

Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number 14/182/14. The contractual start date was in January 2016. The final report began editorial review in April 2019 and was accepted for publication in January 2020. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2020. This work was produced by Mitchell et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2020 Queen’s Printer and Controller of HMSO
Chapter 1 Background and rationale
Against a backdrop of changing sexual repertoires, young people report higher levels of unsafe sex and higher rates of sexually transmitted infections (STIs) than any other age group. 1,2 Early intervention is required to prevent risks converting to poor lifetime sexual health, and schools are particularly well placed to facilitate these interventions. 3 Young people who cite school as their main source of information about sex are less likely to report unsafe sex and previous STI diagnosis. 4 The proportion of people citing school as their main source is increasing,5 but the content and quality of provision of sex education in UK schools is variable. 6 Over two-thirds of young people report inadequate knowledge when they first felt ready for sex,5 suggesting significant room for improved delivery of school-based sex education.
Young people are susceptible to powerful social influences that could enhance or undermine school-based sex education. These include norms and values that are transmitted both offline and online via peer networks. With respect to the latter, social media can increase social connectedness, strengthen social identity and facilitate access to health information, but it also adds risk of exposure to harmful messages, social pressures and bullying. 7
Against this background, we sought to develop and assess a novel school-based intervention that addresses limitations of existing peer-led sex education, while unlocking the potential of peer influence and social media.
Sexual health of young people
Almost one in six young people (aged 16–24 years) report unsafe sex, defined as at least two partners with whom no condom was used in the past year. This is higher than in any other age group. 8 In England in 2015, 15- to 24-year-olds accounted for 62% of heterosexual people diagnosed with chlamydia, 52% of heterosexual people diagnosed with gonorrhoea, 51% of heterosexual people diagnosed with genital warts and 41% of heterosexual people diagnosed with genital herpes. The diagnostic rate of chlamydia was 824 per 100,000 in males aged 15–19 years and 2436 per 100,000 females of the same age. 9 In Scotland, 65% of all diagnoses of chlamydia are among young people aged < 25 years; and among women, 75% of diagnoses were in those < 25 years. 9 There has been a significant shift in young people’s sexual repertoires over recent decades. The proportion of young people (aged 16–24 years) in the UK reporting all three types of intercourse (oral, vaginal and anal) rose from 10% in 1990 to 20% (females) and 25% (males) in 2012, primarily reflecting an increase in those experiencing oral and anal sex. 1
A narrow focus on risk avoidance ignores key inter-relationships between risk and other aspects of sexual health and well-being. Young people’s sexual behaviour is influenced by social factors, including gender stereotypes, peer pressure and social expectations. 10 It is therefore important to look beyond the biological markers of sexual health and focus on outcomes that are more meaningful to young people, such as the quality of sexual relationships, in particular the reduction of sexual violence (including discrimination) and improved sexual experience. 11 Positive romantic relationships are associated with both good physical health and good mental health, and supportive social networks, lending support to the notion of synergistic benefits between these aspects of young people’s lives. 12 There are calls to place greater emphasis on sexual enjoyment to reduce sexual risks (e.g. promoting the pleasurable use of condoms). 13
Reframing adolescent sexual health as a positive developmental process offers a focus on outcomes that may be more meaningful to young people. 14 Sexual health interventions should consider both risk taking and risk reduction, and how pleasure (as an underpinning mechanism) can account for both. Ideally, intervention development should be driven by sexual health policies that promote positive sexual health and well-being, in addition to reducing risks. 13
Sexual health policy in the UK
All four countries in the UK have sexual health strategies that emphasise the importance of prevention and treatment of sexual health problems among young people. A central focus is to develop and reinforce positive cultural norms, openness, respect and responsibility as key drivers of improving sexual health. 15–18
These strategies also indicate the need to implement digital platforms to improve access to sexual health resources and services, including social media for sexual health promotion. 16 School-based sex education is compulsory in England and Wales, but not in Scotland and Northern Ireland. All UK policies focus on developing sexual health knowledge and attitudes in relation to biological outcomes (e.g. STIs and pregnancy). All UK policies include the emotional, social and relational aspects of sexual health.
In addition, Scotland has The Curriculum for Excellence, which seeks to build an educational environment in which young people can become successful learners, confident individuals, responsible citizens and effective contributors to society. 19 The emphasis is on more rounded development, which values personal and social growth in addition to academic achievement, including benchmarks to evaluate sexual health promotion. This fits into the Scottish Government’s broader policy for child and family support and development known as Getting it Right for Every Child20 and a national resource titled Relationships, Sexual Health and Parenthood for use in a range of educational settings. 21
Sexual health interventions: evidence of effectiveness
School-based interventions
Most sexual health interventions for young people are school based, as this setting facilitates access to the widest range of young people in terms of socioeconomic background and vulnerability to poor sexual health. Schools provide a major context for social development22 and are ideally placed to challenge unhealthy and inequitable norms underpinning sexual risk behaviours. 23 For interventions attempting to diffuse change through social networks, schools provide a ‘captive audience’ and naturally occurring friendship groups. 24
School-based interventions tend to comprise one or both of:
-
sexual health education and training to improve knowledge, exploring emotions and sexual norms, developing sexual negotiation skills and self-efficacy, and making informed choices3,25
-
providing access to sexual health services either in or out of school, including condoms or access to other forms of contraception (e.g. hormone-based medication). 26–29
Evidence from older systematic reviews suggests that school-based sex education has an effect on sexual health knowledge and attitudes, but only some programmes delay sexual behaviour and increase condom use. 3 Shepherd et al. 25 are cautious about the impact of such programmes in bringing about behavioural change, acknowledging that significant changes in sexual health knowledge and self-efficacy (e.g. knowing how to use a condom) are more common.
More recent systematic reviews suggest that combining education with contraceptives or access to sexual health services may be more effective. For example, Oringanje et al. 27 found that providing education alongside contraceptives increases condom use and may reduce unintended pregnancies. Interventions that combine education with interactive techniques to improve condom use, teaching how to negotiate sex and providing a range of contraceptives can lead to an increase in knowledge and effective use of contraceptives, delay sexual initiation and improve condom use. 28 Owen et al. 26 found that school-linked sexual health services did not encourage sex or risk-taking, and may at best reduce chlamydia infection (males only) and pregnancy; however, the evidence is based on a small number of mainly US studies of variable quality. Studies rarely show an impact on biological markers, such as human immunodeficiency virus, herpes and syphilis, partly because these are relatively rare outcomes and require extremely large samples to detect an effect. 29
A number of contextual factors affect these outcomes. A review of process data from trials30 suggests two key influences: (1) fidelity, influenced by the extent to which the school has a supportive culture, a flexible administration, and enthusiasm and expertise among those delivering the sexual health content; and (2) acceptability and engagement, influenced by enthusiasm, credibility and expertise of intervention providers, and relevance and enjoyment to young people. Another systematic review31 noted the diversity in approaches of effective interventions, suggesting that a range of mechanisms exist.
Peer interventions
Peer education is a method of disseminating knowledge, values or achieving behaviour change through a social network, delivered by someone of a similar age and standing in that network. 32 The theoretical appeal of peer involvement lies in its potential to reinforce positive values and beliefs, thereby strengthening social norms that might influence sexual behaviour. 33,34 The key mechanisms include role-modelling,35 a shared identity between the peer workers and their peer group, and the ability of the peer workers to influence their networks. 32 There is a range of peer-led roles and approaches, including educator or assistant educator,35 peer supporter (PS) and, occasionally, peer leader. 32
Evidence from systematic reviews on the evaluations of peer sexual health interventions for young people demonstrates a weak effect on sexual attitudes, knowledge and intentions, and ‘unconvincing’ evidence for the impact on sexual behaviour. 32,35,36 Methodologically, reviews have highlighted a paucity of peer-based sexual health interventions for young people that are evaluated using randomised control trials. 32
Two notable studies in the UK33,34 engaged peer educators to replace teaching staff, at least in part; however, in the other studies peer educators assisted teachers. Across peer-led interventions, the dominant model is one of a peer educator (teacher) rather than peers as supporters of positive norms and behaviour. 32–36 Involving youth peers as ‘influencers’ within their sexual networks has been under-researched in the field of sexual health. 36 In a review of peer interventions aimed at addressing a range of health and social issues, Harden et al. 37 identified five studies that compared the effectiveness of peer leaders with teachers in delivering the same intervention. In one sexual health evaluation from the USA, peer leaders were found to be generally more effective than teachers. More specifically, peer leaders are thought to be more effective at establishing conservative (non-risky) norms, but less effective than adults at imparting factual information and getting students involved in classroom activities. 34 A formal teaching role may undermine credibility with peers38 and may be less effective than informal social support work. 39
Participation rates in peer interventions vary and further research is required to optimise the most appropriate level of peer participation, which should consider the level of social ease experienced by peer workers, establish how participation affects peer networks and include theoretically informed outcome measures. 32,35,36
How peer educators are chosen and their reputation among peers is important. 32,33 Most studies rely on self-selection or teacher selection, but both these strategies may result in educators who are not particularly credible and find it difficult to reach high-risk students. 40 The Students Together Against Negative Decisions (STAND) study used peer nomination and diffusion of innovation theory in a youth-focused sexual health intervention in schools. 41 Peer leads delivered an education-based programme to ‘opinion leaders’, who were then asked to engage with their networks (although not via social media). Awareness of the STAND study intervention was high. The intervention was effective at improving knowledge and behaviour among those trained, but had mixed success in diffusing risk reduction practices to other non-trained students. 41
Digital media interventions
Digital media offer inspiration for rethinking sexual health promotion. 42 There has been an exponential increase in the use of digital media by young people in the last decade, including social networking, mobile applications (apps), video sharing, podcasts, online games and video or photo communications. 43 Most (95%) young people in the UK use social networking sites at least once per week, most commonly Instagram (URL: www.instagram.com; Facebook, Inc., Menlo Park, CA, USA), Snapchat (URL: www.snapchat.com; Snap Inc., Santa Monica, CA, USA) and Facebook (URL: www.facebook.com; Facebook, Inc., Menlo Park, CA, USA). 7 Technologies such as smartphones give unprecedented mobile access to the internet. 44 New internet-based platforms, including social media, offer greater opportunity for more interactive communication, possibly at the point of health-related decision-making. Digital media can deliver interventions conveniently and anonymously to young people using personalised information. 45
In theory, digital media offers the potential to deliver sexual health messages to those who are already making use of these technologies and are confident in using them. 46 Recent systematic reviews on the impact of digital media on young people found that it can improve sexual health knowledge (of STIs and emergency contraceptives) and self-efficacy (condom use and STI testing), and reduce sexual risk behaviour, but there has been no demonstrated impact on biological outcomes. 42,47–50
The popularity of social networking sites among young people render these as obvious candidates for sexual health promotion, although those in the health and research communities have been slow in using this approach. 51 A review of early interventions indicated that these sites were mainly used to heighten awareness of online sexual health programmes. 52 Few studies have examined the impact of social networking sites on the sexual health of young people. One cluster randomised controlled trial53 found that a peer-led community-based Facebook intervention called ‘Just/Us’ increased condom use over a 2-month period, although the effect diminished by 6 months. Another pilot study54 reported a potential increase in condom use and reduction in chlamydia infection.
Recommendations from systematic reviews highlight the need to involve young people in the design of digital interventions, the importance of using theory to inform intervention development and the importance of using stronger research designs,42,50 including research in the use of social media for sexual health promotion. 45 Few digital media programs provide tailored advice and none assesses social network interventions in school settings. 42,47,48 On a pragmatic level, findings from the evaluation of the FaceSpace project highlight the importance of securing sufficient resources for developing social network platforms and maintaining a high profile, reach and engagement with young people. 55,56
Summary and scientific rationale
It is over 10 years since Kirby et al. 3 published their seminal review of sex education in schools, and the substantial growth in evidence since then suggests that school interventions have a consistent effect on sexual health knowledge and attitudes, but less so on sexual risk behaviours. A key question, therefore, is how to enhance these effects.
Digital media offer an exciting opportunity to work with young people through their networks using social media platforms. Few digital media programs provide tailored advice and, to our knowledge, none has assessed social network interventions in school settings to tackle sexual health. 42,47,48
Peer interventions could be combined with online social networking sites to enhance effects. The weight of evidence on the effectiveness of peer interventions suggests a similar or weaker pattern to that of traditional school-based interventions. 32,35,36 Four important issues are often overlooked: (1) how peer educators are recruited,30,32 (2) the nature of their influence,36 (3) their position within their network20,40 and (4) the need to establish outcomes that are theoretically informed. 32,35,36 These are issues we sought to address in this study.
The intervention in the current study [Sexually Transmitted infections And Sexual Health (STASH)] builds on a peer-led smoking prevention intervention [A Stop Smoking In Schools Trial (ASSIST)], which recruited and trained ‘influential’ students (aged 12 or 13 years) as PSs in schools to spread and sustain non-smoking norms through informal interactions with peers. 40 A cluster randomised control trial57 found that smoking was reduced over a 2-year period. The intervention is recommended by National Institute for Health and Care Excellence (NICE)58 and is now disseminated under licence in hundreds of schools, in over 30 areas in England, Wales, Scotland and France (see Chapter 2, Developing a theory-informed young people’s sexual health intervention).
ASSIST is based on diffusion of innovation theory, which explains how new ideas are adopted across social networks. 59 Instrumental to this is the influence of early adopters (peer leaders), who seek to bring about change in others. Critically, the peers are tasked with changing (or reinforcing positive) norms and competence. ASSIST also draws on implementation theory (IT), which includes normalisation process theory60 and accounts for how, and to what extent, interventions are embedded in the existing school environment.
Following the Medical Research Council (MRC)’s guidance on the development and evaluation of complex interventions,61 there are five key reasons why a feasibility study is required here. First, our proposed intervention is novel in that it comprises elements that have not been combined in previous sexual health interventions for young people, namely setting (secondary schools) and method of delivery (influential peer leaders, social networking and social media). Second, there are a number of design challenges and uncertainties specific to our proposed approach (detailed in Chapter 2). Third, we need to better understand the extent to which the intervention works as intended, including the facilitators of and barriers to implementation. Fourth, there is the need to establish a theoretical understanding of the mechanisms that may lead to improved sexual health for young people and thereby identify the most appropriate intermediate and outcome variables for a trial. Finally, given the lack of controlled trials and drawing from guidance regarding the best use of resources,61 we need to consider the resource and methodological implications of conducting a large trial, including the feasibility of an economic analysis.
