Insight appeared to be the most difficult to rate, with a weighted kappa of only 0.3 and overall agreement of 76%.
Table 19 shows the inter-rater agreement for the total scores in each of the four sessions and overall. Total scores were pro-rated from 15 items to the equivalent of 17 items because items 8 and 9, retardation and agitation, were visually assessed and could not be rated from the audiotapes. Both intraclass correlations (and concordance coefficients, which are not shown as they were almost identical) showed very good agreement in all sessions. The overall estimate of the measurement variance was 1.55 (standard error 0.75), equivalent to a measurement error for an individual score of 1.25. The measurement error decreased in session 3 but the patient-level variance also decreased, thus resulting in a slightly lower reliability coefficient. However, this difference was not statistically significant. There was no evidence of systematic bias, with one rater tending to score higher or lower than the others (based on a regression with raters as fixed effects), or bias between the primary ratings and the corresponding secondary ratings, based on audiotapes (using paired t-tests).
| Intraclass correlation | Standard error of measurement | |
|---|---|---|
| Session 1 | 0.968 | 1.28 |
| Session 2 | 0.937 | 1.49 |
| Session 3 | 0.896 | 1.02 |
| Session 4 | 0.938 | 1.24 |
| Overall | 0.947 | 1.25 |
Figure 3 shows the difference between a pair of raters in total HDRS score plotted against the level of severity of depression as reflected in the average HDRS score; there is no evidence of variation in measurement error with severity.
FIGURE 3.
Difference in HDRS scores between two raters on the same individuals plotted against their mean score.
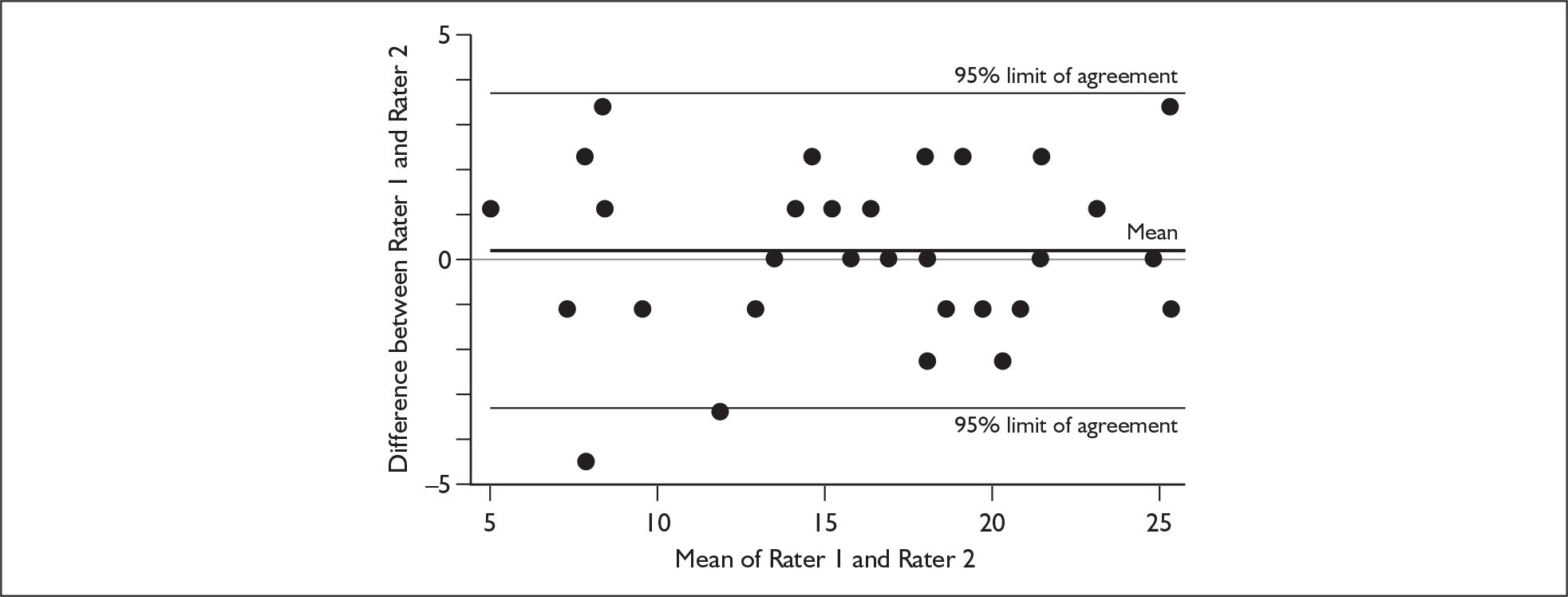
The reference range (–3.31 to 3.69) shows where 95% of the points lie; only one point is outside these limits. The proportion who would have been assigned to a different severity subgroup depending on the rater was 2/42 (5%).
Chapter 4 Results: depression, generic health status and patient satisfaction
This chapter presents the results for effectiveness in terms of changes in the primary outcome, the HDRS score at 12 weeks. Results for the HDRS score at 26 weeks are also presented, followed by analyses of covariance of the HDRS scores at both follow-up points. This is followed by a longitudinal analysis taking both follow-ups into account simultaneously, and similar analyses of the other secondary outcome measures, the BDI score, the SF-36 score and the MISS score. As outlined in the analysis plan (see Chapter 2), the analyses were performed according to intention-to-treat principles (analysing all available data in the groups as randomised independent of the treatment that patients actually received), although some very preliminary results from ‘compliers only’ and ‘blinded only’ are also reported. Interactions between severity group and treatment arm were tested in the models, which included the baseline value of the outcome variable, to adjust for initial severity, recruitment centre and GP as a clustering effect. Treatment effects were also estimated (based on models including treatment × severity interaction terms) for typical members of each subgroup at baseline, e.g. a patient with baseline HDRS 13.5 compared with one whose baseline HDRS was 17.5.
The initial models included only those patients for whom we had complete follow-up. In addition, as there were missing data at follow-up, additional models including covariates significantly associated with having values for the outcomes missing at follow-up (missing status) were fitted. This approach is consistent with the guidance given on www.lshtm.ac.uk/msu/missingdata/guidelines.pdf. Its validity depends on the missing at random (MAR) assumption, i.e. missing status depends only on observed variables). The severity levels at the preceding time point (baseline for 12 weeks and 12 weeks for 26 weeks) were examined first, and then other potential missing value predictors were identified using logistic regression with missing status as the dependent variable, and recruitment centre and other potential missingness predictors as independent variables. A backward selection procedure was employed using p = 0.1 as the significance cut-off for rejecting variables, but always including the recruitment centre. Variables were re-entered into the final model one by one. The missingness predictors were analysed for both the 12-week and 26-week follow-up points and were found to be the same for both.
Although the 12-week HDRS score was the declared primary outcome, the statistically optimal analysis is that based on the longitudinal model, including both follow-up points and taking account of missing value predictors. This is because it makes use of all available data and therefore produces the most precise estimates, and because it takes account of any potential bias due to missing values, as far as possible given the available data. An analysis of potential predictors of outcome was also performed for the HDRS outcome over both follow-up points, including the prespecified potential predictors (listed in Chapters 1 and 2). A similar selection strategy to that described above was employed for the missingness predictors. Interactions between treatment arm and each potential predictor were also tested in these models, to determine whether they predicted response to SSRI treatment. Logistic models for remission to a value of below 8 on the HDRS and to below 50% of the initial HDRS level were also fitted.
Stata version 10 commands xtreg (mle) and xtmixed for continuous outcomes, and xtlogit and xtmelogit for binary outcomes were used.
Descriptive data
As described above, a total of 602 patients were referred into the study by 177 GPs from 115 practices. Of these, 172 (29%) were excluded and 210 (35%) declined to participate, so 220 patients were randomised: 112 to SSRI plus supportive care and 108 to supportive care alone. In the sample analysed at follow-up, there were 186 patients from 103 GPs (average 1.8 patients per GP, range 1–8) at 12 weeks and 167 patients from 96 GPs (average 1.7 patients per GP, range 1–7) at 26 weeks. For the primary outcome (HDRS), 162 patients had both 12- and 26-week data; 29 had neither follow-up, 24 had only the 12-week follow-up; and five had only the 26-week follow-up. Intraclass correlations by GP (after controlling for arm, centre and baseline value) were 0 and 0.012 at 12 and 26 weeks respectively.
Patient characteristics at baseline
Table 20 shows baseline characteristics of the randomised patients. The two arms were well balanced with the exception that the proportions of single people and those with a severe interpersonal difficulty were somewhat higher in the supportive care alone arm. Baseline HDRS, SF-36 and BSI scores were very similar. The BDI score was slightly higher in the supportive care alone arm.
| Supportive care alone (n = 108) | SSRI plus supportive care (n = 112) | |
|---|---|---|
| Age at randomisation | ||
| Mean (range) | 41.3 (19–83) | 38.6 (18–75) |
| [n (%)] | [n (%)] | |
| Mediana | 38.9 | 37.4 |
| Age 18–30 | 32 (30) | 37 (33) |
| Age 31–64 | 67 (62) | 70 (63) |
| Age 65 and over | 8 (7) | 5 (4) |
| Male gender | 36 (33) | 31 (28) |
| White ethnicity | 96 (89) | 99 (88) |
| Previous antidepressant treatmentb | 56 (46) | 49 (44) |
| Previous depressionc | ||
| None | 40 (37) | 41 (37) |
| Once | 42 (39) | 38 (34) |
| Twice or more | 25 (23) | 32 (29) |
| Severity subgroup | ||
| Mild (HDRS 12–15) | 51 (47) | 52 (46) |
| Moderate (HDRS 16–20) | 57 (53) | 60 (54) |
| Centre | ||
| Southampton | 58 (54) | 61 (54) |
| London | 25 (23) | 26 (23) |
| Liverpool | 25 (23) | 25 (22) |
| Marital status | ||
| Married/cohabiting | 56 (52) | 63 (56) |
| Widowed/separated/divorced | 32 (30) | 11 (10) |
| Single | 20 (19) | 37 (33) |
| Accommodation | ||
| Owner-occupied | 50 (46) | 47 (42) |
| Housing association | 23 (21) | 26 (23) |
| Private rental | 22 (20) | 20 (18) |
| Job related | 2 (2) | 1 (1) |
| Parents | 8 (7) | 8 (7) |
| Other | 3 (3) | 10 (9) |
| Occupationd | ||
| Employed | 64 (59) | 76 (68) |
| Unemployed | 44 (41) | 36 (32) |
| Provoking agent in year before baseline (yes) | 82 (76) | 78 (70) |
| Ongoing severe interpersonal difficulty at baseline (yes) | 44 (41) | 33 (29) |
| Mean (SD) | Mean (SD) | |
| BSI score | 18.98 (8.51) | 19.69 (7.24) |
| BDI scoree | 24.31 (7.42) | 22.57 (6.71) |
| HDRS score | 15.68 (2.46) | 15.45 (2.09) |
Changes in the study outcome measures between baseline and follow-up
Table 21 shows the mean scores (and SDs) found for the primary and secondary outcome measures at baseline and follow-up. This demonstrates a fall at both follow-up points in HDRS and BDI score, and increases at both time points in the subscales of the SF-36, particularly the vitality (VT) and mental health (MH) subscales, in both arms of the trial. It also shows slightly greater patient satisfaction scores at both follow-up points in the SSRI plus supportive care arm, although the score in the SSRI plus supportive care arm at 26 weeks is slightly lower than at 12 weeks.
| Outcome measures | Baseline [mean (SD)] | 12-week follow-up [mean (SD)] | 26-week follow-up [mean (SD)] | |||
|---|---|---|---|---|---|---|
| Supportive care alone | SSRI plus supportive care | Supportive care alone | SSRI plus supportive care | Supportive care alone | SSRI plus supportive care | |
| HDRSa | 15.68 (2.46) | 15.45 (2.09) | 11.22 (5.78) | 8.73 (5.20) | 9.73 (5.57) | 7.92 (5.67) |
| BDIa | 24.48 (7.57) | 22.40 (6.74) | 15.15 (9.62) | 12.99 (8.51) | 13.27 (9.14) | 11.05 (8.20) |
| SF-36 scalesb | ||||||
| Physical functioning (PF) | 70.48 (25.63) | 73.93 (25.95) | 73.93 (26.79) | 77.62 (24.95) | 75.52 (28.79) | 77.96 (25.25) |
| Role – physical (RP) | 43.69 (39.17) | 43.99 (38.14) | 57.10 (41.69) | 56.45 (43.13) | 65.33 (40.46) | 60.23 (41.63) |
| Bodily pain (BP) | 52.15 (22.66) | 58.24 (22.35) | 60.18 (26.13) | 67.23 (24.99) | 63.29 (26.24) | 70.07 (27.83) |
| General health (GH) | 47.48 (19.43) | 49.75 (20.05) | 53.52 (22.66) | 57.25 (22.93) | 61.31 (20.17) | 60.16 (24.11) |
| Vitality (VT) | 27.90 (16.68) | 27.81 (17.58) | 41.63 (23.86) | 47.34 (23.55) | 45.22 (24.78) | 51.27 (23.67) |
| Social functioning (SF) | 43.75 (18.99) | 45.54 (22.19) | 60.25 (25.04) | 64.63 (26.29) | 67.93 (27.49) | 70.79 (25.90) |
| Role – emotional (RE) | 19.18 (29.80) | 16.97 (25.92) | 41.38 (43.42) | 52.51 (41.77) | 57.21 (42.92) | 58.71 (41.67) |
| Mental health (MH) | 38.65 (14.55) | 38.84 (13.97) | 54.43 (21.19) | 61.91 (19.99) | 59.79 (19.94) | 63.13 (19.53) |
| MISSb | _ | _ | 148.48 (25.29) | 157.12 (26.14) | 149.88 (25.19) | 154.88 (27.95) |
Missing values at follow-up
In comparison with the number of patients completing the HDRS at baseline, at the 12-week follow-up there were 18 missing values for the HDRS in the supportive care alone arm and 16 in the SSRI plus supportive care arm, due to incomplete follow-up of patients. At 26 weeks, there were 31 missing values for the HDRS in the supportive care alone arm and 22 in the SSRI plus supportive care arm. Those missing HDRS scores at 12 weeks were very little different at baseline than those for whom scores were available (means 15.12 versus 15.64 respectively, p = 0.214) and, similarly, those missing 26-week scores (but who had 12-week scores) were no more or less severe at the 12-week stage than those not lost to follow-up (means 9.62 versus 9.98, p = 0.773).
For the BDI, the numbers of missing values at 12 weeks were 19 and 16 for the two arms respectively, and at 26 weeks, 32 and 24 respectively. For the SF-36, the corresponding figures for the two arms were 3 and 2 at baseline, 22 and 21 at 12 weeks, and 36 and 27 at 26 weeks respectively. For the MISS, the corresponding figures for the two arms were 19 and 18 at 12 weeks, and 34 and 23 at 26 weeks respectively. The baseline values for patients missing at 12 and 26 weeks are shown in Table 22. Baseline patient characteristics, including age, gender, ethnicity, previous depression, previous antidepressant treatment, marital status, accommodation status, employment status, HDRS score, BDI score and BSI score, were examined to determine whether they predicted missing status at 12 and/or 26 weeks.
Younger age at randomisation, recruitment through the London centre and lack of employment were found to be significantly associated with patients being missing at follow-up, for both the 12- and 26-week follow-up points. Age at randomisation, centre, and employment status were therefore included in the analyses of covariance and longitudinal models described below.
| Follow-up point | Supportive care alone | SSRI plus supportive care | ||
|---|---|---|---|---|
| 12 weeks | 26 weeks | 12 weeks | 26 weeks | |
| [n (%)]a | [n (%)]a | [n (%)]a | [n (%)]a | |
| Age at randomisation | ||||
| Mean (range) | 40.6 (19–81) | 37.56 (19–81) | 27.9 (19–43) | 31.23 (19–47) |
| Median | 40.7 | 33.8 | 25.3 | 30.7 |
| 18–30 | 4 (4) | 12 (11) | 11 (10) | 11 (10) |
| 31–64 | 13 (12) | 18 (17) | 5 (5) | 11 (10) |
| 65 and over | 1 (1) | 1 (1) | 0 (0) | 0 (0) |
| Male gender | 6 (6) | 8 (7) | 4 (4) | 7 (6) |
| White ethnicity | 15 (14) | 26 (23) | 13 (12) | 18 (16) |
| Previous antidepressant treatment | 7 (6) | 16 (14) | 7 (6) | 9 (8) |
| Previous depression | ||||
| None | 8 (7) | 10 (9) | 4 (4) | 9 (8) |
| Once | 7 (6) | 12 (11) | 7 (6) | 7 (6) |
| Twice or more | 3 (3) | 9 (8) | 5 (4) | 6 (5) |
| Severity subgroup | ||||
| Mild (HDRS 12–15) | 9 (8) | 16 (14) | 9 (8) | 11 (10) |
| Moderate (HDRS 16–19) | 9 (8) | 15 (14) | 7 (6) | 11 (10) |
| Centre | ||||
| Southampton | 7 (6) | 14 (13) | 7 (6) | 7 (6) |
| London | 6 (6) | 11 (10) | 6 (5) | 11(10) |
| Liverpool | 5 (5) | 6 (5) | 3 (3) | 4 (4) |
| Marital status | ||||
| Married/cohabiting | 5 (5) | 13 (12) | 9 (8) | 11 (10) |
| Widowed/separated/divorced | 9 (8) | 10 (9) | – | 1 (1) |
| Single | 4 (4) | 8 (7) | 7 (6) | 10 (9) |
| Accommodation status | ||||
| Owner/occupied | 4 (4) | 8 (7) | 2 (2) | 6 (5) |
| Housing association | 7 (6) | 11 (10) | 3 (3) | 7 (6) |
| Private rental | 2 (2) | 6 (5) | 5 (4) | 4 (4) |
| Job related | 1 (1) | 1 (1) | 0 | – |
| Parents | 2 (2) | 3 (3) | 4 (4) | 4 (4) |
| Other | 2 (2) | 2 (2) | 2 (2) | 1 (1) |
| Occupation | ||||
| Employed | 11 (10) | 16 (14) | 9 (8) | 12 (11) |
| Unemployed | 6 (6) | 13 (12) | 7 (6) | 10 (9) |
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | |
| Baseline HDRS score | 15.28 (2.82) | 15.65 (2.55) | 14.94 (2.11) | 15.27 (2.08) |
| 12-week HDRS score | _ | 12.00 (7.45) | _ | 5.67 (5.10) |
| Baseline BDI score | 25.33 (7.16) | 25.27 (8.30) | 24.69 (5.15) | 22.59 (8.00) |
| Baseline BSI score | 15.78 (8.29) | 19.50 (8.87) | 22.78 (8.76) | 21.27 (7.51) |
Primary outcome
HDRS scores at 12 weeks
Table 23 and Figure 4 show the baseline and 12-week HDRS scores by treatment arm and severity subgroup. It can be seen that the mean HDRS score fell on average in all four groups, but that in each of the two severity subgroups the fall was greater in the SSRI plus supportive care arm.
| Severity subgroup | Supportive care alone | SSRI plus supportive care | |||
|---|---|---|---|---|---|
| Number of missing values | Mean (SD) | Number of missing values | Mean (SD) | ||
| HDRS at baseline | Mild (12–15) | – | 13.34 (1.12) | – | 13.54 (1.11) |
| Moderate (16–19) | – | 17.71 (1.15) | – | 17.10 (1.01) | |
| Overall | – | 15.68 (2.46) | – | 15.45 (2.09) | |
| HDRS at 12-weeks | Mild (12–15) | 9 | 9.15 (4.95) | 9 | 7.30 (5.05) |
| Moderate (16–19) | 9 | 12.96 (5.90) | 7 | 9.89 (5.07) | |
| Overall | 18 | 11.22 (5.78) | 16 | 8.73 (5.2) | |
| HDRS change from baseline | Mild (12–15) | 9 | 4.32 (4.79) | 9 | 6.28 (5.08) |
| Moderate (16–19) | 9 | 4.73 (5.67) | 7 | 7.25 (4.78) | |
| Overall | 18 | 4.54 (5.26) | 16 | 6.81 (4.91) | |
FIGURE 4.
Mean values for HDRS scores by treatment arm and severity subgroup (bars around mean values are standard errors).
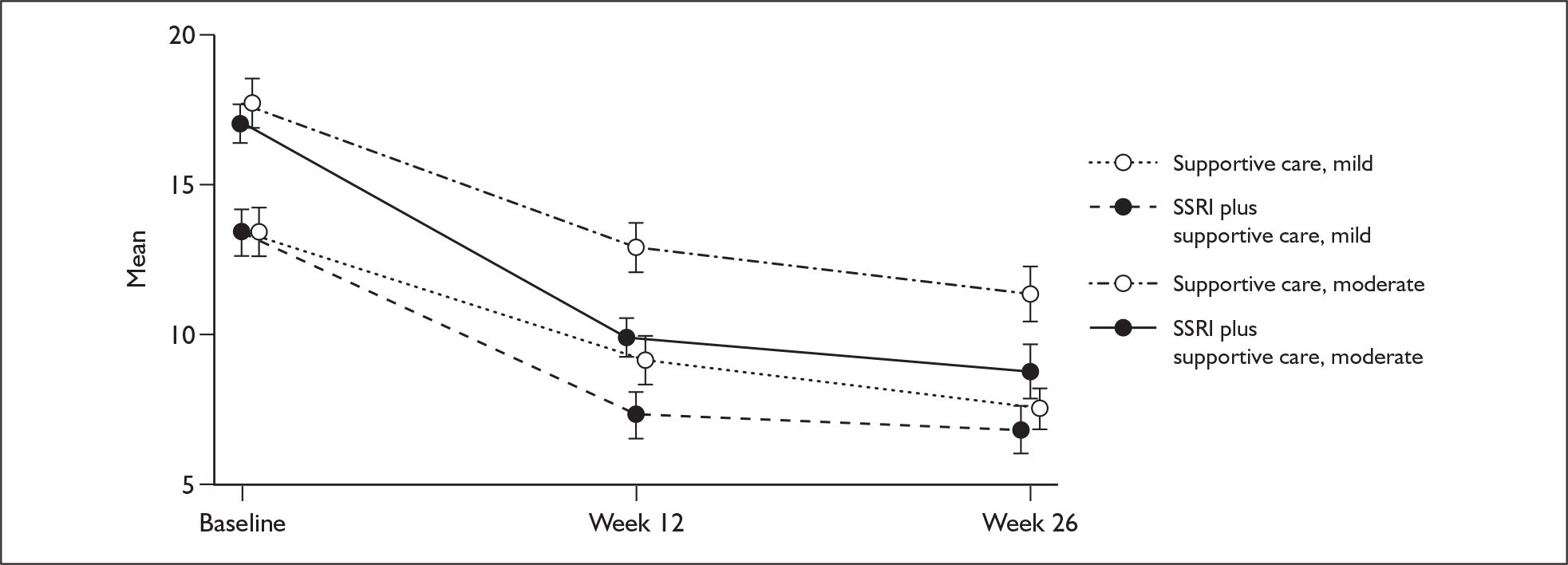
Figure 4 expresses graphically the results shown in Table 23, showing that the difference between trial arms persisted for both subgroups, although attenuated slightly, at the 26-week follow-up.
The box plots in Figure 5 show the variability in the HDRS scores at both follow-up points. The relatively low variability at baseline resulted from the specified inclusion criterion of an HDRS score of 12–19. The plots show that, in terms of their HDRS scores, most patients were better at follow-up but the variability in scores increased and some patients had worse scores at follow-up.
FIGURE 5.
Box plots of HDRS scores at each time point for the two trial arms.
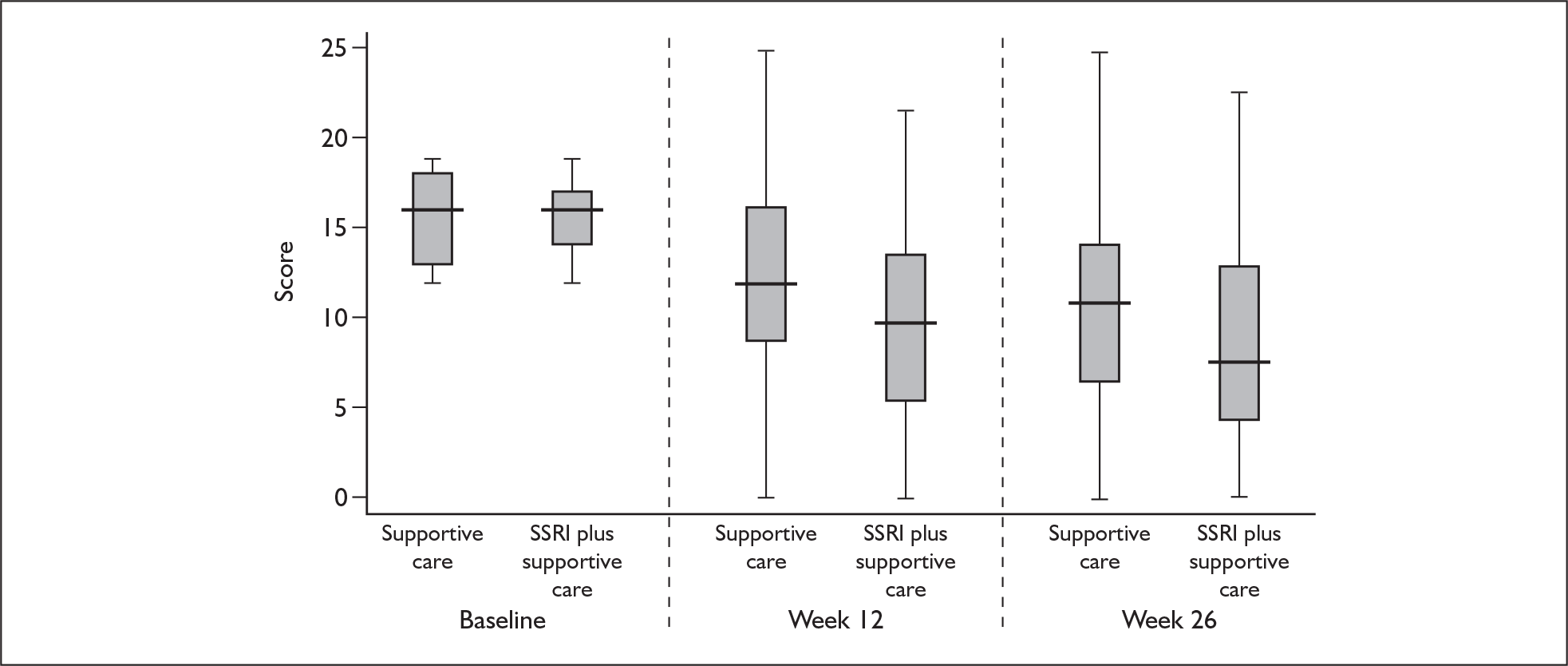
Numbers of patients achieving remission or significant improvement on the HDRS
Table 24 shows the numbers of patients achieving remission (a reduction to an HDRS score of less than 8) and the numbers achieving clinically important improvement (a 50% reduction in HDRS score from the baseline value) at the 12- and 26-week follow-up points.
| 12 weeks | 26 weeks | ||||
|---|---|---|---|---|---|
| Remission to < 8 [n (%)] | Reduction by 50% [n (%)] | Remission to < 8 [n (%)] | Reduction by 50% [n (%)] | ||
| Total sample | Supportive care alone | 22 (24) | 26 (29) | 28 (36) | 28 (36) |
| SSRI plus supportive care | 40 (42) | 42 (44) | 49 (54) | 53 (59) | |
| Mild subgroup (HDRS 12–15) | Supportive care alone | 15 (37) | 14 (34) | 16 (47) | 14 (41) |
| SSRI plus supportive care | 21 (49) | 20 (47) | 24 (59) | 23 (56) | |
| Moderate subgroup (HDRS 16–19) | Supportive care alone | 7 (14) | 12 (24) | 12 (28) | 14 (33) |
| SSRI plus supportive care | 19 (36) | 22 (42) | 25 (51) | 30 (61) | |
At 12 weeks, 22 patients in the supportive care alone arm (24.4% of those followed up) had HDRS scores below 8, compared with 40 (41.7%) in the SSRI plus supportive care arm. The absolute risk reduction (ARR) was therefore 17.2% and the number needed to treat (NNT) to achieve one remission at 12 weeks was 6 (95% CI 4 to 26). At 26 weeks, the corresponding numbers in remission were 28 (36.4%) and 49 (54.4%) respectively, so the ARR was 18.1% and the NNT to achieve one remission at 26 weeks was also 6 (95% CI 3 to 31). At 12 weeks, 26 patients (28.9%) in the supportive care alone arm had a 50% or greater fall in HDRS score from baseline, compared with 42 (43.8%) in the SSRI plus supportive care arm. The ARR was therefore 14.9% and the NNT to achieve improvement in one patient at 12 weeks was 7 (95% CI 4 to 83). At 26 weeks, the corresponding rates of improvement were 28 (36.4%) and 53 (58.9%) respectively, so the ARR was 22.5% and the NNT to achieve improvement in one patient was 5 (95% CI 3 to 13).
Regression analyses for HDRS scores
Table 25 shows the results of the analysis of covariance for the primary outcome, the HDRS score at 12 weeks, including treatment arm, HDRS baseline score and recruitment centre, with the patient’s GP fitted as a random effect. Treatment arm coefficients are for intervention versus control.
| Variable | Coefficient | 95% CI | p-value |
|---|---|---|---|
| Treatment arm | –2.293 | –3.741 to –0.845 | 0.002 |
| Baseline HDRS score | 0.874 | 0.544 to 1.204 | < 0.001 |
| London vs Southampton | 1.211 | –0.658 to 3.080 | 0.204 |
| Liverpool vs Southampton | 1.287 | –0.524 to 3.098 | 0.164 |
This shows a statistically significant difference between the treatment arms in HDRS depression scores after 12 weeks, after adjustment for baseline HDRS score, recruitment centre and clustering by GP. It also shows that baseline HDRS score was a statistically significant independent predictor of 12-week HDRS score. The differences between the arms for the two severity groups when analysed separately were –1.919 (95% CI –3.962 to 0.124) and –2.149 (95% CI –4.229 to –0.069) for the mild and moderate subgroups respectively. The interaction term (difference in treatment effect) for a 4-point increase in baseline severity was 1.10 (95% CI –3.73 to 1.54, p = 0.414) and the significance of the interaction with baseline severity as a continuous variable was p = 0.773, i.e. there was no evidence for a differential effect between the severity subgroups with respect to the differences between arms in HDRS scores.
Table 26 shows that the statistically significant differences in HDRS depression scores at 12 weeks between treatment arms remained after adjustment for the missingness predictors of age and employment status, along with baseline HDRS score, recruitment centre and GP. Once again, the interaction between arm and severity subgroup was not significant (p = 0.667).
| Variable | Coefficient | 95% CI | p-value |
|---|---|---|---|
| Treatment arm | –2.091 | –3.544 to –0.638 | 0.005 |
| Baseline HDRS score | 0.858 | 0.520 to 1.196 | < 0.001 |
| London vs Southampton | 0.939 | –0.935 to 2.814 | 0.326 |
| Liverpool vs Southampton | 1.018 | –0.815 to 2.851 | 0.276 |
| Age at randomisation | 0.001 | –0.051 to 0.054 | 0.962 |
| Employment status (unemployed vs employed) | 1.563 | 0.013 to 3.113 | 0.048 |
Table 27 shows the baseline and 26-week HDRS scores by treatment arm and severity subgroup. Table 28 shows the results of the analysis of covariance for the HDRS score at 26 weeks, including treatment arm, HDRS baseline score and recruitment centre, with the patient’s GP fitted as a random effect.
| Severity subgroup | Supportive care alonew | SSRI plus supportive care | |||
|---|---|---|---|---|---|
| Number of missing values | Mean (SD) | Number of missing values | Mean (SD) | ||
| HDRS at baseline | Mild (12–15) | – | 13.34 (1.12) | – | 13.54 (1.11) |
| Moderate (16–19) | – | 17.71 (1.15) | – | 17.12 (1.04) | |
| Overall | – | 15.68 (2.46) | – | 15.45 (2.09) | |
| HDRS at 26 weeks | Mild (12–15) | 16 | 7.56 (4.01) | 11 | 6.83 (5.02) |
| Moderate (16–19) | 15 | 11.44 (6.06) | 11 | 8.84 (6.05) | |
| Overall | 31 | 9.73 (5.57) | 22 | 7.92 (5.67) | |
| HDRS change from baseline | Mild (12–15) | 16 | 5.71 (4.29) | 11 | 6.73 (5.22) |
| Moderate (16–19) | 15 | 6.19 (5.97) | 11 | 8.27 (5.92) | |
| Overall | 31 | 5.97 (5.27) | 22 | 7.57 (5.64) | |
Table 28 shows that the difference between the treatment arms in changes in the HDRS depression scores after 26 weeks was of borderline statistical significance in this analysis, after adjustment for the other variables. The interaction term, for a 4-point increase in baseline severity, was –1.54 (95% CI –4.18 to 1.35, p = 0.297) and the significance of the interaction with baseline severity as a continuous variable was p = 0.283, indicating that there was no evidence for a differential effect between the severity subgroups with respect to the changes in HDRS scores.
| Variable | Coefficient | 95% CI | p-value |
|---|---|---|---|
| Treatment arm | –1.688 | –3.326 to –0.049 | 0.043 |
| Baseline HDRS score | 0.606 | 0.238 to 0.974 | 0.001 |
| London vs Southampton | 1.157 | –1.273 to 3.587 | 0.351 |
| Liverpool vs Southampton | 0.651 | –1.465 to 2.766 | 0.547 |
The additional missingness predictors (age at randomisation and employment status) were included in the results shown in Table 29. Again, the difference between the treatment arms in changes in HDRS depression scores after 26 weeks was of borderline statistical significance after adjustment for the missingness predictors of age and employment status, along with the baseline HDRS score, recruitment centre and referring GP. The interaction between arm and severity subgroup was not significant (p = 0.181).
| Variable | Coefficient | 95% CI | p-value |
|---|---|---|---|
| Treatment arm | –1.336 | –2.951 to 0.278 | 0.105 |
| Baseline HDRS score | 0.620 | 0.251 to 0.990 | 0.001 |
| London vs Southampton | 0.839 | –1.486 to 3.165 | 0.479 |
| Liverpool vs Southampton | 0.110 | –1.958 to 2.179 | 0.917 |
| Age at randomisation | 0.024 | –0.033 to 0.081 | 0.413 |
| Employment status (unemployed vs employed) | 2.594 | 0.865 to 4.322 | 0.003 |
Longitudinal analysis of HDRS scores at 12 and 26 weeks
Maximum likelihood mixed-effects models were used for the longitudinal analyses, with GP and subject as random effects, and time as a covariate, coded as 1 for 12 weeks and 2 for 26 weeks. The ‘time’ coefficient, therefore, represents the drop in score over 14 weeks, averaged over both treatment arms. Tables 30 and 31 show the results of the longitudinal analysis of HDRS scores at 12 and 26 weeks, excluding and including factors associated with missing status at either time point. Interaction between treatment arm and time was also included in the longitudinal models to test for any evidence for a drop-off or increase in effect over time. Although there was an overall reduction in HDRS scores over time, there was no evidence for a time × treatment interaction (p = 0.574). Severity by arm interaction was assessed using the baseline HDRS score as a continuous variable and, as with the separate time point analyses presented above, was found not to be significant (p = 0.219).
| Variable | Coefficient | 95% CI | p-value |
|---|---|---|---|
| Treatment arm | –2.145 | –3.516 to –0.774 | 0.002 |
| Baseline HDRS score | 0.760 | 0.449 to 1.072 | < 0.001 |
| London vs Southampton | 1.115 | –0.668 to 2.899 | 0.220 |
| Liverpool vs Southampton | 0.878 | –0.839 to 2.594 | 0.316 |
| Time | –1.129 | –1.794 to –0.464 | 0.001 |
| Variable | Coefficient | 95% CI | p-value |
|---|---|---|---|
| Treatment arm | –1.866 | –3.224 to –0.508 | 0.007 |
| Baseline HDRS score | 0.754 | 0.440 to 1.068 | < 0.001 |
| London vs Southampton | 0.785 | –0.980 to 2.549 | 0.383 |
| Liverpool vs Southampton | 0.471 | –1.246 to 2.188 | 0.591 |
| Time | –1.126 | –1.795 to –0.457 | 0.001 |
| Age at randomisation | 0.014 | –0.034 to 0.063 | 0.562 |
| Employment status (unemployed vs employed) | –2.172 | –3.621 to –0.722 | 0.003 |
The model shown in Table 31 includes the variables which were found to predict missingness. These analyses show that there is a highly significant effect of treatment arm over time when the outcomes at both 12 and 26 weeks are included. Once again, the severity by arm interaction was assessed and found not to be significant (p = 0.378). This time × treatment interaction was also tested using the baseline HDRS score as a continuous variable and was found not to be significant (p = 0.239).
Once again, HDRS scores at follow-up are significantly associated with baseline HDRS scores. In addition, employment status is a highly significant predictor of outcome, and the coefficient shows that the effect size is very similar to that of treatment status (with higher scores at follow-up among patients who were unemployed at baseline).
The results from Table 31 are also illustrated in Figure 6, which gives predicted HDRS over time by treatment arm, adjusting for the other variables in the model. For illustration, the reference baseline HDRS score has been set at 15.6, centre to Southampton, age to 40 and employment status to being currently employed.
FIGURE 6.
Estimated mean difference in HDRS scores between treatment arms (longitudinal analysis of HDRS scores at 12 and 26 weeks, including missingness predictors). Bars around estimates give the standard errors. See Table 31 for model.