In conclusion, given the popularity of social media platforms among young people and their potential to access and influence social networks, this is an opportune time to integrate these with peer-based approaches in a closed social system, such as a school. Theoretically, these may act synergistically to develop and strengthen cultural values, thereby supporting social norms that influence sexual behaviour.
Aims and objectives
The aim of this study is to develop and test the feasibility and acceptability of a school-based intervention delivered by PSs (the STASH study) to reduce transmission of STIs and improve the sexual health of secondary school students aged 14–16 years in the UK.
The objectives of the study are to:
-
finalise the design of a school-based STI prevention intervention, in which influential PSs use online social networks and face-to-face interactions to influence norms, knowledge, competence and behaviour, and promote the use of sexual health services
-
assess the recruitment and retention of PSs, as well as feasibility and acceptability of the intervention among PSs, participants and key stakeholders
-
assess the fidelity and reach of intervention delivery by trainers and PSs, including barriers to and facilitators of successful implementation
-
refine and test the programme theory and theoretical basis of the intervention
-
enhance understanding of the potential of social media, when used by influential peers, to diffuse norm change and facilitate social support for healthy sexual behaviour
-
determine key trial design parameters for a possible future large-scale trial, including recruitment, retention rates and strategies, outcome measures, intracluster correlation (ICC) and sample size
-
determine the key components of a future cost-effectiveness analysis and test data collection methods
-
establish whether or not pre-set progression criteria are met and if a larger-scale trial is warranted.
Chapter 2 Developing the STASH intervention
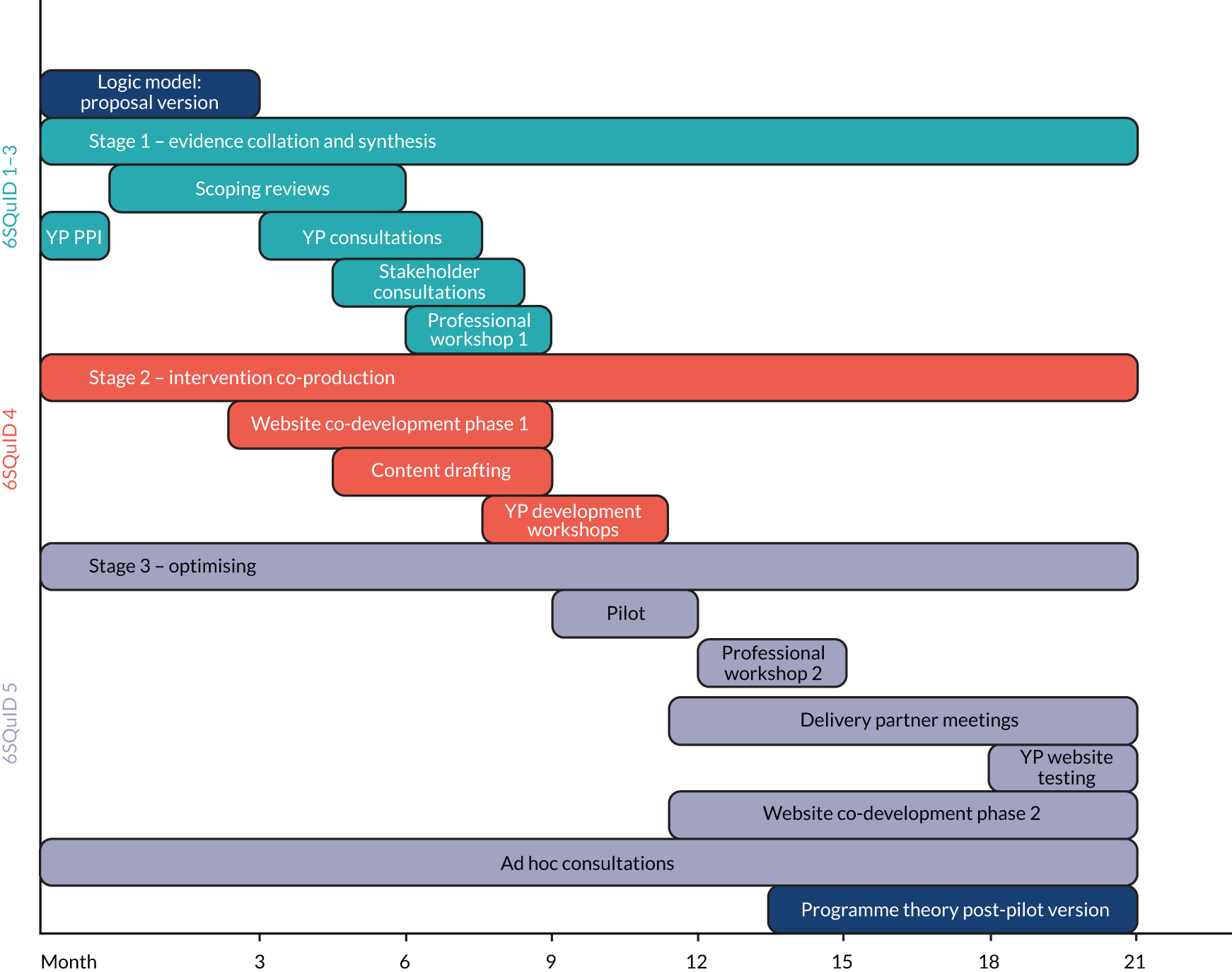
This chapter describes how the intervention developed from the initial plan set out in the funding proposal, to the intervention as delivered in the feasibility study. It details methods (including a pilot) and explains how we integrated our learning from three development stages – (1) evidence collation and synthesis, (2) co-production and (3) optimisation – into design decisions. The intervention development process is summarised in Figure 1.
FIGURE 1.
The STASH study intervention development process (by 6SQuID component). 6SQuID, Six Steps in Quality Intervention Development; PPI, patient and public involvement; YP, young person.
Background
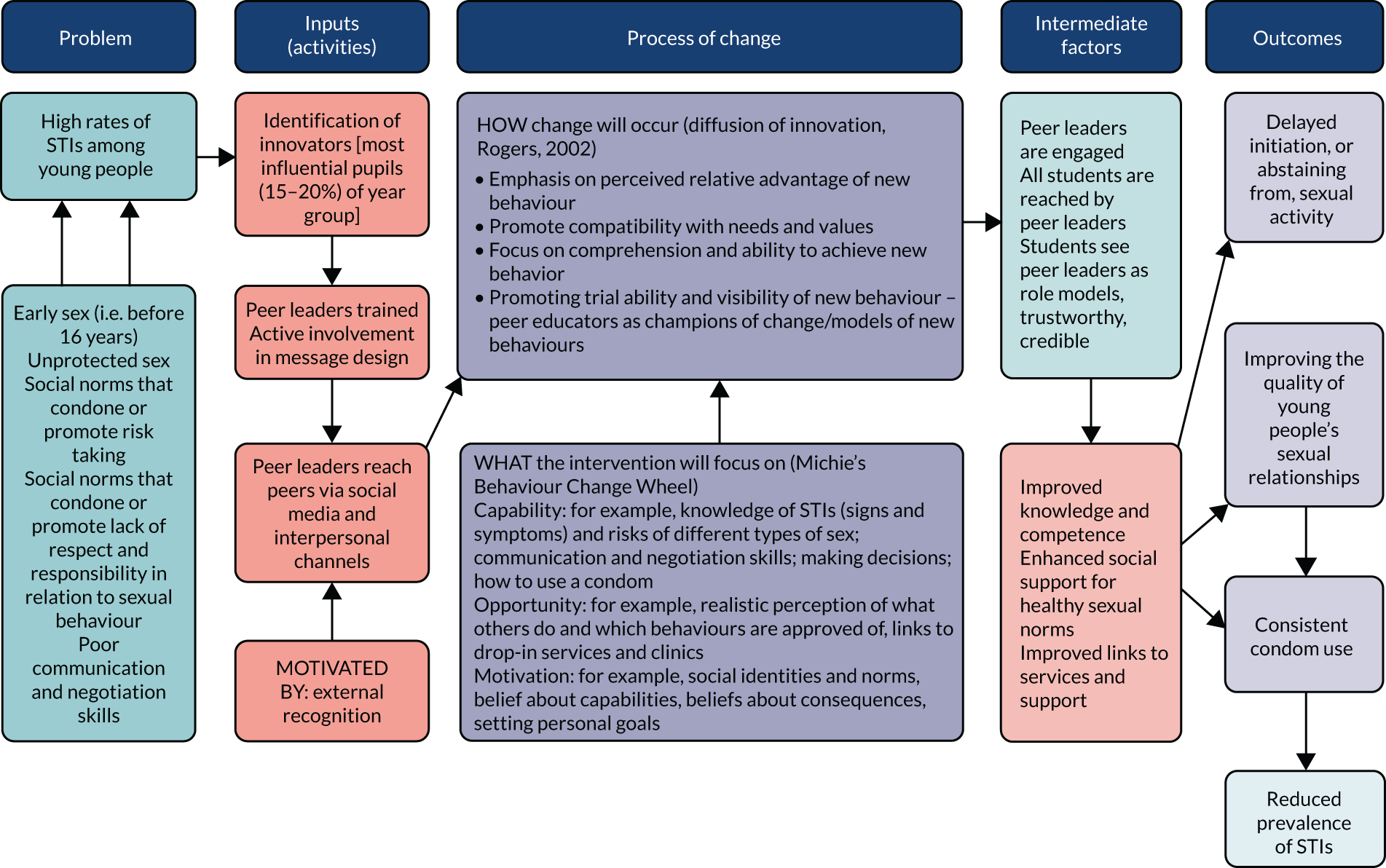
Our starting point was the proposal version of the STASH study logic model (Figure 2). This offers a visual representation of the problem (as conceived), inputs (intervention components that were expected to bring about change), process by which change would occur, intermediate factors and expected end outcomes. This was subsequently developed into a full programme theory that, in addition to theorising the mechanisms of change, hypothesised the conditions under which they would operate effectively. The post-pilot version of the programme theory (see Figure 4) guided the evaluation and identified important contextual factors that might shape outcomes and effects.
FIGURE 2.
The STASH study logic model: proposal stage. Reproduced from Forsyth et al. 62 This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/. The figure includes minor additions and formatting changes to the original figure.
Developing a theory-informed young people’s sexual health intervention
Development work is essential to tailor theoretically grounded programmes to the needs of the target population. 63–65 The STASH study aimed to adapt what was known to work in a successful existing public health intervention to a new problem and context. The planned intervention drew on theories and mechanisms that were effective in ASSIST40 (see Chapter 1), while targeting an older age group (14–16 instead of 12–13 years) and focusing on STI prevention instead of smoking. Therefore, although ASSIST offered a theoretical starting point, the appropriateness of intervention components needed to be reviewed and revised accordingly. We anticipated that these differences would require significant adaptations to the ASSIST content and mode of delivery. Crucially, we also set out to explore how we might harness the potential of social media as a mechanism to communicate messages and, in doing so, modernise ASSIST.
Key intervention components brought forward from ASSIST
We began with the overarching mechanisms of ASSIST:
-
Recruitment and training of ‘influential’ students (PSs) to spread and sustain positive norms through informal interactions with peers. Grounded in diffusion of innovation theory59 and recruitment of ‘early adopters’,66 ASSIST found that recruiting 15% of the year group was effective in the context of smoking prevention. 67
-
Use of professional trainers to train PSs to increase intervention efficacy and credibility, reduce burden on schools and ultimately increase potential for scalability and widespread adoption.
We intended to use the following components from ASSIST.
Nomination
Identify the most influential students in secondary 4 (S4) by blinded peer nomination.
Recruitment
From this influential group, recruit a percentage of the entire year group to act as PSs.
Training
A 2-day PS training programme, delivered by a third-sector organisation in school time, at an external venue, covering PS role, skills and responsibilities, and knowledge building.
Peer supporter-delivered activities
A period in which trained PSs carry out intervention activities.
Trainer-led activities
Follow-up sessions delivered during the PS activity period.
Participant acknowledgement
Peer supporters receive formal recognition for their role.
Our development work followed MRC guidance61 on the development and evaluation of complex interventions, which acknowledges that intervention development is often not linear and may have several phases. We focused on exploring the evidence base and identified relevant theory and pilot work to address ‘key uncertainties’. 61 In the STASH study, ‘key uncertainties’ were the feasibility of a PS approach in a sexual health context, the older age group (compared with ASSIST) and use of social media as a forum for interaction.
We also followed the Six Steps in Quality Intervention Development (6SQuID) framework, which sets out ‘practical, logical, evidence-based ways to maximise effectiveness’. 68 These six steps are:
-
define and understand the problem and its causes
-
identify which causal or contextual factors are malleable and have the greatest scope for change (and who would benefit most)
-
decide on mechanism(s) of change to be utilised
-
clarify how these will be delivered
-
test and refine on a small scale
-
collect sufficient evidence of effectiveness to justify rigorous evaluation/implementation.
We detail the STASH study development stages in line with 6SQuID stages 1 and 2 (grouped here as ‘evidence collation and synthesis’), stages 3 and 4 (grouped here as ‘co-production’) and stage 5 (grouped here as ‘optimising the intervention’). Stage 6 is addressed in Chapters 5–7. We included Michie’s Behaviour Change Wheel/Theoretical Domains Framework in the preliminary logic model69,70 and referred to it in designing the STASH study website and training materials, but found it less applicable to determining macro-level mechanisms of change, as these were, to a large extent, determined by the ASSIST intervention.
Intervention development aims and objectives
The overall aims of the development stage were to finalise the intervention design and refine and test the initial logic model. The broad objectives were to:
-
fully articulate the problem [i.e. young people’s sexual behaviour and risk of STI transmission (6SQuID stage 1)]
-
explore and clarify causal and contextual factors relating to young people’s sexual behaviour and identify those most amenable to change (6SQuID stages 2–4)
-
identify contextual factors that might shape implementation (6SQuID stages 2–4)
-
establish how the STASH study might bring about change in young people’s sexual behaviour (6SQuID stage 3)
-
identify intervention content, including existing high-quality resources (6SQuID stage 3)
-
refine programme theory (overall 6SQuID aims).
Intervention development process
Each stage in this iterative process – and its constituent activities, objectives and methods – is outlined, followed by a synthesis of findings (see Synthesising and operationalising development process findings).
Stage 1: evidence collation and synthesis – 6SQuID steps 1–3 (months 0–9)
The objective of stage 1 was to collate and synthesise evidence to inform key intervention content, establish the most effective delivery format and develop the most appropriate theoretical framework to guide this. We explored necessary adaptations to ASSIST, including a shift to social media as an alternative mechanism for delivering content. Key findings and recommendations derived from each activity are outlined in Appendix 1.
Review of the evidence base: ‘scoping’ literature review
This review examined academic literature for evidence to identify drivers of target behaviours, effective components of school- and digital media-based interventions, and behaviour change theories relevant to young people and sexual health.
Following relevant guidance,71 targeted scoping searches of high-level literature were conducted, including systematic reviews of interventions [peer education, social media, school-based sex and relationships education (SRE)]; review, discussion or state-of-evidence articles (key drivers of risk, facilitators of safer practices and well-being, and issues in young people’s sexual behaviour); and behaviour change theories relevant to young people’s sexual health and well-being.
Search inclusion criteria were:
-
age range 12–19 years (to include age groups encompassing target group)
-
English as the publication language
-
a publication date post 1990
-
Organisation for Economic Co-operation and Development (OECD)/high-income countries.
We excluded studies that were published before 1990, were not in English, focused primarily on primary school or post-statutory education-aged children or were based in non-OECD countries.
Searches used combinations of controlled vocabulary and free text (e.g. title/abstract = ‘adolescent’ and ‘condom use’). We undertook targeted searches of the following databases: Child Development & Adolescent Studies, EMBASE, POPLINE, PsycINFO, PubMed and Web of Science. We also reviewed pertinent theoretical literature on complex interventions and behaviour change, beginning with diffusion of innovation theory (the basis of ASSIST). 59 Targeted manual searches also included reviewing article reference lists, reviews of subsequent publications citing key papers and papers identified through the expertise of the Trial Management Group (TMG).
Reviews of resources and materials: relevant grey literature, sex and relationships education/practitioner resources, digital media sources, potential social/digital media platforms
We collated high-quality SRE resource exemplars (websites, resource packs). We sought to identify key features, examine theoretical grounding, if available, and identify potential content relevant to the STASH study. Grey literature and relevant web resources were identified opportunistically via professional networks of the TMG and by non-systematic and targeted online searches. We identified policy and guidance documents focused on SRE delivery in the UK. Resources were categorised by source, type and quality, and key points summarised. We assessed quality of youth-oriented sexual health web resources [including information sites, YouTube videos (URL: www.youtube.com; YouTube, LLC, San Bruno, CA, USA) and vloggers/influencers], rating them according to relevance to the STASH study, content quality, design quality (appeal to young people) and apparent authority or legitimacy.
Finally, we reviewed candidate social media platforms for user demographics, functionality, appeal and regulatory information. Platforms [e.g. Instagram, WhatsApp (URL: www.whatsapp.com; Facebook, Inc., Menlo Park, CA, USA), Snapchat and Facebook] were appraised for age restrictions, message-sharing functions (including traceability over time, images, audio, video and ability to interface with a website), private group messaging options and whether or not posted content could be visible to the research team to enable evaluation (feasibility).
Consultations (patient and public involvement): young people’s consultation groups
Consultations explored the target group’s attitudes to and use of social media, and views on the proposed intervention format.
Pre-pilot consultations with young people built on earlier consultations at the pre-proposal stage (16 participants aged 14–19 years in central Scotland). In the first development stage, we conducted three group interviews (20 participants in total) with young people outside the intervention area. Two group interviews were school based and the third was with a community centre-based youth group (conducted at a community centre). We identified each via the Project Executive Group (PEG) and sought to ensure a range of socioeconomic backgrounds [two schools serving populations from mixed Scottish Index of Multiple Deprivation (SIMD) quintiles and a youth group located in an area of high relative deprivation]. Discussions were facilitated by the research team (KRM, CP and RF) and audio-recorded. A semistructured topic guide (see Report Supplementary Material 1) asked for views on classroom SRE (including gaps) and key perceived influences on young people’s sexual behaviour and attitudes. We also asked about preferences in relation to proposed intervention format, including what would engage and motivate PSs. We also explored views on the use of social media to spread messages. Discussions were summarised and reviewed for key themes, commonalities and differences, including comparison with the pre-proposal young people data.
Other stakeholder consultations
Consultation activities were designed to explore local constraints on and facilitators of implementation (including concerns) and stakeholder perspectives on young people’s sexual health, SRE and social media use.
We conducted semistructured interviews with four teachers at two secondary schools considering participation in the feasibility trial. Participants were members of school senior management teams, with some involvement in guidance and SRE. A topic guide (see Report Supplementary Material 1) explored factors emerging from the reviews, primarily relating to views on young people’s sexual health and behaviour, young people’s social media use, SRE delivery in their school (topics addressed, effectiveness) and the planned intervention (including suggested improvements and practical advice). Interviews were transcribed, summarised and reviewed for key themes and learning.
We also met with two relevant quality improvement officers/child protection leads in participating local authorities and with each participating school’s senior management team to further explore the above issues. An additional meeting was held with one school to address concerns around the intervention model. Notes from meetings were reviewed for key learning and integrated with the teacher interview findings.
Development workshop with relevant professionals (sexual health and health promotion specialists, peer educators, youth workers, academics)
The first of two ‘professional’ workshops explored and established key messages to underpin intervention format and content, and likely mechanisms of change. Participants (n = 16) were identified via the TMG’s and PEG’s professional networks and knowledge of the local health and education services landscape. In the workshop, small group discussions focused on key issues emerging from literature reviews (e.g. barriers to and facilitators of positive sexual health and relationships for young people) and how to address these in the STASH study, potential behaviour change mechanisms, function and format of the intervention, and potential challenges for PSs.
In Appendix 1, we outline key findings from each review and consultation, and recommendations for intervention design. How these were actioned is detailed in Synthesising and operationalising development process findings.
Stage 2: intervention co-production – 6SQuID step 4 (months 1–9)
Stage 2 addressed 6SQuID step 4 and aimed to develop and refine proposed intervention format and content, guided by learning from stage 1.
First phase website co-development with Antbits development consultancy
Co-production with web development consultancy Antbits (Cambridge, UK) aimed to develop an interactive website and content management system to provide mobile-optimised access and desktop functionality, and multilevel access for use by PSs (level 1) and by trainers and the research team (level 2). In multiple teleconferences with Antbits, the team explored design options and potential for presentation of curated sexual health content (sexual health information, web links, videos, etc.).
Drafting intervention content
An iterative drafting process aimed to generate a set of content for both the STASH study website and PS training and follow-up sessions, organised by topic (e.g. around relationships, consent, STIs), which would constitute a comprehensive resource. Drafts were led by KRM and built on a synthesis of evidence gathered in stage 1, guided by relevant behaviour change theories identified in the reviews. Topics and content were discussed and agreed at development ‘away days’. Draft content was reviewed by an expert SRE educator to refine focus, tone and language.
Young people’s development workshops
KRM and CP revisited the two school-based groups to gauge opinions on draft website content. Following a loose topic guide (see Report Supplementary Material 1), participants reviewed drafts (via tablet and smartboard) and gave views on visual appeal and ease of use, topics and messages, language, acceptability of external links, information gaps and general acceptability. During the sessions, five students took part in brief cognitive interviews to test selected questionnaire items. Workshops were conducted in school time, lasted approximately 1.5 hours and were audio-recorded, with notes written up and reviewed for key learning.
Stage 3: intervention optimisation – 6SQuID step 5 (months 10–21)
The overarching aim of stage 3 was to pilot the intervention in one school and to use learning from the pilot to refine the intervention. Guided by 6SQuID step 5, this stage consisted of six phases, described as follows.
Intervention pilot
The pilot school was selected from among those expressing interest in participation. It was chosen as typical of schools in the locality (regarding size and relative deprivation), and because the senior management team were supportive of the STASH study. The intervention was implemented over 9 weeks, comprising peer nomination, recruitment meeting, PS training and five follow-up sessions. Of 163 students in the year group, 31 (19%) were invited to recruitment, having received the highest number of nominations. Of these students, 19 (61% of those invited, 12% of year group) were trained and 14–17 attended follow-up sessions (attendance varying weekly). No students explicitly withdrew from the PS role, so all 19 students were considered ‘completers’ and awarded a certificate.
The purpose of the pilot was to test and refine the intervention on a small scale. We undertook a process evaluation primarily to identify what did or did not work (and why), and to identify potential improvements in anticipation of the feasibility study. The eight data collection strands were:
-
semistructured interviews with a convenience sample of intervention participants (14 PSs and three S4 friends of PSs who had some engagement with the STASH study)
-
semistructured observation of the PS training
-
PS evaluation of training via a one-page evaluation form (n = 17)
-
trainer feedback sessions (at the close of training days) and in-depth interviews with all three trainers (at the end of pilot)
-
PS online questionnaire (n = 14)
-
semistructured interviews with three teachers (including the STASH study contact teacher and two other teachers with guidance responsibilities and some awareness of the STASH study)
-
Facebook monitoring data (group membership, number of messages sent)
-
project monitoring log (participation numbers, key contextual information, e.g. school interactions, contemporaneous events).
The pilot enabled us to test the data collection tools and analytical approach. The latter was guided by an analytic framework designed to explore fidelity, acceptability, reach, recruitment and retention, context and perceived impact, and to capture any emergent and unanticipated issues. All pilot data were assessed for common themes using an approach informed by the framework method. 72,73 Data from across the data collection strands were collated by the above categories and reviewed in a matrix for commonalities, differences and key learning for the next stage of the study. We also piloted the baseline and follow-up questionnaires.
Second professional workshop
Those attending the first professional workshop were invited back to a second workshop to discuss key findings from stages 1 and 2, particularly the pilot results. Small group discussions focused on how to improve the STASH study website and message-sharing process, on intervention reach and impact, and on PS training and follow-ups. Meeting notes were reviewed for key learning points.
Intervention development meetings
Intervention development meetings consisted of four ‘away days’ with the researchers and delivery partners (West Lothian Drug and Alcohol Service and Fast Forward). Sessions focused primarily on optimising website messages and training content, including the trainer manual, slides and materials (such as games and activities). Detailed notes were taken by the research team and content drafts revised in the course of discussion.
Second phase website co-development
Following handover of the content management system from Antbits, the second phase of website development was led by the research team. Supported by Antbits and the MRC/Chief Scientist Office (CSO) Social and Public Health Sciences Unit in-house graphic designer, the research team worked to streamline and simplify content and structure, and improve visual appeal, primarily via the creation of bespoke infographics.
Website testing with young people
We conducted group interviews with two youth groups: one face to face with an established young people’s action research group (Young Edinburgh Action) and one online using Facebook Messenger (Facebook, Inc., Menlo Park, CA, USA) with a pre-existing friendship group identified through the professional networks of the research team. Groups comprised six (all female) and seven (four female, three male) participants, respectively. Participants were slightly older than the target group (aged 16–17 years), to enable reflection on what information and format they would have preferred at age 14–15 years. Groups discussed relevance, credibility and relatability of newly created content. The face-to-face group was audio-recorded and notes were taken from the audio, whereas the online group generated a transcript of the online discussion. Each was reviewed for key revisions.
Ad hoc consultation meetings (across months 0–21)
A series of meetings were held with school contact teachers, head teachers (HTs) and deputy head teachers (DHTs) at schools considering participation in the trial (two or three per school), academic colleagues, intervention development partners, professional panel participants and local NHS young people’s sexual health specialists. In addition, discussions held in regular PEG, TMG and Trial Steering Committee (TSC) meetings contributed significantly to intervention optimisation.
Synthesising and operationalising development process findings
The following section synthesises findings from across all development activities, showing how these shaped the final intervention. Findings are organised by intervention component (see Key intervention components brought forward from ASSIST). Appendix 1 details specific recommendations from each activity. The synthesis begins with a brief summary of higher-level decisions made regarding the theory underpinning the intervention.
Developing the STASH study programme theory
We conceptualised and used relevant theories at three levels (Figure 3): (1) the social system level (macro theory), (2) the individual level (mid-level theory) and (3) the behaviour level (micro theory). We identified, via literature review, mid-level theories relevant to young people’s sexual health and behaviour. This review, together with stakeholder consultations, informed the choice of behaviour change techniques and training, and website content. We developed our programme theory in line with what we already knew about mechanisms of change in ASSIST and adapted these for the sexual health context.
FIGURE 3.
Use of theory in the STASH study.
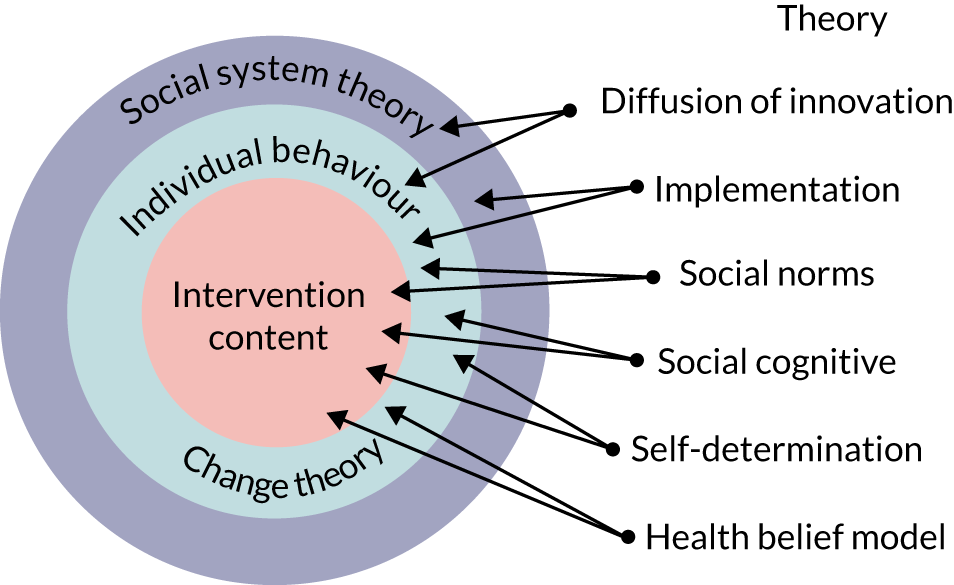
A detailed description of the theories and how we used them is given in Appendix 1 (see Table 19). Following the literature review, we excluded the least relevant of any overlapping theories and applied those most relevant at three levels (see Figure 3): (1) the social system of the intervention, (2) individual behaviour change and (3) specifics of intervention content. Together, these theories describe potential mechanisms for change that might be expected to occur as a result of the intervention. 74 Having explored their relevance and utility in the pilot, we integrated these into the revised programme theory (Figure 4) and feasibility trial.