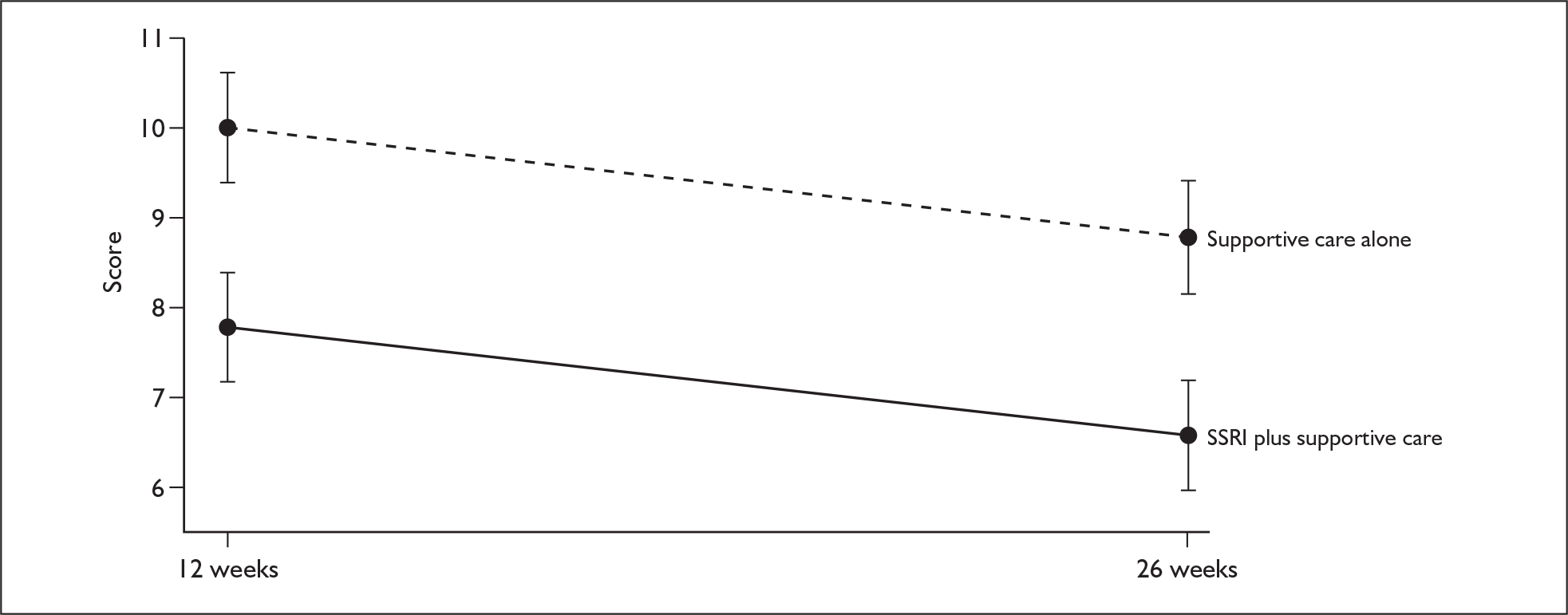
Secondary outcomes
BDI scores
Table 32 shows the longitudinal analysis of BDI scores at 12 and 26 weeks. Table 33 includes the variables that were found to predict missingness. These analyses show that the difference between the two treatment arms in depression scores on the BDI over time was not statistically significant, unlike that for the HDRS scores. Higher BDI scores at follow-up were predicted by higher baseline BDI scores, and were also strongly related to being unemployed at baseline. The test for interaction between arm and severity was not significant.
| Variable | Coefficient | 95% CI | p-value |
|---|---|---|---|
| Treatment arm | –1.510 | –3.692 to 0.671 | 0.175 |
| Baseline BDI score | 0.532 | 0.373 to 0.691 | < 0.001 |
| London vs Southampton | 2.151 | –0.637 to 4.939 | 0.130 |
| Liverpool vs Southampton | 0.768 | –1.921 to 3.458 | 0.576 |
| Time | –1.715 | –2.680 to –0.749 | < 0.001 |
| Variable | Coefficient | 95% CI | p-value |
|---|---|---|---|
| Treatment arm | –1.038 | –3.184 to 1.109 | 0.343 |
| Baseline BDI score | 0.534 | 0.378 to 0.691 | < 0.001 |
| London vs Southampton | 1.742 | –1.008 to 4.492 | 0.214 |
| Liverpool vs Southampton | 0.040 | –2.629 to 2.709 | 0.977 |
| Time | –1.714 | –2.684 to –0.745 | 0.001 |
| Age at randomisation | 0.069 | –0.007 to 0.145 | 0.076 |
| Employment status (unemployed vs employed) | –3.351 | –5.633 to –1.069 | 0.004 |
SF-36 scores
Statistically significant differences between the two treatment arms were found for the MH and VT subscales of the SF-36. No statistically significant differences were found for the remaining subscales. The actual values for all the subscales at baseline and follow-up are shown in Table 21, together with their SDs.
Mental health
Table 34 shows the longitudinal analysis of the MH subscale scores at 12 and 26 weeks. Table 35 includes the variables that were found to predict missingness. These analyses show that differences between arms in MH scores were statistically significant after adjustment for the other variables in the model. Lower MH scores at follow-up were also predicted by lower baseline MH scores, and once again were strongly related to being unemployed at baseline.
| Variable | Coefficient | 95% CI | p-value |
|---|---|---|---|
| Treatment arm | 6.125 | 1.064 to 11.187 | 0.018 |
| Baseline MH score | 0.298 | 0.124 to 0.472 | 0.001 |
| London vs Southampton | –6.822 | –13.356 to –0.289 | 0.041 |
| Liverpool vs Southampton | 0.402 | –5.879 to 6.685 | 0.900 |
| Time | 2.810 | 0.178 to 5.442 | 0.036 |
| Variable | Coefficient | 95% CI | p-value |
|---|---|---|---|
| Treatment arm | 5.049 | 0.038 to 10.060 | 0.048 |
| Baseline MH score | 0.294 | 0.121 to 0.468 | 0.001 |
| London vs Southampton | –5.992 | –12.500 to 0.516 | 0.071 |
| Liverpool vs Southampton | 2.163 | –4.109 to 8.435 | 0.499 |
| Time | 2.873 | 0.228 to 5.517 | 0.033 |
| Age at randomisation | –0.111 | –0.290 to 0.691 | 0.228 |
| Employment status unemployed vs employed) | 6.335 | 0.958 to 11.711 | 0.021 |
Vitality
Table 36 shows the longitudinal analysis of the VT subscale scores at 12 and 26 weeks. The analysis in Table 37 also includes the variables that were found to predict missingness. These analyses show that differences between arms in the VT scores were statistically significant after adjustment for baseline VT score, centre and GP (Table 36). The relationship was found to be slightly weaker after adjustment for the variables that predicted missingness (Table 37), and no longer quite statistically significant at the 5% level. In addition, Table 37 shows that lower VT scores at follow-up were predicted by lower baseline VT scores and by being older at baseline.
| Variable | Coefficient | 95% CI | p-value |
|---|---|---|---|
| Treatment arm | 6.465 | 0.622 to 12.307 | 0.030 |
| Baseline VT score | 0.457 | 0.281 to 0.633 | < 0.001 |
| London vs Southampton | –5.631 | –13.275 to 2.013 | 0.149 |
| Liverpool vs Southampton | –1.450 | –8.700 to 5.800 | 0.695 |
| Time | 3.309 | 0.270 to 6.347 | 0.033 |
| Variable | Coefficient | 95% CI | p-value |
|---|---|---|---|
| Treatment arm | 5.186 | 0.558 to 10.930 | 0.077 |
| Baseline VT score | 0.435 | 0.263 to 0.608 | < 0.001 |
| London vs Southampton | –5.045 | –12.616 to 2.526 | 0.192 |
| Liverpool vs Southampton | 0.608 | –6.582 to 5.780 | 0.868 |
| Time | 3.337 | 0.280 to 6.394 | 0.032 |
| Age at randomisation | –0.259 | –0.462 to –0.056 | 0.012 |
| Employment status (unemployed vs employed) | 6.383 | 0.195 to 12.570 | 0.043 |
Patient satisfaction
Table 38 shows the longitudinal analysis of the MISS scores at 12 and 26 weeks, including baseline HDRS score (as baseline MISS scores were not available) and the variables that were found to predict missingness. This shows that satisfaction scores were significantly different between the treatment arms, with higher scores among patients in the SSRI plus supportive care arm. However, although the differences were statistically significant, they were not large differences in absolute magnitude (as shown in Table 21). None of the other factors in the model below were found to predict satisfaction.
| Variable | Coefficient | 95% CI | p-value |
|---|---|---|---|
| Treatment arm | 7.791 | 1.145 to 14.438 | 0.022 |
| Baseline HDRS score | –0.187 | –1.685 to 1.311 | 0.806 |
| London vs Southampton | –4.585 | –14.594 to 5.424 | 0.369 |
| Liverpool vs Southampton | 3.395 | –6.030 to 12.821 | 0.480 |
| Time | –1.522 | –4.400 to 1.356 | 0.300 |
| Age at randomisation | 0.169 | –0.073 to 0.411 | 0.172 |
| Employment status (unemployed vs employed) | –0.329 | –7.353 to 6.696 | 0.927 |
The MISS data will undergo factor analysis for comparison with the previous literature on the use of the scale, and further analyses will be presented in a subsequent publication.
Exploratory analysis of predictor variables
Predictors of outcome
An analysis of potential predictors of outcome was also performed for the HDRS score over both follow-up points, including the prespecified potential predictors (listed in Chapters 1 and 2). A similar selection strategy was employed, as described above, for the missingness predictors (backward selection using a criterion of p = 0.1, retaining centre, baseline score and GP). Interactions between treatment arm and each potential predictor were also tested in these models.
Tables 39 and 40 show the results of regression analyses, including the predictors listed in the analysis plan outlined in Chapter 2. The two analyses differed only in terms of which LEDS variable was included. Table 39 includes any provoking agent in the year before randomisation, whereas Table 40 includes any ongoing severe interpersonal difficulty at baseline.
| Variable | Coefficient | 95% CI | p-value |
|---|---|---|---|
| Treatment arm | –1.719 | –3.219 to –0.220 | 0.025 |
| Baseline HDRS score | 0.563 | 0.198 to 0.928 | 0.002 |
| London vs Southampton | 0.971 | –1.438 to 3.380 | 0.429 |
| Liverpool vs Southampton | 0.427 | –1.727 to 2.581 | 0.698 |
| Time | –0.993 | –1.751 to –0.236 | 0.010 |
| Age at randomisation | 0.010 | –0.058 to 0.079 | 0.771 |
| Employment status (unemployed vs employed) | 1.475 | –0.284 to 3.233 | 0.100 |
| Gender | –1.270 | –3.067 to 0.528 | 0.166 |
| Ethnicity – black vs white | 0.251 | –3.729 to 4.232 | 0.901 |
| Ethnicity – other vs white | 0.525 | –4.339 to 5.390 | 0.832 |
| Widowed/separated/divorced vs married/cohabiting | 0.067 | –2.002 to 2.137 | 0.949 |
| Single vs married/cohabiting | 1.426 | –0.459 to 3.310 | 0.138 |
| Duration of symptoms | 0.003 | –0.005 to 0.011 | 0.507 |
| Baseline BSI score | 0.185 | 0.081 to 0.290 | 0.001 |
| Perceived cause: physical vs other | 0.029 | –1.974 to 2.033 | 0.977 |
| Previous anti-depressant treatment (yes vs no) | 0.614 | –1.034 to 2.261 | 0.465 |
| Alcohol use (AUDIT score) | –0.004 | –0.242 to 0.234 | 0.972 |
| LEDS provoking agent in year before | 0.102 | –1.659 to 1.863 | 0.909 |
| Variable | Coefficient | 95% CI | p-value |
|---|---|---|---|
| Treatment arm | –1.584 | –3.071 to –0.067 | 0.037 |
| Baseline HDRS score | 0.571 | 0.210 to 0.931 | 0.002 |
| London vs Southampton | 0.728 | –1.712 to 3.168 | 0.559 |
| Liverpool vs Southampton | 0.250 | –1.923 to 2.423 | 0.822 |
| Time | –1.000 | –1.757 to –0.245 | 0.010 |
| Age at randomisation | 0.014 | –0.054 to 0.081 | 0.693 |
| Employment status (unemployed vs employed) | 1.429 | –0.310 to 3.169 | 0.107 |
| Gender | –1.152 | –2.954 to 0.650 | 0.210 |
| Ethnicity (black vs white) | 0.245 | –3.722 to 4.212 | 0.904 |
| Ethnicity (other vs white) | 0.253 | –4.542 to 5.049 | 0.918 |
| Widowed/separated/divorced vs married/cohabiting | –0.062 | –2.113 to 1.990 | 0.953 |
| Single vs married/cohabiting | 1.496 | –0.375 to 3.368 | 0.117 |
| Duration of symptoms | 0.004 | –0.005 to 0.012 | 0.386 |
| Baseline BSI score | 0.168 | 0.059 to 0.276 | 0.002 |
| Perceived cause: physical vs other | –0.281 | –2.304 to 1.741 | 0.785 |
| Previous anti-depressant treatment (yes vs no) | 0.474 | –1.167 to 2.115 | 0.572 |
| Alcohol use (AUDIT score) | –0.006 | –0.241 to 0.230 | 0.962 |
| LEDS severe interpersonal difficulty at baseline | 1.205 | –0.448 to 5.859 | 0.153 |
Interaction between age and gender was found to be not significant. As the number of predictors was large, those which were not significant at the level of p = 0.1 were removed in a backward selection procedure (keeping missingness predictors and centre, baseline level and GP as a clustering effect in the model). The results of the backward selection are presented in Table 41.
| Variable | Coefficient | 95% CI | p-value |
|---|---|---|---|
| Treatment arm | –1.907 | –3.226 to –0.589 | 0.005 |
| Baseline HDRS score | 0.549 | 0.226 to 0.872 | 0.001 |
| London vs Southampton | 1.134 | –0.654 to 2.922 | 0.214 |
| Liverpool vs Southampton | 0.903 | –0.822 to 2.627 | 0.305 |
| Time | –1.104 | –1.773 to –0.436 | 0.001 |
| Age at randomisation | 0.023 | –0.024 to 0.071 | 0.340 |
| Employment status (unemployed vs employed) | –1.940 | –3.349 to –0.531 | 0.007 |
| Baseline BSI score | 0.164 | 0.072 to 0.256 | < 0.001 |
Table 41 confirms that a better outcome, in terms of HDRS averaged scores over the 12- and 26-week follow-up points, is significantly related to being randomised to the SSRI plus supportive care arm, even after adjusting for the other potential predictors measured. In addition, a greater initial severity of depression, being unemployed and having more physical symptoms at baseline were significant predictors of a poorer outcome for depression. The interaction between treatment and time was not significant (p = 0.574).
No interactions between treatment arm and the other predictors included in the model above were found to be significant (p = 0.909 for the interaction between treatment arm and age, p = 0.499 for that between treatment arm and employment status, and p = 0.369 for that between treatment arm and baseline somatic symptom score). Thus, there was no evidence for a differential response to treatment with an SSRI in addition to supportive care for any of these predictors.
Predictors of remission
The overall odds ratio (OR) for remission to HDRS < 8 for intervention versus control, after controlling for centre, baseline level of HDRS, age and employment and clustering for GP, was 2.306 (95% CI 1.194 to 4.453, p = 0.013) at 12 weeks and 2.224 (95% CI 1.100 to 4.497, p = 0.026) at 26 weeks. The ORs for the mild and moderate subgroups were 1.591 and 3.492 at 12 weeks and 1.623 and 3.148 at 26 weeks. The interaction between arm and severity was not significant at either time point (p = 0.328 and p = 0.298 respectively). Logistic models were fitted for remission (HDRS < 8) at follow-up with the variables discussed above as potential predictors. Very similar results, in terms of which variables were predictive, were found.
Further predictor analysis including the effect of compliance and blindness
It is anticipated that a more detailed analysis of predictors will be reported in a subsequent publication. Preliminary results are as follows: compliers are defined as those who take at least 28 days of SSRI medication in the treatment group [63 (56%) in the intervention group] and those who take less than this amount or none in the control group [92 (85%)]. Comparing the HDRS totals by arm (using the same longitudinal model as for the intention-to-treat analysis reported above, i.e. controlling for baseline level, centre, age and employment) for the compliers subgroup gives an estimated effect in favour of SSRI treatment of –1.937 (95% CI –3.538 to –0.336, p = 0.018).
With regard to the unblinding of researchers, a longitudinal analysis of the interviewer-blinded and unblinded groups gives estimates of the differences between arms of –1.032 (95% CI –2.532 to 0.469, p = 0.178) for blinded cases and –4.757 (95% CI –7.342 to –2.171, p < 0.001) for unblinded cases. Further analysis, however, suggests that this does not reflect interviewer bias but rather a complex effect due to non-compliance. There are two reasons for this. First, a parallel analysis of the BDI total shows a similar difference between blinded and unblinded cases [blinded –0.841 (95% CI –3.253 to 1.571, p = 0.494); unblinded –2.866 (95% CI –6.821 to 1.090, p = 0.156)]. This finding for the BDI is not consistent with interviewer bias as an explanation as it is patient completed. For the SF-36 MH scale (also patient completed), the estimates are blinded 1.98 (95% CI –3.812 to 7.773, p = 0.503) and unblinded 16.86 (95% CI 8.613 to 25.10, p < 0.001). Second, compliance and blindness of researchers are linked: researchers tended to be unblinded more often than the average for those patients who had been prescribed antidepressants contrary to randomisation, i.e. non-compliers in the control group (61% of patients in this subgroup revealed their arm to researchers at 12 weeks compared with an average of 25% at 12 weeks).
Thus, this apparent association with ‘blindness’ is likely to reflect a more complex treatment and/or compliance effect to do with the patients, rather than the interviewer. Interpretation of treatment effects in the presence of non-compliance and any independent effect of randomisation itself (given that the patients are all unblinded) will depend on a causal model that can take account of all these factors simultaneously and, specifically, the initial level of severity, the dosage of medication actually received and other individual characteristics of compliers and non-compliers. This will be the subject of further analysis.
Process of care
Number of consultations
The aim was for patients in both arms to be seen by the treating GPs four times, at 2, 4, 8 and 12 weeks after randomisation, and the numbers of consultations reported by the patients on the CSRI questionnaire within the first 12 weeks were as follows: in the supportive care alone arm 100 patients (93%) reported subsequent consultations, with a mean of 3.8 (SD 2.0); in the SSRI plus supportive care arm 108 (96%) reported subsequent consultations, with a mean of 4.1 (SD 2.2).
Treatment with SSRIs
Data on the prescriptions for SSRIs given to participating patients were gathered from their medical records after the end of the 26-week follow-up period. Table 42 shows the number of tablets prescribed to patients.
| Number of tablets prescribed | Number of patients | |
|---|---|---|
| Supportive care alone [n (%)] | Supportive care plus SSRI [n (%)] | |
| 0 | 83 (76.9) | 15 (13.4) |
| 1–30 | 9 (8.3) | 24 (21.4) |
| 31–60 | 3 (2.8) | 9 (8.0) |
| 61–90 | 1 (0.9) | 5 (4.5) |
| 91–120 | 2 (1.9) | 10 (8.9) |
| 121–150 | 2 (1.9) | 12 (10.7) |
| 151–180 | 1 (0.9) | 6 (5.4) |
| > 180 | 7 (6.5) | 31 (27.7) |
| Total number of patients | 108 | 112 |
It is important to note that the numbers of tablets prescribed does not necessarily correspond exactly with the number of days of treatment given, as some SSRIs are given more frequently than once daily, some patients would have stopped treatment and restarted after a gap, and some of the prescriptions given towards the end of the 26 weeks would have been for periods continuing for some time beyond the follow-up period. More detailed analysis of the dates of prescriptions and length in days of each prescription for each individual patient is being carried out to determine the mean and range of length of SSRI treatment in days and will be reported in a subsequent publication. According to the CSRI data, the mean duration of SSRI treatment was 144 days, and two-thirds of participants prescribed SSRIs reported using them for the whole of the 26-week period. However, the medical record data are likely to be more accurate, as the patients were being asked to recall drug use over the previous 26 weeks. During the 12 weeks following randomisation, of those prescribed SSRIs (across both arms): citalopram was received by 20 (16.4%), escitalopram 11 (9.0%), fluoxetine 89 (73.0%), paroxetine 4 (3.3%) and sertraline 4 (3.3%). The distribution was similar for the following 3-month period: citalopram 14 (19.4%), escitalopram 8 (11.1%), fluoxetine 47 (65.3%), paroxetine 3 (4.2%) and sertraline 3 (4.2%). (These percentages do not sum to 100% due to some patients receiving more than one type of SSRI during the follow-up periods.)
Side effects of SSRI medication reported by the patients
At the 12-week follow-up, adverse effects of antidepressants were reported by 47 patients, of whom 37 who were randomised to the SSRI plus supportive care arm and 10 to the supportive care alone arm (patients in this arm could be prescribed antidepressants at the discretion of the GP if they were thought to be getting worse and in need of medication). All the antidepressants taken were SSRIs.
Table 43 shows the number and type of side effects reported by patients who took SSRIs during the first 12 weeks of the study in each arm, in descending order of frequency of occurrence in the SSRI plus supportive care arm. At the 26-week time point, 42 patients reported side effects, of whom 36 were randomised to the intervention arm and six to the control arm.
| Reported side effects of antidepressants taken at 12 weeks | Number of times reported by patients | |
|---|---|---|
| Supportive care alone | SSRI plus supportive care | |
| Gastrointestinal symptoms | 4 | 21 |
| Tiredness/drowsiness/reduced energy | 1 | 9 |
| Itching/irritation/tingling of skin/rash | 1 | 8 |
| Headache | 3 | 6 |
| Reduced libido | 0 | 5 |
| Anxiety/agitation/mood swings | 2 | 4 |
| Tremor/shaking | 1 | 4 |
| Spaced-out/distant/drunk feeling | 0 | 4 |
| Loss of appetite/weight loss | 2 | 3 |
| Flushing/sweating | 1 | 3 |
| Dry mouth | 0 | 3 |
| Dizziness | 0 | 3 |
| Reduced sleep | 1 | 2 |
| Feeling of carelessness | 1 | 1 |
| Increased appetite/weight gain | 0 | 1 |
| Lump in throat | 0 | 1 |
| Light sensitivity | 0 | 1 |
| Dreaming | 0 | 1 |
| Blackout (memory loss) with alcohol | 0 | 1 |
| Total | 17 | 81 |
Table 44 shows the number and type of side effects reported at 26 weeks by patients who took SSRIs in each arm.
| Reported side effects of antidepressants taken at 26 weeks | Number of times reported by patients | |
|---|---|---|
| Supportive care alone | SSRI plus supportive care | |
| Gastrointestinal symptoms | 4 | 19 |
| Flushing/sweating | 1 | 6 |
| Itching/irritation of skin/rash | 0 | 4 |
| Tiredness | 1 | 3 |
| Tremor/shaking | 0 | 3 |
| Dizziness | 0 | 3 |
| Poor concentration/forgetful | 0 | 3 |
| Cramps/painful limbs/muscle spasms | 0 | 3 |
| Loss of appetite/weight loss | 0 | 2 |
| Headache | 1 | 1 |
| Spaced-out feeling | 1 | 1 |
| Reduced sleep | 1 | 1 |
| Dreaming | 1 | 1 |
| Reduced libido | 0 | 1 |
| Dry mouth | 0 | 1 |
| Yawning | 0 | 1 |
| Flashing lights | 0 | 1 |
| Breathlessness | 0 | 1 |
| Feeling low | 0 | 1 |
| Anxiety | 1 | 0 |
| Total | 11 | 56 |
Adverse events reported by the participating GPs
A total of nine adverse events were reported by the GPs (see Appendix 23). They included four events thought to be adverse reactions to the SSRI medication and seven severe adverse events (two in the supportive care alone arm). There were no suspected unexpected severe adverse reactions.
Patient-reported consultation content
The 10-item PSAC questionnaire, measuring the number of reported consultation content items specific to depression, was completed by 183 of 186 patients followed up at 12 weeks (94 of 96 in the SSRI plus supportive care arm and 89 of 90 in the supportive care alone arm), and by 164 of 167 patients at 26 weeks (89 of 90 in the SSRI plus supportive care arm and 75 of 77 in the supportive care alone arm). The overall mean number of items reported was 8.04 (SD 4.4) and the observed values ranged from 0 to 20. The PSAC score did not differ significantly between the two arms of the study [mean score in SSRI plus supportive care arm 8.2 (SD 4.4) compared with 7.8 (4.5) in the supportive care alone arm, p = 0.52]. Thus there was no evidence of a substantial difference in depression-specific consultation content between the study arms. These data will be analysed further and may appear in a subsequent publication.
Chapter 5 Economic evaluation
The economic evaluation was a key component of the THREAD study and involved the following stages:
-
measurement of service use prior to baseline assessment and 26-week follow-up
-
calculation of service costs for each time period
-
comparison of service use and service costs between the two groups (supportive care alone and SSRI plus supportive care)
-
comparisons of cost-effectiveness and cost–utility
-
assessment of impact of interventions on informal care and lost employment.
Service use
Service use during the 6-month periods leading up to the baseline assessment and 26-week follow-up was measured with an adapted version of the CSRI. Services included those provided in the primary care setting (face-to-face GP consultations, GP telephone contacts, practice nurse contacts), secondary care services (inpatient, outpatient, day patient, accident and emergency), community health services (e.g. health visitors, district nurses, counselling or psychological therapists) and social care services (e.g. social workers, housing workers). The CSRI asked patients to state whether they had used specific services, how many contacts they had received and – where relevant – the average duration of service contact (i.e. across all contacts the individual made with each service). Informal care provided by family members and friends was recorded, by asking patients how much extra help (measured in hours per week) they had received specifically because of their health problems. This time was broken down into personal care, childcare, help in the home and help outside the home. The CSRI recorded use of medication for mental health and physical health reasons. The names of medications were recorded along with doses, frequency and duration of use. In addition to service use, the CSRI recorded employment status and interruptions to work as a result of health problems (absenteeism).
The CSRI was not applied at the 12-week follow-up because there were concerns that the information contained within it would ‘unblind’ the researchers conducting the HDRS interviews. Therefore, the CSRI used at 26 weeks was adapted to include questions on the number of service contacts that were received during the previous 3 months, so that the use up to 12 weeks from baseline could be identified as well as that in the 3 months before the 26-week follow-up.
Combining CSRI data and GP record data
CSRI data were augmented with data collected from general practice computerised medical records. These covered a range of services, and for the purposes of the economic evaluation data we used data on GP consultations (surgery, telephone or home visits), practice nurse contacts and prescriptions of mental health medications (specifically antidepressants, anxiolytics and hypnotics). This was the main data source for mental health problem prescribing, while information on drugs for physical health problems was taken from the CSRI. Regarding GP and practice nurse contacts, a comparison between the CSRI and medical record information was made and the source recording the highest level of contact was used (which would differ by patient).
Service use data are summarised in Table 45. In the 6 months before baseline assessment, all patients had GP contacts, which occurred approximately every 6 weeks on average. Slightly less than half also had contacts with practice nurses. More than half were receiving medication for physical health problems, and around one-third had outpatient contacts during the 6 months prior to baseline, which indicates a considerable level of physical health comorbidity in the trial population, as might be expected in a population selected on the basis of having somatic symptoms. A small number of patients (three in the supportive care alone group and one in the SSRI plus supportive care group) were prescribed SSRIs during the 6 months prior to baseline. However, records indicated that none of these four prescriptions was ‘cashed’. Most other services were used by relatively few patients. Overall, there were few noticeable differences between the two groups at baseline, although the group randomised to supportive care alone did have a higher rate of GP telephone contacts.
| Service | 6 months to baseline | Baseline to 12-week follow-up | Baseline to 26-week follow-up | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Supportive care alone | SSRI plus supportive care | Supportive care alone | SSRI plus supportive care | Supportive care alone | SSRI plus supportive care | |||||||
| n (%) | Mean (SD)a | n (%) | Mean (SD)a | n (%) | Mean (SD)a | n (%) | Mean (SD)a | n (%) | Mean (SD)a | n (%) | Mean (SD)a | |
| Inpatient admissionb | 9 (9) | 2.2 (2.2) | 6 (5) | 1.8 (1.3) | 2 (3) | 7.5 (9.2) | 3 (4) | 3.7 (3.1) | 2 (3) | 9.0 (7.1) | 5 (6) | 8.4 (11.8) |
| Outpatient consultation | 41 (39) | 2.9 (2.6) | 37 (33) | 2.4 (1.7) | 17 (23) | 2.1 (2.2) | 19 (22) | 1.8 (1.3) | 24 (32) | 2.7 (2.3) | 28 (33) | 2.3 (2.1) |
| Day patient admission | 3 (3) | 3.7 (3.8) | 2 (2) | 1.0 (0.0) | 1 (1) | 1.0 (–) | 1 (1) | 1.0 (–) | 1 (1) | 1.0 (–) | 1 (1) | 1.0 (–) |
| A&E consultation | 10 (9) | 1.4 (0.7) | 12 (11) | 1.2 (0.4) | 3 (4) | 3.0 (1.4) | 4 (5) | 1.8 (1.5) | 4 (5) | 3.3 (3.9) | 7 (8) | 3.4 (3.6) |
| GP surgery consultation | 108 (100) | 4.1 (2.9) | 112 (100) | 4.4 (2.6) | 100 (93) | 3.8 (2.0) | 108 (96) | 4.1 (2.2) | 105 (97) | 5.5 (3.1) | 109 (97) | 6.5 (3.2) |
| GP telephone contact | 26 (24) | 1.3 (0.8) | 13 (12) | 1.8 (1.2) | 21 (19) | 1.2 (0.5) | 27 (24) | 1.1 (0.3) | 31 (29) | 1.5 (0.8) | 32 (29) | 1.3 (0.6) |
| GP home visit | 3 (3) | 1.3 (0.6) | 0 (0) | – | 3 (3) | 1.7 (1.2) | 3 (3) | 2.7 (2.9) | 6 (6) | 1.3 (0.8) | 5 (5) | 2.0 (2.2) |
| Practice nurse contact | 48 (44) | 1.9 (1.4) | 55 (49) | 1.7 (1.2) | 23 (21) | 1.4 (0.9) | 26 (23) | 1.4 (0.9) | 38 (35) | 1.7 (1.5) | 37 (33) | 2.0 (2.0) |
| District nurse contact | 0 (0) | – | 1 (1) | 4.0 (–) | 0 (0) | – | 1 (1) | 1.0 (–) | 0 (0) | – | 1 (1) | 1.0 (–) |
| Community mental health nurse contact | 1 (1) | 3.0 (–) | 0 (0) | – | 1 (1) | 4.0 (–) | 2 (2) | 1.0 (–) | 1 (1) | 4.0 (–) | 2 (2) | 1.0 (0.0) |
| Other nurse contact | 2 (2) | 5.5 (6.4) | 5 (5) | 2.4 (2.6) | 0 (0) | – | 3 (4) | 1.5 (0.7) | 1 (1) | 1.0 (–) | 3 (4) | 1.7 (0.6) |
| Health visitor contact | 9 (9) | 4.9 (5.3) | 8 (7) | 1.5 (0.5) | 2 (3) | 1.0 (0.0) | 0 (0) | – | 2 (3) | 1.5 (0.7) | 1 (1) | 3.0 (–) |
| Counsellor contact | 7 (7) | 2.0 (1.0) | 9 (8) | 3.2 (2.2) | 12 (16) | 3.6 (3.5) | 11 (13) | 5.1 (2.8) | 15 (20) | 6.3 (4.7) | 13 (15) | 6.1 (3.3) |
| Complementary health care | 9 (9) | 5.9 (4.9) | 5 (5) | 2.0 (1.4) | 5 (7) | 5.0 (4.3) | 3 (4) | 1.7 (1.6) | 7 (10) | 7.4 (6.6) | 6 (7) | 2.5 (2.5) |
| Psychologist contact | 1 (1) | 3.0 (–) | 0 (0) | – | 2 (3) | 7.5 (9.2) | 3 (4) | 1.0 (–) | 3 (4) | 9.3 (14.4) | 3 (4) | 2.0 (1.0) |
| Occupational therapist | 2 (2) | 2.0 (1.4) | 2 (2) | 1.5 (0.7) | 0 (0) | – | 4 (5) | 1.5 (0.7) | 0 (0) | – | 6 (7) | 1.8 (1.0) |
| Social worker contact | 1 (1) | 1.0 (–) | 1 (1) | 12.0 (–) | 1 (1) | 2.0 (–) | 0 (0) | – | 1 (1) | 5.0 (–) | 0 (0) | – |
| Housing worker contact | 3 (3) | 2.7 (2.9) | 4 (4) | 2.3 (1.0) | 0 (0) | – | 3 (4) | 1.0 (0.0) | 2 (3) | 1.0 (0.0) | 4 (5) | 2.0 (1.2) |
| Community support worker | 1 (1) | – | 0 (0) | – | 1 (1) | 12.0 (–) | 2 (2) | 4.3 (4.6) | 1 (1) | 24.0 (–) | 2 (2) | 8.0 (9.9) |
| Day centre attendance | 3 (3) | 15.0 (12.3) | 1 (1) | 3.0 (–) | 2 (3) | 3.0 (–) | 0 (0) | – | 2 (3) | 6.0 (–) | 1 (1) | 3.0 (–) |
| Other services | 10 (9) | – | 6 (6) | – | 3 (4) | – | 8 (9) | – | 4 (5) | – | 11 (13) | – |
| Medication (physical) | 57 (54) | – | 67 (62) | – | – | – | – | – | 44 (59) | – | 54 (61) | – |
| Medication (SSRIs) | 3 (3) | – | 1 (1) | – | 22 (20) | – | 97 (87) | – | 25 (23) | – | 97 (87) | – |
| Medication (other mental health) | 12 (11) | – | 15 (13) | – | 21 (19) | – | 13 (12) | – | 23 (21) | – | 17 (15) | – |
During the period between baseline assessment and 12-week follow-up, the vast majority of patients again had contact with GPs. (The few for whom no contacts were recorded had also dropped out of the study.) There was a reduction in contacts with practice nurses and outpatient consultations compared with baseline. The number of prescriptions of psychotropic drugs other than SSRIs remained similar to baseline. (Drugs for physical health problems were recorded with the CSRI but these data were not separated into the two follow-up periods.) The only key difference was in the use of SSRIs, which, not surprisingly, was higher in the SSRI plus supportive care group. However, it is important to note that 13% of patients in the SSRI plus supportive care group were not prescribed an SSRI, while 20% of patients in the supportive care alone group were prescribed one.
Between baseline assessment and the 26-week follow-up, slightly more patients in the SSRI plus supportive care group were admitted to hospital, but overall the numbers in each group were small at 4–7% (including day care). Again, one-third of patients had used outpatient services. Prescriptions for physical health problems continued to be received by more than half of the sample. As before, differences between the samples were small with the exception of the prescription of SSRIs. Therefore, there appeared to be no evidence that the intervention was reducing the reliance on other services. (Informal care costs are discussed later, alongside the costs of lost employment.)
Service costs
Service use data were combined with information on unit costs obtained from recognised sources. Most unit costs were taken from the annual publication of the Personal Social Services Research Unit (University of Kent). 75 These costs reflect salaries, overheads and capital, and are divided by the amount of face-to-face time that professionals spend with patients. Medication costs were derived from the British National Formulary for September 2007, assuming generic prescribing. 76 Finally, NHS reference costs were used to cost the use of hospital-based services. 77 The unit costs used in the cost calculations are shown in Appendix 24. The year used for unit costs was 2006–7, with the exception of the hospital costs, which were based on the most recently available data, for 2005–6, but inflated to estimate costs in 2006–7.
At baseline, mean costs were highest for GP surgery consultations, outpatient contacts and inpatient episodes (Table 46). Inpatient and outpatient costs were higher for the supportive care alone group, as were the costs of complementary health care and community support workers. The cost of medication for physical health problems was higher for the SSRI plus supportive care group. However, the variation around the means was substantial, as indicated by the SDs.
| Service | 6 months to baseline | Baseline to 12-week follow-up | Baseline to 26-week follow-up | |||
|---|---|---|---|---|---|---|
| Supportive care alone | SSRI plus supportive care | Supportive care alone | SSRI plus supportive care | Supportive care alone | SSRI plus supportive care | |
| Inpatient admissionb | 93 (431) | 49 (248) | 100 (804) | 63 (406) | 120 (831) | 241 (1593) |
| Outpatient consultation | 96 (183) | 67 (125) | 40 (112) | 31 (77) | 75 (155) | 63 (135) |
| Day patient admission | 13 (99) | 2 (16) | 2 (14) | 1 (13) | 2 (14) | 1 (13) |
| A&E consultation | 11 (39) | 11 (32) | 7 (44) | 7 (39) | 15 (90) | 23 (112) |
| GP surgery consultation | 124 (86) | 133 (77) | 104 (65) | 118 (69) | 161 (96) | 190 (101) |
| GP telephone contact | 6 (12) | 4 (12) | 4 (10) | 5 (9) | 8 (14) | 7 (12) |
| GP home visit | 2 (11) | 0 (0) | 2 (16) | 4 (28) | 4 (17) | 4 (29) |
| Practice nurse contact | 8 (13) | 8 (12) | 3 (7) | 3 (7) | 6 (12) | 7 (15) |
| District nurse contact | 0 (0) | 1 (8) | 0 (0) | < 1 (2) | 0 (0) | < 1 (2) |
| Community mental health nurse contact | 3 (28) | 0 (0) | 3 (22) | < 1 (3) | 3 (22) | 1 (5) |
| Other nurse contact | 1 (9) | 1 (13) | 0 (0) | < 1 (2) | < 1 (2) | 1 (3) |
| Health visitor contact | 13 (68) | 3 (14) | < 1 (2) | 0 (0) | < 1 (3) | < 1 (2) |
| Counsellor contact | 5 (20) | 8 (31) | 20 (67) | 18 (58) | 34 (99) | 32 (90) |
| Complementary health care | 11 (51) | 3 (22) | 11 (51) | 2 (14) | 24 (93) | 6 (31) |
| Psychologist contact | 2 (20) | 0 (0) | 11 (91) | 2 (11) | 21 (169) | 5 (27) |
| Occupational therapist | 1 (5) | < 1 (1) | 0 (0) | 2 (8) | 0 (0) | 3 (15) |
| Social worker contact | 1 (12) | 27 (287) | 3 (29) | 0 (0) | 9 (73) | 0 (0) |
| Housing worker contact | 8 (73) | 5 (37) | 0 (0) | 1 (7) | 1 (6) | 5 (31) |
| Community support worker | 16 (163) | 0 (0) | 6 (49) | 13 (113) | 11 (98) | 25 (226) |
| Day centre attendance | 10 (71) | 1 (7) | 2 (12) | 0 (0) | 4 (23) | 1 (8) |
| Other services | 14 (86) | 4 (19) | 5 (39) | 8 (39) | 5 (39) | 17 (82) |
| Medication (physical) | 75 (220) | 91 (250) | 49 (147) | 55 (141) | 99 (295) | 110 (282) |
| Medication (SSRIs) | 0.1 (0.4) | 0.01 (0.14) | 2 (7) | 7 (13) | 5 (21) | 13 (26) |
| Medication (other mental health) | 0.3 (1) | 1 (4) | 3 (11) | 1 (5) | 6 (24) | 2 (14) |
In the 12 weeks after randomisation, the use of inpatient and outpatient care and GP surgery consultations again incurred the highest costs. There were few substantial cost differences between the two groups, with the exception of the SSRI costs. Over the entire 26-week follow-up, the SSRI plus supportive care group had inpatient costs that were double those for the supportive care alone group. This group also had higher GP surgery consultation costs and SSRI costs.
Mean service costs in the 6 months to baseline were £94 higher in the supportive care alone group than in the SSRI plus supportive care group (Table 47). Costs up to the 12-week follow-up were closely matched between the groups, and the difference adjusted for baseline was £28. The 95% CI shows this to be non-significant. (Owing to cost data being skewed, bootstrapping with 10,000 resamples was used to produce percentile CIs. This assumes that the distribution of the original sample is representative of the population from which it is drawn. However, calculation of the CIs is the same, regardless of the nature of this distribution.) However, by the 26-week follow-up the mean costs for the SSRI plus supportive care group were £153 higher than for the supportive care alone group, after adjusting for differences in baseline costs. However, the SDs were large and this difference was also non-significant.
| Supportive care alone | SSRI plus supportive care | Difference adjusted for baseline and 95% CI | |
|---|---|---|---|
| 6 months to baseline | 513 (659) | 419 (547) | – |
| Baseline to 12-week follow-up | 388 (932) | 341 (454) | –28 (–656 to 117) |
| Baseline to 26-week follow-up | 629 (1092) | 759 (1730) | 153 (–500 to 304) |
Incremental cost-effectiveness ratios
Service costs were linked with the HDRS to assess cost-effectiveness at 12 weeks and 26 weeks. Chapter 4 has shown that at the 12-week follow-up the mean fall in HDRS score for the SSRI plus supportive care group was 2.3 points greater than the fall for the supportive care alone group. Therefore, the SSRI plus supportive care group had a better outcome and lower costs and may be described as ‘dominant’. At 26 weeks, the mean fall in HDRS scores was 1.7 points greater in the SSRI plus supportive care group. Given that this group also had a cost that was £153 higher than the supportive care alone group, it was necessary to compute an ICER to assist decision makers in assessing whether adding SSRIs to supportive care represents value for money. An ICER is defined as the difference in costs between two groups divided by the difference in outcomes. At 26 weeks, the ICER is therefore £153 divided by 1.7, i.e. £90. This is the extra cost incurred by the SSRI plus supportive care group in achieving an extra unit of improvement on the HDRS compared with the supportive care alone group.
Cost-effectiveness planes
The above calculations of dominance at 12 weeks and an ICER of £90 at 26 weeks are based on the average cost and HDRS differences and therefore do not take uncertainty around these estimates into account. To address such uncertainty, cost-effectiveness planes were produced to show the probability of the SSRI plus supportive care group having (1) lower costs and better outcomes, (2) higher costs and better outcomes, (3) lower costs and worse outcomes and (4) higher costs and worse outcomes in comparison with supportive care alone. To construct the cost-effectiveness planes, four regression models were run using 1000 bootstrapped resamples. The models used service costs and HDRS scores at 12 weeks and 26 weeks as the dependent variables. The independent variables were the group identifier and the baseline measure of cost or HDRS. The 1000 coefficients for the group identifier variable are 1000 estimates of the cost/outcome differences and these were plotted against each other.
The cost-effectiveness plane showing cost and HDRS differences at 12 weeks is shown in Figure 7. The ‘south-east’ quadrant indicates the situation where the SSRI plus supportive care group has lower costs and better outcome than the supportive care alone group, and 54.9% of resamples showed this result. By contrast, 45.0% of cost–outcome differences were in the ‘north-east’ quadrant, where the SSRI plus supportive care group has better outcomes but also higher costs. Only 0.1% of resamples showed the SSRI plus supportive care group having lower costs and worse outcomes (‘south-west’ quadrant) and none showed higher costs and worse outcomes (‘north-west’ quadrant).
FIGURE 7.
Cost-effectiveness plane of cost and HDRS differences at 12 weeks.
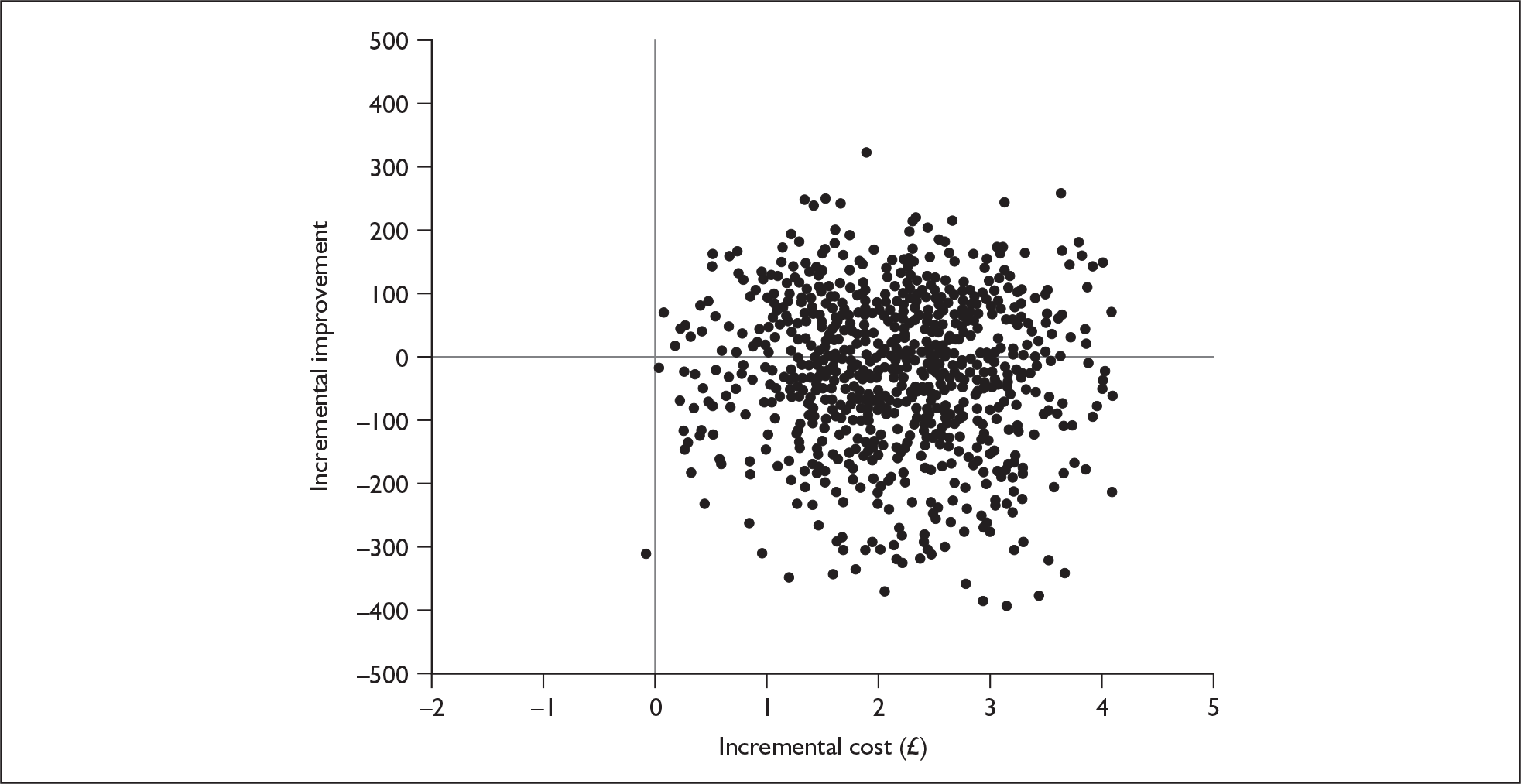
At the 26-week follow-up, the majority (76.7%) of resamples showed that the SSRI plus supportive care group had higher costs and better outcomes (Figure 8). In 22.2% of resamples there were lower costs and better outcomes, while 0.8% of resamples showed higher costs and worse outcomes. Finally, 0.3% of resamples showed the SSRI plus supportive care group to have lower costs and worse outcomes.
FIGURE 8.
Cost-effectiveness plane of cost and HDRS differences at 26 weeks.
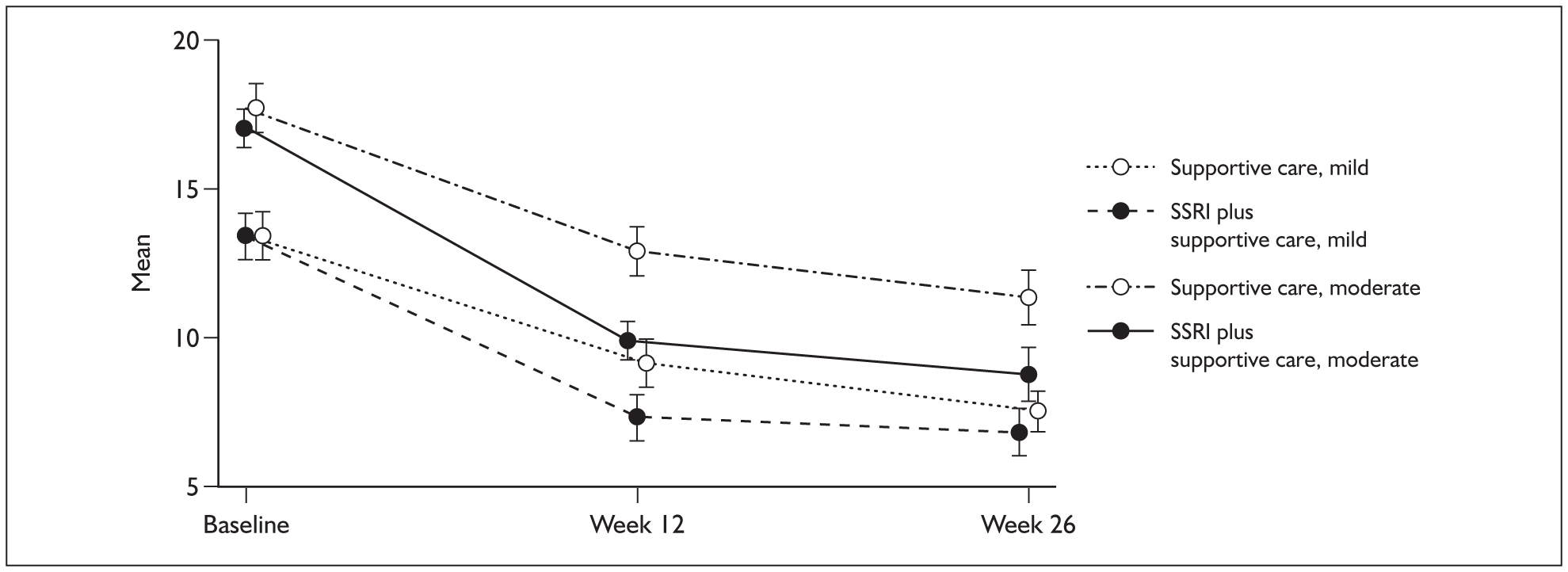
At both 12 weeks and 26 weeks, there was a high likelihood of the SSRI plus supportive care group having higher costs and better outcomes as measured by the HDRS. Whether this incremental improvement in outcome represents good value for money given the likelihood of higher service costs is a value judgement. However, this judgement can be informed by constructing CEACs, which show the likelihood that adding SSRIs to supportive care is more cost-effective than supportive care alone for different values placed on a unit improvement on the HDRS.
Cost-effectiveness acceptability curves
CEACs were constructed using the net-benefit approach. 5 There is a theoretical, but unknown, value (represented by the term λ ) that society would place on a one-unit reduction in depression as measured by the HDRS. Net benefit can be defined as:
where NB = net benefit, E = effectiveness (i.e. reduction in the HDRS score over 12 and 26 weeks compared with baseline) and SC = service costs. For example, if, for a particular patient, the HDRS score is reduced by 8 points during the follow-up period and if their service cost is £250, then we can calculate their net benefit if we know λ. If λ = £0, then the net benefit is –£250, whereas if λ = £40, then the net benefit is £70. Net benefits for all patients were estimated by assuming different values for λ, ranging between £0 and £200 in £20 increments. Then a regression model was used to determine the mean difference in net benefit between the supportive care alone and SSRI plus supportive care groups for every value of λ. For each model, 1000 regression coefficients for the group identifier variable were generated using bootstrapping, and the proportion of these that were greater than 0 indicated the probability that SSRI plus supportive care was more cost-effective (i.e. it resulted in a mean incremental net benefit greater than 0). These probabilities were subsequently used to generate the CEACs.
The 12-week and 26-week CEACs are shown in Figure 9. With regard to the 12-week curve, even if society would not be willing to attach any monetary value to a one-unit reduction in the HDRS there would remain a likelihood of 55% that SSRIs plus supportive care is the most cost-effective option. As a unit improvement is valued at higher levels, this likelihood goes on increasing. While we do not know the true societal value that should be placed on a unit improvement on the HDRS, it can be seen that beyond around £100 the curve flattens out, meaning that further increases have a diminishing impact on the likelihood that adding an SSRI will be the most cost-effective option.
FIGURE 9.
Cost-effectiveness acceptability curves showing probability that SSRIs plus supportive care is most cost-effective option.
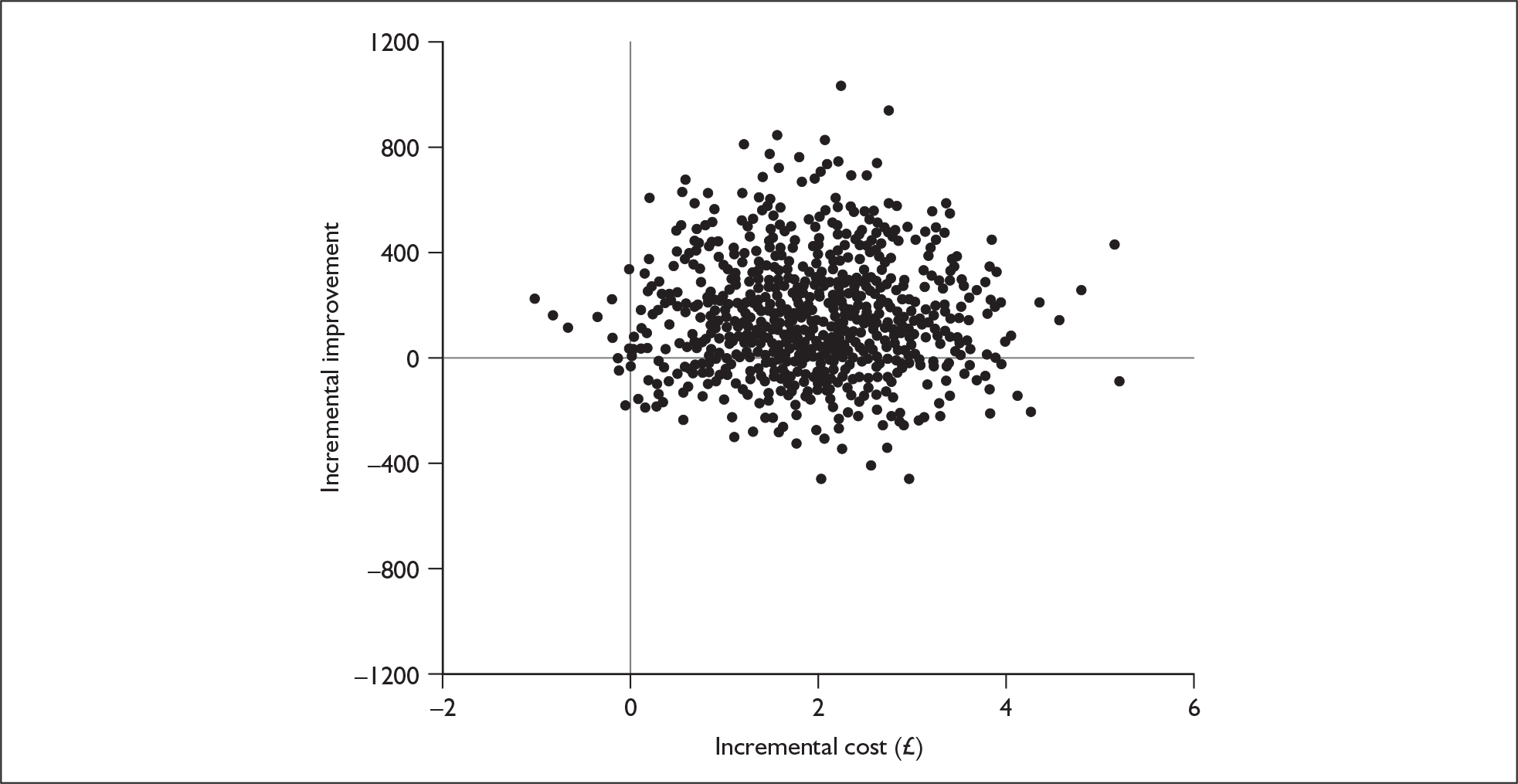
The 26-week CEAC is below the 12-week CEAC, which reflects the reduced difference between the two groups at 26 weeks and the higher cost for the SSRI plus supportive care group. The latter intervention has a greater than 50% likelihood of being the most cost-effective option only if the value placed on a unit reduction on the HDRS is above £80.
Cost–utility analysis
Measuring outcomes using the HDRS has obvious clinical relevance and allows the results of this study to be compared with those of many other depression trials. However, policy makers need to make decisions regarding interventions across all areas of health care, and therefore a generic measure of outcome is also required. The most commonly used generic measure is the QALY, where the time spent in a health state is adjusted by a figure between 0 and 1 to reflect quality of life. This ‘utility’ value was generated from the SF-36 using an algorithm developed by Brazier and colleagues. 78 Clearly, there are other ways of estimating QALYs, and indeed alternative algorithms for calculating utility scores do exist. These may have produced different findings. However, the Brazier et al. method seemed most appropriate because it was based on the SF-36 (rather than the SF-12, as used elsewhere) and on a UK sample. The utility scores at baseline assessment and each follow-up are shown in Table 48. Scores at 12-week follow-up were significantly higher in the SSRI plus supportive care group. At 26-weeks the difference was non-significant.
| Supportive care alone | SSRI plus supportive care | Difference adjusted for baseline (95% CI) | |
|---|---|---|---|
| 6 months to baseline | 0.5748 (0.0714) | 0.5857 (0.0700) | – |
| Baseline to 12-week follow-up | 0.6467 (0.1230) | 0.6856 (0.1237) | 0.0360 (0.0005 to 0.0715) |
| Baseline to 26-week follow-up | 0.6782 (0.1339) | 0.6998 (0.1295) | 0.0175 (–0.0230 to 0.0579) |
Calculation of quality-adjusted life-years
Quality-adjusted life-years were calculated using area under the curve methodology. 79 The baseline utility score was added to the score at 12 weeks and this total was divided by 2, based on the assumption of a linear change over the 12-week period. This figure was then multiplied by 0.25, as only one-quarter of a QALY could be gained over the 12-week period. The QALY gain in the 12-week to 26-week period was calculated in a similar way. Gains in QALYs over the entire 26-week follow-up period were calculated by adding these two 3-month QALY gains. The mean QALY gain between baseline and 12-week follow-up was 0.1522 for the supportive care alone group and 0.1588 for the SSRI plus supportive care group. The difference adjusting for baseline was 0.0045 in favour of the SSRI plus supportive care group. As with the HDRS measure, adding SSRIs to supportive care was ‘dominant’ as costs were lower and QALY gains greater. By 26 weeks, the QALY gain in the supportive care alone group was 0.3176 and in the SSRI plus supportive care group it was 0.3305. The adjusted difference was 0.0103. Dividing the incremental cost of £153 by 0.0103 produced an ICER of £14,854, i.e. a cost of £14,854 would be incurred to gain an extra QALY as a result of prescribing SSRIs along with supportive care.
Uncertainty around the finding of dominance at 12 weeks and the ICER of £14,854 at 26 weeks were explored, as before, using cost-effectiveness planes. At 12 weeks, 52.1% of the resamples showed lower costs and a greater QALY gain for the SSRI plus supportive care group while 44.8% showed higher costs and more QALYs (Figure 10). Only 1.0% showed lower costs and a lower QALY gain and 2.1% showed higher costs and a lower QALY gain. The cost-effectiveness plane for the QALY gain and cost differences by 26 weeks is similar to that for the HDRS at 26 weeks (Figure 11). Most resamples (72.1%) showed higher costs and a greater QALY gain for the SSRI plus supportive care group. Lower costs and more QALYs were revealed in 24.3% of resamples. Lower costs and fewer QALYs were shown by 0.2% of resamples and higher costs and fewer QALYs by 3.4%.
FIGURE 10.
Cost-effectiveness plane of cost and QALY differences at 12 weeks.
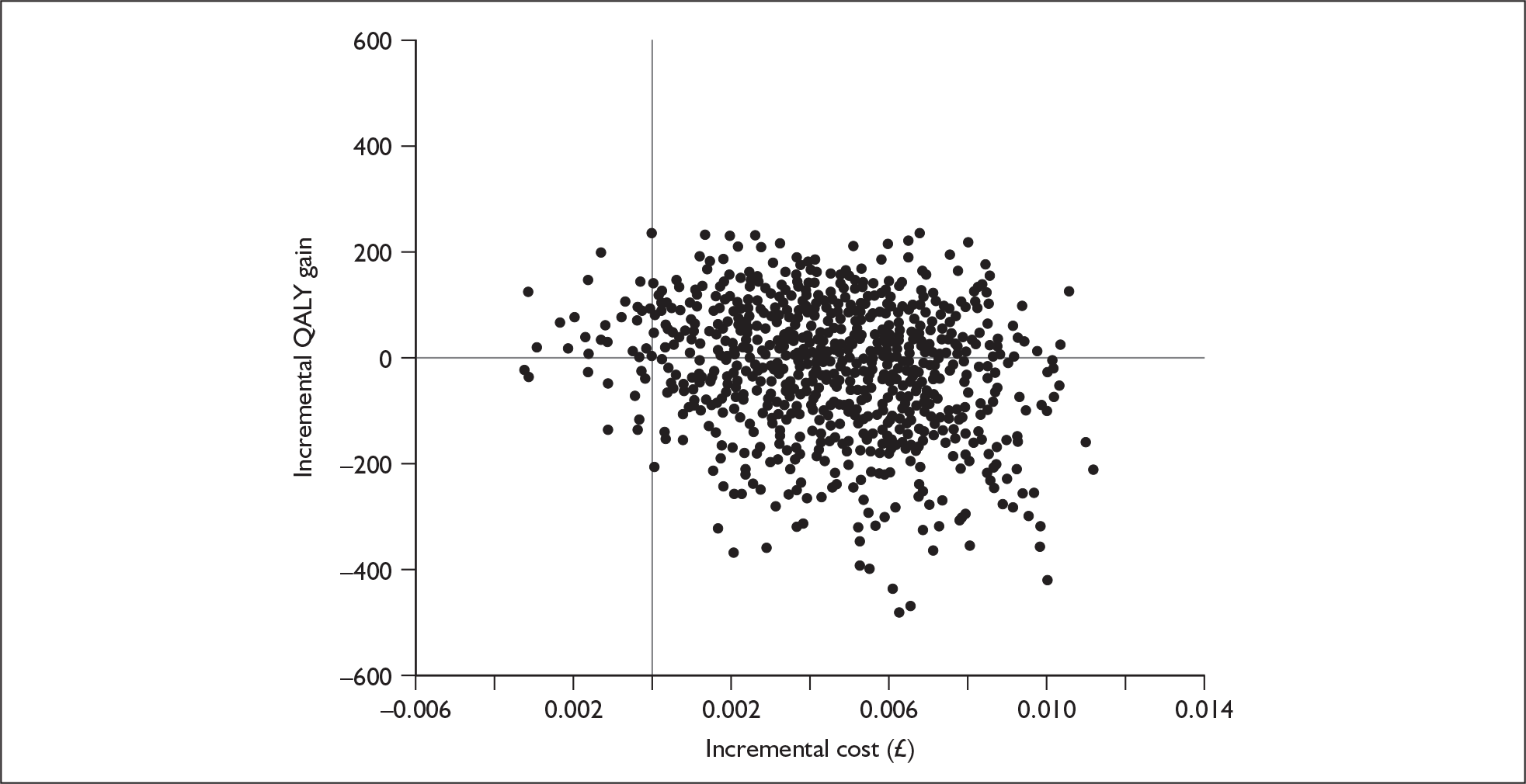
FIGURE 11.
Cost-effectiveness plane of cost and QALY differences at 26 weeks.
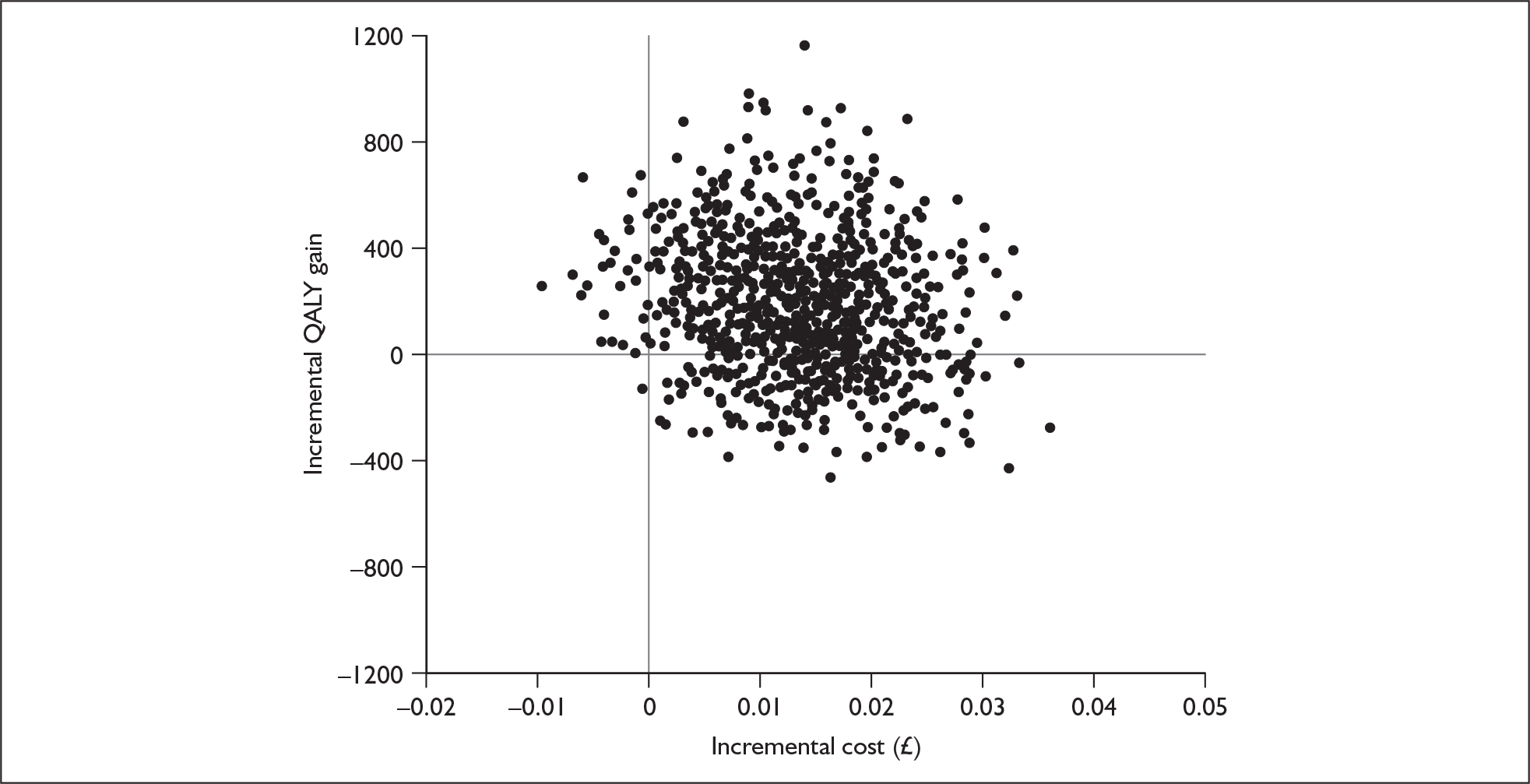
CEACs were produced using the net-benefit approach as described above. The range of λ values was between £0 and £50,000 in £5000 intervals. (This range was chosen as values above this would usually mean that the intervention would not be recommended by NICE.) Figure 12 shows that with a zero value attached to a QALY gain at 12 weeks, there is still a 53% likelihood of SSRIs plus supportive care being cost-effective. With a QALY gain valued at £20,000–£30,000 (the thresholds usually associated with NICE recommendations), there is an 80–85% likelihood of this being the most cost-effective option. The CEAC related to QALYs at 26 weeks is again below the 12-week CEAC. However, there remains a high likelihood that SSRIs plus supportive care are cost-effective: 65% to 75% for a value of £20,000 to £30,000 per QALY respectively.
FIGURE 12.
Cost-effectiveness acceptability curves showing probability that SSRIs plus supportive care is most cost-effective option.
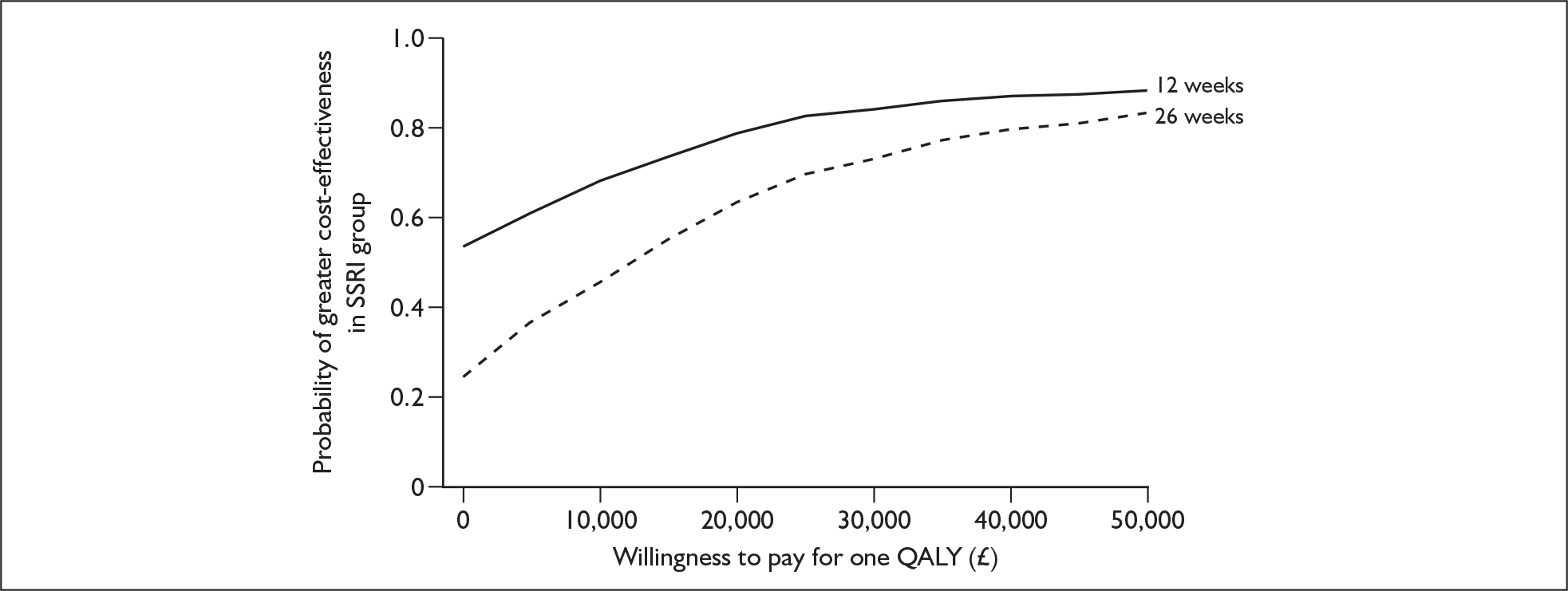
Impact on carers and employment
The above analyses focus on health and social care costs. However, it is likely that people with depression will require help from family members/friends as a result of their condition. In addition, it is well known that depression has a major impact on work. Data on the use and costs of informal care and the impact on work are shown in Table 49.
| 6 months to baseline | Baseline to 26-week follow-up | |||
|---|---|---|---|---|
| Supportive care alone | SSRI plus supportive care | Supportive care alone | SSRI plus supportive care | |
| n (%) using informal care | 13 (12) | 17 (16) | 11 (15) | 13 (15) |
| Mean (SD) hours per weeka | 5.2 (5.2) | 6.4 (8.7) | 4.3 (6.1) | 6.5 (9.3) |
| Mean (SD) cost (£)b | 267 (1021) | 412 (1688) | 202 (672) | 397 (1744) |
| n (%) with lost work | 14 (13) | 14 (13) | 11 (15) | 18 (22) |
| Mean (SD) lost weeksc | 17.6 (11.4) | 11.7 (10.7) | 19.8 (9.7) | 18.3 (10.1) |
| Mean (SD) production loss (£)d | 786 (2856) | 504 (2128) | 1146 (3381) | 1484 (3725) |
While relatively few patients received informal care, the cost was high. The unit cost used was the hourly cost of a homecare worker, and those who did receive informal care did so for a substantial number of hours per week. It can be seen that informal care costs were greatest for the SSRI plus supportive care group during the follow-up period but that this difference was not statistically significant. The costs of informal care were high, and this may be seen as surprising. For some disorders (e.g. dementia), high levels of informal care would be expected, but perhaps not for depression. Informal care costs were not included in the cost-effectiveness analyses because in the UK, NICE generally takes an NHS perspective. However, we have shown that these costs are important and should be investigated further.
Lost employment was experienced by a small number of patients. This could, however, be an underestimate as patients were asked to describe interruptions to work rather than asked specifically for the amount of time off, although many did provide this information. Lost employment costs were, though, substantial if costed at the median wage in the UK in 2007 of £457 per week. These costs increased during the follow-up period but did not differ significantly between the groups. It is interesting, however, that the apparent health improvement for those in the SSRI group was not matched by reductions in lost employment. This may be because (1) receipt of SSRIs ‘reinforced’ the feeling of being unwell and/or (2) doctors may be more likely to sign a patient off work at the same time as issuing a prescription of antidepressants. As with informal care costs, we did not include lost employment costs in the cost-effectiveness analyses because of the perspective taken by NICE.
Chapter 6 Discussion
Summary of the main findings
Primary and secondary outcomes
Statistically significant differences in favour of the SSRI plus supportive care arm at follow-up were found in terms of lower scores on the HDRS, higher scores on the SF-36 MH subscale and higher scores on the MISS, but not in terms of lower BDI scores. Differences in the SF-36 VT score were of borderline significance, and the other SF-36 subscales were not significantly different.
Significant differences between the arms in the mean fall in HDRS score were found at both follow-up points when analysed separately, but were relatively small: 2.3 points at 12 weeks and 1.7 points at 26 weeks. The NNTs for remission (to HDRS < 8) were 6 at 12 weeks and 6 at 26 weeks, and the NNTs for significant improvement (HDRS fall of ≥ 50%) were 7 and 5 respectively. These numbers suggest that the addition of an SSRI is useful clinically, as fewer than eight patients need to be treated for one to gain clinically significant benefit, although these summary figures have to be treated with caution as the CIs around these estimated NNTs were relatively wide.
Predictors of outcome
No significant differences were found between severity subgroups for the HDRS findings in the longitudinal analysis including outcomes at both follow-up points, so we have no evidence of a differential response to treatment between patients with mild and moderate depression in this sample. The mean HDRS scores in the two arms did converge more by 26 weeks in the mild depression subgroup than in the moderate subgroup, but the interaction terms were not significant. However, the study had limited power to determine differences in response between the two severity subgroups (see below).
A poorer outcome in terms of a higher HDRS score at follow-up was significantly related to a higher baseline HDRS score, higher baseline BSI physical symptom score and being unemployed at baseline. It is important to note that the effect size of unemployment was of a similar magnitude to that of the treatment arm. A higher BDI score at follow-up was also significantly related to a higher baseline BDI score and unemployment at baseline. A lower MH score at follow-up was also significantly related to lower baseline values and unemployment at baseline. A lower VT score at follow-up was also significantly related to a lower baseline VT score and older age at randomisation, with a borderline significant relationship to unemployment at baseline.
None of the other possible predictors of outcome was significantly related to the HDRS score at follow-up, including sociodemographic factors, life events and difficulties at baseline, duration of depression, a past history of depression, previous use of antidepressants, a physical versus non-physical patient attribution of symptoms or level of alcohol use. There were also no statistically significant interactions between these possible predictors and trial arm in terms of predicting a differential response to SSRI treatment.
Costs and cost-effectiveness
Costs were slightly higher in the SSRI plus supportive care arm, but not statistically significantly different. Incremental cost-effectiveness ratios and cost-effectiveness planes suggested that adding an SSRI to supportive care is probably cost-effective, with mean costs of £90 per point improvement on the HDRS and £14,854 per QALY gain. The CEAC for utility suggested that adding an SSRI to supportive care is cost-effective at the value of £20,000–£30,000 per QALY used by NICE, with a 65–75% probability. Informal care costs were relatively high, given that the patients had only mild to moderate depression, but did not differ significantly between arms.
The process of care
More than 90% of patients in each arm received supportive care from the GPs, with a mean number of consultations of around four during the 12-week treatment period, as planned. In the event, SSRI antidepressants were received by 87% of patients in the SSRI plus supportive care arm, so 13% were not treated despite being randomised to receive an SSRI. Furthermore, 20% of patients in the supportive care alone arm were also treated with SSRIs, which was permissible within the protocol if, in the GP’s clinical judgement, the patient worsened and required drug treatment. No difference was found in patient-reported consultation content between arms, suggesting that GPs do not discuss non-drug strategies to tackle depression to a greater extent with their patients when they are not prescribing an antidepressant.
Strengths of the study
Even though practitioner referral rates into the study were lower than anticipated and one in three patients referred declined to be randomised, the research team managed to achieve the assessment of our primary outcome in 186 patients, close to our target sample size of 196, through the recruitment of more and more practitioners over more than 3 years. This was particularly challenging, owing to a steady stream of adverse publicity in the media about the effects of antidepressants throughout the course of the trial. 80–83 However, as a result of the team’s efforts, the study had sufficient power to determine a relatively small difference in outcome between the two arms of around 1.5 points on the HDRS. The randomisation process was also successful, with well balanced numbers in the two arms and in the two severity subgroups within each arm. We achieved higher than expected follow-up rates at both time points, reducing the likelihood of bias due to patients dropping out. Patients were followed up for 26 weeks, which is considerably longer than most commercial drug trials which have only 6–12 weeks’ follow-up, and the two follow-up points allowed longitudinal analyses of outcomes, which maximised the power of the sample to detect differences between arms.