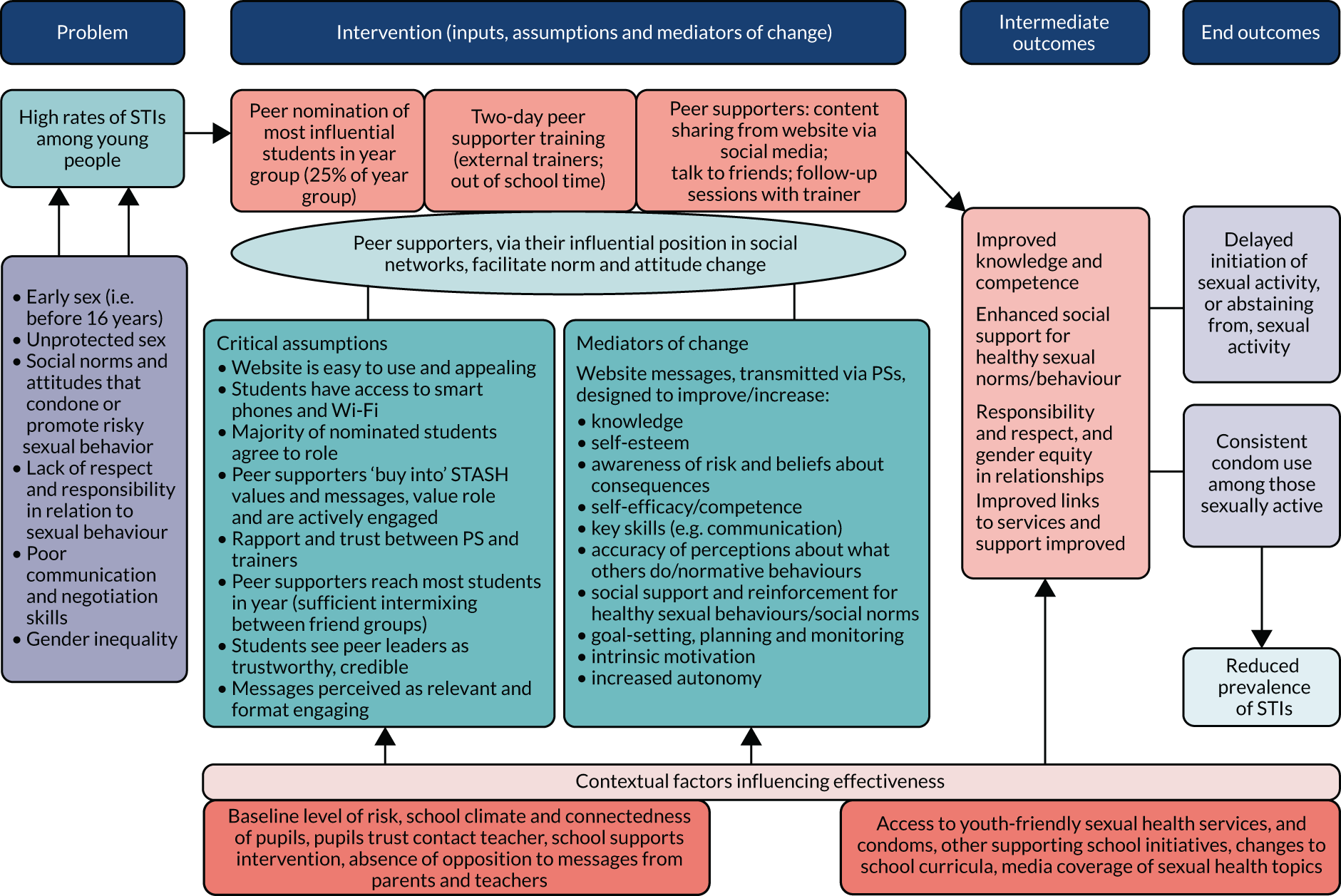
FIGURE 4.
The STASH study programme theory: pre pilot.
Guided by these theories and our consultations (see Synthesising and operationalising development process findings), we established that it would be crucial to prioritise skills development (particularly communication), encourage and support active participation and responsibility-taking (within the intervention and with regard to sexual behaviour), boost intrinsic motivation and self-efficacy, provide SRE information relevant to young people and tailor the intervention to the needs of the target group.
Synthesis and actions relating to key intervention components
Nomination and recruitment
Motivating schools
Our development activities and literature30,65,75 reviews established that school buy-in would be key to successful implementation. ASSIST highlighted that use of external trainers is a key means of limiting school burden and enhancing intervention workability. Our grey literature review and expert consultations identified that helping schools meet national policy requirements would be a strong motivator. This related particularly to the Scottish Government’s Curriculum for Excellence,19 Getting it Right for Every Child20 policy and the National Health and Wellbeing Outcomes. 76 Our schools brochure, therefore, explicitly outlined how the STASH study could help schools meet relevant indicators, particularly around enhancing students’ confidence and sense of responsibility, and addressing stigmatising attitudes.
Peer nomination process
Our consultations with young people and professionals affirmed learning from ASSIST, suggesting that peer nomination (as opposed to teacher or self-selection) would identify the most ‘credible’ or ‘trustworthy’ students40 and that schools should not be allowed to shape the list of peer-nominated students. This was stipulated in the guidance provided to schools.
The ASSIST study also found that to obtain the 15% ‘critical mass’ required for effective diffusion of innovation throughout the year group, 17.5% of nominated students should be invited to recruitment. However, our consultations suggested, and the pilot confirmed, that the sensitive topic and older cohort would require a tougher sell. In the pilot, inviting 31 nominees (19% of year group) resulted in only 19 (12% of year) being trained. To enhance the likelihood of reaching the 15% ‘critical mass’, we increased the proportion of nominees invited to recruitment to 25%. The pilot and young people consultations identified that emphasising potential curriculum vitae (CV) benefits, time with friends, and the sense of responsibility and satisfaction at being nominated, might also enhance uptake.
Discussions on peer recruitment at professional workshops and TMG meetings mooted whether or not the older cohort and sensitive topic might necessitate alternative recruitment questions to those used in ASSIST. The TMG therefore designed four new nomination questions (see The STASH study intervention design for the feasibility trial) and piloted those alongside existing ASSIST questions. Learning from the pilot also highlighted the importance of practical considerations – such as allowing plenty of time for circulation and return of parent and carer consent forms – to avoid losing some potential recruits.
Peer supporter training
Intervention content
Most development activities fed into decisions about training and website content. The literature reviewed suggested that young people’s sexual health knowledge tends to converge around risk, STIs and contraception, and that current gaps in SRE include communication, consent, pornography, sexual pleasure and online literacy. 6,77 Stakeholder consultation highlighted that current SRE packages are outdated and lack information on contemporary issues, such as consent and coercion, a view echoed in the young people consultations. Young people also expressed a desire for relatable experiential information and, echoing the literature, suggested that the use of humour78 and interactive components would enhance training and online content. In collaboration with the trainers, we integrated each of these considerations into content design.
The online resource review identified a vast array of training activities and websites aimed at young people, of varying relevance to the STASH study. Selection from among these was based on the extent to which resources linked to our key content-guiding theories (e.g. sought to change perception of social norms, boost self-efficacy and support new behaviours) (see Appendix 1), as well as their likely appeal to young people and their potential for interactive learning. Several shortlisted resources were tested with young people in the development phase. Among these were two key videos that conveyed experiential information and behaviour modelling. [‘Ryan and Natalie’ uses a gently comedic approach to illustrate a young couple navigating their first sexual encounter [URL: www.truetube.co.uk/film/screwball (accessed 4 August 2020)], whereas ‘Tea and Consent’ [URL: https://www.youtube.com/watch?v=pZwvrxVavnQ (accessed 4 August 2020)], developed for Thames Valley Police, also uses humour and a tea metaphor to explain sexual consent.] We identified Hannah Witton as an important ‘influencer’ [URL: https://hannahwitton.com (accessed 4 May 2020)] and that the BISH (best in sexual health) website had strong appeal to young people [URL: www.bishuk.com (accessed 4 May 2020)].
Some activity types were excluded or reduced post pilot. Role-plays, in particular, were used more selectively in the feasibility study, following observation of PS discomfort in performing these during the pilot training.
Values
Our theoretical grounding suggested that a clear set of values should be conveyed to participants, so that they could judge congruence with their own priorities and understandings. 60 We therefore included an overview of ‘STASH study values’ within the PS training. These values drew on the literature, policy and stakeholder consultations. Foremost among these were aims to address negative gender norms,23,79 to take a broadly ‘sex-positive’ rather than risk-focused approach and to draw on a rights-based discourse of sexual health. 80 A rights-based approach was familiar to students and teachers from the current Scottish curriculum.
Peer supporter role
Theory-guiding development, expert consultations and findings from the pilot similarly highlighted the necessity of clearly articulated role expectations for PSs. From pilot to feasibility trial, the role was refined and distilled to four key components: (1) give information, (2) influence attitudes, (3) promote the STASH study website and (4) signpost friends to trusted adults or sexual health services. These components were revisited repeatedly throughout training. Beyond these, the other key feature of the PS role was to establish and post in a secret Facebook group.
During the development stage, concerns were raised by professional workshop participants and education stakeholders about whether or not the role required too much of students. Fears coalesced around whether PSs would have the requisite maturity to handle potentially inappropriate responses from peers (including online ridicule) and whether or not they could appropriately manage potentially sensitive disclosures, including those raising safeguarding or child protection issues. To signal the responsibility inherent in the role, PSs were asked to sign a ‘STASH study charter’ on completion of the training. This reiterated role expectations and the STASH study values. The training included a session on recognising and handling sensitive disclosures, with emphasis on swift referral to an appropriate adult if anything gave cause for concern. We emphasised that PSs should not offer any sort of counselling beyond what would typically happen in their everyday friendships (see Chapter 3, Assessment of harms).
Discussion of the PS role, supported by the literature, foregrounded the importance of building generic skills of communication and listening, essential to the PS role. 81 We therefore kept the ASSIST format of building generic PS skills on training day 2, including several activities adapted from ASSIST.
Training activity format
Close consideration was given to the most effective format for all training activities, whether newly designed or drawn from ASSIST. Adaptations and revisions drew primarily on observational data from the pilot training and intervention delivery partner meetings, in which the training format was finalised. It was agreed that activities should prioritise smaller group work – which process evaluation data suggested was more effective – and that fewer topics should be covered, but in more depth (with remaining topics moved to the follow-up sessions). Based on these same sources, it was decided that use of the website and Facebook groups should be more fully integrated into the training (to improve PSs’ familiarity and confidence with content and process). It was also decided that information and skills training should be integrated across both days, rather than allocated 1 day each.
Peer supporter-led activities
Using social media
The use of social media in the STASH study was novel and, therefore, a key focus of the development stage. Our review of platforms, stakeholder consultations (patient and public involvement) and design decisions, suggested the following priorities for functionality: appeal to young people; provide options to post web links, images and/or text; provide an option to create private, invite-only groups; ease of viewing messages and message stability; potential for monitoring; and potential for interface with a website. This ruled out popular platforms such as Snapchat (messages disappear, primarily images) and Twitter (messages likely to be lost in traffic, primarily appeals to older users) (URL: www.twitter.com; Twitter, Inc., San Francisco, CA, USA). Instagram (primarily visual) at the time had no option for private groups or for a bespoke application programming interface (API) to link to the STASH study website. We ruled out WhatsApp, on the basis that this would necessitate participants sharing mobile telephone numbers with fellow group members. We also ruled out school-linked platforms [such as Glow (URL: https://glowconnect.org.uk/)], which might limit credibility and perceived student ownership of the project. Ultimately, Facebook was identified as the only platform to meet all priorities. Although not the most popular choice for the target group, consultations did suggest that the platform was widely used and that young people would be willing to utilise it for the STASH study. A priority emphasised by young people throughout the consultations was privacy and control over who would see their posts, and the ‘secret’ group functionality of Facebook addressed this particularly well.
The reviewed literature suggested that the best use of a digital platform in this context would be one that drew on dynamic and interactive components. We therefore created sharable content for the STASH study website, which participants were able to post and comment on in Facebook groups, and adapt if desired.
The STASH study website
The first website iteration required PSs to log in with individual passwords. However, pilot data suggested that this created an unnecessary barrier, should technical issues arise (e.g. forgotten password). We also subsequently realised that opening the website to all students could allow PSs to direct friends to visit for themselves. The final version, therefore, required only a school-wide password (circulated by PSs). An additional login for PSs, via a bespoke API (created by Antbits), allowed PSs to post messages directly to their Facebook groups. Website accessibility was thus increased, while maintaining a degree of security that limited contamination beyond S4 at participating schools. We reiterated at training that PSs should give the STASH study password to friends in S4 at their school only, and they were provided with STASH study cards indicating the web address to facilitate this.
Based on the pilot and professional workshop findings, the website was significantly streamlined for the feasibility trial stage. Key revisions included removal of subsections for different activity types, replacing textual messages with more visually appealing bespoke infographics and memes, reducing external links (participants tended not to click on these) and dropping conversation prompts (which were minimally engaged with). The TMG proposed ‘gamifying’ the online component of the STASH study as a means of boosting interactivity, engagement and motivation, but ultimately dropped this idea, prioritising simplicity over desirable ‘add-ons’. Instead, it was agreed that PSs could be motivated in a ‘low-tech’ way by offering a ‘PS of the week’ prize at follow-up. We also considered a search function and ‘escape’ button (allowing students to quickly close the site); however, given the significant work required to refine basic functionality, these additions were not possible within our resources.
Participants in website testing groups were positive about the revised website, particularly with the inclusion of humorous memes and brightly coloured visuals.
The final version of the STASH study website [URL: www.stashtrial.org.uk (accessed 4 May 2020)] was organised under eight topics:
-
What’s STASH all about?
-
Is my relationship good?
-
What’s normal?
-
Am I ready for sex?
-
What’s consent?
-
How do I avoid risk?
-
Are pics and porn OK?
-
How do I feel good about myself?
Each topic had a website page, comprising an overview and a series of easily sharable messages (text, memes, infographics, embedded videos, external links; see Appendix 2 for examples) and a list of support sources.