A range of relevant primary and secondary outcomes were measured, including depressive symptoms, generic health status, patient satisfaction and costs. Costs were carefully gathered from a health service perspective using both patient questionnaires and GP medical records to maximise completeness,70 and informal care costs, including interruption of work and costs to family and friends, were also gathered. Most of the assessments carried out were self-completed, avoiding the possibility of observer bias. Interviewer training and frequent inter-rater reliability checks ensured high quality and consistent measurement of the HDRS primary outcome, and greatly reduced the likelihood of observer bias.
Data were collected on patients seen in surgeries who were eligible for the study but were not referred and on patients who were referred but not randomised, which allowed exploration of the representativeness of randomised patients. In addition, reasons for non-participation were gathered from those patients referred to the study team who did not consent to be randomised.
Therefore, in a number of respects, this study compares very favourably with primary care trials of antidepressants identified in a recent systematic review, most of which were small, commercially funded studies of short duration and low methodological quality. 23,84 It is crucial that clinicians working in primary care have good quality evidence from primary care studies to inform their practice. The 2004 NICE guidelines on antidepressant treatment were based on a review including 31 outpatient-based studies, three inpatient studies, 13 mixed studies and only one from primary care. 11 Among the 19 studies for which it was possible to determine baseline severity, four were of moderate depression, six of severe depression and nine of very severe depression. 11 Therefore, there was clearly a need for further, comparable studies of the treatment of mild to moderate depression in primary care.
Limitations of the study
The study was powered to detect only a relatively large difference in outcome, of 2.5 points on the HDRS, between the mild and moderate severity subgroups, and was not powered to detect equivalence in the effect of treatment. Therefore, while we found little evidence of a differential response to treatment between the two severity subgroups, we cannot say that adding an SSRI to supportive care is as effective in mild depression as in moderate depression. The power of the study was even more limited for the analyses of the other possible predictors of outcome and response to treatment, which must be regarded as exploratory.
We allowed GPs to prescribe antidepressants to patients in the supportive care alone arm if their depression persisted or worsened, so the drug treatment of 20% of patients in that arm was not a protocol violation as such. We did not collect any data on why GPs failed to prescribe SSRIs to 13% of the patients randomised to the SSRI plus supportive care arm, although this was probably because the GP and patient between them decided they did not want to use them after all. Qualitative interviews with the participating GPs might have shed light on why they failed to follow the randomisation recommendations in a minority of cases in both arms.
In an open label pragmatic trial of this nature, it is often not possible to keep the researchers responsible for assessing outcome in the patients blind to allocation to trial arm. In this study, the researchers were unblinded in 25% of cases at 12 weeks and 33% at 26 weeks, which raises the possibility of observer bias. In this respect, it is also important to note that we did not see similar changes in the self-completed BDI to the observer-rated changes in the HDRS. However, we consider that observer bias is an unlikely explanation for the effects found on the HDRS, for a number of reasons. First, the careful training and frequent inter-rater reliability checks would have greatly reduced the likelihood of observer bias, as the researchers were taught how to interpret patient responses to the individual items on the HDRS in a consistent way, and they were aware that a random sample of their audiotaped interviews would be rated again by a second researcher and discussed with one of the trainers. Second, we did see corresponding changes to the HDRS findings in the self-completed MH and VT subscales of the SF-36, as well as in self-rated patient satisfaction scores, so the lack of changes in the BDI may have been due to a relative insensitivity to change (see below), rather than because it was self-completed. Third, there was no expectation in the study group either way about the likely outcome which might have biased the researchers towards finding an effect. The study group included investigators holding a range of contrasting views about the effectiveness of antidepressants, and we consciously and explicitly maintained equipoise about the likely findings in discussion in study group meetings, stressing that we were interested in the outcome whatever the result.
We experienced greater loss to follow-up in the London centre than in the other two, which was due partly to a member of the team leaving the study and a gap in the availability of a researcher in London to carry out follow-up assessments for a few months until a replacement could be appointed. There was also differential loss to follow-up between the two treatment arms, raising the possibility of attrition bias. More patients were lost to follow-up in the supportive care alone arm, perhaps because they did not receive ‘active’ treatment, but we cannot say whether they were likely to fare better or worse than those remaining in the study. However, the difference in follow-up rates was relatively small (only 3% at the 12-week follow-up point, at which the primary outcome was determined) and we took steps to take account of these issues, by inclusion of recruitment centre and predictors of missing data in the adjusted analyses of outcome. The validity of this approach assumes that the predictors have been correctly identified; if the data were not missing at random (NMAR) then there is still a possibility of bias in the estimates.
Generalisability
The design of the study was very close to real-life practice in terms of the decision GPs face, i.e. whether or not to treat patients with new episodes of depression with SSRI antidepressants, as well as providing support by means of follow-up consultations. It was also close to real-life practice in that the GPs themselves delivered the treatment, so the results are readily generalisable to UK primary care. The pattern of treatment recorded in the GP records in this trial is comparable to that found in routine practice, judging from previous studies of medical record data in UK general practice. 85–87 It is possible to estimate treatment effects, including allowance for both non-compliance with treatment and loss to follow-up, using a complier average causal effect (CACE) analysis,88 which we will explore and may present in a subsequent publication.
The tallies of surgery logs completed by a number of the study GPs at various points during the study showed that only around 1 in 10 patients with a new episode of depression were referred into the study, mainly because the rest did not fulfil the inclusion criteria, particularly in terms of a lack of equipoise about the benefits of drug treatment on the part of the doctor or patient or both. This raises the question of how representative were the participating patients of all patients presenting with depression, but inevitably we could include in a randomised trial only those patients who were in equipoise about treatment, and whose doctors were in equipoise. It is more difficult to carry out a randomised trial of treatment that is already established in practice, as most doctors and many patients already have opinions about its effectiveness, which would not be such a problem for a trial of a new treatment. We found evidence that male patients were less likely to be referred into the study, but referred patients were representative in terms of age. We also had relatively few patients referred in the upper age group even though we had issued no age restriction to the GPs. This may reflect known lower rates of treatment in older people (which Age Concern has highlighted in a recent report89) or possibly a reluctance to enter older people into a trial, because of the extra demands for assessments which are then placed on them. Qualitative interviews with the participating GPs might have given better insight into why some eligible patients were not referred than did the limited information written in the surgery logs.
Only one in three referred patients was randomised, due partly to a number having HDRS scores outside the required range of severity, but also again due in part to a lack of patient equipoise about the effects of treatment and a subsequent unwillingness to be randomised, especially to the drug treatment arm. However, those patients who were randomised were generally representative in terms of both gender and age of the patients referred into the study. No preference arms were included in the study design, which it might be supposed would have allowed more patients to join the study given that many declined to be randomised owing to a strong preference against having antidepressants. However, piloting of preference arms partway through the study suggested that adding them tended to reduce the numbers of patients agreeing to be randomised, compromising the most important objective of the trial. Again, qualitative interviews might have engendered greater understanding of why so many patients declined to be randomised after accepting referral into the study than did the relatively brief questions asked when consent was withheld.
The inclusion criteria were kept as wide as possible given the constraints of the trial. In addition to the 87 who were excluded because of an HDRS score outside the defined range, a further 50 patients were excluded because they had received antidepressant treatment within the last 12 months. This exclusion criterion was designed to limit the sample to patients presenting with new bouts of depression; it was set at 12 months because depression is a relapsing condition and recurrence of symptoms within 12 months is common, and probably represents a relapse rather than a new episode. We wanted to determine the effectiveness and cost-effectiveness in new episodes and to be clear that we were not dealing with relapsing chronic depression. It is possible that we may have excluded fewer patients if we had relaxed this criterion, but we thought it was important. We do not have any data on the number who would have been excluded if the criterion had been 6 months instead of 12, for example, so we are unable to say whether this criterion was unnecessarily strict.
However, unlike some antidepressant studies, we did not exclude people on the basis of physical comorbidities, and the sample included many patients with physical health problems, evidenced by the number of medications and outpatient attendances for non-mental health problems. This is to be expected in a relatively non-selected primary care sample where one of the inclusion criteria is the presence of somatic symptoms. The patients were found to be similar, in terms of their levels of use of services and generic health status on the SF-36, to those in previous primary care trials of depression treatment. 90–92 We also measured the number of physical symptoms and alcohol consumption so that we could explore the effects on outcome of depression and response to treatment of these very common complicating factors.
Interpretation of the study findings in light of previous research
Changes in primary and secondary outcomes
The results are consistent with our initial hypothesis that treatment with an SSRI plus supportive care is more effective and cost-effective than supportive care alone, for mild to moderate depression in UK primary care. It is also consistent with two out of three of the placebo-controlled studies of antidepressant treatment referred to in Chapter 1, which demonstrated benefits in mild to moderate depression. 25,28,31 The mean differences found in HDRS scores (2.3 at 12 weeks and 1.7 at 26 weeks) are greater than the mean difference of 1.0 found by Judd et al. 28 in a placebo-controlled trial of fluoxetine, but not as great as the 2.9 point mean difference found by Perahia et al. 31 in their post hoc analysis of two placebo-controlled trials of duloxetine.
A randomised controlled trial of usual care with or without antidepressant medication for primary care patients with depression has recently been carried out in the Netherlands, measuring clinical effectiveness but not cost-effectiveness. 93 The study was very similar to ours, as patients were randomised to usual care alone (four consultations within 3 months) or to treatment with the SSRI paroxetine plus usual care, although they were followed up for 52 weeks rather than for 26 weeks as in our study. However, the results showed no significant differences between the treatment groups in an intention-to-treat analysis, in terms of depressive symptoms measured using the Montgomery–Åsberg Depression Rating Scale (MADRS),94 or in terms of mental or physical functioning on the SF-36, although there was slightly greater patient satisfaction in the paroxetine arm at 13 weeks’ follow-up (but not at 52 weeks). 93 Post hoc subgroup analysis suggested that patients with more severe depression, but not those with minor depression, might benefit from antidepressant treatment. However, with a sample size of 181, which had fallen to 160 at 13 weeks’ follow-up, the trial was smaller than ours and probably lacked sufficient power to detect a clinically significant effect of treatment. It was described as an equivalence trial, but the difference chosen for the power calculation was relatively large, i.e. five points on the MADRS. In fact, the study demonstrated a three-point mean difference in MADRS scores at 26 weeks in favour of the paroxetine arm, which is a similar effect size to ours, but this was not statistically significant in the Netherlands trial. Their patients had to have symptoms for only 2 weeks rather than the 8 weeks specified in our study, so more patients may have had transient depression and recovered without drug treatment. Their patient sample had much greater variance in depression scores at baseline than ours, because they did not specify a narrow range for inclusion as we did, which further reduced the power of the study to detect small differences between arms. The other difference was that a significant minority of patients in their trial received specialised help from mental health services, and this happened twice as often in the usual care arm than in the paroxetine arm. All these factors would tend to reduce the differences found between the two arms in the Netherlands trial.
As we found no significant effect of severity subgroup on response, the results do not support our second hypothesis that SSRI treatment plus supportive care is relatively more effective among patients scoring 16–19 on the HDRS in comparison with those scoring 12–15, in contrast to the previous placebo-controlled study of amitriptyline by Paykel et al. ,20 although as stated above the power was limited to detect differences between severity subgroups.
This was not a placebo-controlled trial and the benefits found could be due largely to a placebo effect of the SSRIs. A recent systematic review and meta-analysis by Kirsch et al. ,95 of 35 published and unpublished placebo-controlled trials of SSRIs registered with the US Food and Drugs Administration, suggested that there is a significant placebo response to antidepressants which may account for most of their effect in depression except at the highest levels of severity (HDRS scores of 28 or more). It should be noted that the meta-analysis included only one trial in mild depression and its conclusions rested on extrapolation from trials in moderate to severe depression,95 but it is consistent with previous research suggesting that drug–placebo differences are greater for more severe depression. 96,97
Drug treatment may be an important symbolic gesture on behalf of the GP in the patient’s eyes, conveying the message that the doctor takes the patient’s problems seriously and believes it when the patient says that their depression is serious. 98 Antidepressants may help to ‘exculpate’ patients, invoking a disease, or a biochemical imbalance, as a cause of their problems which allows them to accept less responsibility for the situation in which they find themselves. 99,100 Antidepressants may also help patients to cope better with their problems by improving their sleep and reducing anxiety symptoms, and so help their symptoms of depression indirectly. 11 In relation to this point, however, preliminary analysis of the HDRS results in this study shows that the core symptoms of depression did change, suggesting that sleep and relief of anxiety symptoms were not responsible for the benefits found. A more extensive analysis of the individual HDRS symptoms is planned, and may appear in a subsequent publication.
However, whether or not the benefit of antidepressant treatment found in this study is due to a placebo effect, it is important to consider whether it is a clinically significant effect. Kirsch et al. 95 suggest that a difference between arms of less than 3 points on the HDRS is not clinically significant, because this was the drug–placebo difference regarded as significant by the NICE Depression guideline development group. 11 However, we understand that this was a decision based on a consensus arrived at through discussion by clinicians, service users and carers involved in the guideline development, and was not based on an objective validation of changes in HDRS scores against levels of patient functioning or quality of life. It is also important to note that the mean difference in scores among a group of patients is only the average of a range of individual responses, with some patients improving considerably more than the average and some not improving at all, or even getting worse on treatment, as we showed was the case in this study by means of the box plots of HDRS scores at the three measurement points. It is also important to consider that the HDRS is an ordinal scale, but not an interval scale, which means that a difference of 2 points at the mild end of the spectrum may be more important than a difference of 2 points at the severe end. 101
It is important to note that the difference in favour of the SSRI plus supportive care arm was found despite the fact that 20% of patients in the supportive care alone arm also received SSRIs. According to the CSRI data, the mean duration of SSRI treatment taken was 144 days, and two-thirds of participants prescribed SSRIs reported using them for the whole of the 26-week period. Further analysis of the number, dates and length of prescriptions for each patient according to their GP records will be carried out to determine the duration of treatment, which is likely to be more accurate than patient recall over 26 weeks. It is important to note that, although guidelines recommend at least 6 months’ treatment with antidepressants,11 the pattern of prescribing recorded in the GP records is comparable with previous medical record-based studies of the amount and duration of antidepressant treatment in UK general practice. 85–87
The negative result for the BDI is interesting, given the positive findings for the HDRS. As stated above, this is unlikely to be due to the fact that it is self-completed, since positive changes were seen in the self-completed SF-36 MH and VT subscales and MISS satisfaction scores. It may be because the version of the BDI that we used measures different aspects of depression to the HDRS and is less sensitive to change. There is evidence that the BDI measures more trait-like features of personality such as chronic low self-esteem and pessimism rather than the core symptoms of depression. 102 The HDRS is closer to the DSM-IV concept of depressive disorder7 because it measures the mandatory symptoms of depression (depressed mood, loss of interest), all the somatic and most of the cognitive symptoms, whereas the BDI primarily measures cognitive symptoms. 103 As a result the BDI shows a lack of sensitivity to change with physical treatments such as antidepressants when compared with the HDRS or the MADRS. 102 The BDI is more likely to improve in trials of psychotherapy such as cognitive behaviour therapy where chronic low self-esteem is usually a specific target of the treatment. The version of the BDI we used in this study has been replaced by a second edition, the BDI-II. One of the main objectives of this new version was to improve its content validity by adding, eliminating or rewording items to conform more closely to the US DSM-IV diagnostic criteria for depression. As a result, the BDI-II displays greater reliability and sensitivity to change. 104
The observed changes in SF-36 scores over the 26 weeks were similar to those found in previous studies of treating depression in primary care in both the UK and the US. The HTA-funded Assessing Health Economics Antidepressants Study (AHEAD) comparison of the health economics of three classes of antidepressants reported changes in mean MH scores over 6 months of treatment from 37 at baseline rising to 70, comparable to the change from 39 to 61 in the SSRI plus supportive care group in this study. 92,105 In the AHEAD study, the role – emotional (RE) scores rose from 23 to 58 and the general health (GH) scores rose from 54 to 65, which again were comparable to the changes we saw in the SSRI-treated group from 18 to 58 for RE and from 49 to 61 for GH. 92,105 Lin et al. ,91 in their trial of collaborative stepped care for depression, reported changes over 6 months in mean social functioning (SF) scores, rising from 50 at baseline to 71 in treated patients and from 52 rising to 68 in controls, comparable to the changes we found in SF scores (46 rising to 71 and 44 rising to 68 respectively). They found changes in RE scores from 26 rising to 55 in treated patients and from 24 to 52 in controls, again comparable to the changes we found in RE scores (17 rising to 59 and 19 rising to 57 respectively). 91
Differences between arms in the mean total scores on the MISS, although statistically significant, were relatively small, with a difference of only 5 points between 150 in the supportive care alone arm and 155 in the SSRI plus supportive care alone arm. We plan to carry out a factor analysis of the MISS scores, to determine which of the underlying factors within the questionnaire changed and which did not change, and this may appear in a subsequent publication.
Predictors of outcome
It is striking that the negative effect of unemployment at baseline on HDRS and SF-36 scores at follow-up was as large as the positive effect of adding an SSRI to supportive care, which is consistent with previous research showing the important relationship between unemployment and depression. 35,37 Frank et al. ,106 in their trial of treating minor depression, found that remission was more likely among patients who were in employment.
Life events and difficulties have been found repeatedly to be related to the onset of depression40–42,107,108 and to recovery,44,109–111 but in this study neither provoking agents in the previous year nor ongoing severe interpersonal difficulties at baseline were significant predictors of outcome. Further exploration of life events and difficulties both before entry and during the course of the trial is ongoing. Initial exploration does suggest that the presence of a severe interpersonal difficulty at baseline may reduce the likelihood of remission to HDRS < 8 in the absence of a positive life event post baseline, so a positive life event during the course of treatment may act as a moderator, to increase the likelihood of remission. This requires further analysis and may appear in a subsequent publication. Further analysis is also planned of the nature of the supportive care patients reported that they received in the GP consultations through the PSAC questionnaire, and possible relationships between life events and difficulties, supportive care received, depressive symptoms and patient satisfaction.
Other studies of depression in primary care have shown important effects of psychosocial factors, in addition to those listed in Chapter 1. Walker et al. 112 found that psychosocial vulnerabilities, including a history of childhood emotional abuse and loneliness, were associated with a poorer response to a collaborative care intervention. More recently, Lyness et al. 113 reported that poorer subjective social support conferred a higher risk for poor outcome.
The outcome on the HDRS was worse for those with a greater number of physical symptoms at baseline. Rubinstein et al. 114 also found that fewer common physical symptoms at baseline predicted a better outcome at 6 months’ follow-up, along with a lower severity of depression symptoms at baseline, the presence of social support and having completed 3 months of antidepressants at sample entry. However, we found no evidence that a greater number of physical symptoms affected patient responses to treatment, which is in line with previous studies suggesting that patients with depression accompanying physical health problems can still benefit from antidepressant drug treatment. 54 It is interesting to note that the number of physical symptoms was not related to outcome on the BDI. This may be because the HDRS includes somatic symptoms of depression and so is likely to correlate with the BSI to an extent, whereas the BDI measures more cognitive aspects of depression.
Predictors of response to treatment
It is important to stress that the lack of significant interactions between the possible predictors and response to treatment means that we have not identified any ways in which GPs might make decisions about which patients to treat with antidepressants. The addition of an SSRI to supportive care improved outcome in terms of the HDRS whether or not the patients had high numbers of somatic symptoms, and whether or not the patient was unemployed, which implies that GPs should not base decisions on whether to treat a patient with an SSRI on the patient’s presentation with physical symptoms or their employment status.
Chapter 7 Conclusions
Implications for practice
The results of this study demonstrate that GP prescribing of SSRI antidepressants for patients with mild to moderate depression, on top of supportive care provided over four consultations in 12 weeks, is more effective than supportive care alone, and is cost-effective at the levels used by NICE to make judgements about recommending treatments within the NHS. However, the results do not support a policy of indiscriminate prescribing to all general practice patients with depression, and we should emphasise certain caveats.
First, our inclusion criteria included persistent symptoms of depression for at least 8 weeks. This study has not provided any evidence to support prescribing for patients with a shorter duration of symptoms. Current NICE guidance advises a period of watchful waiting before considering prescription of antidepressants, and our results support a policy of waiting until patients have had symptoms for at least 8 weeks, and then treating them with an SSRI if they have not improved, in line with NICE guidance.
Second, patients had to score at least 12 on the HDRS for inclusion which, while close to the mildest end of the spectrum of depression, does not include all patients diagnosed as depressed by their GPs. We excluded 47 patients out of 602 referred into the study as a result of HDRS scores of less than 12. We chose this threshold as it corresponded to the lower end of the severity range on the HDRS for which benefit has been shown in placebo-controlled trials. 20,25,31 Previous research has shown evidence of functional impairment due to very mild depression,12,13 right down to a level of 7 on the HDRS,115 but this study has not provided any evidence to support prescribing for very mild depression below a score of 12. This score on the HDRS is at the threshold level of severity for diagnosing mild major depressive disorder, as discussed in Chapter 1, and corresponds approximately to a score of 12 on the Patient Health Questionnaire, 9-item version (PHQ-9),116,117 or a score of 9 on the Hospital Anxiety and Depression Scale depression subscale (HADS-D). 116 These two measures are now commonly used to measure the severity of depression in UK practices as a result of the inclusion of incentives to measure severity in the UK GP contract quality and outcomes framework in April 2006. We can therefore recommend, on the basis of these findings, that SSRI antidepressants should be considered in someone who has been experiencing symptoms for at least 8 weeks and has a PHQ-9 score of 12 or more or a HADS-D score of 9 or more.
Given that there may be benefits to be gained from prescribing SSRIs for mild depression, we need to consider whether these benefits outweigh the possible adverse effects in any individual patient. It is important to consider the risk of overdose, as illustrated by two patients who took overdoses of paracetamol during the course of this trial, although fortunately none took an overdose of SSRIs. The side effects of medication are generally minor, as we found in this study, but occasionally can be severe and include, for example, the potentially fatal serotonin syndrome. Patients with epilepsy may suffer fits due to the lowering of the seizure threshold by antidepressant medication, which may stop them driving and cause them to lose their job. In addition to these physical risks of medication, prescribing may be perceived as ‘disposing’ of the patient, precluding a greater exploration of their life difficulties,118,119 and of non-drug strategies to tackle depression, although we found no evidence of differences between arms in reported discussion of non-drug strategies in this study. The increasing availability of non-drug treatment alternatives such as computerised CBT-based self-help15 and psychological therapies120 may obviate the need to risk prescribing for more and more practitioners in the future.
Implications for further research
More research is needed on the natural history of mild to moderate depression and predictors of chronicity because, although many patients recover within weeks in the absence of treatment, a significant proportion do not remit in the short term (more than 45% at 6 months in this study). Better ways of early identification of those who are less likely to recover in the short term would help GPs to target additional treatment or referral for psychological or psychiatric treatment to those more likely to need extra help.
More placebo-controlled studies of antidepressants for mild depression in primary care are needed, as the evidence base for the treatment of mild depression in particular is still relatively small. 11,23,84,95 More research is also needed into self-help, exercise, diet and novel non-drug treatments for mild depression, as the evidence base for non-drug treatments is also very small. 11
More research is required into the differences between the HDRS and BDI and other measures of depression, to explore whether they measure different aspects of depression and whether there are differences between them in sensitivity to change in relation to drug, psychological and other treatments. 103 This would help to inform the choice of the most appropriate measure for future trials. We intend to look at the elements of the HDRS and BDI in this study for a possible future publication.
More research is needed into supportive care or watchful waiting,11 to explore the therapeutic aspects, what supportive care should include and how to optimise it. We intend to look further into the relationship between reported consultation content, life events and difficulties and outcome in this study, including patient satisfaction. We will also carry out an exploratory factor analysis of underlying constructs in the MISS measure of satisfaction used in this study.
Finally, better measures of outcome for depression studies need to be developed, including patient-derived measures. The Psychological Outcome Profiles (PSYCHLOPS) measure developed at King’s College London is one such instrument, which is intended to measure change in those issues of importance to the individual patient or client, and is ideally suited to situations where clients present with varied mental health issues that might not be adequately captured by standardised instruments (see www.psychlops.org.uk).
Conclusion
Treatment with an SSRI plus supportive care is more effective than supportive care alone for patients with mild to moderate depression in UK primary care, at least for those with symptoms persisting for 8 weeks and with an HDRS score of 12 or more. The additional benefit is relatively small, and may be at least in part a placebo effect, but is probably cost-effective at the levels used by NICE to make judgements about recommending treatments within the NHS.
Acknowledgements
We wish to thank all the general practitioners who participated in the study, from the following practices:
3 Swans Surgery, Salisbury; Aldermoor Surgery, Southampton; Barton Surgery, Barton-on-Sea; Bath Lodge Surgery, Southampton; Bemerton Heath Surgery, Salisbury; Blackthorn Health Centre, Southampton; Burdwood Surgery, Thatcham; Chancellor House Surgery, Reading; Chawton House Surgery, Lymington; Chawton Park Surgery, Alton; Corbin Avenue Surgery, Ferndown; Cowplain Family Practice, Portsmouth; Cross Plain Surgery, Salisbury; Denmead Health Clinic, Waterlooville; Derry Down Clinic, Andover; Dr Caird & Partners, Farnborough; Dr Rahman & Partner, Aldershot; Dr Shad, Aldershot; Endless Street Surgery, Salisbury; Farnham Centre for Health, Farnham; Fordingbridge Surgery, Fordingbridge; Forton Medical Centre, Gosport; Fryern Surgery, Eastleigh; Gratton Surgery, Winchester; Hanway Group Practice, Portsmouth; Herbert Avenue Surgery, Poole; Highcliffe Medical Centre, Bournemouth; Holdenhurst Road Practice, Bournemouth; Hook Surgery, Hook; James Fisher Medical Centre, Bournemouth; Milton Park Practice, Portsmouth; New Street Surgery, Salisbury; Nightingale Practice, Romsey; Overton Surgery, Overton; Park Lane Surgery, Stubbington; Pinehill Surgery, Bordon; Providence Surgery, Bournemouth; Rowlands Castle Surgery, Portsmouth; Rowner Health Centre, Gosport; Sandford Surgery, Wareham; Shepherds Spring Medical Centre, Andover; Somers Town Health Centre, Portsmouth; Springfield Surgery, Godalming; St Lukes Surgery, Southampton; The Alma Partnership, Winton Health Centre, Bournemouth; The Barn Practice, Gillingham; The Chineham Medical Practice, Basingstoke; The Health Centre, Bognor Regis; The Oaklands Practice, Yately; The Old Orchard Surgery, Wilton; The Rooks Down Practice, Basingstoke; University Health Centre, Southampton; Victory Surgery, Portsmouth, Waterside Medical Centre, Gosport, Whalebridge Practice, Swindon; Wilton Health Centre; Barnes Surgery, Barnes; Bickersteth Road Surgery, Tooting; Boundfield Medical Centre, Catford; Bridge Lane Group Practice, Battersea; Downlands Surgery, Old Coulsdon; Fairview Medical Centre, Norbury; Hurley Clinic, Kennington Lane; Palace Road Surgery, Palace Road; Queens Road Partnership, New Cross; Rushey Green Group Practice, Lewisham; Sandmere Practice, Clapham; Selsdon Park Medical Centre, Sesldon; Surrey Docks Health Centre, Surrey Docks; Sydenham Green Health Centre, Sydenham; The Exchange Surgery, Streatham; The Lordship Lane Surgery, East Dulwich; The Surgery, Croydon; Torridon Road Medical Practice, Catford; Tudor Lodge Health Centre, Wimbledon; Violet Lane Medical Practice, Croydon; Warlingham Green Medical Practice, Warlingham; 30 Hillside Road, Huyton; 104 Woodplumpton Road, Preston; Aintree Park Group Practice, Orrell Park; Bousfield Surgery, Kirkdale; Brownlow Group Practice, Liverpool; Burnside Surgery, Bolton; Danebridge Medical Centre, Northwich; Dr CC Hulbert & Partners, Laurel Bank Surgery, Malpas; Dr C Holme & Partners, Handbridge Medical Centre, Chester; Eastview Surgery, Waterloo; Eccles Health Centre, Eccles; Grove Road Surgery, Wallasey; Haydock Medical Centre, St Helens; Holmes Chapel Health Centre, Cheshire; Kiltearn Medical Centre, Nantwich; Kings Park Surgery, Bootle; Leasowe Primary Care Centre, Wirral; Margaret Thompson Medical Centre, Speke; Parkfield Medical Centre, Wirral; Park Road Group Practice, Liverpool; Prenton Medical Centre, Wirral; Priory Medical Centre, Anfield; Princes Park Health Centre, Toxteth; Riverside Centre for Health, Toxteth; Rutherford Medical Centre, Mossley Hill; Speke Health Centre, Speke; Spring House Surgery, Bolton; The Halliwell Surgery, Bolton; The Orchard Surgery, Bromborough; The Strand Medical Centre, Bootle; The Surgery, Deepdale Road, Preston; The Surgery, Long Lane, Garston; The Surgery, Mather Avenue, Liverpool; Vauxhall Primary Health Care, Liverpool; Westminster Surgery, Ellesmere Port; Westmoreland Group Practice, Fazakerley; Wistaston Surgery, Crewe.
We also wish to acknowledge the help of Mauricio Moreno at the Institute of Psychiatry for data management, David Baldwin for the initial training of the researchers in the use of the HDRS, the Trial Steering Committee (Chair Debbie Sharp and members Linda Gask, Ros Corney and Sue Collinson), the Data Monitoring and Ethics Committee (Chair Michael King and members Michael Campbell and Sally Kerry), the Mental Health Research Network staff in the London, West and North West hubs for their help in promoting the study to practices, the Department of Health for funding the NHS service support costs for the GPs and, of course, the National Institute for Health Research Health Technology Assessment programme for providing the funding for the project.
Lastly, and most important of all, we wish to thank all the participating patients.
Contribution of authors
Tony Kendrick (Professor of Primary Care) was the Chief Investigator and was involved in the conception and design of the study, interpretation of data, drafting and revising the report and approving the final version. Judy Chatwin (Trial Co-ordinator) was involved in modifying the design of the study, data collection, analysis, drafting and revising the report and approving the final version. Chris Dowrick (Professor of Primary Medical Care), André Tylee (Professor of Primary Medical Care and Mental Health), Richard Morriss (Professor of Psychiatry and Community Mental Health), Robert Peveler (Professor of Liaison Psychiatry) and Tirril Harris (Visiting Research Fellow) were involved in the conception and design of the study, interpretation of data, drafting and revising the report and approving the final version. Morven Leese (Reader in Medical Statistics) and Paul McCrone (Reader in Health Economics) were involved in the conception and design of the study, analysis and interpretation of data, drafting and revising the report and approving the final version. Michael Moore (Senior Lecturer), Richard Byng (Senior Clinical Research Fellow), George Brown (Professor Emeritus), Mark Gabbay (Head of Division of Primary Care) and Tom Craig (Professor of Social and Community Psychiatry) were involved in modification of the design, interpretation of data, drafting and revising the report and approving the final version. Sophie Barthel (Research Associate) was involved in analysis and interpretation of data, drafting and revising the report and approving the final version. Helen Mander (Researcher), Adele Ring (Researcher), Vikki Kelly (Researcher) and Vuokko Wallace (Researcher) were involved in modification of the design, data collection, revising the report and approving the final version. Anthony Mann (Professor Emeritus) was involved in the conception and design of the study, revising the final report and approving the final version.
Publications
Chatwin J, Kendrick TR. Protocol for the THREAD (THREshold for AntiDepressants) study: a randomised controlled trial to determine the clinical and cost effectiveness of antidepressants plus supportive care, versus supportive care alone, for mild to moderate depression in UK general practice. BMC Fam Pract 2007;8(1):2.
Morriss R, Leese M, Chatwin J, Baldwin D. Inter-rater reliability of the Hamilton depression rating scale as a diagnostic and outcome measure of depression in primary care. J Affect Disord 2008;111(2)204–13.
Disclaimers
The views expressed in this publication are those of the authors and not necessarily those of the HTA programme or the Department of Health.
References
- Middleton N, Gunnell D, Whitley E, Dorling D, Frankel S. Secular trends in antidepressant prescribing in the UK, 1975–1998. J Public Health Med 2001;23:262-7.
- Rix S, Paykel ES, Lelliott P, Tylee A, Freeling P, Gask L, et al. Impact of a national campaign on GP education: an evaluation of the defeat depression campaign. Br J Gen Pract 1999;49:99-102.
- Anderson I. Antidepressant drug treatment in primary care: when, what and how?. J Prim Care Ment Health 2000;4:3-5.
- Martin RM, Hilton SR, Kerry SM, Richards NM. General practitioners’ perceptions of the tolerability of antidepressant drugs: a comparison of selective serotonin reuptake inhibitors and tricyclic antidepressants. BMJ 1997;314:646-51.
- Anderson IM, Nutt DJ, Deakin JFW. Evidence-based guidelines for treating depressive disorders with antidepressants: a revision of the 1993 British Association for Psychopharmacology guidelines. J Psychopharmacol 2000;14:3-20.
- World Health Organization . The ICD-10 Classification of Mental and Behavioural Disorders: Diagnostic Criteria for Research 1993.
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders DSM-IV-TR 2000.
- Ustun TB, Ayuso-Mateos JL, Chatterji S, Mathers C, Murray C. Global burden of depressive disorders in the year 2000. Br J Psychiatry 2004;184:386-92.
- Murray C, Lopez AD. Alternative projections of mortality and disability by cause 1990–2020: global burden of disease study. Lancet 1997;349:1498-504.
- Paykel ES, Priest RG. Recognition and management of depression in general practice: consensus statement. BMJ 1992;305:1198-202.
- National Collaborating Centre for Mental Health . Depression: Management of Depression in Primary and Secondary Care 2004.
- Judd LJ, Paulus MP, Wells KB, Rapaport MH. Socioeconomic burden of subsyndromal depressive symptoms and major depression in a sample of the general population. Am J Psychiatry 1996;153:1411-17.
- Rapaport MH, Judd LJ, Schettler PJ, Yonkers KA, Thase ME, Kupfer DJ, et al. A descriptive analysis of minor depression. Am J Psychiatry 2002;159:637-43.
- Moncrieff J, Pomerleau J. Trends in sickness benefits in Great Britain and the contribution of mental disorders. J Public Health Med 2000;2:59-67.
- Proudfoot J, Ryden C, Everitt B, Shapiro DA, Goldberg D, Mann A, et al. Clinical efficacy of computerised cognitive–behavioural therapy for anxiety and depression in primary care; randomised controlled trial. Br J Psychiatry 2004;185:46-54.
- Kendrick T. Why can’t GPs follow guidelines on depression? We must question the basis of the guidelines themselves. BMJ 2000;320:200-1.
- Anonymous . Mild depression in general practice: time for a rethink?. Drug Ther Bull 2003;41:60-4.
- Layard R. the Centre for Economic Performance Mental Health Policy Group . The Depression Report: A New Deal for Depression and Anxiety Disorders 2006.
- Hamilton M. Development of a rating scale for primary depressive illness. Br J Soc Clin Psychol 1967;6.
- Paykel ES, Hollyman JA, Freeling P, Sedgwick P. Predictors of therapeutic benefit from amitriptyline in mild depression: a general practice placebo-controlled trial. J Affect Disord 1988;14:83-95.
- Katon W, von Korff M, Lin E, Walker E, Simon GE, Bush T, et al. Collaborative management to achieve treatment guidelines. Impact on depression in primary care. JAMA 1995;273:1026-31.
- Peveler R, George C, Kinmonth A-L, Campbell M, Thompson C. Effect of antidepressant drug counselling and information leaflets on adherence to drug treatment in primary care: randomised controlled trial. BMJ 1999;319:612-15.
- Arroll B, MacGillivray S, Ogston S, Reid I, Sullivan F, Williams B, et al. Efficacy and tolerability of tricyclic antidepressants and SSRIs compared with placebo for treatment of depression in primary care: a meta-analysis. Ann Fam Med 2005;3:449-56.
- Barrett JE, Williams JW, Oxman TE, Katon W, Frank E, Hegel MT, et al. The treatment effectiveness project. A comparison of the effectiveness of paroxetine, problem-solving therapy, and placebo in the treatment of minor depression and dysthymia in primary care patients: background and research plan. Gen Hosp Psychiatry 1999;21:260-73.
- Barrett JE, Williams JW, Oxman TE, Frank E, Katon W, Sullivan M, et al. Treatment of dysthymia and minor depression in primary care: a randomized trial in patients aged 18 to 59 years. J Fam Pract 2001;50:405-12.
- Williams JW, Barrett J, Oxman TE, Frank E, Katon W, Sullivan M, et al. Treatment of dysthymia and minor depression in primary care: a randomized controlled trial in older adults. JAMA 2000;284:1519-26.
- de Lima MS, Hotopf M, Wessely S. The efficacy of drug treatments for dysthymia: a systematic review and meta-analysis. Psychol Med 1999;29:1273-89.
- Judd LJ, Rapaport MH, Yonkers KA, Rush AJ, Frank E, Thase ME, et al. Randomized, placebo-controlled trial of fluoxetine for acute treatment of minor depressive disorder. Am J Psychiatry 2004;161:1864-71.
- Grundy CT, Lambert MJ, Grundy EM. Assessing clinical significance: application to the Hamilton rating scale for depression. J Ment Health 1996;5:25-33.
- Potts MK, Daniels M, Burnam MA, Wells KB. A structured interview version of the Hamilton depression rating scale; evidence of reliability and versatility of administration. J Psychiatr Res 1990;24:335-50.
- Perahia D, Kajdasz DK, Walker DJ, Raskin J, Tylee A. Duloxetine 60mg once daily in the treatment of milder major depressive disorder. Int J Clin Pract 2006;60:613-20.
- Montgomery SA. Guidelines for treating depressive illness with antidepressants. J Psychopharmacol 1993;7:19-23.
- School of Public Health UoL, Centre for Health Economics UoY, Research Unit RCoP . Effective Health Care Bulletin: He Treatment of Depression in Primary Care 1993.
- Regier DA, Farmer ME, Rae DS, Myers JK, Kramer M, Robins L, et al. One-month prevalence of mental disorders in the United States and sociodemographic characteristics: the epidemiologic catchment area study. Acta Psych Scand 1993;88:35-47.
- Weich S, Lewis G. Poverty, unemployment, and common mental disorders: population based cohort study. BMJ 1998;317:115-19.
- Bruce M, Takeuchi DT, Leaf PJ. Poverty and psychiatric status: longitudinal evidence from the New Haven epidemiologic catchment area study. Arch Gen Psychiatry 1991;48:470-4.
- Kessler RC, Turner JB, House J. Intervening processes in the relationship between unemployment and health. Psychol Med 1987;17:949-61.
- Romans SE, Walton VA, McNoe B, Herbison GP, Mullen PE. Otago women’s health survey 30-month follow-up I: onset patterns of non-psychotic psychiatric disorder. Br J Psychiatry 1993;163:733-8.
- Platt S, Martin C, Hunt S, Goldberg D, Tantam D. The public health impact of mental disorder. Toronto: Hogrefe and Huber; 1990.
- Brown GW, Harris T. Social origins of depression: a study of psychiatric disorder in women. London: Tavistock Publications; 1978.
- Brown GW, Bifulco A, Harris T. Life events, vulnerability and onset of depression: some refinements. Br J Psychiatry 1987;150:30-42.
- Brown GW, Harris TO, Hepworth C. Loss, humiliation and entrapment among women developing depression: a patient and non-patient comparison. Psychol Med 1995;25:7-21.
- Oldehinkel AJ, Ormel J, Neeleman J. Predictors of time to remission from depression in primary care patients: do some people benefit more from positive life change than others?. J Abnorm Psychol 2000;109:299-307.
- Harris T, Brown GW, Robinson R. Befriending as an intervention for chronic depression among women in an inner city. 2. Role of fresh start experiences and baseline psychosocial factors in remission from depression. Br J Psychiatry 1999;174:225-32.
- Ronalds C, Creed R, Stone K, Webb S, Tomenson B. Outcome of anxiety and depressive disorders in primary care. Br J Psychiatry 1997;171:427-33.
- Dowrick C, Buchan I. Twelve month outcome of depression in general practice: does detection or disclosure make a difference?. BMJ 1995;311:1274-6.
- Goldberg D, Privett M, Ustun B, Simon G, Linden M. The effects of detection and treatment on the outcome of major depression in primary care: a naturalistic study in 15 cities. Br J Gen Pract 1998;48:1840-4.
- Dowrick C, Dunn G, Ayuso-Mateos JL, Dalgard OS, Page H, Lehtinen V, et al. Problem solving treatment and group psychoeducation for depression: multicentre randomised controlled trial. BMJ 2000;321:1450-4.
- Lam DH, Green B, Power MJ, Checkley S. The impact of social cognitive variables on the initial level of depression and recovery. J Affect Disord 1994;32:75-83.
- Tylee AT, Freeling P, Kerry S. Why do general practitioners recognize major depression in one woman patient yet miss it in another?. Br J Gen Pract 1993;43:327-30.
- Mumford DB, Bavington JT, Bhatnagar KS, Hussain Y, Mirza S, Naraghi MM. The Bradford somatic inventory: a multi-ethnic inventory of somatic symptoms reported by anxious and depressed patients in Britain and the Indo-Pakistan subcontinent. Br J Psychiatry 1991;158:379-86.
- Garcia-Campayo J, Campos R, Marcos G, Perez-Echeverria MJ, Lobo A. Somatisation in primary care in Spain: ii. Differences between somatisers and psychologisers. Br J Psychiatry 1996;168:348-53.
- Parker G. Evaluating treatments for the mood disorders: time for the evidence to get real. Aust N Z J Psychiatry 2004;38:408-14.
- Gill D, Hatcher S. Antidepressants for depression in medical illness. Oxford: Cochrane Library Issue 2; 2002.
- Fallon BA. Pharmacotherapy of somatoform disorders. J Psychosomat Res 2004;56:455-60.
- Robbins J, Kirmayer L. Attributions of common somatic symptoms. Psychol Med 1991;21:1029-45.
- Morriss RK, Gask L, Ronalds C, Downes-Grainger E, Thompson H, Goldberg D. Clinical and patient satisfaction outcomes of a new treatment for somatized mental disorder taught to general practitioners. Br J Gen Pract 1999;49:263-7.
- Babor TF, Grant M. From clinical research to secondary prevention: international collaboration in the development of the alcohol use disorders identification test (AUDIT). Alcohol Health Res World 1989;13:371-4.
- Maier W, Bech P, Coppen A. The Hamilton scales. Berlin Heidelberg: Springer-Verlag; 1990.
- Paykel ES, Bech P, Coppen A. The Hamilton scales. Berlin Heidelberg: Springer-Verlag; 1990.
- Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry 1961;4:53-61.
- Brown C, Schulberg H, Madonia MJ. Assessment of depression in primary care practice with the Beck depression inventory and the Hamilton rating scale for depression. Psychol Assess 1995;7:59-65.
- Ware JE, Sherbourne CD. The MOS 36-item short form health survey (SF-36). Med Care 1992;30:473-81.
- Wolf MH, Putnam SM, James SA, Stiles WB. The medical interview satisfaction scale: development of a scale to measure patient perceptions of physician behaviour. J Behav Med 1978;1:391-40.
- Howie J, Heaney DJ, Maxwell M, Walker J. A comparison of a patient enablement instrument (PEI) against two established satisfaction scales as an outcome measure of primary care consultations. Fam Pract 1998;15:165-71.
- Kinnersley P, Stott N, Peters TJ, Harvey I, Hackett P. A comparison of methods for measuring patient satisfaction with consultations in primary care. Fam Pract 1996;13:41-5.
- Little P, Dorward M, Warner G, Moore M, Stephens K, Senior J, et al. Randomised controlled trial of effect of leaflets to empower patients in consultations in primary care. BMJ 2004;328:441-4.
- Kinnersley P, Stott N, Peters TJ, Harvey I. The patient-centredness of consultations and outcome in primary care. Br J Gen Pract 1999;49:711-16.
- Beecham J, Knapp M, Thornicroft G, Brewin CR, Wing JK. Measuring mental health needs. London: Gaskell; 1992.
- Mistry H, Buxton M, Longworth L, Chatwin J, Peveler R. Comparison of GP records and patient self-report questionnaires for estimation of costs. Eur J Health Econ 2005;56:261-6.
- Wing JK, Babor TF, Brugha T, Burke J, Cooper JE, Giel R, et al. SCAN. Schedules for clinical assessment in neuropsychiatry. Arch Gen Psychiatry 1990;47:589-93.
- Morisky DE, Green LW, Devine D. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care 1986;24:67-74.
- Hollyman JA, Freeling P, Paykel ES, Bhat A, Sedgewick P. Double-blind placebo-controlled trial of amitriptyline among depressed patients in general practice. J R Coll Gen Pract 1988;38:393-7.
- Royal College of General Practitioners . Key Demographic Statistics from UK General Practice 2006. www.rcgp.org.uk/pdf/ISS_FACT_06_KeyStats.pdf.
- Curtis L. Unit costs of health and social care. Canterbury: Personal Social Services Research Unit; 2007.
- British Medical Association, Royal Pharmaceutical Society of Great Britain . British National Formulary 2007.
- Department of Health . NHS Reference Costs 2005. www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_062884 (accessed 4 April 2008).
- Brazier JE, Roberts JF, Deverill MD. The estimation of a preference based measure of health from the SF-36. J Health Econ 2002;21:271-92.
- Richardson G, Manca A. Calculation of quality adjusted life years in the published literature: a review of methodology and transparency. Health Econ 2004;13:1203-10.
- Panorama . Seroxat: Emails from the Edge 2003.
- Duff G. Safety of Seroxat (paroxetine) in Children and Adolescents under 18 Years – Contraindication in the Treatment of Depressive Illness – Epinet Message 2003.
- Committee on Safety of Medicines . Selective Serotonin Reuptake Inhibitor (SSRI) Antidepressants 2004.
- Panorama . Secrets of the Drug Trials 2007.
- MacGillivray S, Arroll B, Hatcher S, Ogston S, Reid I, Sullivan F, et al. Efficacy and tolerability of selective serotonin reuptake inhibitors compared with tricyclic antidepressants in depression treated in primary care: systematic review and meta-analysis. BMJ 2003;326.
- Donoghue J, Tylee A, Wildgust H. Cross sectional database analysis of antidepressant prescribing in general practice in the United Kingdom, 1993–5. BMJ 1996;313:861-2.
- Donoghue JM, Tylee A. The treatment of depression: prescribing patterns of antidepressants in primary care in the UK. Br J Psychiatry 1996;168:164-8.
- Dunn RL, Donoghue JM, Ozminski RJ, Stephenson D, Hylan TR. Longitudinal patterns of antidepressant prescribing in primary care in the UK: comparison with treatment guidelines. J Psychopharmacol 1999;13:136-43.
- Dunn G, Maracy M, Dowrick C, Ayuso-Mateos JL, Dalgard OS, Page H, et al. Estimating psychological treatment effects from a randomised controlled trial with both non-compliance and loss to follow-up. Br J Psychiatry 2003;183:323-31.
- Age Concern . Undiagnosed, Untreated, at Risk 2008.
- Simon GE, Katon W, Rutter C, von Korff M, Robinson P, Bush T, et al. Impact of improved depression treatment in primary care on daily functioning and disability. Psychol Med 1998;28:693-701.
- Lin E, von Korff M, Russo J, Katon W, Simon GE, Unutzer J, et al. Can depression treatment in primary care reduce disability? A stepped care approach. Arch Fam Med 2000;9:1052-8.
- Kendrick T, Peveler R, Longworth L, Baldwin D, Moore M, Chatwin J, et al. Cost-effectiveness and cost-utility of tricyclic antidepressants, selective serotonin reuptake inhibitors and lofepramine – randomised controlled trial. Br J Psychiatry 2006;188:337-45.
- Hermens M, van Hout H, Terluin B, Ader HJ, Penninx B, van Marwijk H, et al. Clinical effectiveness of usual care with or without antidepressant medication for primary care patients with minor or mild-major depressi on: a randomized equivalence trial. BMC Med 2007;5. 10.1186/1741--7015‐5-36.
- Montgomery SA, Åsberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry 1979;134:382-9.
- Kirsch I, Deacon BJ, Huedo-Medina TB, Scoboria A, Moore TJ, Johnson BT. Initial severity and antidepressant benefits: a meta-analysis of data submitted to the Food and Drug Administration. PLoS Med 2008;5.
- Elkin I, Shea T, Watkins JT, Imber SD, Sotsky SM, Collins JF, et al. National Institute of Mental Health treatment of depression collaborative research program: general effectiveness of treatments. Arch Gen Psychiatry 1989;46:971-82.
- Khan A, Leventhal R, Khan S, Brown WA. Severity of depression and response to antidepressants and placebo: an analysis of the Food and Drug Administration database. J Clin Psychopharmacol 2002;22:40-5.
- Frank J. Persuasion and healing: a comparative study of psychotherapy. New York: Schocken Books; 1974.
- Salmon P, Peters S, Stanley I. Patients’ perceptions of medical explanations for somatisation disorders: qualitative analysis. BMJ 1999;318:372-6.
- Johnston O, Kumar S, Kendall K, Peveler R, Gabbay J, Kendrick T. Qualitative study of depression management in primary care: GP and patient goals, and the value of listening. Br J Gen Pract 2007;57:872-9.
- Tennant P. Antidepressant benefits: misinferance from ordinal scales? (Rapid response.). BMJ 2008. www.bmj.com/cgi/eletters/336/7642/466#191157.
- Svanborg P, Asberg M. A comparison between the Beck depression inventory (BDI) and the self-rating version of the Montgomery Asberg depression rating scale (MADRS). J Affect Disord 2001;64:203-16.
- Uher R, Farmer A, Maier W, Rietschel M, Hauser J, Marusic A, et al. Measuring depression: comparison and integration of three scales in the GENDEP study. Psychol Med 2008;38:289-300.
- Beck AT, Steer RA, Brown GK. Beck depression inventory®–II (BDI®–II). Oxford: Pearson UK; 1996.
- Peveler R, Kendrick T, Buxton M, Longworth L, Baldwin D, Moore M, et al. A randomised controlled trial to compare the cost-effectiveness of tricyclic antidepressants, selective serotonin reuptake inhibitors and lofepramine. Health Technol Assess 2005;9.
- Frank E, Rucci P, Katon W, Barrett J, Williams JW, Oxman T, et al. Correlates of remission in primary care patients treated for minor depression. Gen Hosp Psychiatry 2002;24:12-9.
- Brown GW, Andrews B, Harris TO, Adler Z, Bridge L. Social support, self-esteem and depression. Psychol Med 1986;16:813-31.
- Brown GW, Adler Z, Bifulco A. Life events, difficulties and recovery from chronic depression. Br J Psychiatry 1988;152:487-98.
- Brown GW, Lemyre L, Bifulco A. Social factors and recovery from anxiety and depressive disorders. A test of specificity. Br J Psychiatry 1992;161:44-5.
- Brown GW, Moran P. Clinical and psychosocial origins of chronic depressive episodes. I: A community survey. Br J Psychiatry 1994;165:447-56.
- Brown GW, Harris TO, Hepworth C, Robinson R. Clinical and psychosocial origins of chronic depressive episodes. II: A patient enquiry. Br J Psychiatry 1994;165:457-65.
- Walker EA, Katon W, Russo J, von Korff M, Lin E, Simon G, et al. Predictors of outcome in a primary care depression trial. J Gen Intern Med 2000;15:859-67.
- Lyness JM, Heo M, Datto CJ, Ten Have TR, Katz IR, Drayer R, et al. Outcomes of minor and subsyndromal depression among elderly patients in primary care settings. Ann Intern Med 2006;144:496-504.
- Rubinstein LV, Rayburn NR, Keeler EB, Ford DE, Rost KM, Sherbourne CD. Predicting outcomes of primary care patients with major depression: development of a depression prognosis index. Psychiatr Serv 2007;58:1049-56.
- Mintz J, Mintz LI, Arruda MJ, Hwang SS. Treatments of depression and the functional capacity to work. Arch Gen Psychiatry 1992;49:761-8.
- Lowe B, Spitzer RL, Grafe K, Kroenke K, Quenter A, Zipfel S, et al. Comparative validity of three screening questionnaires for DSM-IV depressive disorders and physicians’ diagnoses. J Affect Disord 2004;78:131-40.
- Gilbody SM, Richards D, Barkham M. Diagnosing depression in primary care using self-completed instruments: UK validation of PHQ-9 and CORE-OM. Br J Gen Pract 2007;57:650-2.
- Dowrick C. Beyond depression. A new approach to understanding and management. Oxford: Oxford University Press; 2004.
- May C, Allison G, Chapple A, Chew-Graham C, Dixon C, Gask L, et al. Framing the doctor–patient relationship in chronic illness: a comparative study of general practitioners’ accounts. Sociol Health Illness 2004;26:135-58.
- Layard R. The Centre for Economic Performance’s Mental Health Policy Group . The Depression Report: A New Deal for Depression and Anxiety Disorders 2006.
Appendix 1 Initial letter to GPs
Version 3 5/7/04
Dear Dr
Trial of SSRIs for mild to moderate depression in primary care
We would like your help with an important study of treatment for depression. This project has been funded by the NHS R&D Health Technology Assessment programme and we are aiming to recruit patients from general practices around three centres: Southampton, London (co-ordinated by the Institute of Psychiatry and King’s College London) and Liverpool.
What is the research question?
Current clinical guidelines recommend antidepressant medication as first-line treatment for depression in primary care, at least if patients fulfil criteria for major depressive disorder. However, as you know, antidepressants are often prescribed for depressive symptoms below the threshold for major depression. There has been relatively little research in primary care to guide us on the severity threshold at which antidepressants should be offered. Another issue that needs to be addressed is whether predictors of response to antidepressant treatment can be identified, to help us decide which patients should be offered them.
To address these questions we will carry out a randomised controlled trial of SSRIs versus supportive care alone, measuring possible predictors of response at baseline.
What would you have to do?
We would ask you to refer to the study patients that you find to be depressed in your surgery consultations, for whom the decision whether or not to prescribe an antidepressant is uncertain (please see the enclosed sheet giving inclusion and exclusion criteria). To avoid asking too much of you in busy appointment slots, we would like you simply to outline the nature of the study, hand out an information sheet describing the trial and ask whether the patient is willing to see a researcher to discuss possible enrolment. Patients referred to the researcher (by fax, at your convenience) will be contacted within a few days, given more information in person about the study, and asked for their consent in writing (please see the enclosed patient information sheet).
Patients included in the study would need a follow-up consultation arranged with you two weeks after the initial consultation, to begin treatment if appropriate, then further follow-ups two, four, eight, and twelve weeks after the second consultation. You would be asked to prescribe an SSRI for those randomised to the active treatment arm, and to give supportive care to those in the non-drug arm, in follow-up 10-minute surgery appointments. Patients in both arms may be referred for counselling if you wish. If patients in the non-drug arm become clinically worse, you will be free to prescribe antidepressant drugs if this is indicated, in your judgement. Patients in the SSRI arm should be treated for four months after recovery.
How much work is involved?
We hope that you might recruit between two and four patients for the study, over a 6 month period, although the study will actually be accepting patients for 15 months and should you wish to continue, your involvement would be much appreciated. Your practice would be paid NHS R&D service support costs for the extra consultations involved. This would be at locum rates as advertised in Medeconomics. There would also be payment for your staff time spent retrieving the patients’ medical records for the researchers, at the end of the study.
What do you need to do next?
Please would you think about possible involvement in this study, and discuss it with your partners. They do not have to be involved too, if you do agree to take part yourself. We will telephone your Practice Manager in two weeks to see whether you might be interested. If you are interested, we would like to come and describe the study to you in more detail, and answer any questions you may have.
We hope that you will consider joining us in this important study which should establish the threshold of severity for the prescription of antidepressants in general practice, including identifying possible predictors of patient response. Such information is vital for our day to day practice.
We look forward to discussing this further with you.
Best wishes.
Yours sincerely
Tony Kendrick
Appendix 2 Summary sheet for GPs
Version 3
Dated 5/7/04
STUDY OF SSRIs PLUS SUPPORTIVE CARE vs SUPPORTIVE CARE ALONE FOR MILD TO MODERATE DEPRESSION IN PRIMARY CARE
(THREshold for AntiDepressants STUDY)
The purpose of the study is to consider whether treatment with an SSRI plus supportive care is more effective and cost-effective than supportive care alone. If it is more effective, does this apply across the whole range of severity of symptoms of mild depression? The study will also consider what patient factors might predict a beneficial response.
Inclusion criteria
Patients attending surgery who:
-
are found to be depressed and potentially in need of antidepressant treatment
-
have had symptoms of depression for at least four weeks
-
are aged 18 years and above
-
have somatic as well as psychological symptoms.
Exclusion criteria
The following patients are not suitable for inclusion:
-
Those with depression that definitely requires treatment with antidepressants
-
Those already in contact with psychiatric services
-
Those already receiving cognitive–behavioural treatment or counselling
-
Those for whom substance misuse requires specific treatment
-
Those with any active suicidal intentions
-
Pregnant or breast-feeding women, or women of child-bearing age without satisfactory contraception
-
Those considered to be too physically unwell to participate
-
House-bound patients
-
Those without the spoken and written language skills necessary to take part
-
Temporary residents
-
Patients where SSRIs are contraindicated
-
Those who have received treatment for depression within the previous 12 months
-
Those who continue to take St John’s Wort.
Recruitment procedure
The GP should simply outline the nature of the study, hand out the information sheet describing the trial, and determine whether the patient is willing to see a researcher to discuss possible randomisation.
Patients who indicate that they are willing to discuss participation in the trial should be referred by the GP, by fax, to the researcher at the local centre, giving the patient’s name and contact details. Patients referred to the study will be contacted by a researcher at each site, as soon as possible after referral, usually within two days but always within the week, to arrange an initial face to face contact, either at the patient’s home or at the doctor’s surgery, if the patient prefers. The researcher will explain the study procedures in detail to the patient, give written information, and then visit one week later to ask for their informed consent in writing to participate.
Patient involvement
Patients will be interviewed and will complete questionnaires, including questions about their sociodemographic details, depressive symptoms, social functioning, life events, depressive thoughts, physical symptoms, social support and quality of life.
What happens after the assessment interview?
If the patient is suitable for inclusion in the study then:
-
the patient is randomised
-
a copy of the consent form and allocated treatment arm are faxed through to the practice
-
the GP needs to see the patient about 2 weeks after referral to the study.
If the patient is unsuitable for inclusion in the study, a fax will be sent to the practice informing them of the reasons why the patient could not be randomised and if they will be reassessed at a later date or not.
If the patient is undecided about participation but is willing to be contacted at a later date, a fax will be sent saying that the patient is agreeable to being contacted again in 4 weeks.
GP INVOLVEMENT
Patients in both arms will need to be seen for review of symptoms at follow-up appointments 2, 4, 8 and 12 weeks after randomisation. Those in the supportive care-alone arm should not usually be prescribed antidepressants, since the aim of the study is to determine whether this practice is necessary in milder depression, but this may be over-ridden if the patient’s depression worsens and in the GP’s clinical judgement the patient needs drug treatment.
Guidelines
If the patient has been randomised to SSRIs then the following guidelines are suggested:
| Initial consultation following randomisation | 2 week follow-up | 4 week follow-up | 8 week follow-up |
|---|---|---|---|
| Discuss the outcome of the randomisation with the patient, choose and prescribe an appropriate SSRI and carry out the consultation in your usual way | Address any side effects and re-emphasise that treatment often takes a few weeks to work and should not be discontinued without discussion | If the patient has not responded then consider increasing the dose, assuming no intolerable side effects | If the treatment is still unsuccessful then it is suggested that the patient be changed to an alternative drug |
If the treatment is successful, it is suggested that treatment is continued for 4 months after recovery.
| Local Researcher: | Study Co-ordinator: Judy Chatwin |
|---|---|
| Helen Mander (Southampton) Phone | Phone or fax: |
| Vuokko Wallace (London) Phone | Mobile phone: |
| Adele Ring (Liverpool) Phone | E-mail: |
| <Study web address> | |
Appendix 3 Consent to be contacted by researcher
Appendix 4 Participant information sheet
Version 5: 5/7/04
Study of antidepressants for mild to moderate depression
You are being invited to take part in a research study. Before you decide it is important for you to understand why the research is being done and what it will involve. Please take time to read the following information carefully and discuss it with others if you wish. Ask us if there is anything that is not clear or if you would like more information. Take time to decide whether or not you wish to take part. Thank you for reading this.
What is the purpose of the study?
We know antidepressants work for people with more severe forms of depression. They are also being prescribed more in recent years for milder forms of depression, but we don’t know if they are necessary in these milder cases. It may be that people with mild depression get better just as quickly with support from their GP and/or counselling from a practice counsellor. It is important for us to know whether the many patients seen by GPs with mild to moderate depression should be offered antidepressants. This three year study aims to find the answer to this question, to guide GPs in their practice in future.
Why have you been chosen?
The symptoms you have described to your GP, such as low mood, tiredness, negative thoughts and sleep difficulties are features of what doctors call mild to moderate depression. We recognise that often they can also be seen as an understandable response to life’s difficulties. Your GP would like you to discuss possibly taking part in this study with a member of the research team, who will contact you within the next week. Altogether 300 people will join the study.
What is mild to moderate depression?
Most people have changes in mood throughout each day. Most people also have days or even weeks when their mood is lower than usual. Such disturbances of mood are usually mild and pass with time. Occasionally low mood may last longer and, if you seek help, your GP might consider a diagnosis of mild depression. We recognise that some people may feel ‘down’ or ‘stressed’ but might not consider themselves to be depressed. Depression is defined clinically by the number of symptoms (see below) that are present; they have to be there for at least two weeks. Moderate and severe depression is distinguished from mild depression because the symptoms are worse and have more of an effect on everyday life. Your GP thinks that the symptoms you are experiencing are in the mild end of the spectrum and are different from severe depression. This spectrum is represented in the diagram below.

What are the symptoms of mild to moderate depression?
Depression affects people in different ways but is generally characterised by a persistently low mood or lack of enjoyment. Other symptoms sufferers often describe include:
-
Tiredness and lack of energy
-
Poor sleep
-
Changes in appetite
-
Irritability
-
Poor concentration
-
Loss of interest and motivation
-
Thinking too much about negative things or needless worry
-
Physical symptoms such as back or neck pain, churning stomach or palpitations
Do you have to take part?
It is up to you to decide whether or not to take part. A member of the research team will discuss this with you, taking as long as you need, within the next week. If you do decide to take part you will be asked to sign a consent form. You will still be free to withdraw at any time and without giving a reason. If you decide not to take part, or to withdraw at any time, this will not affect the care you receive from your GP or other health professionals involved in your care.
What will happen to you if you take part?
First of all, you will be interviewed by the researcher, either at your doctor’s practice, or at your home, or at another convenient place, at a time convenient to you. This interview will take approximately 1½ hours, and if necessary can be completed over two visits. The interview will include questions about your age, occupation, marital status, home background, education, past history, current symptoms, quality of life, and recent life events which might have led to depression. We would like to audiotape part of the interview, with your permission, to make sure we have sufficient detail about the context and meaning to you of any recent life events which might have contributed to depression.
Following this initial interview, a researcher from the study will contact you to tell you whether or not you are being asked to take the antidepressant, you will also be asked to return to see your GP. Whether you are in the group to be prescribed an antidepressant, or in the group to be followed up with supportive care alone, will be determined by a computer which has no information about you – that is, by chance. You have a one in two chance of being prescribed antidepressant medication.
What do you have to do?
If you are put into the group to be given an antidepressant, we would like you to take this medication regularly, each day, (it often takes two to three weeks to start working). Whichever of the two groups you are in, we would also like you to see your GP for further check-ups after 2, 4, 8, and 12 weeks.
Twelve weeks after the start of your involvement in the study you will be interviewed again by the researcher, who will ask you about your symptoms, how these have affected your life, and the treatments you have received. This interview should take around 1 hour. A further research interview, with similar questions, lasting around an hour and a half, will then take place six months after the start of the study. Your involvement would then be finished. At the end of six months, sections of your general practice medical records would be looked at by the researcher to check what treatment you have received.
What is the medicine being tested?
A type of antidepressant known as a selective serotonin reuptake inhibitor, or SSRI. These are antidepressant drugs which are licensed for use in depression and have been in regular use in the UK for several years – they are not experimental treatments. We know they are generally very safe drugs which usually cause few side-effects. Recognised side-effects include nausea, stomach ache, diarrhoea or constipation, changes in appetite, and changes in the pattern of sleep. Less common side effects include nervousness, headache, tremor, dizziness, drowsiness, rashes, joint pains, and sexual difficulties. Rare side effects include retention of urine, visual disturbances, changes in blood sugar, fever, abnormal bleeding, hair loss, and possibly aggressive behaviour.
If you are put in the group asked to take an antidepressant, and you suffer any symptoms you think might be side-effects, please mention these to your GP at the follow-up appointments, or sooner if you are concerned, by contacting your GP’s practice. If you suffer mild side-effects, such as an upset stomach, we would like you to continue taking the medicine if you are able. If you are in doubt, stop taking it and discuss it with your GP at the next follow-up appointment.
What are the possible disadvantages and risks of taking part?
If you are put into the antidepressant treatment group, the main risk is that of developing side-effects, as above. However your GP will be asking you about these effects during the follow-up, and if necessary will stop giving you the medication, to stop you suffering the side-effects.
What are the possible benefits of taking part?
If you are put into the antidepressant group, it is possible that you may recover from your depression more quickly. However, we do not know if this is the case – the study is designed to find this out. We hope that the supportive care you receive from your GP and/or counsellor, whichever group you are put into, will help you get better quickly in any case.
The information we get from this study may help us to treat future patients with mild to moderate depression better.
What if new information becomes available?
Sometimes during the course of a research project, new information becomes available about the treatment that is being studied. If this happens, your GP will tell you about it and discuss whether you want to continue in the study. If you decide to withdraw your GP will arrange for your care to be continued in the usual way. If you decide to continue in the study you will be asked to sign an updated consent form.
Confidentiality
All information which is collected about you during the course of the research will be kept strictly confidential; the only exception would be if the interview revealed a significant risk of harm to yourself or others, in which case information may be fed back to your doctor but only after discussion with you. Any information about you which leaves the practice will have your name and address removed so that you cannot be recognised from it.
What will happen to the results of the study?
The results should be published in a medical journal within 18 months of the end of the study. They will also be fed back to your GP. You can obtain a copy of the results from the research team, through your GP. You will not be identified in any report or publication arising from the study.
Who is organising and funding the study?
The study has been funded by the Department of Health, through the National Coordinating Centre for Health Technology Assessment. It has been organised by the Universities of Southampton, London and Liverpool. Your doctor is not being paid anything extra for including you in this study, beyond the usual costs of the consultations arranged for your follow-up.
Who has reviewed the study?
The study has been reviewed and approved by the Local Research Ethics Committee.
Contact for further information
| Study Co-ordinator | Phone | |
| Local Researcher | (Southampton) | Phone |
| Local Researcher | (London) | Phone |
| Local Researcher | (Liverpool) | Phone |
Appendix 5 Consent form to participate
Appendix 6 Consent form if undecided
Appendix 7 Fax to GP indicating randomisation arm
Appendix 8 Fax to GP – patient not suitable for study
Appendix 9 Hamilton Depression Rating Scale (HDRS): 17-item interview
Appendix 10 Beck Depression Inventory (BDI)
Referral No. Randomisation ID.
Timepoint:
Here are 21 groups of statements. Please read each group carefully. Then pick out the one statement in each group which best describes the way you have been feeling in the PAST WEEK, INCLUDING TODAY. Circle the number beside the statement you picked. If several statements in the group seem to apply equally well, circle each one. Be sure to read all the statements in each group before making your choice.
| 1. | I do not feel sad | 0 | 2. | I am not particularly discouraged about the future | 0 |
| I feel sad | 1 | I feel discouraged about the future | 1 | ||
| I am sad all the time and I can’t snap out of it | 2 | I feel I have nothing to look forward to | 2 | ||
| I am so sad or unhappy that I can’t stand it | 3 | I feel that the future is hopeless and that things cannot improve | 3 | ||
| 3. | I do not feel like a failure | 0 | 4. | I get as much satisfaction out of things as I used to | 0 |
| I feel I have failed more than the average person | 1 | I don’t enjoy things the way I used to | 1 | ||
| As I look back on my life, all I can see is a lot of failures | 2 | I don’t get real satisfaction out of anything anymore | 2 | ||
| I feel I am a complete failure as a person | 3 | I am dissatisfied or bored with everything | 3 | ||
| 5. | I don’t feel particularly guilty | 0 | 6. | I don’t feel I am being punished | 0 |
| I feel guilty a good part of the time | 1 | I feel I may be punished | 1 | ||
| I feel quite guilty most of the time | 2 | I expect to be punished | 2 | ||
| I feel guilty all of the time | 3 | I feel I am being punished | 3 | ||
| 7. | I don’t feel disappointed in myself | 0 | 8. | I don’t feel I am any worse than anyone else | 0 |
| I am disappointed in myself | 1 | I am critical of myself for my weaknesses or mistakes | 1 | ||
| I am disgusted with myself | 2 | I blame myself all the time for my faults | 2 | ||
| I hate myself | 3 | I blame myself for everything bad that happens | 3 | ||
| 9. | I don’t have any thoughts of killing myself | 0 | 10. | I don’t cry any more than usual | 0 |
| I have thoughts of killing myself, but I would not carry them out | 1 | I cry more now that I used to | 1 | ||
| I would like to kill myself | 2 | I cry all the time now | 2 | ||
| I would kill myself if I had the chance | 3 | I used to be able to cry but now I can’t cry even though I want to | 3 | ||
| Date completed | |||||
| 11. | I am no more irritated now than I ever am | 0 | 12. | I have not lost interest in other people | 0 |
| I get annoyed or irritated more easily | 1 | I am less interested in other people than I used to be | 1 | ||
| I feel irritated all the time now | 2 | I have lost most of my interest in other people | 2 | ||
| I don’t get irritated at all by the things that used to irritate me | 3 | I have lost all of my interest in others | 3 | ||
| 13. | I make decisions about as well as I ever could | 0 | 14. | I don’t feel I look any worse than I used to | 0 |
| I put off making decisions more than I used to | 1 | I am worried that I am looking old or unattractive | 1 | ||
| I have greater difficulty in making decisions than before | 2 | I feel there are permanent changes in my appearance that make me look unattractive | 2 | ||
| I can’t make decisions at all any more | 3 | I believe that I look ugly | 3 | ||
| 15. | I can work about as well as before | 0 | 16. | I can sleep as well as I used to | 0 |
| It takes extra effort to get started at doing something | 1 | I don’t sleep as well as I used to | 1 | ||
| I have to push myself very hard to do anything | 2 | I wake up 1–2 hours earlier than usual and find it hard to get back to sleep | 2 | ||
| I can’t do any work at all | 3 | I wake up several hours earlier than I used to and cannot get back to sleep | 3 | ||
| 17. | I don’t get more tired than usual | 0 | 18. | My appetite is no worse than usual | 0 |
| I get tired more easily than I used to | 1 | My appetite is not as good as it used to be | 1 | ||
| I get tired from doing almost anything | 2 | My appetite is much worse now | 2 | ||
| I am too tired to do anything | 3 | I have no appetite at all anymore | 3 | ||
| 19. | I haven’t lost much weight, if any, lately | 0 | 20. | I am no more worried about my health than usual | 0 |
| I have lost more than 5 pounds | 1 | I am worried about physical problems such as aches and pains; or upset stomach or constipation | 1 | ||
| I have lost more than 10 pounds | 2 | I am very worried about physical problems and it’s hard to think of much else | 2 | ||
| I have lost more than 15 pounds | 3 | I am so worried about my physical problems that I cannot think about anything else | 3 | ||
|
I am purposely trying to lose weight by eating less: ❑ Yes ❑ No |
|||||
| 21. | I have not noticed any recent change in my interest in sex | 0 | Total score | ||
| I am less interested in sex than I used to be | 1 | ||||
| I am much less interested in sex now | 2 | Date completed | |||
| I have lost interest in sex completely | 3 | ||||
Appendix 11 Short Form-36 (SF-36)
Appendix 12 Medical Interview Satisfaction Scale (MISS)
Appendix 13 Client Service Receipt Inventory (CSRI): baseline
Appendix 14 Client Service Receipt Inventory (CSRI): 6-month follow-up
Appendix 15 Sociodemographic interview
Appendix 16 Date of onset and previous treatment information
Appendix 17 Shortened Life Events and Difficulties Schedule
Appendix 18 Alcohol Use Disorders Identification Test (AUDIT)
Appendix 19 Bradford Somatic Inventory (BSI)
Referral No. Randomisation ID.