School support and intervention profile
The pilot process evaluation echoed the existing literature in highlighting that school leadership support and contact teacher amenability to the intervention were key preconditions for successful implementation. Learning from ASSIST suggested that the contact teacher should attend PS training. Although invited, the pilot contact teacher (a DHT) was able to attend for only a brief portion of the training and instead sent a pupil support staff member. This led the TMG to reflect on whether or not a less senior member of staff would be more suited to the contact teacher role. The pilot findings also generated TMG discussions about how we might increase awareness of the STASH study across the entire staff body and led to suggestions such as highlighting the STASH study at staff meetings. Post-pilot student and teacher interviews indicated that the profile of the STASH study across the school was low. The TMG discussed and agreed that at the training PSs (and the teacher present) should agree how best to ‘announce’ the STASH study to their wider year group. Following the suggestion of one PS, STASH study PS badges were provided to PSs to identify them as such.
Trainer-led activities
Adaptations from ASSIST
The ASSIST study used pro forma diaries to track PS activity and, although these helped prompt PSs, the process evaluation found that entries were sometimes fabricated or omitted and did not offer an accurate activity record. 82 In the STASH study, the trainers and research team were able to monitor Facebook activity directly and a decision was made to capture face-to-face conversations via reports to trainers at weekly follow-ups, rather than via the more cumbersome and potentially less reliable diary method (although the conversations remained self-reported).
Previous research suggested that ‘booster’ sessions enhance intervention effectiveness. 65 The pilot confirmed that, as with ASSIST, regular follow-ups provided an acceptable means of ‘checking in’, troubleshooting and encouraging PSs. We extended this model by adding interactive learning activities to these sessions. This was done to supplement the training (as it was not possible to cover all relevant topics therein) and to maintain interest and momentum. Given the complexity of the issues and behaviours the STASH study sought to address, we added one further follow-up session for the feasibility stage, giving a total of five, plus a sixth session to conduct evaluation activities (PS questionnaire, group interviews).
To meet the concerns of teachers and child protection officers consulted regarding online bullying and sensitive online disclosures, we stipulated that a trainer (via a generic STASH study trainer account) should be a member of all PS groups. Pilot data suggested that this was acceptable to PSs, offering additional reassurance and opportunity to contact trainers with queries between follow-ups.
Peer supporter acknowledgement
During all intervention development stages, there was much discussion about how best to motivate PSs, as this was known to be essential. 60,81,83 Informed by ASSIST, and by feedback from students and professionals, we opted to provide formal academic recognition with a University of Glasgow certificate, in addition to a £10 voucher on completion of the PS questionnaire. PSs were also given the opportunity to bank time spent on the STASH study towards attainment of a Saltire Award (Scottish Volunteer Award scheme for 12- to 25-year-olds). 84 On a week-to-week basis, commitment was rewarded by a ‘PS of the week’ prize (a STASH study highlighter).
Revisiting the STASH study programme theory
As a result of the development work, we were able to more clearly articulate the critical assumptions underlying the intervention, the potential mediating factors and key contextual factors. The pre-pilot programme theory is shown in Figure 4.
The STASH study intervention design for the feasibility trial
Following development, refinement and optimisation, and ahead of the feasibility study, the final design of the STASH trial was determined as follows.
Peer nomination
All students in S4 (aged 14–16 years) are asked to complete a peer nomination questionnaire. Each school is given a different combination of nomination questions. Three are the same as those used in ASSIST:
-
Who do you respect in S4 at your school?
-
Who are good leaders in sports or other group activities in S4 at your school?
-
Who do you look up to in S4 at your school?’
Four questions are newly designed for the STASH study:
-
With whom in S4 would you feel comfortable to talk about something personal or sensitive?
-
Who in S4 is good at encouraging and persuading others to do things?
-
Whose opinion do you trust and value most in S4 at your school?
-
Who in S4 is confident at talking to people outside their friendship group?
The 25% of young people receiving most nominations, stratified by gender, are invited to a recruitment meeting.
Peer supporter recruitment
A meeting is held with nominees in each school, in which trainers explain the intervention purpose, the PS role and answer questions. The aim is to recruit 15% of the year group to participate in PS training. If recruitment attendance is poor or role uptake low (or skewed significantly towards one gender), a second recruitment meeting is held.
Two-day peer supporter training
A 2-day PS training session is held in school time, at an external venue, facilitated by Fast Forward and West Lothian Drug and Alcohol Service. The training is intended to equip PSs with the knowledge, skills and confidence required for the role; build motivation and enthusiasm for the role; generate trust and rapport within the PS group and among PSs and trainers; build sexual health knowledge and skills; improve understanding of risks and consequences; build self-esteem and self-efficacy; reinforce social support for healthy sexual norms; and boost intrinsic motivation and autonomy. PSs are required to sign a code of conduct during training and agree a plan to ‘announce’ the project to their year group.
Peer support work
The period in which PSs are active varies between schools: 5 weeks in three schools and 10 weeks in three schools.
Activities
Peer supporters are to establish ‘secret’ Facebook groups (invitation only groups with the highest privacy setting), comprising friends and the STASH study trainer. PSs are encouraged to post messages from the STASH study website to this group and to initiate face-to-face conversations centred on the STASH study messages. They are asked to alert friends to the STASH study website and to local support sources. To ensure maximum reach, PSs use STASH study cards to advertise a non-sharing version of the STASH study website, particularly to students who do not use Facebook. PSs are supported by a trainer for the duration of this period, as well as by an appointed contact teacher. As far as possible, PSs are encouraged to engage with intervention resources flexibly; for instance, they can choose which messages and links to share, and have the option of editing messages into their own words.
Trainer-led activities include moderation of group discussions and monitoring posts, supporting the PSs and facilitating follow-up meetings (weekly or fortnightly) with all PSs for the intervention duration.
Acknowledgement
Peer supporters who fulfil the requirements of the role would be provided with University of Glasgow certificates and, if they complete the online questionnaire, a £10 gift voucher. Schools may also support PSs towards attainment of an accredited Saltire Award.
Chapter 3 Study methods
This chapter describes the methods for the feasibility trial. The study objectives are described in Chapter 1, Aims and objectives. The development of the STASH study intervention (including methods of the development stage) can be found in Chapter 2. A full description of the post-pilot intervention can be found in Chapter 2, The STASH study intervention design for the feasibility trial.
In this chapter we describe the overall study design, and present the progression criteria regarding the feasibility and acceptability of the intervention and evaluation methods (the primary outcome for the trial). We then describe the process evaluation [including social network analysis (SNA)], piloting of outcome measures and economic evaluation. Within each of these sections, we describe the aims, methods, measures and analysis.
Study design and setting
The STASH study was a non-randomised feasibility study conducted with students in six mixed-sex, state-funded secondary schools in Lothian, Scotland, during the 2017/18 academic year (August 2017 to June 2018).
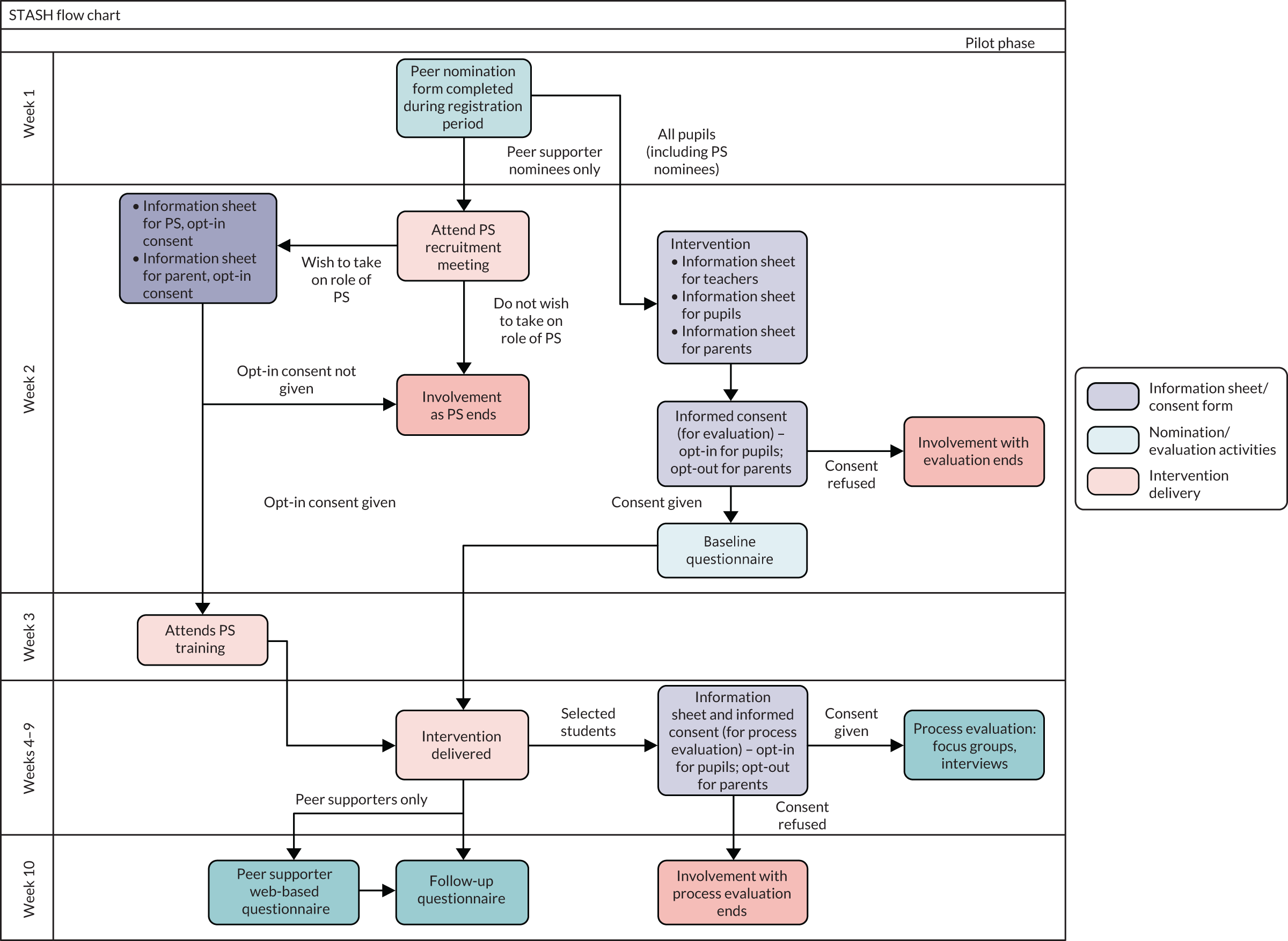
All six study schools received the intervention and provided both intervention and control data. The latter were provided by students in the year above the intervention group and were collected prior to the delivery of the intervention. These were then compared with data from the intervention year group collected 1 year later. Control and intervention participants were therefore the same age when they completed the control and follow-up questionnaire, respectively, but the intervention year group had received the intervention and the control group had not. A flow chart for the study is shown in Figure 5 and a flow chart for participant involvement in the intervention and evaluation is shown in Figure 6.
FIGURE 5.
The STASH study flow chart. Reproduced from the STASH protocol, Forsyth et al. 62 This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/. The figure includes minor additions and formatting changes to the original figure.
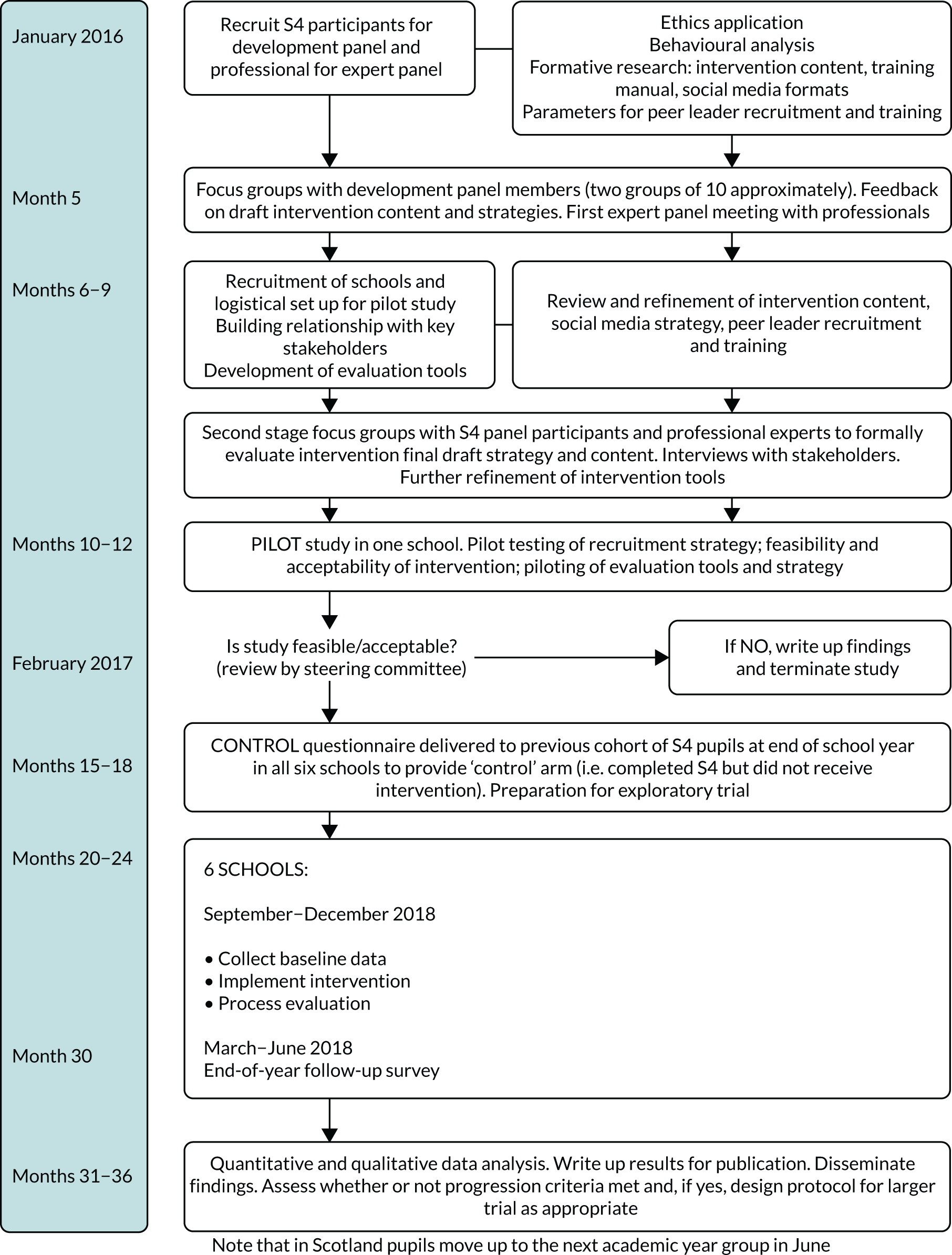
FIGURE 6.