During the past month . . .
| YES (1) | NO (0) | ||
|---|---|---|---|
| 1. | Have you had severe headaches? | ||
| 2. | Have you had fluttering or a feeling of something moving in your stomach? | ||
| 3. | Have you had pain or tension in your neck and shoulders? | ||
| 4. | Has your skin been burning or itching all over? | ||
| 5. | Have you had a feeling of constriction of your head, as if it was being gripped tightly from outside? | ||
| 6. | Have you felt pain in the chest or heart? | ||
| 7. | Has your mouth or throat felt dry? | ||
| 8. | Has there been darkness or mist in front of your eyes? | ||
| 9. | Have you felt a burning sensation in your stomach? | ||
| 10. | Have you felt a lack of energy (weakness) much of the time? | ||
| 11. | Has your head felt hot or burning? | ||
| 12. | Have you been sweating a lot? | ||
| 13. | Have you felt as if there was pressure or tightness on your chest or heart? | ||
| 14. | Have you been suffering ache or discomfort in the abdomen? | ||
| 15. | Has there been a choking sensation in your throat? | ||
| 16. | Have your hands or feet had pins and needles or gone numb? | ||
| 17. | Have you felt aches or pains all over the body? | ||
| 18. | Have you had a feeling of heat inside your body? | ||
| 19. | Have you been aware of palpitations (heart pounding)? | ||
| 20. | Have you felt pain or burning in your eyes? | ||
| 21. | Have you suffered from indigestion? | ||
| 22. | Have you been trembling or shaking? | ||
| 23. | Have you been passing urine more frequently? | ||
| 24. | Have you been having low back trouble? | ||
| 25. | Has your stomach felt swollen or bloated? | ||
| 26. | Has your head felt heavy? | ||
| 27. | Have you been feeling tired, even when you are not working? | ||
| 28. | Have you been getting pain in your legs? | ||
| 29. | Have you been feeling sick in the stomach (nausea)? | ||
| 30. | Have you had a feeling of pressure inside your head, as if your head was going to burst? | ||
| 31. | Have you had difficulty in breathing, even when resting? | ||
| 32. | Have you felt tingling (pins and needles) all over the body? | ||
| 33. | Have you been troubled by constipation? | ||
| 34. | Have you wanted to open your bowels (go to the toilet) more often than usual? | ||
| 35. | Have your palms been sweating a lot? | ||
| 36. | Have you had difficulty in swallowing, as if there was a lump in your throat? | ||
| 37. | Have you been feeling giddy or dizzy? | ||
| 38. | Have you had a bitter taste in your mouth? | ||
| 39. | Has your whole body felt heavy? | ||
| 40. | Have you had a burning sensation when passing urine? | ||
| 41. | Have you been hearing a buzzing noise in your ears or head? | ||
| 42. | Has your heart felt weak or sinking? | ||
| 43. | Have you suffered from excessive wind (gas) or belching? | ||
| 44. | Have your hands or feet felt cold? | ||
| Men only | |||
| 45. | Have you had difficulty getting a full erection? | ||
| 46. | Have you felt that you have been passing semen in your urine? | ||
Appendix 20 Symptom attribution questionnaire
Appendix 21 Patient preference questionnaire
Appendix 22 Care received questionnaire
Appendix 23 Adverse events
| 26-week study period | Treatment arm | Event no. and date | Type of event | Brief description | Comments | Centre and PCT | Reported |
|---|---|---|---|---|---|---|---|
| 24/11/04–25/5/05 |
SSRI plus supportive care (fluoxetine) 30/11/04 (30 tabs) 10/1/05 (56 tabs) 23/5/05 (56 tabs) |
1 11/3/05 |
SAE | Paracetamol overdose, overnight hospitalisation required | No impact for patients in trial |
Southampton Southampton City |
Discussed at Study Group Copies of report sent to the Chairs of TSC and DMEC Included in progress report to HTA (Sept 05) and annual safety reports to MHRA and MREC |
| 22/2/05–23/8/05 |
SSRI plus supportive care (fluoxetine) 23/2/05 (28 caps) (citalopram) 11/3/05 (14 tabs) 15/8/05 (28 tabs) |
2a 28/2/05 |
AR | Uncontrollable shaking (dyskinesia) | Recognised side effect |
Liverpool Central Liverpool |
Discussed at Study Group Copies of report sent to the Chairs of TSC and DMEC Included in progress report to HTA (Sept 05) and annual safety reports to MHRA and MREC |
|
2b 12/5/05 |
AE | Admission to hospital for evacuation of retained products of conception (ERPC) following miscarriage but discharged the same day | Patient stopped medication on realising that she was pregnant. No impact for patients in trial |
Discussed at Study Group Copies of report sent to the Chairs of TSC and DMEC Included in progress report to HTA (Sept 05) and annual safety reports to MHRA and MREC |
|||
|
2c 20/7/05 |
SAE | Admission to hospital for lateral release right knee ligaments | Not study related so no further action required | Discovered through patient records on 31/7/06 (not previously accessed as preference patient). Will be included in HTA report (Sept 06) and annual safety reports to MHRA and MREC | |||
| 17/1/05–21/7/05 | Supportive care alone |
3 13/3/05 |
SAE | Died from rapid widespread cancer | No medication involved. Not study related so no further action taken |
Southampton New Forest |
No medication involved. To be reported in annual safety reports to MREC, HTA and MHRA |
| 23/8/05–23/3/06 |
SSRI plus supportive care (fluoxetine) 26/9/05 (30 tabs) |
4a 12/3/06 |
SAE | Admission to hospital for ERPC following miscarriage | Patient only took medication for 30 days and was not taking medication at time of conception. Event not related to study |
Southampton S Wiltshire |
Discussed at Study Group Copies of report sent to the Chairs of TSC and DMEC (19/7/06) To be reported to MREC, HTA and MHRA in regular reports |
|
4b 18/3/06 |
SAE | Admission to hospital for septic arthritis in the knee | Event not related to study | To be reported to MREC, MHRA and HTA (Sept 06) in regular reports | |||
| 5/4/06– 5/10/06 |
SSRI plus supportive care (citalopram) 6/4/06 (28 tabs) |
5 15/4/06 |
AR | Pains in spine, arms and head | Recognised side effect. No impact for patients in trial |
Southampton Guildford & Waverley |
Discussed at Study Group Copies of report sent to the Chairs of TSC and DMEC (19/7/06) To be reported to HTA (Sept 06), MREC and MHRA in regular reports |
| 27/4/05–26/10/05 | Supportive care alone |
6 12/8/05 |
SAE | Hospitalisation for planned operation for arthritic foot | Not related to the trial so no further action required |
Southampton Bournemouth |
Reported to HTA (Sept 06), MREC and MHRA in regular reports |
| 7/4/06–6/10/06 |
SSRI plus supportive care (fluoxetine 20 mg) 8/6/06 23/6/06 6/7/06 6/9/06 |
7 26/5/06 |
SAE | The patient took an overdose of paracetamol and ibuprofen and was taken to A&E | No impact for patients in trial. Further investigation revealed that no medication was prescribed before the event |
London Lewisham |
Reported to Study Group (20/11/06) and HTA in regular progress report (1/3/07) |
| 14/8/06–14/2/07 |
SSRI plus supportive care (fluoxetine 20mg) 16/8/06 30/8/06 19/9/06 |
8 30/8/06 |
AR | The patient described hot skin, red face, unable to drive and a ‘bad head’ | The patient had been prescribed fluoxetine 20 mg daily. No impact for patients in trial |
Liverpool Bolton |
Reported to Study Group (20/11/06) and HTA in regular progress report (1/3/07) |
| 8/2/06–9/8/07 | SSRI plus supportive care (citalopram, sertraline, velafaxine, fluoxetine) |
9 15/2/07 |
AR | Patient reported sedation, nausea and headache | Recognised side effect. No impact for patients in trial |
Southampton Fareham & Gosport |
Reported to Study Group (18/6/07) and reported to HTA in regular progress report (Sept 07) |
Appendix 24 Unit costs used in economic evaluation
| Service | Unit cost | Source |
|---|---|---|
| Inpatient admission | £471 per day | NHS Reference Costs |
| Outpatient consultation | £108 per attendance | NHS Reference Costs |
| Day patient | £108 per attendance | NHS Reference Costs |
| A&E consultation | £91 per visit | NHS Reference Costs |
| GP surgery consultation | £22 per consultation | PSSRU |
| GP telephone contact | £23 per consultation | PSSRU |
| GP home visit | £49 per visit | PSSRU |
| Practice nurse contact | £10 per contact | PSSRU |
| District nurse contact | £61 per hour | PSSRU |
| Community mental health nurse contact | £72 per hour | PSSRU |
| Other nurse contact | £47 per hour | PSSRU |
| Health visitor contact | £84 per hour | PSSRU |
| Counsellor contact | £48 per hour | PSSRU |
| Psychologist contact | £66 per hour | PSSRU |
| Occupational therapist | £57 per hour | PSSRU |
| Social worker contact | £77 per hour | PSSRU |
| Housing worker contact | £77 per hour | PSSRU |
| Community support worker | £69 per hour | PSSRU |
| Day centre attendance | £23 per attendance | PSSRU |
| Physiotherapist | £40 per hour | PSSRU |
List of abbreviations
- AHEAD
- Assessing Health Economics Antidepressants Study
- ARR
- absolute risk reduction
- AUDIT
- Alcohol Use Disorders Identification Test
- BDI
- Beck Depression Inventory
- BP
- bodily pain (SF-36 subscale)
- BSI
- Bradford Somatic Inventory
- CBT
- cognitive behavioural therapy
- CEAC
- cost-effectiveness acceptability curve
- CI
- confidence interval
- CSRI
- Client Service Receipt Inventory
- DMEC
- Data Monitoring and Ethics Committee
- DSM-IV
- Diagnostic and Statistical Manual (4th edition)
- GH
- general health (SF-36 subscale)
- GP
- general practitioner
- HADS
- Hospital Anxiety and Depression Scale
- HDRS
- Hamilton Depression Rating Scale
- HTA
- Health Technology Assessment
- ICD-10
- International Classification of Diseases (10th edition)
- ICER
- incremental cost-effectiveness ratio
- LEDS
- Life Events and Difficulties Schedule
- MADRS
- Montgomery–Åsberg Depression Rating Scale
- MH
- mental health (SF-36 subscale)
- MISS
- Medical Interview Satisfaction Scale
- MREC
- Multi-centre Research Ethics Committee
- NICE
- National Institute for Health and Clinical Excellence
- NNT
- number needed to treat
- PCT
- primary care trust
- PF
- physical functioning (SF-36 subscale)
- PHQ-9
- Patient Health Questionnaire, 9-item version
- PSAC
- psychosocially active consultation
- QALY
- quality-adjusted life-year
- R&D
- research and development
- RCGP
- Royal College of General Practitioners
- RE
- role – emotional (SF-36 subscale)
- RP
- role – physical (SF-36 subscale)
- SD
- standard deviation
- SF
- social functioning (SF-36 subscale)
- SF-36
- Medical Outcomes Study Short Form 36-item questionnaire
- SSRI
- selective serotonin reuptake inhibitor
- TSC
- Trial Steering Committee
- VT
- vitality (SF-36 subscale)
All abbreviations that have been used in this report are listed here unless the abbreviation is well known (e.g. NHS), or it has been used only once, or it is a non-standard abbreviation used only in figures/tables/appendices, in which case the abbreviation is defined in the figure legend or in the notes at the end of the table.
Notes
Health Technology Assessment reports published to date
-
Home parenteral nutrition: a systematic review.
By Richards DM, Deeks JJ, Sheldon TA, Shaffer JL.
-
Diagnosis, management and screening of early localised prostate cancer.
A review by Selley S, Donovan J, Faulkner A, Coast J, Gillatt D.
-
The diagnosis, management, treatment and costs of prostate cancer in England and Wales.
A review by Chamberlain J, Melia J, Moss S, Brown J.
-
Screening for fragile X syndrome.
A review by Murray J, Cuckle H, Taylor G, Hewison J.
-
A review of near patient testing in primary care.
By Hobbs FDR, Delaney BC, Fitzmaurice DA, Wilson S, Hyde CJ, Thorpe GH, et al.
-
Systematic review of outpatient services for chronic pain control.
By McQuay HJ, Moore RA, Eccleston C, Morley S, de C Williams AC.
-
Neonatal screening for inborn errors of metabolism: cost, yield and outcome.
A review by Pollitt RJ, Green A, McCabe CJ, Booth A, Cooper NJ, Leonard JV, et al.
-
Preschool vision screening.
A review by Snowdon SK, Stewart-Brown SL.
-
Implications of socio-cultural contexts for the ethics of clinical trials.
A review by Ashcroft RE, Chadwick DW, Clark SRL, Edwards RHT, Frith L, Hutton JL.
-
A critical review of the role of neonatal hearing screening in the detection of congenital hearing impairment.
By Davis A, Bamford J, Wilson I, Ramkalawan T, Forshaw M, Wright S.
-
Newborn screening for inborn errors of metabolism: a systematic review.
By Seymour CA, Thomason MJ, Chalmers RA, Addison GM, Bain MD, Cockburn F, et al.
-
Routine preoperative testing: a systematic review of the evidence.
By Munro J, Booth A, Nicholl J.
-
Systematic review of the effectiveness of laxatives in the elderly.
By Petticrew M, Watt I, Sheldon T.
-
When and how to assess fast-changing technologies: a comparative study of medical applications of four generic technologies.
A review by Mowatt G, Bower DJ, Brebner JA, Cairns JA, Grant AM, McKee L.
-
Antenatal screening for Down’s syndrome.
A review by Wald NJ, Kennard A, Hackshaw A, McGuire A.
-
Screening for ovarian cancer: a systematic review.
By Bell R, Petticrew M, Luengo S, Sheldon TA.
-
Consensus development methods, and their use in clinical guideline development.
A review by Murphy MK, Black NA, Lamping DL, McKee CM, Sanderson CFB, Askham J, et al.
-
A cost–utility analysis of interferon beta for multiple sclerosis.
By Parkin D, McNamee P, Jacoby A, Miller P, Thomas S, Bates D.
-
Effectiveness and efficiency of methods of dialysis therapy for end-stage renal disease: systematic reviews.
By MacLeod A, Grant A, Donaldson C, Khan I, Campbell M, Daly C, et al.
-
Effectiveness of hip prostheses in primary total hip replacement: a critical review of evidence and an economic model.
By Faulkner A, Kennedy LG, Baxter K, Donovan J, Wilkinson M, Bevan G.
-
Antimicrobial prophylaxis in colorectal surgery: a systematic review of randomised controlled trials.
By Song F, Glenny AM.
-
Bone marrow and peripheral blood stem cell transplantation for malignancy.
A review by Johnson PWM, Simnett SJ, Sweetenham JW, Morgan GJ, Stewart LA.
-
Screening for speech and language delay: a systematic review of the literature.
By Law J, Boyle J, Harris F, Harkness A, Nye C.
-
Resource allocation for chronic stable angina: a systematic review of effectiveness, costs and cost-effectiveness of alternative interventions.
By Sculpher MJ, Petticrew M, Kelland JL, Elliott RA, Holdright DR, Buxton MJ.
-
Detection, adherence and control of hypertension for the prevention of stroke: a systematic review.
By Ebrahim S.
-
Postoperative analgesia and vomiting, with special reference to day-case surgery: a systematic review.
By McQuay HJ, Moore RA.
-
Choosing between randomised and nonrandomised studies: a systematic review.
By Britton A, McKee M, Black N, McPherson K, Sanderson C, Bain C.
-
Evaluating patient-based outcome measures for use in clinical trials.
A review by Fitzpatrick R, Davey C, Buxton MJ, Jones DR.
-
Ethical issues in the design and conduct of randomised controlled trials.
A review by Edwards SJL, Lilford RJ, Braunholtz DA, Jackson JC, Hewison J, Thornton J.
-
Qualitative research methods in health technology assessment: a review of the literature.
By Murphy E, Dingwall R, Greatbatch D, Parker S, Watson P.
-
The costs and benefits of paramedic skills in pre-hospital trauma care.
By Nicholl J, Hughes S, Dixon S, Turner J, Yates D.
-
Systematic review of endoscopic ultrasound in gastro-oesophageal cancer.
By Harris KM, Kelly S, Berry E, Hutton J, Roderick P, Cullingworth J, et al.
-
Systematic reviews of trials and other studies.
By Sutton AJ, Abrams KR, Jones DR, Sheldon TA, Song F.
-
Primary total hip replacement surgery: a systematic review of outcomes and modelling of cost-effectiveness associated with different prostheses.
A review by Fitzpatrick R, Shortall E, Sculpher M, Murray D, Morris R, Lodge M, et al.
-
Informed decision making: an annotated bibliography and systematic review.
By Bekker H, Thornton JG, Airey CM, Connelly JB, Hewison J, Robinson MB, et al.
-
Handling uncertainty when performing economic evaluation of healthcare interventions.
A review by Briggs AH, Gray AM.
-
The role of expectancies in the placebo effect and their use in the delivery of health care: a systematic review.
By Crow R, Gage H, Hampson S, Hart J, Kimber A, Thomas H.
-
A randomised controlled trial of different approaches to universal antenatal HIV testing: uptake and acceptability. Annex: Antenatal HIV testing – assessment of a routine voluntary approach.
By Simpson WM, Johnstone FD, Boyd FM, Goldberg DJ, Hart GJ, Gormley SM, et al.
-
Methods for evaluating area-wide and organisation-based interventions in health and health care: a systematic review.
By Ukoumunne OC, Gulliford MC, Chinn S, Sterne JAC, Burney PGJ.
-
Assessing the costs of healthcare technologies in clinical trials.
A review by Johnston K, Buxton MJ, Jones DR, Fitzpatrick R.
-
Cooperatives and their primary care emergency centres: organisation and impact.
By Hallam L, Henthorne K.
-
Screening for cystic fibrosis.
A review by Murray J, Cuckle H, Taylor G, Littlewood J, Hewison J.
-
A review of the use of health status measures in economic evaluation.
By Brazier J, Deverill M, Green C, Harper R, Booth A.
-
Methods for the analysis of quality-of-life and survival data in health technology assessment.
A review by Billingham LJ, Abrams KR, Jones DR.
-
Antenatal and neonatal haemoglobinopathy screening in the UK: review and economic analysis.
By Zeuner D, Ades AE, Karnon J, Brown J, Dezateux C, Anionwu EN.
-
Assessing the quality of reports of randomised trials: implications for the conduct of meta-analyses.
A review by Moher D, Cook DJ, Jadad AR, Tugwell P, Moher M, Jones A, et al.
-
‘Early warning systems’ for identifying new healthcare technologies.
By Robert G, Stevens A, Gabbay J.
-
A systematic review of the role of human papillomavirus testing within a cervical screening programme.
By Cuzick J, Sasieni P, Davies P, Adams J, Normand C, Frater A, et al.
-
Near patient testing in diabetes clinics: appraising the costs and outcomes.
By Grieve R, Beech R, Vincent J, Mazurkiewicz J.
-
Positron emission tomography: establishing priorities for health technology assessment.
A review by Robert G, Milne R.
-
The debridement of chronic wounds: a systematic review.
By Bradley M, Cullum N, Sheldon T.
-
Systematic reviews of wound care management: (2) Dressings and topical agents used in the healing of chronic wounds.
By Bradley M, Cullum N, Nelson EA, Petticrew M, Sheldon T, Torgerson D.
-
A systematic literature review of spiral and electron beam computed tomography: with particular reference to clinical applications in hepatic lesions, pulmonary embolus and coronary artery disease.
By Berry E, Kelly S, Hutton J, Harris KM, Roderick P, Boyce JC, et al.
-
What role for statins? A review and economic model.
By Ebrahim S, Davey Smith G, McCabe C, Payne N, Pickin M, Sheldon TA, et al.
-
Factors that limit the quality, number and progress of randomised controlled trials.
A review by Prescott RJ, Counsell CE, Gillespie WJ, Grant AM, Russell IT, Kiauka S, et al.
-
Antimicrobial prophylaxis in total hip replacement: a systematic review.
By Glenny AM, Song F.
-
Health promoting schools and health promotion in schools: two systematic reviews.
By Lister-Sharp D, Chapman S, Stewart-Brown S, Sowden A.
-
Economic evaluation of a primary care-based education programme for patients with osteoarthritis of the knee.
A review by Lord J, Victor C, Littlejohns P, Ross FM, Axford JS.
-
The estimation of marginal time preference in a UK-wide sample (TEMPUS) project.
A review by Cairns JA, van der Pol MM.
-
Geriatric rehabilitation following fractures in older people: a systematic review.
By Cameron I, Crotty M, Currie C, Finnegan T, Gillespie L, Gillespie W, et al.
-
Screening for sickle cell disease and thalassaemia: a systematic review with supplementary research.
By Davies SC, Cronin E, Gill M, Greengross P, Hickman M, Normand C.
-
Community provision of hearing aids and related audiology services.
A review by Reeves DJ, Alborz A, Hickson FS, Bamford JM.
-
False-negative results in screening programmes: systematic review of impact and implications.
By Petticrew MP, Sowden AJ, Lister-Sharp D, Wright K.
-
Costs and benefits of community postnatal support workers: a randomised controlled trial.
By Morrell CJ, Spiby H, Stewart P, Walters S, Morgan A.
-
Implantable contraceptives (subdermal implants and hormonally impregnated intrauterine systems) versus other forms of reversible contraceptives: two systematic reviews to assess relative effectiveness, acceptability, tolerability and cost-effectiveness.
By French RS, Cowan FM, Mansour DJA, Morris S, Procter T, Hughes D, et al.
-
An introduction to statistical methods for health technology assessment.
A review by White SJ, Ashby D, Brown PJ.
-
Disease-modifying drugs for multiple sclerosis: a rapid and systematic review.
By Clegg A, Bryant J, Milne R.
-
Publication and related biases.
A review by Song F, Eastwood AJ, Gilbody S, Duley L, Sutton AJ.
-
Cost and outcome implications of the organisation of vascular services.
By Michaels J, Brazier J, Palfreyman S, Shackley P, Slack R.
-
Monitoring blood glucose control in diabetes mellitus: a systematic review.
By Coster S, Gulliford MC, Seed PT, Powrie JK, Swaminathan R.
-
The effectiveness of domiciliary health visiting: a systematic review of international studies and a selective review of the British literature.
By Elkan R, Kendrick D, Hewitt M, Robinson JJA, Tolley K, Blair M, et al.
-
The determinants of screening uptake and interventions for increasing uptake: a systematic review.
By Jepson R, Clegg A, Forbes C, Lewis R, Sowden A, Kleijnen J.
-
The effectiveness and cost-effectiveness of prophylactic removal of wisdom teeth.
A rapid review by Song F, O’Meara S, Wilson P, Golder S, Kleijnen J.
-
Ultrasound screening in pregnancy: a systematic review of the clinical effectiveness, cost-effectiveness and women’s views.
By Bricker L, Garcia J, Henderson J, Mugford M, Neilson J, Roberts T, et al.
-
A rapid and systematic review of the effectiveness and cost-effectiveness of the taxanes used in the treatment of advanced breast and ovarian cancer.
By Lister-Sharp D, McDonagh MS, Khan KS, Kleijnen J.
-
Liquid-based cytology in cervical screening: a rapid and systematic review.
By Payne N, Chilcott J, McGoogan E.
-
Randomised controlled trial of non-directive counselling, cognitive–behaviour therapy and usual general practitioner care in the management of depression as well as mixed anxiety and depression in primary care.
By King M, Sibbald B, Ward E, Bower P, Lloyd M, Gabbay M, et al.
-
Routine referral for radiography of patients presenting with low back pain: is patients’ outcome influenced by GPs’ referral for plain radiography?
By Kerry S, Hilton S, Patel S, Dundas D, Rink E, Lord J.
-
Systematic reviews of wound care management: (3) antimicrobial agents for chronic wounds; (4) diabetic foot ulceration.
By O’Meara S, Cullum N, Majid M, Sheldon T.
-
Using routine data to complement and enhance the results of randomised controlled trials.
By Lewsey JD, Leyland AH, Murray GD, Boddy FA.
-
Coronary artery stents in the treatment of ischaemic heart disease: a rapid and systematic review.
By Meads C, Cummins C, Jolly K, Stevens A, Burls A, Hyde C.
-
Outcome measures for adult critical care: a systematic review.
By Hayes JA, Black NA, Jenkinson C, Young JD, Rowan KM, Daly K, et al.
-
A systematic review to evaluate the effectiveness of interventions to promote the initiation of breastfeeding.
By Fairbank L, O’Meara S, Renfrew MJ, Woolridge M, Sowden AJ, Lister-Sharp D.
-
Implantable cardioverter defibrillators: arrhythmias. A rapid and systematic review.
By Parkes J, Bryant J, Milne R.
-
Treatments for fatigue in multiple sclerosis: a rapid and systematic review.
By Brañas P, Jordan R, Fry-Smith A, Burls A, Hyde C.
-
Early asthma prophylaxis, natural history, skeletal development and economy (EASE): a pilot randomised controlled trial.
By Baxter-Jones ADG, Helms PJ, Russell G, Grant A, Ross S, Cairns JA, et al.
-
Screening for hypercholesterolaemia versus case finding for familial hypercholesterolaemia: a systematic review and cost-effectiveness analysis.
By Marks D, Wonderling D, Thorogood M, Lambert H, Humphries SE, Neil HAW.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of glycoprotein IIb/IIIa antagonists in the medical management of unstable angina.
By McDonagh MS, Bachmann LM, Golder S, Kleijnen J, ter Riet G.
-
A randomised controlled trial of prehospital intravenous fluid replacement therapy in serious trauma.
By Turner J, Nicholl J, Webber L, Cox H, Dixon S, Yates D.
-
Intrathecal pumps for giving opioids in chronic pain: a systematic review.
By Williams JE, Louw G, Towlerton G.
-
Combination therapy (interferon alfa and ribavirin) in the treatment of chronic hepatitis C: a rapid and systematic review.
By Shepherd J, Waugh N, Hewitson P.
-
A systematic review of comparisons of effect sizes derived from randomised and non-randomised studies.
By MacLehose RR, Reeves BC, Harvey IM, Sheldon TA, Russell IT, Black AMS.
-
Intravascular ultrasound-guided interventions in coronary artery disease: a systematic literature review, with decision-analytic modelling, of outcomes and cost-effectiveness.
By Berry E, Kelly S, Hutton J, Lindsay HSJ, Blaxill JM, Evans JA, et al.
-
A randomised controlled trial to evaluate the effectiveness and cost-effectiveness of counselling patients with chronic depression.
By Simpson S, Corney R, Fitzgerald P, Beecham J.
-
Systematic review of treatments for atopic eczema.
By Hoare C, Li Wan Po A, Williams H.
-
Bayesian methods in health technology assessment: a review.
By Spiegelhalter DJ, Myles JP, Jones DR, Abrams KR.
-
The management of dyspepsia: a systematic review.
By Delaney B, Moayyedi P, Deeks J, Innes M, Soo S, Barton P, et al.
-
A systematic review of treatments for severe psoriasis.
By Griffiths CEM, Clark CM, Chalmers RJG, Li Wan Po A, Williams HC.
-
Clinical and cost-effectiveness of donepezil, rivastigmine and galantamine for Alzheimer’s disease: a rapid and systematic review.
By Clegg A, Bryant J, Nicholson T, McIntyre L, De Broe S, Gerard K, et al.
-
The clinical effectiveness and cost-effectiveness of riluzole for motor neurone disease: a rapid and systematic review.
By Stewart A, Sandercock J, Bryan S, Hyde C, Barton PM, Fry-Smith A, et al.
-
Equity and the economic evaluation of healthcare.
By Sassi F, Archard L, Le Grand J.
-
Quality-of-life measures in chronic diseases of childhood.
By Eiser C, Morse R.
-
Eliciting public preferences for healthcare: a systematic review of techniques.
By Ryan M, Scott DA, Reeves C, Bate A, van Teijlingen ER, Russell EM, et al.
-
General health status measures for people with cognitive impairment: learning disability and acquired brain injury.
By Riemsma RP, Forbes CA, Glanville JM, Eastwood AJ, Kleijnen J.
-
An assessment of screening strategies for fragile X syndrome in the UK.
By Pembrey ME, Barnicoat AJ, Carmichael B, Bobrow M, Turner G.
-
Issues in methodological research: perspectives from researchers and commissioners.
By Lilford RJ, Richardson A, Stevens A, Fitzpatrick R, Edwards S, Rock F, et al.
-
Systematic reviews of wound care management: (5) beds; (6) compression; (7) laser therapy, therapeutic ultrasound, electrotherapy and electromagnetic therapy.
By Cullum N, Nelson EA, Flemming K, Sheldon T.
-
Effects of educational and psychosocial interventions for adolescents with diabetes mellitus: a systematic review.
By Hampson SE, Skinner TC, Hart J, Storey L, Gage H, Foxcroft D, et al.
-
Effectiveness of autologous chondrocyte transplantation for hyaline cartilage defects in knees: a rapid and systematic review.
By Jobanputra P, Parry D, Fry-Smith A, Burls A.
-
Statistical assessment of the learning curves of health technologies.
By Ramsay CR, Grant AM, Wallace SA, Garthwaite PH, Monk AF, Russell IT.
-
The effectiveness and cost-effectiveness of temozolomide for the treatment of recurrent malignant glioma: a rapid and systematic review.
By Dinnes J, Cave C, Huang S, Major K, Milne R.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of debriding agents in treating surgical wounds healing by secondary intention.
By Lewis R, Whiting P, ter Riet G, O’Meara S, Glanville J.
-
Home treatment for mental health problems: a systematic review.
By Burns T, Knapp M, Catty J, Healey A, Henderson J, Watt H, et al.
-
How to develop cost-conscious guidelines.
By Eccles M, Mason J.
-
The role of specialist nurses in multiple sclerosis: a rapid and systematic review.
By De Broe S, Christopher F, Waugh N.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of orlistat in the management of obesity.
By O’Meara S, Riemsma R, Shirran L, Mather L, ter Riet G.
-
The clinical effectiveness and cost-effectiveness of pioglitazone for type 2 diabetes mellitus: a rapid and systematic review.
By Chilcott J, Wight J, Lloyd Jones M, Tappenden P.
-
Extended scope of nursing practice: a multicentre randomised controlled trial of appropriately trained nurses and preregistration house officers in preoperative assessment in elective general surgery.
By Kinley H, Czoski-Murray C, George S, McCabe C, Primrose J, Reilly C, et al.
-
Systematic reviews of the effectiveness of day care for people with severe mental disorders: (1) Acute day hospital versus admission; (2) Vocational rehabilitation; (3) Day hospital versus outpatient care.
By Marshall M, Crowther R, Almaraz- Serrano A, Creed F, Sledge W, Kluiter H, et al.
-
The measurement and monitoring of surgical adverse events.
By Bruce J, Russell EM, Mollison J, Krukowski ZH.
-
Action research: a systematic review and guidance for assessment.
By Waterman H, Tillen D, Dickson R, de Koning K.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of gemcitabine for the treatment of pancreatic cancer.
By Ward S, Morris E, Bansback N, Calvert N, Crellin A, Forman D, et al.
-
A rapid and systematic review of the evidence for the clinical effectiveness and cost-effectiveness of irinotecan, oxaliplatin and raltitrexed for the treatment of advanced colorectal cancer.
By Lloyd Jones M, Hummel S, Bansback N, Orr B, Seymour M.
-
Comparison of the effectiveness of inhaler devices in asthma and chronic obstructive airways disease: a systematic review of the literature.
By Brocklebank D, Ram F, Wright J, Barry P, Cates C, Davies L, et al.
-
The cost-effectiveness of magnetic resonance imaging for investigation of the knee joint.
By Bryan S, Weatherburn G, Bungay H, Hatrick C, Salas C, Parry D, et al.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of topotecan for ovarian cancer.
By Forbes C, Shirran L, Bagnall A-M, Duffy S, ter Riet G.
-
Superseded by a report published in a later volume.
-
The role of radiography in primary care patients with low back pain of at least 6 weeks duration: a randomised (unblinded) controlled trial.
By Kendrick D, Fielding K, Bentley E, Miller P, Kerslake R, Pringle M.
-
Design and use of questionnaires: a review of best practice applicable to surveys of health service staff and patients.
By McColl E, Jacoby A, Thomas L, Soutter J, Bamford C, Steen N, et al.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of paclitaxel, docetaxel, gemcitabine and vinorelbine in non-small-cell lung cancer.
By Clegg A, Scott DA, Sidhu M, Hewitson P, Waugh N.
-
Subgroup analyses in randomised controlled trials: quantifying the risks of false-positives and false-negatives.
By Brookes ST, Whitley E, Peters TJ, Mulheran PA, Egger M, Davey Smith G.
-
Depot antipsychotic medication in the treatment of patients with schizophrenia: (1) Meta-review; (2) Patient and nurse attitudes.
By David AS, Adams C.
-
A systematic review of controlled trials of the effectiveness and cost-effectiveness of brief psychological treatments for depression.
By Churchill R, Hunot V, Corney R, Knapp M, McGuire H, Tylee A, et al.
-
Cost analysis of child health surveillance.
By Sanderson D, Wright D, Acton C, Duree D.
-
A study of the methods used to select review criteria for clinical audit.
By Hearnshaw H, Harker R, Cheater F, Baker R, Grimshaw G.
-
Fludarabine as second-line therapy for B cell chronic lymphocytic leukaemia: a technology assessment.
By Hyde C, Wake B, Bryan S, Barton P, Fry-Smith A, Davenport C, et al.
-
Rituximab as third-line treatment for refractory or recurrent Stage III or IV follicular non-Hodgkin’s lymphoma: a systematic review and economic evaluation.
By Wake B, Hyde C, Bryan S, Barton P, Song F, Fry-Smith A, et al.
-
A systematic review of discharge arrangements for older people.
By Parker SG, Peet SM, McPherson A, Cannaby AM, Baker R, Wilson A, et al.
-
The clinical effectiveness and cost-effectiveness of inhaler devices used in the routine management of chronic asthma in older children: a systematic review and economic evaluation.
By Peters J, Stevenson M, Beverley C, Lim J, Smith S.
-
The clinical effectiveness and cost-effectiveness of sibutramine in the management of obesity: a technology assessment.
By O’Meara S, Riemsma R, Shirran L, Mather L, ter Riet G.
-
The cost-effectiveness of magnetic resonance angiography for carotid artery stenosis and peripheral vascular disease: a systematic review.
By Berry E, Kelly S, Westwood ME, Davies LM, Gough MJ, Bamford JM, et al.
-
Promoting physical activity in South Asian Muslim women through ‘exercise on prescription’.
By Carroll B, Ali N, Azam N.
-
Zanamivir for the treatment of influenza in adults: a systematic review and economic evaluation.
By Burls A, Clark W, Stewart T, Preston C, Bryan S, Jefferson T, et al.
-
A review of the natural history and epidemiology of multiple sclerosis: implications for resource allocation and health economic models.
By Richards RG, Sampson FC, Beard SM, Tappenden P.
-
Screening for gestational diabetes: a systematic review and economic evaluation.
By Scott DA, Loveman E, McIntyre L, Waugh N.
-
The clinical effectiveness and cost-effectiveness of surgery for people with morbid obesity: a systematic review and economic evaluation.
By Clegg AJ, Colquitt J, Sidhu MK, Royle P, Loveman E, Walker A.
-
The clinical effectiveness of trastuzumab for breast cancer: a systematic review.
By Lewis R, Bagnall A-M, Forbes C, Shirran E, Duffy S, Kleijnen J, et al.
-
The clinical effectiveness and cost-effectiveness of vinorelbine for breast cancer: a systematic review and economic evaluation.
By Lewis R, Bagnall A-M, King S, Woolacott N, Forbes C, Shirran L, et al.
-
A systematic review of the effectiveness and cost-effectiveness of metal-on-metal hip resurfacing arthroplasty for treatment of hip disease.
By Vale L, Wyness L, McCormack K, McKenzie L, Brazzelli M, Stearns SC.
-
The clinical effectiveness and cost-effectiveness of bupropion and nicotine replacement therapy for smoking cessation: a systematic review and economic evaluation.
By Woolacott NF, Jones L, Forbes CA, Mather LC, Sowden AJ, Song FJ, et al.
-
A systematic review of effectiveness and economic evaluation of new drug treatments for juvenile idiopathic arthritis: etanercept.
By Cummins C, Connock M, Fry-Smith A, Burls A.
-
Clinical effectiveness and cost-effectiveness of growth hormone in children: a systematic review and economic evaluation.
By Bryant J, Cave C, Mihaylova B, Chase D, McIntyre L, Gerard K, et al.
-
Clinical effectiveness and cost-effectiveness of growth hormone in adults in relation to impact on quality of life: a systematic review and economic evaluation.
By Bryant J, Loveman E, Chase D, Mihaylova B, Cave C, Gerard K, et al.
-
Clinical medication review by a pharmacist of patients on repeat prescriptions in general practice: a randomised controlled trial.
By Zermansky AG, Petty DR, Raynor DK, Lowe CJ, Freementle N, Vail A.
-
The effectiveness of infliximab and etanercept for the treatment of rheumatoid arthritis: a systematic review and economic evaluation.
By Jobanputra P, Barton P, Bryan S, Burls A.
-
A systematic review and economic evaluation of computerised cognitive behaviour therapy for depression and anxiety.
By Kaltenthaler E, Shackley P, Stevens K, Beverley C, Parry G, Chilcott J.
-
A systematic review and economic evaluation of pegylated liposomal doxorubicin hydrochloride for ovarian cancer.
By Forbes C, Wilby J, Richardson G, Sculpher M, Mather L, Reimsma R.
-
A systematic review of the effectiveness of interventions based on a stages-of-change approach to promote individual behaviour change.
By Riemsma RP, Pattenden J, Bridle C, Sowden AJ, Mather L, Watt IS, et al.
-
A systematic review update of the clinical effectiveness and cost-effectiveness of glycoprotein IIb/IIIa antagonists.
By Robinson M, Ginnelly L, Sculpher M, Jones L, Riemsma R, Palmer S, et al.
-
A systematic review of the effectiveness, cost-effectiveness and barriers to implementation of thrombolytic and neuroprotective therapy for acute ischaemic stroke in the NHS.
By Sandercock P, Berge E, Dennis M, Forbes J, Hand P, Kwan J, et al.
-
A randomised controlled crossover trial of nurse practitioner versus doctor-led outpatient care in a bronchiectasis clinic.
By Caine N, Sharples LD, Hollingworth W, French J, Keogan M, Exley A, et al.
-
Clinical effectiveness and cost – consequences of selective serotonin reuptake inhibitors in the treatment of sex offenders.
By Adi Y, Ashcroft D, Browne K, Beech A, Fry-Smith A, Hyde C.
-
Treatment of established osteoporosis: a systematic review and cost–utility analysis.
By Kanis JA, Brazier JE, Stevenson M, Calvert NW, Lloyd Jones M.
-
Which anaesthetic agents are cost-effective in day surgery? Literature review, national survey of practice and randomised controlled trial.
By Elliott RA Payne K, Moore JK, Davies LM, Harper NJN, St Leger AS, et al.
-
Screening for hepatitis C among injecting drug users and in genitourinary medicine clinics: systematic reviews of effectiveness, modelling study and national survey of current practice.
By Stein K, Dalziel K, Walker A, McIntyre L, Jenkins B, Horne J, et al.
-
The measurement of satisfaction with healthcare: implications for practice from a systematic review of the literature.
By Crow R, Gage H, Hampson S, Hart J, Kimber A, Storey L, et al.
-
The effectiveness and cost-effectiveness of imatinib in chronic myeloid leukaemia: a systematic review.
By Garside R, Round A, Dalziel K, Stein K, Royle R.
-
A comparative study of hypertonic saline, daily and alternate-day rhDNase in children with cystic fibrosis.
By Suri R, Wallis C, Bush A, Thompson S, Normand C, Flather M, et al.
-
A systematic review of the costs and effectiveness of different models of paediatric home care.
By Parker G, Bhakta P, Lovett CA, Paisley S, Olsen R, Turner D, et al.
-
How important are comprehensive literature searches and the assessment of trial quality in systematic reviews? Empirical study.
By Egger M, Jüni P, Bartlett C, Holenstein F, Sterne J.
-
Systematic review of the effectiveness and cost-effectiveness, and economic evaluation, of home versus hospital or satellite unit haemodialysis for people with end-stage renal failure.
By Mowatt G, Vale L, Perez J, Wyness L, Fraser C, MacLeod A, et al.
-
Systematic review and economic evaluation of the effectiveness of infliximab for the treatment of Crohn’s disease.
By Clark W, Raftery J, Barton P, Song F, Fry-Smith A, Burls A.
-
A review of the clinical effectiveness and cost-effectiveness of routine anti-D prophylaxis for pregnant women who are rhesus negative.
By Chilcott J, Lloyd Jones M, Wight J, Forman K, Wray J, Beverley C, et al.
-
Systematic review and evaluation of the use of tumour markers in paediatric oncology: Ewing’s sarcoma and neuroblastoma.
By Riley RD, Burchill SA, Abrams KR, Heney D, Lambert PC, Jones DR, et al.
-
The cost-effectiveness of screening for Helicobacter pylori to reduce mortality and morbidity from gastric cancer and peptic ulcer disease: a discrete-event simulation model.
By Roderick P, Davies R, Raftery J, Crabbe D, Pearce R, Bhandari P, et al.
-
The clinical effectiveness and cost-effectiveness of routine dental checks: a systematic review and economic evaluation.
By Davenport C, Elley K, Salas C, Taylor-Weetman CL, Fry-Smith A, Bryan S, et al.
-
A multicentre randomised controlled trial assessing the costs and benefits of using structured information and analysis of women’s preferences in the management of menorrhagia.
By Kennedy ADM, Sculpher MJ, Coulter A, Dwyer N, Rees M, Horsley S, et al.
-
Clinical effectiveness and cost–utility of photodynamic therapy for wet age-related macular degeneration: a systematic review and economic evaluation.
By Meads C, Salas C, Roberts T, Moore D, Fry-Smith A, Hyde C.
-
Evaluation of molecular tests for prenatal diagnosis of chromosome abnormalities.
By Grimshaw GM, Szczepura A, Hultén M, MacDonald F, Nevin NC, Sutton F, et al.
-
First and second trimester antenatal screening for Down’s syndrome: the results of the Serum, Urine and Ultrasound Screening Study (SURUSS).
By Wald NJ, Rodeck C, Hackshaw AK, Walters J, Chitty L, Mackinson AM.
-
The effectiveness and cost-effectiveness of ultrasound locating devices for central venous access: a systematic review and economic evaluation.
By Calvert N, Hind D, McWilliams RG, Thomas SM, Beverley C, Davidson A.
-
A systematic review of atypical antipsychotics in schizophrenia.
By Bagnall A-M, Jones L, Lewis R, Ginnelly L, Glanville J, Torgerson D, et al.
-
Prostate Testing for Cancer and Treatment (ProtecT) feasibility study.
By Donovan J, Hamdy F, Neal D, Peters T, Oliver S, Brindle L, et al.
-
Early thrombolysis for the treatment of acute myocardial infarction: a systematic review and economic evaluation.
By Boland A, Dundar Y, Bagust A, Haycox A, Hill R, Mujica Mota R, et al.
-
Screening for fragile X syndrome: a literature review and modelling.
By Song FJ, Barton P, Sleightholme V, Yao GL, Fry-Smith A.
-
Systematic review of endoscopic sinus surgery for nasal polyps.
By Dalziel K, Stein K, Round A, Garside R, Royle P.
-
Towards efficient guidelines: how to monitor guideline use in primary care.
By Hutchinson A, McIntosh A, Cox S, Gilbert C.
-
Effectiveness and cost-effectiveness of acute hospital-based spinal cord injuries services: systematic review.
By Bagnall A-M, Jones L, Richardson G, Duffy S, Riemsma R.
-
Prioritisation of health technology assessment. The PATHS model: methods and case studies.
By Townsend J, Buxton M, Harper G.
-
Systematic review of the clinical effectiveness and cost-effectiveness of tension-free vaginal tape for treatment of urinary stress incontinence.
By Cody J, Wyness L, Wallace S, Glazener C, Kilonzo M, Stearns S, et al.
-
The clinical and cost-effectiveness of patient education models for diabetes: a systematic review and economic evaluation.
By Loveman E, Cave C, Green C, Royle P, Dunn N, Waugh N.
-
The role of modelling in prioritising and planning clinical trials.
By Chilcott J, Brennan A, Booth A, Karnon J, Tappenden P.
-
Cost–benefit evaluation of routine influenza immunisation in people 65–74 years of age.
By Allsup S, Gosney M, Haycox A, Regan M.
-
The clinical and cost-effectiveness of pulsatile machine perfusion versus cold storage of kidneys for transplantation retrieved from heart-beating and non-heart-beating donors.
By Wight J, Chilcott J, Holmes M, Brewer N.
-
Can randomised trials rely on existing electronic data? A feasibility study to explore the value of routine data in health technology assessment.
By Williams JG, Cheung WY, Cohen DR, Hutchings HA, Longo MF, Russell IT.
-
Evaluating non-randomised intervention studies.
By Deeks JJ, Dinnes J, D’Amico R, Sowden AJ, Sakarovitch C, Song F, et al.
-
A randomised controlled trial to assess the impact of a package comprising a patient-orientated, evidence-based self- help guidebook and patient-centred consultations on disease management and satisfaction in inflammatory bowel disease.
By Kennedy A, Nelson E, Reeves D, Richardson G, Roberts C, Robinson A, et al.
-
The effectiveness of diagnostic tests for the assessment of shoulder pain due to soft tissue disorders: a systematic review.
By Dinnes J, Loveman E, McIntyre L, Waugh N.
-
The value of digital imaging in diabetic retinopathy.
By Sharp PF, Olson J, Strachan F, Hipwell J, Ludbrook A, O’Donnell M, et al.
-
Lowering blood pressure to prevent myocardial infarction and stroke: a new preventive strategy.
By Law M, Wald N, Morris J.
-
Clinical and cost-effectiveness of capecitabine and tegafur with uracil for the treatment of metastatic colorectal cancer: systematic review and economic evaluation.
By Ward S, Kaltenthaler E, Cowan J, Brewer N.
-
Clinical and cost-effectiveness of new and emerging technologies for early localised prostate cancer: a systematic review.
By Hummel S, Paisley S, Morgan A, Currie E, Brewer N.
-
Literature searching for clinical and cost-effectiveness studies used in health technology assessment reports carried out for the National Institute for Clinical Excellence appraisal system.
By Royle P, Waugh N.
-
Systematic review and economic decision modelling for the prevention and treatment of influenza A and B.
By Turner D, Wailoo A, Nicholson K, Cooper N, Sutton A, Abrams K.
-
A randomised controlled trial to evaluate the clinical and cost-effectiveness of Hickman line insertions in adult cancer patients by nurses.
By Boland A, Haycox A, Bagust A, Fitzsimmons L.
-
Redesigning postnatal care: a randomised controlled trial of protocol-based midwifery-led care focused on individual women’s physical and psychological health needs.
By MacArthur C, Winter HR, Bick DE, Lilford RJ, Lancashire RJ, Knowles H, et al.
-
Estimating implied rates of discount in healthcare decision-making.
By West RR, McNabb R, Thompson AGH, Sheldon TA, Grimley Evans J.
-
Systematic review of isolation policies in the hospital management of methicillin-resistant Staphylococcus aureus: a review of the literature with epidemiological and economic modelling.
By Cooper BS, Stone SP, Kibbler CC, Cookson BD, Roberts JA, Medley GF, et al.
-
Treatments for spasticity and pain in multiple sclerosis: a systematic review.
By Beard S, Hunn A, Wight J.
-
The inclusion of reports of randomised trials published in languages other than English in systematic reviews.
By Moher D, Pham B, Lawson ML, Klassen TP.
-
The impact of screening on future health-promoting behaviours and health beliefs: a systematic review.
By Bankhead CR, Brett J, Bukach C, Webster P, Stewart-Brown S, Munafo M, et al.
-
What is the best imaging strategy for acute stroke?
By Wardlaw JM, Keir SL, Seymour J, Lewis S, Sandercock PAG, Dennis MS, et al.
-
Systematic review and modelling of the investigation of acute and chronic chest pain presenting in primary care.
By Mant J, McManus RJ, Oakes RAL, Delaney BC, Barton PM, Deeks JJ, et al.
-
The effectiveness and cost-effectiveness of microwave and thermal balloon endometrial ablation for heavy menstrual bleeding: a systematic review and economic modelling.
By Garside R, Stein K, Wyatt K, Round A, Price A.
-
A systematic review of the role of bisphosphonates in metastatic disease.
By Ross JR, Saunders Y, Edmonds PM, Patel S, Wonderling D, Normand C, et al.
-
Systematic review of the clinical effectiveness and cost-effectiveness of capecitabine (Xeloda®) for locally advanced and/or metastatic breast cancer.
By Jones L, Hawkins N, Westwood M, Wright K, Richardson G, Riemsma R.
-
Effectiveness and efficiency of guideline dissemination and implementation strategies.
By Grimshaw JM, Thomas RE, MacLennan G, Fraser C, Ramsay CR, Vale L, et al.
-
Clinical effectiveness and costs of the Sugarbaker procedure for the treatment of pseudomyxoma peritonei.
By Bryant J, Clegg AJ, Sidhu MK, Brodin H, Royle P, Davidson P.
-
Psychological treatment for insomnia in the regulation of long-term hypnotic drug use.
By Morgan K, Dixon S, Mathers N, Thompson J, Tomeny M.
-
Improving the evaluation of therapeutic interventions in multiple sclerosis: development of a patient-based measure of outcome.
By Hobart JC, Riazi A, Lamping DL, Fitzpatrick R, Thompson AJ.
-
A systematic review and economic evaluation of magnetic resonance cholangiopancreatography compared with diagnostic endoscopic retrograde cholangiopancreatography.
By Kaltenthaler E, Bravo Vergel Y, Chilcott J, Thomas S, Blakeborough T, Walters SJ, et al.
-
The use of modelling to evaluate new drugs for patients with a chronic condition: the case of antibodies against tumour necrosis factor in rheumatoid arthritis.
By Barton P, Jobanputra P, Wilson J, Bryan S, Burls A.
-
Clinical effectiveness and cost-effectiveness of neonatal screening for inborn errors of metabolism using tandem mass spectrometry: a systematic review.
By Pandor A, Eastham J, Beverley C, Chilcott J, Paisley S.
-
Clinical effectiveness and cost-effectiveness of pioglitazone and rosiglitazone in the treatment of type 2 diabetes: a systematic review and economic evaluation.
By Czoski-Murray C, Warren E, Chilcott J, Beverley C, Psyllaki MA, Cowan J.
-
Routine examination of the newborn: the EMREN study. Evaluation of an extension of the midwife role including a randomised controlled trial of appropriately trained midwives and paediatric senior house officers.
By Townsend J, Wolke D, Hayes J, Davé S, Rogers C, Bloomfield L, et al.
-
Involving consumers in research and development agenda setting for the NHS: developing an evidence-based approach.
By Oliver S, Clarke-Jones L, Rees R, Milne R, Buchanan P, Gabbay J, et al.
-
A multi-centre randomised controlled trial of minimally invasive direct coronary bypass grafting versus percutaneous transluminal coronary angioplasty with stenting for proximal stenosis of the left anterior descending coronary artery.
By Reeves BC, Angelini GD, Bryan AJ, Taylor FC, Cripps T, Spyt TJ, et al.
-
Does early magnetic resonance imaging influence management or improve outcome in patients referred to secondary care with low back pain? A pragmatic randomised controlled trial.
By Gilbert FJ, Grant AM, Gillan MGC, Vale L, Scott NW, Campbell MK, et al.
-
The clinical and cost-effectiveness of anakinra for the treatment of rheumatoid arthritis in adults: a systematic review and economic analysis.
By Clark W, Jobanputra P, Barton P, Burls A.
-
A rapid and systematic review and economic evaluation of the clinical and cost-effectiveness of newer drugs for treatment of mania associated with bipolar affective disorder.
By Bridle C, Palmer S, Bagnall A-M, Darba J, Duffy S, Sculpher M, et al.
-
Liquid-based cytology in cervical screening: an updated rapid and systematic review and economic analysis.
By Karnon J, Peters J, Platt J, Chilcott J, McGoogan E, Brewer N.
-
Systematic review of the long-term effects and economic consequences of treatments for obesity and implications for health improvement.
By Avenell A, Broom J, Brown TJ, Poobalan A, Aucott L, Stearns SC, et al.
-
Autoantibody testing in children with newly diagnosed type 1 diabetes mellitus.
By Dretzke J, Cummins C, Sandercock J, Fry-Smith A, Barrett T, Burls A.
-
Clinical effectiveness and cost-effectiveness of prehospital intravenous fluids in trauma patients.
By Dretzke J, Sandercock J, Bayliss S, Burls A.
-
Newer hypnotic drugs for the short-term management of insomnia: a systematic review and economic evaluation.
By Dündar Y, Boland A, Strobl J, Dodd S, Haycox A, Bagust A, et al.
-
Development and validation of methods for assessing the quality of diagnostic accuracy studies.
By Whiting P, Rutjes AWS, Dinnes J, Reitsma JB, Bossuyt PMM, Kleijnen J.
-
EVALUATE hysterectomy trial: a multicentre randomised trial comparing abdominal, vaginal and laparoscopic methods of hysterectomy.
By Garry R, Fountain J, Brown J, Manca A, Mason S, Sculpher M, et al.
-
Methods for expected value of information analysis in complex health economic models: developments on the health economics of interferon-β and glatiramer acetate for multiple sclerosis.
By Tappenden P, Chilcott JB, Eggington S, Oakley J, McCabe C.
-
Effectiveness and cost-effectiveness of imatinib for first-line treatment of chronic myeloid leukaemia in chronic phase: a systematic review and economic analysis.
By Dalziel K, Round A, Stein K, Garside R, Price A.
-
VenUS I: a randomised controlled trial of two types of bandage for treating venous leg ulcers.
By Iglesias C, Nelson EA, Cullum NA, Torgerson DJ, on behalf of the VenUS Team.
-
Systematic review of the effectiveness and cost-effectiveness, and economic evaluation, of myocardial perfusion scintigraphy for the diagnosis and management of angina and myocardial infarction.
By Mowatt G, Vale L, Brazzelli M, Hernandez R, Murray A, Scott N, et al.
-
A pilot study on the use of decision theory and value of information analysis as part of the NHS Health Technology Assessment programme.
By Claxton K, Ginnelly L, Sculpher M, Philips Z, Palmer S.
-
The Social Support and Family Health Study: a randomised controlled trial and economic evaluation of two alternative forms of postnatal support for mothers living in disadvantaged inner-city areas.
By Wiggins M, Oakley A, Roberts I, Turner H, Rajan L, Austerberry H, et al.
-
Psychosocial aspects of genetic screening of pregnant women and newborns: a systematic review.
By Green JM, Hewison J, Bekker HL, Bryant, Cuckle HS.
-
Evaluation of abnormal uterine bleeding: comparison of three outpatient procedures within cohorts defined by age and menopausal status.
By Critchley HOD, Warner P, Lee AJ, Brechin S, Guise J, Graham B.
-
Coronary artery stents: a rapid systematic review and economic evaluation.
By Hill R, Bagust A, Bakhai A, Dickson R, Dündar Y, Haycox A, et al.
-
Review of guidelines for good practice in decision-analytic modelling in health technology assessment.
By Philips Z, Ginnelly L, Sculpher M, Claxton K, Golder S, Riemsma R, et al.
-
Rituximab (MabThera®) for aggressive non-Hodgkin’s lymphoma: systematic review and economic evaluation.
By Knight C, Hind D, Brewer N, Abbott V.
-
Clinical effectiveness and cost-effectiveness of clopidogrel and modified-release dipyridamole in the secondary prevention of occlusive vascular events: a systematic review and economic evaluation.
By Jones L, Griffin S, Palmer S, Main C, Orton V, Sculpher M, et al.
-
Pegylated interferon α-2a and -2b in combination with ribavirin in the treatment of chronic hepatitis C: a systematic review and economic evaluation.
By Shepherd J, Brodin H, Cave C, Waugh N, Price A, Gabbay J.
-
Clopidogrel used in combination with aspirin compared with aspirin alone in the treatment of non-ST-segment- elevation acute coronary syndromes: a systematic review and economic evaluation.
By Main C, Palmer S, Griffin S, Jones L, Orton V, Sculpher M, et al.
-
Provision, uptake and cost of cardiac rehabilitation programmes: improving services to under-represented groups.
By Beswick AD, Rees K, Griebsch I, Taylor FC, Burke M, West RR, et al.
-
Involving South Asian patients in clinical trials.
By Hussain-Gambles M, Leese B, Atkin K, Brown J, Mason S, Tovey P.
-
Clinical and cost-effectiveness of continuous subcutaneous insulin infusion for diabetes.
By Colquitt JL, Green C, Sidhu MK, Hartwell D, Waugh N.
-
Identification and assessment of ongoing trials in health technology assessment reviews.
By Song FJ, Fry-Smith A, Davenport C, Bayliss S, Adi Y, Wilson JS, et al.
-
Systematic review and economic evaluation of a long-acting insulin analogue, insulin glargine
By Warren E, Weatherley-Jones E, Chilcott J, Beverley C.
-
Supplementation of a home-based exercise programme with a class-based programme for people with osteoarthritis of the knees: a randomised controlled trial and health economic analysis.
By McCarthy CJ, Mills PM, Pullen R, Richardson G, Hawkins N, Roberts CR, et al.
-
Clinical and cost-effectiveness of once-daily versus more frequent use of same potency topical corticosteroids for atopic eczema: a systematic review and economic evaluation.
By Green C, Colquitt JL, Kirby J, Davidson P, Payne E.
-
Acupuncture of chronic headache disorders in primary care: randomised controlled trial and economic analysis.
By Vickers AJ, Rees RW, Zollman CE, McCarney R, Smith CM, Ellis N, et al.
-
Generalisability in economic evaluation studies in healthcare: a review and case studies.
By Sculpher MJ, Pang FS, Manca A, Drummond MF, Golder S, Urdahl H, et al.
-
Virtual outreach: a randomised controlled trial and economic evaluation of joint teleconferenced medical consultations.
By Wallace P, Barber J, Clayton W, Currell R, Fleming K, Garner P, et al.
-
Randomised controlled multiple treatment comparison to provide a cost-effectiveness rationale for the selection of antimicrobial therapy in acne.
By Ozolins M, Eady EA, Avery A, Cunliffe WJ, O’Neill C, Simpson NB, et al.
-
Do the findings of case series studies vary significantly according to methodological characteristics?
By Dalziel K, Round A, Stein K, Garside R, Castelnuovo E, Payne L.
-
Improving the referral process for familial breast cancer genetic counselling: findings of three randomised controlled trials of two interventions.
By Wilson BJ, Torrance N, Mollison J, Wordsworth S, Gray JR, Haites NE, et al.
-
Randomised evaluation of alternative electrosurgical modalities to treat bladder outflow obstruction in men with benign prostatic hyperplasia.
By Fowler C, McAllister W, Plail R, Karim O, Yang Q.
-
A pragmatic randomised controlled trial of the cost-effectiveness of palliative therapies for patients with inoperable oesophageal cancer.
By Shenfine J, McNamee P, Steen N, Bond J, Griffin SM.
-
Impact of computer-aided detection prompts on the sensitivity and specificity of screening mammography.
By Taylor P, Champness J, Given- Wilson R, Johnston K, Potts H.
-
Issues in data monitoring and interim analysis of trials.
By Grant AM, Altman DG, Babiker AB, Campbell MK, Clemens FJ, Darbyshire JH, et al.
-
Lay public’s understanding of equipoise and randomisation in randomised controlled trials.
By Robinson EJ, Kerr CEP, Stevens AJ, Lilford RJ, Braunholtz DA, Edwards SJ, et al.
-
Clinical and cost-effectiveness of electroconvulsive therapy for depressive illness, schizophrenia, catatonia and mania: systematic reviews and economic modelling studies.
By Greenhalgh J, Knight C, Hind D, Beverley C, Walters S.
-
Measurement of health-related quality of life for people with dementia: development of a new instrument (DEMQOL) and an evaluation of current methodology.
By Smith SC, Lamping DL, Banerjee S, Harwood R, Foley B, Smith P, et al.
-
Clinical effectiveness and cost-effectiveness of drotrecogin alfa (activated) (Xigris®) for the treatment of severe sepsis in adults: a systematic review and economic evaluation.
By Green C, Dinnes J, Takeda A, Shepherd J, Hartwell D, Cave C, et al.
-
A methodological review of how heterogeneity has been examined in systematic reviews of diagnostic test accuracy.
By Dinnes J, Deeks J, Kirby J, Roderick P.
-
Cervical screening programmes: can automation help? Evidence from systematic reviews, an economic analysis and a simulation modelling exercise applied to the UK.
By Willis BH, Barton P, Pearmain P, Bryan S, Hyde C.
-
Laparoscopic surgery for inguinal hernia repair: systematic review of effectiveness and economic evaluation.
By McCormack K, Wake B, Perez J, Fraser C, Cook J, McIntosh E, et al.
-
Clinical effectiveness, tolerability and cost-effectiveness of newer drugs for epilepsy in adults: a systematic review and economic evaluation.
By Wilby J, Kainth A, Hawkins N, Epstein D, McIntosh H, McDaid C, et al.
-
A randomised controlled trial to compare the cost-effectiveness of tricyclic antidepressants, selective serotonin reuptake inhibitors and lofepramine.
By Peveler R, Kendrick T, Buxton M, Longworth L, Baldwin D, Moore M, et al.
-
Clinical effectiveness and cost-effectiveness of immediate angioplasty for acute myocardial infarction: systematic review and economic evaluation.
By Hartwell D, Colquitt J, Loveman E, Clegg AJ, Brodin H, Waugh N, et al.
-
A randomised controlled comparison of alternative strategies in stroke care.
By Kalra L, Evans A, Perez I, Knapp M, Swift C, Donaldson N.
-
The investigation and analysis of critical incidents and adverse events in healthcare.
By Woloshynowych M, Rogers S, Taylor-Adams S, Vincent C.
-
Potential use of routine databases in health technology assessment.
By Raftery J, Roderick P, Stevens A.
-
Clinical and cost-effectiveness of newer immunosuppressive regimens in renal transplantation: a systematic review and modelling study.
By Woodroffe R, Yao GL, Meads C, Bayliss S, Ready A, Raftery J, et al.
-
A systematic review and economic evaluation of alendronate, etidronate, risedronate, raloxifene and teriparatide for the prevention and treatment of postmenopausal osteoporosis.
By Stevenson M, Lloyd Jones M, De Nigris E, Brewer N, Davis S, Oakley J.
-
A systematic review to examine the impact of psycho-educational interventions on health outcomes and costs in adults and children with difficult asthma.
By Smith JR, Mugford M, Holland R, Candy B, Noble MJ, Harrison BDW, et al.
-
An evaluation of the costs, effectiveness and quality of renal replacement therapy provision in renal satellite units in England and Wales.
By Roderick P, Nicholson T, Armitage A, Mehta R, Mullee M, Gerard K, et al.
-
Imatinib for the treatment of patients with unresectable and/or metastatic gastrointestinal stromal tumours: systematic review and economic evaluation.
By Wilson J, Connock M, Song F, Yao G, Fry-Smith A, Raftery J, et al.
-
Indirect comparisons of competing interventions.
By Glenny AM, Altman DG, Song F, Sakarovitch C, Deeks JJ, D’Amico R, et al.
-
Cost-effectiveness of alternative strategies for the initial medical management of non-ST elevation acute coronary syndrome: systematic review and decision-analytical modelling.
By Robinson M, Palmer S, Sculpher M, Philips Z, Ginnelly L, Bowens A, et al.
-
Outcomes of electrically stimulated gracilis neosphincter surgery.
By Tillin T, Chambers M, Feldman R.
-
The effectiveness and cost-effectiveness of pimecrolimus and tacrolimus for atopic eczema: a systematic review and economic evaluation.
By Garside R, Stein K, Castelnuovo E, Pitt M, Ashcroft D, Dimmock P, et al.
-
Systematic review on urine albumin testing for early detection of diabetic complications.
By Newman DJ, Mattock MB, Dawnay ABS, Kerry S, McGuire A, Yaqoob M, et al.
-
Randomised controlled trial of the cost-effectiveness of water-based therapy for lower limb osteoarthritis.
By Cochrane T, Davey RC, Matthes Edwards SM.
-
Longer term clinical and economic benefits of offering acupuncture care to patients with chronic low back pain.
By Thomas KJ, MacPherson H, Ratcliffe J, Thorpe L, Brazier J, Campbell M, et al.
-
Cost-effectiveness and safety of epidural steroids in the management of sciatica.
By Price C, Arden N, Coglan L, Rogers P.
-
The British Rheumatoid Outcome Study Group (BROSG) randomised controlled trial to compare the effectiveness and cost-effectiveness of aggressive versus symptomatic therapy in established rheumatoid arthritis.
By Symmons D, Tricker K, Roberts C, Davies L, Dawes P, Scott DL.
-
Conceptual framework and systematic review of the effects of participants’ and professionals’ preferences in randomised controlled trials.
By King M, Nazareth I, Lampe F, Bower P, Chandler M, Morou M, et al.
-
The clinical and cost-effectiveness of implantable cardioverter defibrillators: a systematic review.
By Bryant J, Brodin H, Loveman E, Payne E, Clegg A.
-
A trial of problem-solving by community mental health nurses for anxiety, depression and life difficulties among general practice patients. The CPN-GP study.
By Kendrick T, Simons L, Mynors-Wallis L, Gray A, Lathlean J, Pickering R, et al.
-
The causes and effects of socio-demographic exclusions from clinical trials.
By Bartlett C, Doyal L, Ebrahim S, Davey P, Bachmann M, Egger M, et al.
-
Is hydrotherapy cost-effective? A randomised controlled trial of combined hydrotherapy programmes compared with physiotherapy land techniques in children with juvenile idiopathic arthritis.
By Epps H, Ginnelly L, Utley M, Southwood T, Gallivan S, Sculpher M, et al.
-
A randomised controlled trial and cost-effectiveness study of systematic screening (targeted and total population screening) versus routine practice for the detection of atrial fibrillation in people aged 65 and over. The SAFE study.
By Hobbs FDR, Fitzmaurice DA, Mant J, Murray E, Jowett S, Bryan S, et al.
-
Displaced intracapsular hip fractures in fit, older people: a randomised comparison of reduction and fixation, bipolar hemiarthroplasty and total hip arthroplasty.
By Keating JF, Grant A, Masson M, Scott NW, Forbes JF.
-
Long-term outcome of cognitive behaviour therapy clinical trials in central Scotland.
By Durham RC, Chambers JA, Power KG, Sharp DM, Macdonald RR, Major KA, et al.
-
The effectiveness and cost-effectiveness of dual-chamber pacemakers compared with single-chamber pacemakers for bradycardia due to atrioventricular block or sick sinus syndrome: systematic review and economic evaluation.
By Castelnuovo E, Stein K, Pitt M, Garside R, Payne E.
-
Newborn screening for congenital heart defects: a systematic review and cost-effectiveness analysis.
By Knowles R, Griebsch I, Dezateux C, Brown J, Bull C, Wren C.
-
The clinical and cost-effectiveness of left ventricular assist devices for end-stage heart failure: a systematic review and economic evaluation.
By Clegg AJ, Scott DA, Loveman E, Colquitt J, Hutchinson J, Royle P, et al.
-
The effectiveness of the Heidelberg Retina Tomograph and laser diagnostic glaucoma scanning system (GDx) in detecting and monitoring glaucoma.
By Kwartz AJ, Henson DB, Harper RA, Spencer AF, McLeod D.
-
Clinical and cost-effectiveness of autologous chondrocyte implantation for cartilage defects in knee joints: systematic review and economic evaluation.
By Clar C, Cummins E, McIntyre L, Thomas S, Lamb J, Bain L, et al.
-
Systematic review of effectiveness of different treatments for childhood retinoblastoma.
By McDaid C, Hartley S, Bagnall A-M, Ritchie G, Light K, Riemsma R.
-
Towards evidence-based guidelines for the prevention of venous thromboembolism: systematic reviews of mechanical methods, oral anticoagulation, dextran and regional anaesthesia as thromboprophylaxis.
By Roderick P, Ferris G, Wilson K, Halls H, Jackson D, Collins R, et al.
-
The effectiveness and cost-effectiveness of parent training/education programmes for the treatment of conduct disorder, including oppositional defiant disorder, in children.
By Dretzke J, Frew E, Davenport C, Barlow J, Stewart-Brown S, Sandercock J, et al.
-
The clinical and cost-effectiveness of donepezil, rivastigmine, galantamine and memantine for Alzheimer’s disease.
By Loveman E, Green C, Kirby J, Takeda A, Picot J, Payne E, et al.
-
FOOD: a multicentre randomised trial evaluating feeding policies in patients admitted to hospital with a recent stroke.
By Dennis M, Lewis S, Cranswick G, Forbes J.
-
The clinical effectiveness and cost-effectiveness of computed tomography screening for lung cancer: systematic reviews.
By Black C, Bagust A, Boland A, Walker S, McLeod C, De Verteuil R, et al.
-
A systematic review of the effectiveness and cost-effectiveness of neuroimaging assessments used to visualise the seizure focus in people with refractory epilepsy being considered for surgery.
By Whiting P, Gupta R, Burch J, Mujica Mota RE, Wright K, Marson A, et al.
-
Comparison of conference abstracts and presentations with full-text articles in the health technology assessments of rapidly evolving technologies.
By Dundar Y, Dodd S, Dickson R, Walley T, Haycox A, Williamson PR.
-
Systematic review and evaluation of methods of assessing urinary incontinence.
By Martin JL, Williams KS, Abrams KR, Turner DA, Sutton AJ, Chapple C, et al.
-
The clinical effectiveness and cost-effectiveness of newer drugs for children with epilepsy. A systematic review.
By Connock M, Frew E, Evans B-W, Bryan S, Cummins C, Fry-Smith A, et al.
-
Surveillance of Barrett’s oesophagus: exploring the uncertainty through systematic review, expert workshop and economic modelling.
By Garside R, Pitt M, Somerville M, Stein K, Price A, Gilbert N.
-
Topotecan, pegylated liposomal doxorubicin hydrochloride and paclitaxel for second-line or subsequent treatment of advanced ovarian cancer: a systematic review and economic evaluation.
By Main C, Bojke L, Griffin S, Norman G, Barbieri M, Mather L, et al.
-
Evaluation of molecular techniques in prediction and diagnosis of cytomegalovirus disease in immunocompromised patients.
By Szczepura A, Westmoreland D, Vinogradova Y, Fox J, Clark M.
-
Screening for thrombophilia in high-risk situations: systematic review and cost-effectiveness analysis. The Thrombosis: Risk and Economic Assessment of Thrombophilia Screening (TREATS) study.
By Wu O, Robertson L, Twaddle S, Lowe GDO, Clark P, Greaves M, et al.
-
A series of systematic reviews to inform a decision analysis for sampling and treating infected diabetic foot ulcers.
By Nelson EA, O’Meara S, Craig D, Iglesias C, Golder S, Dalton J, et al.
-
Randomised clinical trial, observational study and assessment of cost-effectiveness of the treatment of varicose veins (REACTIV trial).
By Michaels JA, Campbell WB, Brazier JE, MacIntyre JB, Palfreyman SJ, Ratcliffe J, et al.
-
The cost-effectiveness of screening for oral cancer in primary care.
By Speight PM, Palmer S, Moles DR, Downer MC, Smith DH, Henriksson M, et al.
-
Measurement of the clinical and cost-effectiveness of non-invasive diagnostic testing strategies for deep vein thrombosis.
By Goodacre S, Sampson F, Stevenson M, Wailoo A, Sutton A, Thomas S, et al.
-
Systematic review of the effectiveness and cost-effectiveness of HealOzone® for the treatment of occlusal pit/fissure caries and root caries.
By Brazzelli M, McKenzie L, Fielding S, Fraser C, Clarkson J, Kilonzo M, et al.
-
Randomised controlled trials of conventional antipsychotic versus new atypical drugs, and new atypical drugs versus clozapine, in people with schizophrenia responding poorly to, or intolerant of, current drug treatment.
By Lewis SW, Davies L, Jones PB, Barnes TRE, Murray RM, Kerwin R, et al.
-
Diagnostic tests and algorithms used in the investigation of haematuria: systematic reviews and economic evaluation.
By Rodgers M, Nixon J, Hempel S, Aho T, Kelly J, Neal D, et al.
-
Cognitive behavioural therapy in addition to antispasmodic therapy for irritable bowel syndrome in primary care: randomised controlled trial.
By Kennedy TM, Chalder T, McCrone P, Darnley S, Knapp M, Jones RH, et al.
-
A systematic review of the clinical effectiveness and cost-effectiveness of enzyme replacement therapies for Fabry’s disease and mucopolysaccharidosis type 1.
By Connock M, Juarez-Garcia A, Frew E, Mans A, Dretzke J, Fry-Smith A, et al.
-
Health benefits of antiviral therapy for mild chronic hepatitis C: randomised controlled trial and economic evaluation.
By Wright M, Grieve R, Roberts J, Main J, Thomas HC, on behalf of the UK Mild Hepatitis C Trial Investigators.
-
Pressure relieving support surfaces: a randomised evaluation.
By Nixon J, Nelson EA, Cranny G, Iglesias CP, Hawkins K, Cullum NA, et al.
-
A systematic review and economic model of the effectiveness and cost-effectiveness of methylphenidate, dexamfetamine and atomoxetine for the treatment of attention deficit hyperactivity disorder in children and adolescents.
By King S, Griffin S, Hodges Z, Weatherly H, Asseburg C, Richardson G, et al.
-
The clinical effectiveness and cost-effectiveness of enzyme replacement therapy for Gaucher’s disease: a systematic review.
By Connock M, Burls A, Frew E, Fry-Smith A, Juarez-Garcia A, McCabe C, et al.
-
Effectiveness and cost-effectiveness of salicylic acid and cryotherapy for cutaneous warts. An economic decision model.
By Thomas KS, Keogh-Brown MR, Chalmers JR, Fordham RJ, Holland RC, Armstrong SJ, et al.
-
A systematic literature review of the effectiveness of non-pharmacological interventions to prevent wandering in dementia and evaluation of the ethical implications and acceptability of their use.
By Robinson L, Hutchings D, Corner L, Beyer F, Dickinson H, Vanoli A, et al.
-
A review of the evidence on the effects and costs of implantable cardioverter defibrillator therapy in different patient groups, and modelling of cost-effectiveness and cost–utility for these groups in a UK context.
By Buxton M, Caine N, Chase D, Connelly D, Grace A, Jackson C, et al.
-
Adefovir dipivoxil and pegylated interferon alfa-2a for the treatment of chronic hepatitis B: a systematic review and economic evaluation.
By Shepherd J, Jones J, Takeda A, Davidson P, Price A.
-
An evaluation of the clinical and cost-effectiveness of pulmonary artery catheters in patient management in intensive care: a systematic review and a randomised controlled trial.
By Harvey S, Stevens K, Harrison D, Young D, Brampton W, McCabe C, et al.
-
Accurate, practical and cost-effective assessment of carotid stenosis in the UK.
By Wardlaw JM, Chappell FM, Stevenson M, De Nigris E, Thomas S, Gillard J, et al.
-
Etanercept and infliximab for the treatment of psoriatic arthritis: a systematic review and economic evaluation.
By Woolacott N, Bravo Vergel Y, Hawkins N, Kainth A, Khadjesari Z, Misso K, et al.
-
The cost-effectiveness of testing for hepatitis C in former injecting drug users.
By Castelnuovo E, Thompson-Coon J, Pitt M, Cramp M, Siebert U, Price A, et al.
-
Computerised cognitive behaviour therapy for depression and anxiety update: a systematic review and economic evaluation.
By Kaltenthaler E, Brazier J, De Nigris E, Tumur I, Ferriter M, Beverley C, et al.
-
Cost-effectiveness of using prognostic information to select women with breast cancer for adjuvant systemic therapy.
By Williams C, Brunskill S, Altman D, Briggs A, Campbell H, Clarke M, et al.
-
Psychological therapies including dialectical behaviour therapy for borderline personality disorder: a systematic review and preliminary economic evaluation.
By Brazier J, Tumur I, Holmes M, Ferriter M, Parry G, Dent-Brown K, et al.
-
Clinical effectiveness and cost-effectiveness of tests for the diagnosis and investigation of urinary tract infection in children: a systematic review and economic model.
By Whiting P, Westwood M, Bojke L, Palmer S, Richardson G, Cooper J, et al.
-
Cognitive behavioural therapy in chronic fatigue syndrome: a randomised controlled trial of an outpatient group programme.
By O’Dowd H, Gladwell P, Rogers CA, Hollinghurst S, Gregory A.
-
A comparison of the cost-effectiveness of five strategies for the prevention of nonsteroidal anti-inflammatory drug-induced gastrointestinal toxicity: a systematic review with economic modelling.
By Brown TJ, Hooper L, Elliott RA, Payne K, Webb R, Roberts C, et al.
-
The effectiveness and cost-effectiveness of computed tomography screening for coronary artery disease: systematic review.
By Waugh N, Black C, Walker S, McIntyre L, Cummins E, Hillis G.
-
What are the clinical outcome and cost-effectiveness of endoscopy undertaken by nurses when compared with doctors? A Multi-Institution Nurse Endoscopy Trial (MINuET).
By Williams J, Russell I, Durai D, Cheung W-Y, Farrin A, Bloor K, et al.
-
The clinical and cost-effectiveness of oxaliplatin and capecitabine for the adjuvant treatment of colon cancer: systematic review and economic evaluation.
By Pandor A, Eggington S, Paisley S, Tappenden P, Sutcliffe P.
-
A systematic review of the effectiveness of adalimumab, etanercept and infliximab for the treatment of rheumatoid arthritis in adults and an economic evaluation of their cost-effectiveness.
By Chen Y-F, Jobanputra P, Barton P, Jowett S, Bryan S, Clark W, et al.
-
Telemedicine in dermatology: a randomised controlled trial.
By Bowns IR, Collins K, Walters SJ, McDonagh AJG.
-
Cost-effectiveness of cell salvage and alternative methods of minimising perioperative allogeneic blood transfusion: a systematic review and economic model.
By Davies L, Brown TJ, Haynes S, Payne K, Elliott RA, McCollum C.
-
Clinical effectiveness and cost-effectiveness of laparoscopic surgery for colorectal cancer: systematic reviews and economic evaluation.
By Murray A, Lourenco T, de Verteuil R, Hernandez R, Fraser C, McKinley A, et al.
-
Etanercept and efalizumab for the treatment of psoriasis: a systematic review.
By Woolacott N, Hawkins N, Mason A, Kainth A, Khadjesari Z, Bravo Vergel Y, et al.
-
Systematic reviews of clinical decision tools for acute abdominal pain.
By Liu JLY, Wyatt JC, Deeks JJ, Clamp S, Keen J, Verde P, et al.
-
Evaluation of the ventricular assist device programme in the UK.
By Sharples L, Buxton M, Caine N, Cafferty F, Demiris N, Dyer M, et al.
-
A systematic review and economic model of the clinical and cost-effectiveness of immunosuppressive therapy for renal transplantation in children.
By Yao G, Albon E, Adi Y, Milford D, Bayliss S, Ready A, et al.
-
Amniocentesis results: investigation of anxiety. The ARIA trial.
By Hewison J, Nixon J, Fountain J, Cocks K, Jones C, Mason G, et al.
-
Pemetrexed disodium for the treatment of malignant pleural mesothelioma: a systematic review and economic evaluation.
By Dundar Y, Bagust A, Dickson R, Dodd S, Green J, Haycox A, et al.
-
A systematic review and economic model of the clinical effectiveness and cost-effectiveness of docetaxel in combination with prednisone or prednisolone for the treatment of hormone-refractory metastatic prostate cancer.
By Collins R, Fenwick E, Trowman R, Perard R, Norman G, Light K, et al.
-
A systematic review of rapid diagnostic tests for the detection of tuberculosis infection.
By Dinnes J, Deeks J, Kunst H, Gibson A, Cummins E, Waugh N, et al.
-
The clinical effectiveness and cost-effectiveness of strontium ranelate for the prevention of osteoporotic fragility fractures in postmenopausal women.
By Stevenson M, Davis S, Lloyd-Jones M, Beverley C.
-
A systematic review of quantitative and qualitative research on the role and effectiveness of written information available to patients about individual medicines.
By Raynor DK, Blenkinsopp A, Knapp P, Grime J, Nicolson DJ, Pollock K, et al.
-
Oral naltrexone as a treatment for relapse prevention in formerly opioid-dependent drug users: a systematic review and economic evaluation.
By Adi Y, Juarez-Garcia A, Wang D, Jowett S, Frew E, Day E, et al.
-
Glucocorticoid-induced osteoporosis: a systematic review and cost–utility analysis.
By Kanis JA, Stevenson M, McCloskey EV, Davis S, Lloyd-Jones M.
-
Epidemiological, social, diagnostic and economic evaluation of population screening for genital chlamydial infection.
By Low N, McCarthy A, Macleod J, Salisbury C, Campbell R, Roberts TE, et al.
-
Methadone and buprenorphine for the management of opioid dependence: a systematic review and economic evaluation.
By Connock M, Juarez-Garcia A, Jowett S, Frew E, Liu Z, Taylor RJ, et al.
-
Exercise Evaluation Randomised Trial (EXERT): a randomised trial comparing GP referral for leisure centre-based exercise, community-based walking and advice only.
By Isaacs AJ, Critchley JA, See Tai S, Buckingham K, Westley D, Harridge SDR, et al.
-
Interferon alfa (pegylated and non-pegylated) and ribavirin for the treatment of mild chronic hepatitis C: a systematic review and economic evaluation.
By Shepherd J, Jones J, Hartwell D, Davidson P, Price A, Waugh N.
-
Systematic review and economic evaluation of bevacizumab and cetuximab for the treatment of metastatic colorectal cancer.