Movement of participants through intervention and evaluation.
Participants
Participants were year 4 students (aged 14–16 years) in secondary schools meeting the study inclusion criteria. (In Scotland, secondary school education begins at age 11 years and comprises 6 years, with compulsory education ending after 4 years.)
Intervention participants were students in S4 during the academic year (2017/18) when the STASH study was delivered. Control participants were in S4 in the previous academic year (2016/17).
Inclusion criteria
Secondary 4 students (aged 14–16 years) in state-funded schools who had received, or were receiving, teacher-led sex education, regardless of their sexual experience or individual level of risk, were eligible to participate.
Exclusion criteria
Students attending private or independent schools or state schools not currently delivering comprehensive sex education were ineligible.
The STASH study was designed to augment rather than replace usual sex education. Therefore, to participate, schools had to be already providing SRE. At the time of study, most Lothian schools were delivering a version of the Sexual Health and Relationships Education (SHARE) package85 as part of their personal and social education curriculum. Faith schools were included in the invitation to participate, but none took up the offer.
Sample size
As a feasibility study, the STASH study was not designed to identify an estimate of effect and thus a standard power calculation was not appropriate. We anticipated that 1400 participants would be sufficient to allow qualitative and quantitative progression criteria to be assessed and provide information on key parameters for the design of a future trial, and that a cluster of six schools would enable us to generate an estimate – albeit imprecise – of ICC, when combined with a range of ICC estimates from published evaluations of similar interventions, using the model outlined by Turner et al. 86 The average year size for West Lothian is 160 students and, allowing for a non-response rate of 15% due to student absence, we estimated a sample size across six schools of approximately 700 intervention participants and 700 control participants. We thus aimed to recruit six schools.
Selection and recruitment of schools
Schools in the study area were introduced to the STASH study by management staff at West Lothian and South West Edinburgh education authorities. The research team followed up these introductions by e-mail and visited those expressing interest. All interested schools received a STASH study brochure outlining project steps, roles and responsibilities. HTs and DHTs agreed to participate on behalf of the school and usually handed on responsibility for the STASH study to a contact teacher (typically someone with responsibility for personal and social education, physical education or pastoral care). A senior staff member was asked to sign a research agreement, after which point the school was considered formally recruited into the study.
At the end of the evaluation activity, schools received £500 compensation for any disruption caused by the intervention or evaluation activities and an extra £500 to cover backfill costs for teachers to attend sessions such as the STASH study training.
Criteria for progression to a full trial
The main aim of the feasibility trial was to assess the feasibility and acceptability of the intervention and evaluation methods to PSs, the target group and stakeholders. The primary study outcome was whether or not the study met progression criteria regarding the feasibility and acceptability of the intervention and evaluation methods.
The criteria, outlined in Table 1 were discussed within the TMG and agreed via discussion with the TSC after the pilot and before the main feasibility stage. The results reported in Chapters 5–7 are focused on ascertaining whether or not these criteria were met, as well as contextualising the broader experience of the trial in relation to the criteria and study objectives. There was some debate within the TMG around criterion 1. The figure of 60% (for role uptake among nominated students) was set based on learning from ASSIST67 and in view of the need to ensure that PSs had reach or influence across their social networks. However, it was acknowledged that with an older year group in a public examination year and a more sensitive intervention topic, it would be harder to recruit PSs in the STASH trial than in ASSIST. The question of whether or not 60% was still required in an intervention engaging social media as well as face-to-face interaction was also raised. These issues are discussed in Chapters 5 and 6 and revisited in Chapter 9.
| Number/chapter | Target | Assessed by | ||
|---|---|---|---|---|
| Green | Amber | Red | ||
| 1 | Acceptability of role/feasibility | Was it feasible to recruit PSs? | ||
| Chapter 5 | In each of four schools, 60% of nominated students are recruited and complete the training | 50%, in each of four schools | Amber target achieved in fewer than four schools | Attendance monitoring at recruitment meetings and training (monitoring log) |
| 2a | Reach/feasibility | Were PSs able to carry out the role? | ||
| Chapter 6 | In each of four schools 60% of PSs complete the training, send three or more messages/have three or more conversations and attend two or more follow-up meetings | 50%, in each of four schools | Amber target achieved in fewer than four schools | PS questionnaire administered at last follow-up session; project monitoring log; PS activity log |
| 2b | Acceptability | Was the STASH study acceptable to PSs? | ||
| Chapter 5 | In each of four schools 60% of PSs report that they ‘liked’ the role | 45%, in each of four schools | Amber target achieved in fewer than four schools | PS questionnaire: ‘I liked being a PS’ (five-point Likert scale) |
| 3a | Acceptability | Was the STASH study acceptable to the wider target group? | ||
| Chapter 5 | In each of four schools, 60% of students who are exposed to the STASH study agree that the intervention was acceptable | 50%, in each of four schools | Amber target achieved in fewer than four schools | Follow-up questionnaire: ‘The way the STASH project was run was acceptable’/‘The information given in the STASH study was acceptable’ (five-point Likert scale) |
| 3b | Acceptability | Was the STASH study acceptable to participating schools? | ||
| Chapter 5 | No major acceptability issues raised | One or two major issues | Major acceptability issues | Teacher interviews at end of intervention |
| 3c | Acceptability | Was the STASH study acceptable to parents? | ||
| Chapter 5 | Less than 15% of PSs report that their parents/carers were unhappy about them being a PS | Less than 20% | Amber target not met | PS questionnaire (‘My parents/carers were happy that I was a PS’); teacher interviews; PS interviews |
| 4 | Acceptability of evaluation/feasibility | Were the evaluation methods acceptable and feasible? | ||
| Chapter 4 | In each of four schools, student response rates of > 70% at baseline and follow-up | Student response rates of > 60%, in each of four schools | Amber target not met | Control, baseline and follow-up questionnaire; PS and non-PS interviews |
A traffic light system was adopted, in which meeting the green target was a very strong indication to proceed, amber was a medium indication to proceed and red an indication of doubt (i.e. whether or not to proceed). Amber and red targets required discussion with TSC and an identified mitigating strategy. In the case of a red, other indicators should be amber or green to proceed. Table 1 describes the criteria, target, measure, method and time of measurement.
Process evaluation
Purpose of process evaluation
The process evaluation was undertaken primarily to assess whether or not progression criteria were met (see Table 1), but more broadly to evaluate the following:87
-
Implementation: what was put in place and exactly how was it implemented?
-
Mechanisms of impact: how did the intervention produce change?
-
Context: how did contextual factors shape implementation and outcomes?
In line with the study objectives, we sought to assess (1) the extent to which it was possible to recruit and retain PSs, (2) the acceptability of the role to PSs and key stakeholders and (3) the extent of intervention fidelity (i.e. whether or not PSs, trainers and schools were able to carry out the intervention activities as intended). The process evaluation also sought to identify barriers to and facilitators of successful implementation, to contribute to refining and testing the programme theory and to investigate the potential and limits of using social media to diffuse messages. We also evaluated the extent of friendships outside the school and therefore estimated potential contamination in a full-scale cluster randomised trial.
We undertook a SNA as part of the process evaluation. This sought to assess the potential reach of PSs across the S4 year group, by examining their position within the year group network. We wanted to understand the extent to which the nomination and recruitment process had resulted in PSs who could serve as ‘information hubs’ (network centrality) and who, as a group, could span an effective number of friendship subgroups within the year.
We also used SNA to investigate how friendship interactions were shaped and sustained by network properties, as well as individual characteristics, before and after the intervention. The analysis highlighted how perceived friendships interacted with the PS role. We also looked at homophily, that is whether subgroups within each school network were formed around gender (e.g. did young women tend to be friends with young women?) or sexual behaviour (did sexually active students mainly befriend other sexually active individuals?), and whether or not students influenced each other’s behaviours.
Process methods
We undertook basic process evaluation activities in all six schools and enhanced data collection in four ‘case study’ schools. One school was excluded as a case study school, as it had recently been part of a highly intensive research study, whereas another was specifically included because we were interested in exploring intervention feasibility in a very small school. In selecting two case studies from the remaining four schools, we sought balance in terms of urban/periurban location, school size and proportion of free school meals (FSM) (see Chapter 4).
Evaluation activities for all schools comprised:
-
A monitoring log (spreadsheet) of all intervention activities (e.g. attendance at training and follow-up meetings by gender, field notes from school visits and informal conversations between research team/teachers).
-
An anonymous evaluation questionnaire on PS training, completed by PSs (n = 104) and school staff (n = 12). It was completed immediately following training and capturing views on training activities, students’ perceptions of what they gained and staff views of content and organisation.
-
An anonymous online questionnaire for all PSs (n = 88, 85% response rate). It was completed in a computer room during the final follow-up session. PSs received a £10 voucher on completion. Data were captured on the specifics of PS activity and engagement (see Measures used in process evaluation).
-
Interviews with the STASH study trainer (n = 3). Conducted separately with each trainer, these addressed perceptions of intervention components (including what worked and what did not work, and why), their role and potential future improvements.
-
Reflective record of all activity sessions (recruitment, training and follow-up) completed by trainers (n = 48). These captured student attendance and engagement, and any modifications made to the session plan.
-
PS activity log (spreadsheet) recording Facebook group membership (by gender) and posting activity. Anonymous data were extracted via the STASH study trainer account (with PS consent obtained at the intervention’s outset). The number of face-to-face conversations self-reported at follow-up sessions was also logged (extracted from trainer reflective records).
-
Items on a follow-up questionnaire assessing engagement in the STASH study intervention activities, views on acceptability of format and content.
-
Items on friendship ties from baseline and follow-up questionnaires for SNA (see Measures used in process evaluation).
Enhanced process evaluation activities comprised:
-
Structured observation conducted by the research team at recruitment (n = 4), PS training (n = 8) and follow-up (n = 8). A non-participant observer sat in a discreet place and, using an observation guide, recorded data on fidelity (activities carried out as intended), acceptability (apparent responses of/interaction with students, challenges arising), exposure (degree of student engagement) and any relevant contextual information.
-
Semistructured interviews with PS and non-PS students (11 groups/pairs, n = 42 participants). PS interviewees were selected to give a mix of gender and engagement (whether using Facebook or face-to-face interaction only). Non-PS students were recruited via PSs (with support from the contact teacher) as we were interested in understanding views of students who had some exposure to the intervention activities. Interviews addressed awareness of the STASH study, acceptability and engagement with messages and perceptions of impact.
-
Semistructured individual or paired interviews with school staff and the STASH study contact teacher plus a member of senior management team with pastoral responsibilities and some awareness of the STASH study intervention (seven interviews, n = 8 participants). Interviews focused on perceived value and impact of intervention, and potential barriers and facilitators from the schools’ perspectives.
Measures used in process evaluation
The PS questionnaire (see Report Supplementary Material 2) focused on PS experiences regarding the feasibility and acceptability of the role. It comprised a wide range of items, measuring PS activity, time spent on the role, how easy or difficult they found the role, extent to which they were able to meet challenges and difficulties (including technical issues), views on the role and the STASH study website and training content, perceptions of parent and teacher views on their involvement, how their peer group responded and interest in ongoing involvement.
The process evaluation also used measures from the baseline and follow-up questionnaires (see Piloting of outcome measures). These focused on measuring exposure to the STASH study activities among all students; the acceptability of intervention content and activities among those exposed; the use of Facebook; whether the STASH study was more or less relevant, helpful or interesting compared with usual classroom SRE; whether or not it was age appropriate; and the likelihood of using the STASH study website or talking to a PS in future.
For the SNA, students were asked to name up to six friends and for each to give information on gender, if in year group, if connected on Facebook, if they would share private information with the person, and if time spent together was in school, outside school and/or online (yes/no options).
Analysis of process data
The process evaluation framework details data sources for all process research questions, whereas the qualitative analysis plan gives more detail on the analysis (see Report Supplementary Material 3). Quantitative data from the follow-up questionnaire (see Report Supplementary Material 4) and PS questionnaire (see Report Supplementary Material 2) were summarised descriptively and stratified by gender, as relevant. A descriptive summary was produced from the PS activity log (Microsoft Excel® file; Microsoft Corporation, Redmond, WA, USA), collating group membership numbers, total posts, total reactions to posts and reported face-to-face activity. Information on Facebook group membership was documented by school for the SNA.
Project monitoring data were entered into a different Excel document and subsequently summarised descriptively. Data included specifics on PS nomination, recruitment, training, attendance at follow-ups and completion, broken down by gender and school; contemporaneous events, such as relevant news stories; significant communication with schools; and key school information.
Transcribed qualitative data from observations (recruitment, training and follow-up) and interviews (teachers, trainers, PSs and non-PSs) were entered into NVivo 11 qualitative analysis software (QSR International, Warrington, UK) to manage data retrieval. We undertook a thematic analytic approach informed by the framework method. 88 A coding framework was developed and applied to transcripts, based on the key aims of the process evaluation [i.e. fidelity, acceptability, exposure, reach, contextual factors (including barriers to and facilitators of implementation), plus researcher reflections on the process of implementation]. From this descriptive stage, data were interpreted further to establish links between themes, develop potential explanations around such links and to better understand the functioning of the intervention. Quotations were selected both to exemplify and illuminate key findings, and to illustrate variation in participant experiences and perspectives. The primary aim was to assess the overall feasibility of the intervention, based on analysis of these constituent themes.
Social network analysis
We conducted a SNA study to evaluate the potential reach of PSs across their social networks. From a SNA perspective, a network is composed of a set of nodes and a set of ties connecting some of the nodes. In this case, nodes corresponded to students in school and a tie appears each time there is a reported friendship relationship among them.
In principle, it can be assumed that each node is capable of connecting with anyone else in its network. However, individuals tend to have preferred patterns of connections because they tend to enjoy some ties more than others. These preferences, usually reciprocated, generate a specific pattern among all members of the network.
In general, SNA measures and routines help in the rigorous and systematic visualisation of the distribution of preferences represented by a tie among pairs of individuals and in testing and exploring the properties of the network (e.g. closeness, cohesion and clustering).