By Tappenden P, Jones R, Paisley S, Carroll C.
-
A systematic review and economic evaluation of epoetin alfa, epoetin beta and darbepoetin alfa in anaemia associated with cancer, especially that attributable to cancer treatment.
By Wilson J, Yao GL, Raftery J, Bohlius J, Brunskill S, Sandercock J, et al.
-
A systematic review and economic evaluation of statins for the prevention of coronary events.
By Ward S, Lloyd Jones M, Pandor A, Holmes M, Ara R, Ryan A, et al.
-
A systematic review of the effectiveness and cost-effectiveness of different models of community-based respite care for frail older people and their carers.
By Mason A, Weatherly H, Spilsbury K, Arksey H, Golder S, Adamson J, et al.
-
Additional therapy for young children with spastic cerebral palsy: a randomised controlled trial.
By Weindling AM, Cunningham CC, Glenn SM, Edwards RT, Reeves DJ.
-
Screening for type 2 diabetes: literature review and economic modelling.
By Waugh N, Scotland G, McNamee P, Gillett M, Brennan A, Goyder E, et al.
-
The effectiveness and cost-effectiveness of cinacalcet for secondary hyperparathyroidism in end-stage renal disease patients on dialysis: a systematic review and economic evaluation.
By Garside R, Pitt M, Anderson R, Mealing S, Roome C, Snaith A, et al.
-
The clinical effectiveness and cost-effectiveness of gemcitabine for metastatic breast cancer: a systematic review and economic evaluation.
By Takeda AL, Jones J, Loveman E, Tan SC, Clegg AJ.
-
A systematic review of duplex ultrasound, magnetic resonance angiography and computed tomography angiography for the diagnosis and assessment of symptomatic, lower limb peripheral arterial disease.
By Collins R, Cranny G, Burch J, Aguiar-Ibáñez R, Craig D, Wright K, et al.
-
The clinical effectiveness and cost-effectiveness of treatments for children with idiopathic steroid-resistant nephrotic syndrome: a systematic review.
By Colquitt JL, Kirby J, Green C, Cooper K, Trompeter RS.
-
A systematic review of the routine monitoring of growth in children of primary school age to identify growth-related conditions.
By Fayter D, Nixon J, Hartley S, Rithalia A, Butler G, Rudolf M, et al.
-
Systematic review of the effectiveness of preventing and treating Staphylococcus aureus carriage in reducing peritoneal catheter-related infections.
By McCormack K, Rabindranath K, Kilonzo M, Vale L, Fraser C, McIntyre L, et al.
-
The clinical effectiveness and cost of repetitive transcranial magnetic stimulation versus electroconvulsive therapy in severe depression: a multicentre pragmatic randomised controlled trial and economic analysis.
By McLoughlin DM, Mogg A, Eranti S, Pluck G, Purvis R, Edwards D, et al.
-
A randomised controlled trial and economic evaluation of direct versus indirect and individual versus group modes of speech and language therapy for children with primary language impairment.
By Boyle J, McCartney E, Forbes J, O’Hare A.
-
Hormonal therapies for early breast cancer: systematic review and economic evaluation.
By Hind D, Ward S, De Nigris E, Simpson E, Carroll C, Wyld L.
-
Cardioprotection against the toxic effects of anthracyclines given to children with cancer: a systematic review.
By Bryant J, Picot J, Levitt G, Sullivan I, Baxter L, Clegg A.
-
Adalimumab, etanercept and infliximab for the treatment of ankylosing spondylitis: a systematic review and economic evaluation.
By McLeod C, Bagust A, Boland A, Dagenais P, Dickson R, Dundar Y, et al.
-
Prenatal screening and treatment strategies to prevent group B streptococcal and other bacterial infections in early infancy: cost-effectiveness and expected value of information analyses.
By Colbourn T, Asseburg C, Bojke L, Philips Z, Claxton K, Ades AE, et al.
-
Clinical effectiveness and cost-effectiveness of bone morphogenetic proteins in the non-healing of fractures and spinal fusion: a systematic review.
By Garrison KR, Donell S, Ryder J, Shemilt I, Mugford M, Harvey I, et al.
-
A randomised controlled trial of postoperative radiotherapy following breast-conserving surgery in a minimum-risk older population. The PRIME trial.
By Prescott RJ, Kunkler IH, Williams LJ, King CC, Jack W, van der Pol M, et al.
-
Current practice, accuracy, effectiveness and cost-effectiveness of the school entry hearing screen.
By Bamford J, Fortnum H, Bristow K, Smith J, Vamvakas G, Davies L, et al.
-
The clinical effectiveness and cost-effectiveness of inhaled insulin in diabetes mellitus: a systematic review and economic evaluation.
By Black C, Cummins E, Royle P, Philip S, Waugh N.
-
Surveillance of cirrhosis for hepatocellular carcinoma: systematic review and economic analysis.
By Thompson Coon J, Rogers G, Hewson P, Wright D, Anderson R, Cramp M, et al.
-
The Birmingham Rehabilitation Uptake Maximisation Study (BRUM). Homebased compared with hospital-based cardiac rehabilitation in a multi-ethnic population: cost-effectiveness and patient adherence.
By Jolly K, Taylor R, Lip GYH, Greenfield S, Raftery J, Mant J, et al.
-
A systematic review of the clinical, public health and cost-effectiveness of rapid diagnostic tests for the detection and identification of bacterial intestinal pathogens in faeces and food.
By Abubakar I, Irvine L, Aldus CF, Wyatt GM, Fordham R, Schelenz S, et al.
-
A randomised controlled trial examining the longer-term outcomes of standard versus new antiepileptic drugs. The SANAD trial.
By Marson AG, Appleton R, Baker GA, Chadwick DW, Doughty J, Eaton B, et al.
-
Clinical effectiveness and cost-effectiveness of different models of managing long-term oral anti-coagulation therapy: a systematic review and economic modelling.
By Connock M, Stevens C, Fry-Smith A, Jowett S, Fitzmaurice D, Moore D, et al.
-
A systematic review and economic model of the clinical effectiveness and cost-effectiveness of interventions for preventing relapse in people with bipolar disorder.
By Soares-Weiser K, Bravo Vergel Y, Beynon S, Dunn G, Barbieri M, Duffy S, et al.
-
Taxanes for the adjuvant treatment of early breast cancer: systematic review and economic evaluation.
By Ward S, Simpson E, Davis S, Hind D, Rees A, Wilkinson A.
-
The clinical effectiveness and cost-effectiveness of screening for open angle glaucoma: a systematic review and economic evaluation.
By Burr JM, Mowatt G, Hernández R, Siddiqui MAR, Cook J, Lourenco T, et al.
-
Acceptability, benefit and costs of early screening for hearing disability: a study of potential screening tests and models.
By Davis A, Smith P, Ferguson M, Stephens D, Gianopoulos I.
-
Contamination in trials of educational interventions.
By Keogh-Brown MR, Bachmann MO, Shepstone L, Hewitt C, Howe A, Ramsay CR, et al.
-
Overview of the clinical effectiveness of positron emission tomography imaging in selected cancers.
By Facey K, Bradbury I, Laking G, Payne E.
-
The effectiveness and cost-effectiveness of carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma: a systematic review and economic evaluation.
By Garside R, Pitt M, Anderson R, Rogers G, Dyer M, Mealing S, et al.
-
Drug-eluting stents: a systematic review and economic evaluation.
By Hill RA, Boland A, Dickson R, Dündar Y, Haycox A, McLeod C, et al.
-
The clinical effectiveness and cost-effectiveness of cardiac resynchronisation (biventricular pacing) for heart failure: systematic review and economic model.
By Fox M, Mealing S, Anderson R, Dean J, Stein K, Price A, et al.
-
Recruitment to randomised trials: strategies for trial enrolment and participation study. The STEPS study.
By Campbell MK, Snowdon C, Francis D, Elbourne D, McDonald AM, Knight R, et al.
-
Cost-effectiveness of functional cardiac testing in the diagnosis and management of coronary artery disease: a randomised controlled trial. The CECaT trial.
By Sharples L, Hughes V, Crean A, Dyer M, Buxton M, Goldsmith K, et al.
-
Evaluation of diagnostic tests when there is no gold standard. A review of methods.
By Rutjes AWS, Reitsma JB, Coomarasamy A, Khan KS, Bossuyt PMM.
-
Systematic reviews of the clinical effectiveness and cost-effectiveness of proton pump inhibitors in acute upper gastrointestinal bleeding.
By Leontiadis GI, Sreedharan A, Dorward S, Barton P, Delaney B, Howden CW, et al.
-
A review and critique of modelling in prioritising and designing screening programmes.
By Karnon J, Goyder E, Tappenden P, McPhie S, Towers I, Brazier J, et al.
-
An assessment of the impact of the NHS Health Technology Assessment Programme.
By Hanney S, Buxton M, Green C, Coulson D, Raftery J.
-
A systematic review and economic model of switching from nonglycopeptide to glycopeptide antibiotic prophylaxis for surgery.
By Cranny G, Elliott R, Weatherly H, Chambers D, Hawkins N, Myers L, et al.
-
‘Cut down to quit’ with nicotine replacement therapies in smoking cessation: a systematic review of effectiveness and economic analysis.
By Wang D, Connock M, Barton P, Fry-Smith A, Aveyard P, Moore D.
-
A systematic review of the effectiveness of strategies for reducing fracture risk in children with juvenile idiopathic arthritis with additional data on long-term risk of fracture and cost of disease management.
By Thornton J, Ashcroft D, O’Neill T, Elliott R, Adams J, Roberts C, et al.
-
Does befriending by trained lay workers improve psychological well-being and quality of life for carers of people with dementia, and at what cost? A randomised controlled trial.
By Charlesworth G, Shepstone L, Wilson E, Thalanany M, Mugford M, Poland F.
-
A multi-centre retrospective cohort study comparing the efficacy, safety and cost-effectiveness of hysterectomy and uterine artery embolisation for the treatment of symptomatic uterine fibroids. The HOPEFUL study.
By Hirst A, Dutton S, Wu O, Briggs A, Edwards C, Waldenmaier L, et al.
-
Methods of prediction and prevention of pre-eclampsia: systematic reviews of accuracy and effectiveness literature with economic modelling.
By Meads CA, Cnossen JS, Meher S, Juarez-Garcia A, ter Riet G, Duley L, et al.
-
The use of economic evaluations in NHS decision-making: a review and empirical investigation.
By Williams I, McIver S, Moore D, Bryan S.
-
Stapled haemorrhoidectomy (haemorrhoidopexy) for the treatment of haemorrhoids: a systematic review and economic evaluation.
By Burch J, Epstein D, Baba-Akbari A, Weatherly H, Fox D, Golder S, et al.
-
The clinical effectiveness of diabetes education models for Type 2 diabetes: a systematic review.
By Loveman E, Frampton GK, Clegg AJ.
-
Payment to healthcare professionals for patient recruitment to trials: systematic review and qualitative study.
By Raftery J, Bryant J, Powell J, Kerr C, Hawker S.
-
Cyclooxygenase-2 selective non-steroidal anti-inflammatory drugs (etodolac, meloxicam, celecoxib, rofecoxib, etoricoxib, valdecoxib and lumiracoxib) for osteoarthritis and rheumatoid arthritis: a systematic review and economic evaluation.
By Chen Y-F, Jobanputra P, Barton P, Bryan S, Fry-Smith A, Harris G, et al.
-
The clinical effectiveness and cost-effectiveness of central venous catheters treated with anti-infective agents in preventing bloodstream infections: a systematic review and economic evaluation.
By Hockenhull JC, Dwan K, Boland A, Smith G, Bagust A, Dundar Y, et al.
-
Stepped treatment of older adults on laxatives. The STOOL trial.
By Mihaylov S, Stark C, McColl E, Steen N, Vanoli A, Rubin G, et al.
-
A randomised controlled trial of cognitive behaviour therapy in adolescents with major depression treated by selective serotonin reuptake inhibitors. The ADAPT trial.
By Goodyer IM, Dubicka B, Wilkinson P, Kelvin R, Roberts C, Byford S, et al.
-
The use of irinotecan, oxaliplatin and raltitrexed for the treatment of advanced colorectal cancer: systematic review and economic evaluation.
By Hind D, Tappenden P, Tumur I, Eggington E, Sutcliffe P, Ryan A.
-
Ranibizumab and pegaptanib for the treatment of age-related macular degeneration: a systematic review and economic evaluation.
By Colquitt JL, Jones J, Tan SC, Takeda A, Clegg AJ, Price A.
-
Systematic review of the clinical effectiveness and cost-effectiveness of 64-slice or higher computed tomography angiography as an alternative to invasive coronary angiography in the investigation of coronary artery disease.
By Mowatt G, Cummins E, Waugh N, Walker S, Cook J, Jia X, et al.
-
Structural neuroimaging in psychosis: a systematic review and economic evaluation.
By Albon E, Tsourapas A, Frew E, Davenport C, Oyebode F, Bayliss S, et al.
-
Systematic review and economic analysis of the comparative effectiveness of different inhaled corticosteroids and their usage with long-acting beta2 agonists for the treatment of chronic asthma in adults and children aged 12 years and over.
By Shepherd J, Rogers G, Anderson R, Main C, Thompson-Coon J, Hartwell D, et al.
-
Systematic review and economic analysis of the comparative effectiveness of different inhaled corticosteroids and their usage with long-acting beta2 agonists for the treatment of chronic asthma in children under the age of 12 years.
By Main C, Shepherd J, Anderson R, Rogers G, Thompson-Coon J, Liu Z, et al.
-
Ezetimibe for the treatment of hypercholesterolaemia: a systematic review and economic evaluation.
By Ara R, Tumur I, Pandor A, Duenas A, Williams R, Wilkinson A, et al.
-
Topical or oral ibuprofen for chronic knee pain in older people. The TOIB study.
By Underwood M, Ashby D, Carnes D, Castelnuovo E, Cross P, Harding G, et al.
-
A prospective randomised comparison of minor surgery in primary and secondary care. The MiSTIC trial.
By George S, Pockney P, Primrose J, Smith H, Little P, Kinley H, et al.
-
A review and critical appraisal of measures of therapist–patient interactions in mental health settings.
By Cahill J, Barkham M, Hardy G, Gilbody S, Richards D, Bower P, et al.
-
The clinical effectiveness and cost-effectiveness of screening programmes for amblyopia and strabismus in children up to the age of 4–5 years: a systematic review and economic evaluation.
By Carlton J, Karnon J, Czoski-Murray C, Smith KJ, Marr J.
-
A systematic review of the clinical effectiveness and cost-effectiveness and economic modelling of minimal incision total hip replacement approaches in the management of arthritic disease of the hip.
By de Verteuil R, Imamura M, Zhu S, Glazener C, Fraser C, Munro N, et al.
-
A preliminary model-based assessment of the cost–utility of a screening programme for early age-related macular degeneration.
By Karnon J, Czoski-Murray C, Smith K, Brand C, Chakravarthy U, Davis S, et al.
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.
By Shepherd J, Jones J, Frampton GK, Tanajewski L, Turner D, Price A.
-
Absorbent products for urinary/faecal incontinence: a comparative evaluation of key product categories.
By Fader M, Cottenden A, Getliffe K, Gage H, Clarke-O’Neill S, Jamieson K, et al.
-
A systematic review of repetitive functional task practice with modelling of resource use, costs and effectiveness.
By French B, Leathley M, Sutton C, McAdam J, Thomas L, Forster A, et al.
-
The effectiveness and cost-effectivness of minimal access surgery amongst people with gastro-oesophageal reflux disease – a UK collaborative study. The reflux trial.
By Grant A, Wileman S, Ramsay C, Bojke L, Epstein D, Sculpher M, et al.
-
Time to full publication of studies of anti-cancer medicines for breast cancer and the potential for publication bias: a short systematic review.
By Takeda A, Loveman E, Harris P, Hartwell D, Welch K.
-
Performance of screening tests for child physical abuse in accident and emergency departments.
By Woodman J, Pitt M, Wentz R, Taylor B, Hodes D, Gilbert RE.
-
Curative catheter ablation in atrial fibrillation and typical atrial flutter: systematic review and economic evaluation.
By Rodgers M, McKenna C, Palmer S, Chambers D, Van Hout S, Golder S, et al.
-
Systematic review and economic modelling of effectiveness and cost utility of surgical treatments for men with benign prostatic enlargement.
By Lourenco T, Armstrong N, N’Dow J, Nabi G, Deverill M, Pickard R, et al.
-
Immunoprophylaxis against respiratory syncytial virus (RSV) with palivizumab in children: a systematic review and economic evaluation.
By Wang D, Cummins C, Bayliss S, Sandercock J, Burls A.
-
Deferasirox for the treatment of iron overload associated with regular blood transfusions (transfusional haemosiderosis) in patients suffering with chronic anaemia: a systematic review and economic evaluation.
By McLeod C, Fleeman N, Kirkham J, Bagust A, Boland A, Chu P, et al.
-
Thrombophilia testing in people with venous thromboembolism: systematic review and cost-effectiveness analysis.
By Simpson EL, Stevenson MD, Rawdin A, Papaioannou D.
-
Surgical procedures and non-surgical devices for the management of non-apnoeic snoring: a systematic review of clinical effects and associated treatment costs.
By Main C, Liu Z, Welch K, Weiner G, Quentin Jones S, Stein K.
-
Continuous positive airway pressure devices for the treatment of obstructive sleep apnoea–hypopnoea syndrome: a systematic review and economic analysis.
By McDaid C, Griffin S, Weatherly H, Durée K, van der Burgt M, van Hout S, Akers J, et al.
-
Use of classical and novel biomarkers as prognostic risk factors for localised prostate cancer: a systematic review.
By Sutcliffe P, Hummel S, Simpson E, Young T, Rees A, Wilkinson A, et al.
-
The harmful health effects of recreational ecstasy: a systematic review of observational evidence.
By Rogers G, Elston J, Garside R, Roome C, Taylor R, Younger P, et al.
-
Systematic review of the clinical effectiveness and cost-effectiveness of oesophageal Doppler monitoring in critically ill and high-risk surgical patients.
By Mowatt G, Houston G, Hernández R, de Verteuil R, Fraser C, Cuthbertson B, et al.
-
The use of surrogate outcomes in model-based cost-effectiveness analyses: a survey of UK Health Technology Assessment reports.
By Taylor RS, Elston J.
-
Controlling Hypertension and Hypotension Immediately Post Stroke (CHHIPS) – a randomised controlled trial.
By Potter J, Mistri A, Brodie F, Chernova J, Wilson E, Jagger C, et al.
-
Routine antenatal anti-D prophylaxis for RhD-negative women: a systematic review and economic evaluation.
By Pilgrim H, Lloyd-Jones M, Rees A.
-
Amantadine, oseltamivir and zanamivir for the prophylaxis of influenza (including a review of existing guidance no. 67): a systematic review and economic evaluation.
By Tappenden P, Jackson R, Cooper K, Rees A, Simpson E, Read R, et al.
-
Improving the evaluation of therapeutic interventions in multiple sclerosis: the role of new psychometric methods.
By Hobart J, Cano S.
-
Treatment of severe ankle sprain: a pragmatic randomised controlled trial comparing the clinical effectiveness and cost-effectiveness of three types of mechanical ankle support with tubular bandage. The CAST trial.
By Cooke MW, Marsh JL, Clark M, Nakash R, Jarvis RM, Hutton JL, et al. , on behalf of the CAST trial group.
-
Non-occupational postexposure prophylaxis for HIV: a systematic review.
By Bryant J, Baxter L, Hird S.
-
Blood glucose self-monitoring in type 2 diabetes: a randomised controlled trial.
By Farmer AJ, Wade AN, French DP, Simon J, Yudkin P, Gray A, et al.
-
How far does screening women for domestic (partner) violence in different health-care settings meet criteria for a screening programme? Systematic reviews of nine UK National Screening Committee criteria.
By Feder G, Ramsay J, Dunne D, Rose M, Arsene C, Norman R, et al.
-
Spinal cord stimulation for chronic pain of neuropathic or ischaemic origin: systematic review and economic evaluation.
By Simpson, EL, Duenas A, Holmes MW, Papaioannou D, Chilcott J.
-
The role of magnetic resonance imaging in the identification of suspected acoustic neuroma: a systematic review of clinical and costeffectiveness and natural history.
By Fortnum H, O’Neill C, Taylor R, Lenthall R, Nikolopoulos T, Lightfoot G, et al.
-
Dipsticks and diagnostic algorithms in urinary tract infection: development and validation, randomised trial, economic analysis, observational cohort and qualitative study.
By Little P, Turner S, Rumsby K, Warner G, Moore M, Lowes JA, et al.
-
Systematic review of respite care in the frail elderly.
By Shaw C, McNamara R, Abrams K, Cannings-John R, Hood K, Longo M, et al.
-
Neuroleptics in the treatment of aggressive challenging behaviour for people with intellectual disabilities: a randomised controlled trial (NACHBID).
By Tyrer P, Oliver-Africano P, Romeo R, Knapp M, Dickens S, Bouras N, et al.
Health Technology Assessment programme
-
Director, NIHR HTA programme, Professor of Clinical Pharmacology, University of Liverpool
-
Director, Medical Care Research Unit, University of Sheffield
Prioritisation Strategy Group
-
Director, NIHR HTA programme, Professor of Clinical Pharmacology, University of Liverpool
-
Director, Medical Care Research Unit, University of Sheffield
-
Dr Bob Coates, Consultant Advisor, NETSCC, HTA
-
Dr Andrew Cook, Consultant Advisor, NETSCC, HTA
-
Dr Peter Davidson, Director of Science Support, NETSCC, HTA
-
Professor Robin E Ferner, Consultant Physician and Director, West Midlands Centre for Adverse Drug Reactions, City Hospital NHS Trust, Birmingham
-
Professor Paul Glasziou, Professor of Evidence-Based Medicine, University of Oxford
-
Dr Nick Hicks, Director of NHS Support, NETSCC, HTA
-
Dr Edmund Jessop, Medical Adviser, National Specialist, National Commissioning Group (NCG), Department of Health, London
-
Ms Lynn Kerridge, Chief Executive Officer, NETSCC and NETSCC, HTA
-
Dr Ruairidh Milne, Director of Strategy and Development, NETSCC
-
Ms Kay Pattison, Section Head, NHS R&D Programme, Department of Health
-
Ms Pamela Young, Specialist Programme Manager, NETSCC, HTA
HTA Commissioning Board
-
Director, NIHR HTA programme, Professor of Clinical Pharmacology, University of Liverpool
-
Director, Medical Care Research Unit, University of Sheffield
-
Senior Lecturer in General Practice, Department of Primary Health Care, University of Oxford
-
Professor Ann Ashburn, Professor of Rehabilitation and Head of Research, Southampton General Hospital
-
Professor Deborah Ashby, Professor of Medical Statistics, Queen Mary, University of London
-
Professor John Cairns, Professor of Health Economics, London School of Hygiene and Tropical Medicine
-
Professor Peter Croft, Director of Primary Care Sciences Research Centre, Keele University
-
Professor Nicky Cullum, Director of Centre for Evidence-Based Nursing, University of York
-
Professor Jenny Donovan, Professor of Social Medicine, University of Bristol
-
Professor Steve Halligan, Professor of Gastrointestinal Radiology, University College Hospital, London
-
Professor Freddie Hamdy, Professor of Urology, University of Sheffield
-
Professor Allan House, Professor of Liaison Psychiatry, University of Leeds
-
Dr Martin J Landray, Reader in Epidemiology, Honorary Consultant Physician, Clinical Trial Service Unit, University of Oxford?
-
Professor Stuart Logan, Director of Health & Social Care Research, The Peninsula Medical School, Universities of Exeter and Plymouth
-
Dr Rafael Perera, Lecturer in Medical Statisitics, Department of Primary Health Care, Univeristy of Oxford
-
Professor Ian Roberts, Professor of Epidemiology & Public Health, London School of Hygiene and Tropical Medicine
-
Professor Mark Sculpher, Professor of Health Economics, University of York
-
Professor Helen Smith, Professor of Primary Care, University of Brighton
-
Professor Kate Thomas, Professor of Complementary & Alternative Medicine Research, University of Leeds
-
Professor David John Torgerson, Director of York Trials Unit, University of York
-
Professor Hywel Williams, Professor of Dermato-Epidemiology, University of Nottingham
-
Ms Kay Pattison, Section Head, NHS R&D Programmes, Research and Development Directorate, Department of Health
-
Dr Morven Roberts, Clinical Trials Manager, Medical Research Council
Diagnostic Technologies & Screening Panel
-
Professor of Evidence-Based Medicine, University of Oxford
-
Consultant Paediatrician and Honorary Senior Lecturer, Great Ormond Street Hospital, London
-
Professor Judith E Adams, Consultant Radiologist, Manchester Royal Infirmary, Central Manchester & Manchester Children’s University Hospitals NHS Trust, and Professor of Diagnostic Radiology, Imaging Science and Biomedical Engineering, Cancer & Imaging Sciences, University of Manchester
-
Ms Jane Bates, Consultant Ultrasound Practitioner, Ultrasound Department, Leeds Teaching Hospital NHS Trust
-
Dr Stephanie Dancer, Consultant Microbiologist, Hairmyres Hospital, East Kilbride
-
Professor Glyn Elwyn, Primary Medical Care Research Group, Swansea Clinical School, University of Wales
-
Dr Ron Gray, Consultant Clinical Epidemiologist, Department of Public Health, University of Oxford
-
Professor Paul D Griffiths, Professor of Radiology, University of Sheffield
-
Dr Jennifer J Kurinczuk, Consultant Clinical Epidemiologist, National Perinatal Epidemiology Unit, Oxford
-
Dr Susanne M Ludgate, Medical Director, Medicines & Healthcare Products Regulatory Agency, London
-
Dr Anne Mackie, Director of Programmes, UK National Screening Committee
-
Dr Michael Millar, Consultant Senior Lecturer in Microbiology, Barts and The London NHS Trust, Royal London Hospital
-
Mr Stephen Pilling, Director, Centre for Outcomes, Research & Effectiveness, Joint Director, National Collaborating Centre for Mental Health, University College London
-
Mrs Una Rennard, Service User Representative
-
Dr Phil Shackley, Senior Lecturer in Health Economics, School of Population and Health Sciences, University of Newcastle upon Tyne
-
Dr W Stuart A Smellie, Consultant in Chemical Pathology, Bishop Auckland General Hospital
-
Dr Nicholas Summerton, Consultant Clinical and Public Health Advisor, NICE
-
Ms Dawn Talbot, Service User Representative
-
Dr Graham Taylor, Scientific Advisor, Regional DNA Laboratory, St James’s University Hospital, Leeds
-
Professor Lindsay Wilson Turnbull, Scientific Director of the Centre for Magnetic Resonance Investigations and YCR Professor of Radiology, Hull Royal Infirmary
-
Dr Tim Elliott, Team Leader, Cancer Screening, Department of Health
-
Dr Catherine Moody, Programme Manager, Neuroscience and Mental Health Board
-
Dr Ursula Wells, Principal Research Officer, Department of Health
Pharmaceuticals Panel
-
Consultant Physician and Director, West Midlands Centre for Adverse Drug Reactions, City Hospital NHS Trust, Birmingham
-
Professor in Child Health, University of Nottingham
-
Mrs Nicola Carey, Senior Research Fellow, School of Health and Social Care, The University of Reading
-
Mr John Chapman, Service User Representative
-
Dr Peter Elton, Director of Public Health, Bury Primary Care Trust
-
Dr Ben Goldacre, Research Fellow, Division of Psychological Medicine and Psychiatry, King’s College London
-
Mrs Barbara Greggains, Service User Representative
-
Dr Bill Gutteridge, Medical Adviser, London Strategic Health Authority
-
Dr Dyfrig Hughes, Reader in Pharmacoeconomics and Deputy Director, Centre for Economics and Policy in Health, IMSCaR, Bangor University
-
Professor Jonathan Ledermann, Professor of Medical Oncology and Director of the Cancer Research UK and University College London Cancer Trials Centre
-
Dr Yoon K Loke, Senior Lecturer in Clinical Pharmacology, University of East Anglia
-
Professor Femi Oyebode, Consultant Psychiatrist and Head of Department, University of Birmingham
-
Dr Andrew Prentice, Senior Lecturer and Consultant Obstetrician and Gynaecologist, The Rosie Hospital, University of Cambridge
-
Dr Martin Shelly, General Practitioner, Leeds, and Associate Director, NHS Clinical Governance Support Team, Leicester
-
Dr Gillian Shepherd, Director, Health and Clinical Excellence, Merck Serono Ltd
-
Mrs Katrina Simister, Assistant Director New Medicines, National Prescribing Centre, Liverpool
-
Mr David Symes, Service User Representative
-
Dr Lesley Wise, Unit Manager, Pharmacoepidemiology Research Unit, VRMM, Medicines & Healthcare Products Regulatory Agency
-
Ms Kay Pattison, Section Head, NHS R&D Programme, Department of Health
-
Mr Simon Reeve, Head of Clinical and Cost-Effectiveness, Medicines, Pharmacy and Industry Group, Department of Health
-
Dr Heike Weber, Programme Manager, Medical Research Council
-
Dr Ursula Wells, Principal Research Officer, Department of Health
Therapeutic Procedures Panel
-
Consultant Physician, North Bristol NHS Trust
-
Professor of Psychiatry, Division of Health in the Community, University of Warwick, Coventry
-
Professor Jane Barlow, Professor of Public Health in the Early Years, Health Sciences Research Institute, Warwick Medical School, Coventry
-
Ms Maree Barnett, Acting Branch Head of Vascular Programme, Department of Health
-
Mrs Val Carlill, Service User Representative
-
Mrs Anthea De Barton-Watson, Service User Representative
-
Mr Mark Emberton, Senior Lecturer in Oncological Urology, Institute of Urology, University College Hospital, London
-
Professor Steve Goodacre, Professor of Emergency Medicine, University of Sheffield
-
Professor Christopher Griffiths, Professor of Primary Care, Barts and The London School of Medicine and Dentistry
-
Mr Paul Hilton, Consultant Gynaecologist and Urogynaecologist, Royal Victoria Infirmary, Newcastle upon Tyne
-
Professor Nicholas James, Professor of Clinical Oncology, University of Birmingham, and Consultant in Clinical Oncology, Queen Elizabeth Hospital
-
Dr Peter Martin, Consultant Neurologist, Addenbrooke’s Hospital, Cambridge
-
Dr Kate Radford, Senior Lecturer (Research), Clinical Practice Research Unit, University of Central Lancashire, Preston
-
Mr Jim Reece Service User Representative
-
Dr Karen Roberts, Nurse Consultant, Dunston Hill Hospital Cottages
-
Dr Phillip Leech, Principal Medical Officer for Primary Care, Department of Health
-
Ms Kay Pattison, Section Head, NHS R&D Programme, Department of Health
-
Dr Morven Roberts, Clinical Trials Manager, Medical Research Council
-
Professor Tom Walley, Director, NIHR HTA programme, Professor of Clinical Pharmacology, University of Liverpool
-
Dr Ursula Wells, Principal Research Officer, Department of Health
Disease Prevention Panel
-
Medical Adviser, National Specialist, National Commissioning Group (NCG), London
-
Director, NHS Sustainable Development Unit, Cambridge
-
Dr Elizabeth Fellow-Smith, Medical Director, West London Mental Health Trust, Middlesex
-
Dr John Jackson, General Practitioner, Parkway Medical Centre, Newcastle upon Tyne
-
Professor Mike Kelly, Director, Centre for Public Health Excellence, NICE, London
-
Dr Chris McCall, General Practitioner, The Hadleigh Practice, Corfe Mullen, Dorset
-
Ms Jeanett Martin, Director of Nursing, BarnDoc Limited, Lewisham Primary Care Trust
-
Dr Julie Mytton, Locum Consultant in Public Health Medicine, Bristol Primary Care Trust
-
Miss Nicky Mullany, Service User Representative
-
Professor Ian Roberts, Professor of Epidemiology and Public Health, London School of Hygiene & Tropical Medicine
-
Professor Ken Stein, Senior Clinical Lecturer in Public Health, University of Exeter
-
Dr Kieran Sweeney, Honorary Clinical Senior Lecturer, Peninsula College of Medicine and Dentistry, Universities of Exeter and Plymouth
-
Professor Carol Tannahill, Glasgow Centre for Population Health
-
Professor Margaret Thorogood, Professor of Epidemiology, University of Warwick Medical School, Coventry
-
Ms Christine McGuire, Research & Development, Department of Health
-
Dr Caroline Stone, Programme Manager, Medical Research Council
Expert Advisory Network
-
Professor Douglas Altman, Professor of Statistics in Medicine, Centre for Statistics in Medicine, University of Oxford
-
Professor John Bond, Professor of Social Gerontology & Health Services Research, University of Newcastle upon Tyne
-
Professor Andrew Bradbury, Professor of Vascular Surgery, Solihull Hospital, Birmingham
-
Mr Shaun Brogan, Chief Executive, Ridgeway Primary Care Group, Aylesbury
-
Mrs Stella Burnside OBE, Chief Executive, Regulation and Improvement Authority, Belfast
-
Ms Tracy Bury, Project Manager, World Confederation for Physical Therapy, London
-
Professor Iain T Cameron, Professor of Obstetrics and Gynaecology and Head of the School of Medicine, University of Southampton
-
Dr Christine Clark, Medical Writer and Consultant Pharmacist, Rossendale
-
Professor Collette Clifford, Professor of Nursing and Head of Research, The Medical School, University of Birmingham
-
Professor Barry Cookson, Director, Laboratory of Hospital Infection, Public Health Laboratory Service, London
-
Dr Carl Counsell, Clinical Senior Lecturer in Neurology, University of Aberdeen
-
Professor Howard Cuckle, Professor of Reproductive Epidemiology, Department of Paediatrics, Obstetrics & Gynaecology, University of Leeds
-
Dr Katherine Darton, Information Unit, MIND – The Mental Health Charity, London
-
Professor Carol Dezateux, Professor of Paediatric Epidemiology, Institute of Child Health, London
-
Mr John Dunning, Consultant Cardiothoracic Surgeon, Papworth Hospital NHS Trust, Cambridge
-
Mr Jonothan Earnshaw, Consultant Vascular Surgeon, Gloucestershire Royal Hospital, Gloucester
-
Professor Martin Eccles, Professor of Clinical Effectiveness, Centre for Health Services Research, University of Newcastle upon Tyne
-
Professor Pam Enderby, Dean of Faculty of Medicine, Institute of General Practice and Primary Care, University of Sheffield
-
Professor Gene Feder, Professor of Primary Care Research & Development, Centre for Health Sciences, Barts and The London School of Medicine and Dentistry
-
Mr Leonard R Fenwick, Chief Executive, Freeman Hospital, Newcastle upon Tyne
-
Mrs Gillian Fletcher, Antenatal Teacher and Tutor and President, National Childbirth Trust, Henfield
-
Professor Jayne Franklyn, Professor of Medicine, University of Birmingham
-
Mr Tam Fry, Honorary Chairman, Child Growth Foundation, London
-
Professor Fiona Gilbert, Consultant Radiologist and NCRN Member, University of Aberdeen
-
Professor Paul Gregg, Professor of Orthopaedic Surgical Science, South Tees Hospital NHS Trust
-
Bec Hanley, Co-director, TwoCan Associates, West Sussex
-
Dr Maryann L Hardy, Senior Lecturer, University of Bradford
-
Mrs Sharon Hart, Healthcare Management Consultant, Reading
-
Professor Robert E Hawkins, CRC Professor and Director of Medical Oncology, Christie CRC Research Centre, Christie Hospital NHS Trust, Manchester
-
Professor Richard Hobbs, Head of Department of Primary Care & General Practice, University of Birmingham
-
Professor Alan Horwich, Dean and Section Chairman, The Institute of Cancer Research, London
-
Professor Allen Hutchinson, Director of Public Health and Deputy Dean of ScHARR, University of Sheffield
-
Professor Peter Jones, Professor of Psychiatry, University of Cambridge, Cambridge
-
Professor Stan Kaye, Cancer Research UK Professor of Medical Oncology, Royal Marsden Hospital and Institute of Cancer Research, Surrey
-
Dr Duncan Keeley, General Practitioner (Dr Burch & Ptnrs), The Health Centre, Thame
-
Dr Donna Lamping, Research Degrees Programme Director and Reader in Psychology, Health Services Research Unit, London School of Hygiene and Tropical Medicine, London
-
Mr George Levvy, Chief Executive, Motor Neurone Disease Association, Northampton
-
Professor James Lindesay, Professor of Psychiatry for the Elderly, University of Leicester
-
Professor Julian Little, Professor of Human Genome Epidemiology, University of Ottawa
-
Professor Alistaire McGuire, Professor of Health Economics, London School of Economics
-
Professor Rajan Madhok, Medical Director and Director of Public Health, Directorate of Clinical Strategy & Public Health, North & East Yorkshire & Northern Lincolnshire Health Authority, York
-
Professor Alexander Markham, Director, Molecular Medicine Unit, St James’s University Hospital, Leeds
-
Dr Peter Moore, Freelance Science Writer, Ashtead
-
Dr Andrew Mortimore, Public Health Director, Southampton City Primary Care Trust
-
Dr Sue Moss, Associate Director, Cancer Screening Evaluation Unit, Institute of Cancer Research, Sutton
-
Professor Miranda Mugford, Professor of Health Economics and Group Co-ordinator, University of East Anglia
-
Professor Jim Neilson, Head of School of Reproductive & Developmental Medicine and Professor of Obstetrics and Gynaecology, University of Liverpool
-
Mrs Julietta Patnick, National Co-ordinator, NHS Cancer Screening Programmes, Sheffield
-
Professor Robert Peveler, Professor of Liaison Psychiatry, Royal South Hants Hospital, Southampton
-
Professor Chris Price, Director of Clinical Research, Bayer Diagnostics Europe, Stoke Poges
-
Professor William Rosenberg, Professor of Hepatology and Consultant Physician, University of Southampton
-
Professor Peter Sandercock, Professor of Medical Neurology, Department of Clinical Neurosciences, University of Edinburgh
-
Dr Susan Schonfield, Consultant in Public Health, Hillingdon Primary Care Trust, Middlesex
-
Dr Eamonn Sheridan, Consultant in Clinical Genetics, St James’s University Hospital, Leeds
-
Dr Margaret Somerville, Director of Public Health Learning, Peninsula Medical School, University of Plymouth
-
Professor Sarah Stewart-Brown, Professor of Public Health, Division of Health in the Community, University of Warwick, Coventry
-
Professor Ala Szczepura, Professor of Health Service Research, Centre for Health Services Studies, University of Warwick, Coventry
-
Mrs Joan Webster, Consumer Member, Southern Derbyshire Community Health Council
-
Professor Martin Whittle, Clinical Co-director, National Co-ordinating Centre for Women’s and Children’s Health, Lymington