In the present study, students were asked to name up to six friends and for each to give information on gender, if in year group, if connected on Facebook, if they would share private information with the person, and if time spent together was in school, outside school and/or online (yes/no options).
First, we used a direct reach measure, that is the number of students directly connected to a PS (% of the total) to evaluate the potential reach of PS through their direct friendship ties. Second, we measured target reach, corresponding to the number of friendship clusters containing a PS, expressed as a percentage, and revealing the distribution of PS within friendship subgroups. In this case, we applied the algorithm developed by Girvan and Newman89 based on the identification of ties whose removal contribute to the breakdown of the network in small subgroups. Third, we applied standard SNA centrality measures to compare (1) students who were nominated but declined the PS role, (2) students who were nominated and took up the PS role and (3) other students. In particular, we used indegree, two-step reach90 centrality and eigenvector centrality. Indegree corresponds to the number of incoming ties, that is the number of times an individual was named as a friend. This can be interpreted as a measure of popularity, as high indegree scores indicate students who have been named as a friend by many others. The two-step reach centrality measure indicates the potential of PSs to spread the STASH study information with other students within two steps (e.g. via word of mouth). This measure examines how close each student is to all the others. Eigenvector centrality indicates how well connected an individual is by considering how well connected their friends are. This measure can also be considered as an indication of popularity: students with high eigenvector centrality are connected to other students who are themselves well connected. Table 2 summarises the measures and their visual representations.
| SNA centrality measure | Definition | Visual representation |
|---|---|---|
| Indegree | The number of ties going towards a node |
|
| Two-step reach | The number of nodes a given node is able to reach in k steps; in our case k = 2 |

|
| Eigenvector | Each node’s centrality is proportional to the sum of the centrality scores of the nodes that are connected to it |

|
To analyse changes in ties from baseline to follow-up, we applied a stochastic actor-oriented model for network dynamics. 91–93 These classes of statistical simulations are commonly used to test hypotheses regarding the co-evolution of behaviours and networks related to a set of individuals. In our case, we used stochastic actor-oriented models to analyse the formation of ties among students considering individual characteristics (gender, being a PS or not being a PS), behavioural characteristics (sexual experience, self-assessed confidence to refuse unprotected sex, self-assessed knowledge of STI risk) and the influence of PSs in promoting preventative healthy sexual behaviours.
Each network was analysed separately and then a Fisher’s test (which combines independent p-values of parameter estimates and standard errors across the networks) was used to determine the presence of significant differences among schools. We used meta-analysis to aggregate the resulting values of the parameter estimates for each school and compare them on a common scale (see Appendix 3). Finally, we used the goodness of fit test to examine whether or not our data samples fit the simulated networks. 94 These analyses were conducted in the simulation investigation for empirical network analysis package (version 1.2–14, released 5 December 2018) in the R statistical software (The R Foundation for Statistical Computing, Vienna, Austria).
Piloting of outcome measures
Purpose
A key study objective was to identify key trial design parameters for a future evaluation, including candidate primary and secondary outcomes, ICC and sample size. Since setting this objective, the DELTA2 guidance has been published, which advises against using estimates of effect from pilot studies to calculate the sample size for a full trial because of their imprecision. 95 We therefore did not seek to fully meet this objective. The purpose of collecting these outcomes was to pilot our outcome measures and analysis methods to assess the utility of these for a future definitive trial. The quantitative analysis was not intended to offer any guide to the intervention’s effectiveness due to lack of statistical power.
Outcome methods
The control questionnaire was administered first (March–June 2017) to the S4 year group above the intervention cohort. We administered the baseline questionnaire in August/September 2017 to the intervention cohort, who had just moved up to become the new S4 year group. We administered the follow-up questionnaire to this same S4 group post intervention (March–June 2018). Compared with the control questionnaire, the baseline questionnaire had a reduced set of outcome measures and the follow-up questionnaire had additional exposure measures.
Outcome measures
Baseline characteristics
Student characteristics describing the study sample were collected at baseline. These were:
-
gender
-
age
-
SIMD
-
residence
-
ethnicity
-
number of examinations being taken
-
plans for leaving school
-
views on religion.
School characteristics were collected at baseline for each school:
-
total number of students (student roll)
-
urban/rural
-
FSM (per cent)
-
National 5 examination results.
Potential primary and secondary outcome measures
The end outcomes for the trial we sought to test were:
-
delayed initiation or abstinence from sexual activity
-
consistent condom use among those who are sexually active.
We considered a range of potential primary outcome indicators to set an indicative primary outcome for use in any subsequent trial. Given that sexual behaviour would be expected to increase from baseline to follow-up due to maturation effects, the primary comparisons were between intervention and controls at follow-up.
Potential primary outcomes collected were:
-
condom use at last vaginal intercourse
-
condom or dental dam use at last oral sex
-
number of sexual partners in last 3 months and whether or not a condom was used
-
frequency of condom use in the last 6 months
-
proportion of students who have not had sex in the past 6 months or have not had sex at all.
Potential secondary outcomes collected were:
-
STI prevention and sexual health-related knowledge (drawn from, and adaptations of, existing survey items, e.g. Sexunzipped96), including knowing where to seek help locally (adapted from the Healthy Respect study97)
-
ease of talking about sex with parents/carers and friends [adapted Natsal measure;98 URL: www.natsal.ac.uk/natsal-3/questionnaire.aspx (accessed 5 May 2020)]
-
ease of talking about sex with a boyfriend or girlfriend [adapted Natsal measure;98 URL: www.natsal.ac.uk/natsal-3/questionnaire.aspx (accessed 5 May 2020)]
-
confidence in STI prevention skills (adapted from range of existing survey items, e.g. Sexunzipped96)
-
‘competence’ at first intercourse or competence at last intercourse [adapted from Natsal measure;99 URL: www.natsal.ac.uk/natsal-3/questionnaire.aspx (accessed 5 May 2020)]
-
sexual attitudes and adherence to sexual health norms (12 new items, adapted from a range of existing survey items)
-
perception of whether or not others are sexually active (newly designed item)
-
intimate relationship well-being (seven newly designed items)
-
distress about sex life (adapted Natsal measure100)
-
use of internet and social media for finding sexual health information, sexting and viewing sexual images (six newly designed items)
-
Short Warwick–Edinburgh Mental Well-Being Scale (SWEMWBS)101
-
conversations about STASH study-related topics (10 newly designed items)
-
self-esteem – two items from the Randomised Intervention trial of PuPil-Led sex Education (RIPPLE) study,33 plus a single-item global measure102
-
self-reported sexual activity.
Effect modifiers
A number of effect modifiers were measured. These included the student characteristics (see Baseline characteristics), along with:
-
self-reported risk behaviours in peer group
-
school climate and engagement103 (items drawn from the Beyond Blue School Climate Questionnaire)
-
parental monitoring (three newly designed items, drawing from existing measures)
-
sexual attraction (modified version of the Kinsey scale) and sexual identity (adapted item from Natsal)
-
self-regulation104 (three items drawn from the 36-item Adolescent Self-Regulatory Inventory104)
-
importance of social media to social life (two newly designed items).
Student roles and exposure
Derived variables were created to categorise students by their role in the intervention and by their level of exposure. These measures were used both in the process and outcome analysis. They are summarised below.
Intervention identification (intervention group only)
-
PS: those who attended training, regardless of whether or not they completed the role.
-
Nominee: nominated and invited to recruitment meeting, but did not attend training.
-
Other student: neither of the above.
Level of exposure (intervention group only)
-
Trained PS.
-
Exposed non-PS student reporting one or more of the following:
-
been shown the STASH study website by a PS or accessed it themselves
-
joined, viewed posts or followed links in a STASH study Facebook group
-
talked to friends about STASH study Facebook posts
-
talked to or asked a PS about a STASH study topic.
-
-
Unexposed: non-PS student who did not meet any above condition.
-
Unknown: non-PS student who did not complete the follow-up questionnaire (meaning exposed/unexposed status could not be assigned).
Development of measures over subsequent survey administrations
As a key purpose of the outcome analysis was to pilot measures, a small number of changes were made across subsequent survey administrations. Some items were improved, for instance the item on gender became two stage to allow students to report sex at birth and current gender identity. Minor modifications were made to response options (e.g. separated out ‘never or almost never’ options for items on parental monitoring) and small tweaks were made to instructions or explanations (e.g. ‘a penis in a vagina’ added as explanation to item on sexual intercourse in the follow-up questionnaire). Other changes were substantive. For instance, the question bank on ‘competence’ (extent to which sex is wanted, protected, not under influence of drugs/alcohol and not regretted) was switched from being asked about first sex to most recent sex, because the number eligible to report on their most recent sexual encounter was much larger.
Outcome data analysis
The full details of the outcome measures are given in the statistical analysis plan (see Report Supplementary Material 5).
Continuous variables were summarised by the number of observations, number of missing values, the mean and standard deviation (SD), the median and interquartile range, and the minimum and maximum values. Categorical variables were summarised by the number of observations, number of missing values and the number and percentage of subjects who are in each of the categories. No missing data were imputed.
Baseline student characteristics were summarised overall and by study group. Characteristics were also summarised separately for those who did not complete the follow-up survey, to investigate any systematic dropout. School characteristics were summarised overall and listed for each school. Feasibility and acceptability outcomes were summarised overall and by school. Outcomes collected for both the control and intervention groups were summarised by study group.
Questionnaire validation was carried out for the potential primary and secondary outcomes. Principal component analysis (PCA) was applied to the entire questionnaire (at baseline) to assess whether or not there was a small number of individual domains that explained the majority of the variability in the data set. PCA was also applied to items with certain question banks (groups of questions assessing the same topic or underlying construct). Principal components representing clear question domains (i.e. combinations of questionnaire items) were taken forward into the primary and secondary outcomes analysis. Validated measures were not included in the PCA process.
To assess the effect of the intervention on the potential primary outcome, mixed-effect logistic regression models were fitted to study group, with a fixed effect for study group and a random effect for school. Similar models, adjusted for appropriate effect modifiers, were run to identify the factors that had an effect on the outcome. This helped indicate whether or not future studies should adjust for such factors.
The model-estimated odds ratios (ORs) and corresponding 95% confidence intervals (CIs) were reported for the intervention effect and any effect modifiers, for each of the models. The ICC is a key parameter that the study sought to estimate to inform decisions about the sample size for a full evaluation of the STASH intervention. This is based on generalised linear mixed models fitted to the primary outcome, with a random effect for school and no fixed effects. Models were fitted to the data from all follow-up and control participants and separately by study group. Sample size estimates were provided for all ICCs estimated, as estimates of the ICC can vary between study groups. The ICC was estimated using methods detailed in Wu et al. 105 and implemented using R code [URL: https://github.com/timothyslau/ICC.merMod/blob/master/functions.R (accessed 5 May 2020)].
These analyses were exploratory and focused on identifying appropriate outcome measures. As the study lacks statistical power, little value can be given to the estimates of difference between the control and intervention groups. Furthermore, there were notable differences between the control group and intervention group, particularly in relation to gender, which would be much less likely to occur in an appropriately powered study. Therefore, estimates of effect are liable to be affected not only by random error, but also by confounders (including unmeasured factors), which cannot be fully controlled for.
Economic evaluation
Aim
The aim of the economic evaluation was to determine the key components of a future cost-effectiveness analysis and test data collection methods.
Measures
To calculate STI-related health-care costs, we assessed the feasibility of collecting self-reported health-related health-care resource use (STI testing and treatment, contraception, including out-of-pocket costs) at follow-up. This included contacts with school specialists, health-care professionals in STI services and primary care, STI treatment and prevention, and pregnancy-related costs. Control and intervention students were asked at the end of S4 to report the number of times they had used each service in the past 6 months. We report descriptive statistics, including missing data, to evaluate the feasibility and acceptability of collecting this information.
The National Institute for Health and Care Excellence recommends that evaluations of new interventions include a cost-effectiveness analysis: the incremental cost per unit gain in an effectiveness measure. Quality-adjusted life-years (QALYs) calculated using the EuroQol-5 Dimensions (EQ-5D) are the preferred effectiveness measure in cost-effectiveness analyses. 106 There is no preference-based tariff for the EQ-5D that can be used to calculate QALYs in children. Instead, we explored the Child Health Utility 9D (CHU-9D) to calculate utility scores,107 completed at baseline and at the end of S4 in control schools, and at the end of S4 in intervention schools.
Quality-adjusted life-years are not always the most suitable effectiveness measure in economic evaluations of public health interventions. 108 We evaluated if the CHU-9D was sensitive to changes in the potential primary outcome, to determine its suitability in an economic evaluation of the STASH study. We also report descriptive statistics for the CHU-9D and its relationship with (1) SWEMWBS and (2) self-esteem, to provide a picture of how it functions within this population group.
Calculating the cost of the STASH study
The key cost of the STASH study is the cost associated with the identification and training of the PSs, as well as trainer-led activities (e.g. follow-up sessions). Based on data collected, we calculated the average number of hours spent by trainers in each activity. This was multiplied by the hourly cost of a trainer to give the average cost per trainer. Any additional costs of the training, in particular the cost of the 2-day training, including room hire and refreshments, was also collected and included as part of the total cost per trainer. We also collected information on the amount of time spent by teachers on STASH study-related activities, including booking rooms, co-ordinating with other teachers and attending sessions. Teacher time spent on the STASH study was multiplied by average hourly gross earnings of a UK secondary school teacher in 2017 of £23.24,109 to calculate the total cost of teacher time spent on the STASH study. This is considered the ‘opportunity cost of STASH’. Although it is not a direct cost to the school, it is a cost as teachers could have spent this time doing other education-related activities, which may have had a greater or lesser benefit to students than time spent on the STASH study.
The total cost of PS training plus the total cost of teacher time was divided by the number of students in the intervention arm to obtain the cost per student of the STASH study. Ninety-five per cent CIs were calculated based on 3000 bootstrap replications.
Calculating the cost of sexually transmitted infection-related health-care use
Resource use for each student was multiplied by unit costs from the most recent Unit Costs of Health and Social Care published by the Personal Social Services Research Unit,110 reference costs111 and other published sources, when required (Table 3). To calculate the mean difference in costs between control and intervention students, we used a general linear model with random effects for school and controlling for imbalances between control and intervention groups. Ninety-five per cent CIs were calculated based on 3000 bootstrap replications.
| Resource | Unit cost (£) | Reference |
|---|---|---|
| Sexual health clinic | 121.12 | Reference costs111 |
| School nurse (band 5 nurse for 20 minutes) | 12.00 | PSSRU112 |
| GP (including direct staff costs) | 31.00 | PSSRU112 |
| General practice nurse (20 minutes) | 12.00 | PSSRU112 |
| Condoms (pack of three) | 2.29 | Boots Company plc (Nottingham, UK)113 |
| Other contraception (assume the pill and over 6 months) | 19.90 | BNF114 |
| Pregnancy test | 3.99 | Boots Company plc115 |
| STI test | 16.00 | Reference costs111 |
| Emergency contraception | 16.00 | BNF114 |
Quality of Life
Descriptive statistics are reported for CHU-9D utility scores by gender, sexual orientation and FSM (a proxy for socioeconomic status).
Descriptive statistics for the mean utility values by intervention and control students, and at each time point, are also reported. The difference between control and intervention students was calculated using a multilevel model, with time and the intervention as a fixed effect, including schools as a random effect and adjusting for imbalances between control and intervention groups.
Multilevel model linear regression models accounting for individual and time were used to describe the linear relationship between the CHU-9D and (1) well-being (SWEMWBS) and (2) self-esteem. These were also used to test the sensitivity of the CHU-9D in changes in the proposed primary outcome and, hence, its suitability as an effectiveness measure in a cost-effectiveness analysis of the STASH study.
Analysis
Cost-effectiveness analysis
Although the study was not designed as a confirmatory trial, an analysis was conducted to provide an initial estimate of the probability that the STASH study intervention is cost-effective compared with current practice from a health-care and wider cost perspective.
We estimated the mean incremental cost per 1-point gain in utility of the intervention compared with control from a health-care cost perspective, in line with the NICE guidance106 on economic evaluations. Costs and utilities are from the bootstrap adjusted analyses. A secondary analysis included the cost of the STASH study and out-of-pocket costs.
We used the bootstrap results to calculate the cost-effectiveness acceptability curve: the probability that the intervention is cost-effective compared with control for a range of values of willingness to pay for a gain in utility. We also reported a cost-effectiveness plane of the bootstrap results.
Missing data
In the follow-up questionnaire, free-text responses were allowed for the number of times a sexual health resource was used. As a result, students erroneously entered responses, such as the clinic they used, or entered the response ‘a few’, rather than the number of times that they used that service or resource. For each variable when this occurred, the results for that resource were interrogated and the most likely number was selected; for example, if the student entered a clinic name for resource use and the mode for that response was ‘1’ then the value ‘1’ was entered, and if they entered ‘a few’ and the mode was ‘2’ then the value ‘2’ was entered.
All analyses are complete case.
Subgroup and sensitivity analyses
We conducted a subgroup analysis for gender (boys and girls). Different assumptions regarding the cost of the STASH study are included as sensitivity analyses.
Ethics and governance
Ethics approval
Ethics approval was granted by the University of Glasgow Medical, Veterinary and Life Sciences College Ethics Committee in two stages:
-
intervention development/pilot, project number 200150088
-
feasibility study, project number 20160002.
Written consent was sought from all participants taking part in research activities, using information sheets and oral explanations by researchers. The exception was observations made at PS activities; here, participants were given a verbal explanation of the researcher’s presence and advised that no identifying information would be recorded. All students and their parents in the S4 intervention group were sent information on the STASH study. Parents and carers were given the opportunity to opt out their child from the survey and qualitative interviews. PSs and their parents gave written (opt-in) consent to take on the PS role. PSs were advised that the research team would have access to activity in secret Facebook groups to log activity (such as the number of posts and ‘likes’), but that no personal data would be recorded. At all study stages, participants were informed that they could withdraw from any research component at any time without prejudicing their experience at school. Research participants were reassured that their answers would be treated in confidence. In qualitative interviews, participants were advised that the researcher would only break confidentiality if they made a disclosure suggesting that they might be at risk of serious harm or of harming others. The intervention website included links to local and national referral services for sexual health and well-being, as well as child protection services.
All researchers and fieldworkers working in schools had Protecting Vulnerable Groups clearance.
Assessment of harms
The intervention was low risk to participants. The team anticipated that the main risk would be psychological harm resulting from online bullying and breaches of private information by peers. The issue of ‘harm’ was investigated in the process evaluation. Procedures were developed for reporting trial protection concerns in schools (see Report Supplementary Material 6 and 7). The former was designed in consultation with the child protection lead for West Lothian Health Education Authority and the latter in consultation with the TSC.
A number of steps were taken to mitigate the possibility of harm: PSs were required to sign up to a code of conduct (the STASH study charter); social media use was confined to private (‘secret’, i.e. non-visible, invite-only) Facebook groups, of which a STASH study trainer was a member; trainers undertook monitoring ‘spot checks’ and PSs were encouraged to report inappropriate posting to the trainer and/or STASH study contact teacher; PSs had the option of privately messaging the trainer with any concerns; and trainers were advised to pass on any concerns to the contact teacher without delay. Procedures for dealing with inappropriate online behaviour followed the information and communication technologies code of conduct and discipline code of participating schools.
Peer supporters were trained on how to respond to any sensitive disclosures from their peers (such as respecting privacy) and on when to share a disclosure with the staff contact teacher (or school teacher designated to handle child protection issues). They were advised that any disclosures that made them feel worried or uncomfortable should be reported without delay to the contact teacher/designated member of staff. After this point, the school procedure for handling disclosures relating to child protection would be followed.
In terms of reporting ‘harms’ to the TSC and funders, the procedure set out that if alerted to a harm, the principal investigators would triage according to severity and report to the TSC and funders as appropriate. If a harm was reported for which causality by intervention was deemed possible, probable or definite, the principal investigators would communicate to the TSC within 15 days.
Governance
Trial management, data monitoring and quality assurance
The study was overseen by a TSC, consisting of an independent chairperson and three other independent members, including a lay representative (a parent and sex education specialist) and the two principal investigators (LM and KRM). The TSC met three times in total to examine the proposed methods, assess progress following the pilot and assess whether or not emerging trial results suggested that progression to full-scale evaluation was warranted. With the agreement of the TSC, no separate Data Monitoring and Ethics Committee was established because the study was deemed low risk, non-randomised and did not include interim analysis. The TSC were asked to cover the functions of the Data Monitoring and Ethics Committee, in particular in relation to ethical issues, and monitor any unintended outcomes and the continuation of the trial. The TMG met 6-weekly for the duration of the study and comprised the principal investigators, the co-investigators, study manager (RF) and process evaluation lead (CP).
Patient and public involvement
The study was co-produced with young people and professional stakeholders via an extensive series of consultations and development workshops (see Chapter 2). Working with a local youth organisation, we established a Young People’s Advisory Group to advise on study design. The group met once in the initial phases of the project. A subsequent meeting was planned, but proved too difficult to arrange because many of the original members were no longer in contact with the youth group. Instead, the study sought input from teachers and students involved in the pilot to optimise the feasibility study stage. In terms of study oversight, our TSC included a lay member who had a strong professional interest in young people’s sexual health but no training in the evaluation of complex interventions.
Chapter 4 Recruitment, evaluation acceptability and survey sample characteristics
This chapter describes the recruitment of schools into the study, retention in the study, the study sample, and the feasibility and acceptability of the data collection methods.
Recruitment of schools into the study
All schools in West Lothian and south-west Edinburgh (n = 17) were initially contacted. Two schools did not respond to the e-mail introduction (and two follow-up e-mails). Five schools declined the invitation. Of these schools, two said that they did not have capacity, one expressed concern that the PS role would be too burdensome for students and two did not provide a reason (both were Roman Catholic). Of the 10 schools that expressed initial interest in participation, three ultimately decided that they did not have the capacity to take part and the other seven were recruited into the study. One school agreed to be the pilot school (reported in Chapter 2) and the other six schools took part in the feasibility trial.
In pre-study recruitment meetings, teachers were generally positive about the idea of the STASH study. The teachers recognised a need for high-quality and contemporary SRE, and saw that the STASH study could provide this. The teachers also saw how participation in the study could assist them in meeting nationally set health and well-being targets,116 and valued the potential leadership opportunities for PSs (see Chapter 5). Concerns raised focused primarily on the potential time commitment and on the use of social media. Regarding the time commitment, concern was raised about teacher time involved in delivering the survey and about students in a public examination year taking 2 days out of school. Regarding social media, several teachers expressed concern about the potential for online bullying. The teachers described how recent cases of social media bullying in school had led them to view social media negatively. Some teachers therefore felt uneasy about endorsing social media use. The research team explained that the STASH study could potentially provide young people (and schools) with an alternative view of social media, with social media potentially playing a positive role in health education and behaviour change. The team also sought to reassure teachers that the Facebook chats would be monitored by a trainer, and this reassurance seemed important in the decision to participate. Questions raised at this stage also concerned the nomination of PSs by other students, and the research team emphasised that PSs should be invited to the recruitment session regardless of teachers’ perceptions of their suitability to take on the role.
The school sample
All schools were mixed-sex, state-run schools in the Lothian region of Scotland. They were varied in terms of the geographic location, area-level deprivation (using the SIMD) and educational attainment. Table 4 shows the key characteristics of the sample.
| School | School size (number of students)a | FSM eligibility (%) | SIMD quintile (1 = high deprivation)b | Students achieving literacy/numeracy at level 5 (%)c | Rural/urban |
|---|---|---|---|---|---|
| 1 | 1046 | 23.4 | 1 | 64 | Large town |
| 2 | 686 | 4.5 | 5 | 73 | Suburban/semi-rural |
| 3 | 1082 | 3.9 | 3 | 70 | City (central) |
| 4 | 278 | 43.5 | 2 | 30 | City (outskirts) |
| 5 | 808 | 17.0 | 3 | 52 | Large town |
| 6 | 736 | 23.0 (n = 169) | 2 | 61 | Large town |
Retention of schools in the study
All six schools in the feasibility trial remained in the study until the final data collection point and all schools undertook the key components of the intervention (see Chapter 2, The STASH study intervention design for the feasibility trial). All planned evaluation activities were carried out in each of the six schools. In one school (school 4), the contact teacher went on long-term sick leave and the role was taken up by a senior staff member who had not been part of the decision to participate in the STASH study but who was committed to the intervention. The impact of this is described in Chapters 5 and 6.
Acceptability of the outcome evaluation
Undertaking the control, baseline and follow-up surveys
We opted to investigate the feasibility and acceptability of web-based computer-assisted personal interview over paper-and-pencil interview. Computer-assisted self-interviewing enables more complex skip patterns, improves internal consistency and reduces missing items,117 but they are rarely used in school surveys. 118
The control, baseline and follow-up web-based computer-assisted personal interview questionnaires were completed by students using school computers, with paper versions available in case of technological difficulties. Dates for data collection were arranged 4 months in advance and contact teachers were asked to book computing suites, apprise relevant staff and provide class lists. Reminders were sent 3 weeks prior to data collection. At the data collection sessions, a teacher was usually present to take the register and help with queries. Two fieldworkers were allocated to each computer room, with two or three rooms used at each session. A lead fieldworker moved between rooms, to ensure that participants had arrived in the correct room and to support the fieldworkers in answering any questions. Once the class was seated and the teacher had completed the register, the fieldworker would read a short script to the class. The script provided information about the study and emphasised that data would be confidential. Participants were given an envelope containing their username, password and a web slip with a link to the questionnaire website. Participants were asked to complete the questionnaire as if they were doing an examination, with two fieldworkers per classroom ‘invigilating’ this process. Most schools completed their data collection with three visits per wave of data collection. Occasionally, additional mop-up sessions were scheduled if absence was particularly high at one of the data collection sessions.
Timetabling fieldwork
Adverse weather in March 2018 had an impact on fieldwork at follow-up in schools 1 and 4; both schools were closed as a result of snow on the scheduled week for data collection, and rescheduling of fieldwork at short notice proved challenging because of increasing proximity to public examinations (April/May). In one school, maths revision classes were scheduled after the data collection date had been set and were given priority over the survey; the research team were keen to respect these decisions. Fieldwork was also occasionally disrupted by school activities, such as field trips, work experience or special events. Sometimes these were arranged after the data collection date had been set or the STASH study contact teachers were not made aware of them. Extracurricular activities were generally held during less-pressured times in the academic calendar, such as post examinations (June). There was therefore no ‘ideal time’ to collect data, as periods away from examinations were also those in which more extracurricular activities were scheduled.
Workload for schools
The STASH study contact teacher was required to organise booking of computer suites, arrange movement of students from class to the suites to complete the questionnaire and herd any stragglers or students who had not received the communication about the survey. According to fieldworker reports, school information technology infrastructure was a limiting factor, with the number of available personal computers and computer rooms dictating the number of data collection sessions required. Fieldwork staff reported that network connectivity was acceptable in five schools, but problematic in school 6. There was also a small number of technical issues associated with the web survey, including recurrent login issues.
Ease of data collection varied between schools, but was always smoother if the STASH study contact teacher was present or available. When the contact teacher was absent or called to deal with another issue, fieldworkers were reliant on other teachers to access booked rooms and herd students. Schools varied in their capacity to cope with the absence of the STASH study contact teacher, with those assigning a clear stand-in or depute contact teacher managing more easily. In two schools, the STASH study teacher was rarely available: one through absence and one through lack of capacity. Schools also varied in the extent to which the contact teacher was able to secure ‘buy-in’ for the survey from other teaching staff, and this became increasingly difficult in the run up to examinations.
In interviews (see Chapter 3, Process evaluation), teachers highlighted logistical issues with the evaluation, referring to it as ‘a lot of work’ and ‘a bind’, particularly around organising the computer rooms. This was particularly so when schools felt that they were ‘quite limited in [. . .] resources when it comes to computers’. For this reason, teachers in two schools (schools 3 and 6) suggested that paper questionnaires would be more manageable. Another teacher (school 5) agreed that ‘a lot of organisation was needed’ to co-ordinate questionnaire sessions, but that they had all gone ‘according to plan’.
We used 53 paper questionnaires due to various logistical or technological difficulties. It was notable that data quality in the paper versions was lower. There were 62 instances of non-adherence to filtering or question instructions (skip patterns and prompts prevented these in the web survey).
Confidentiality
Adherence to examination conditions for survey completion varied between schools and classes. Fieldworkers tended to allow some general chat, unless they picked up that students were influencing or observing the responses of others. Fieldworkers reported that, owing to the layout of the computing suites, there was often little space between students. In addition, fieldworkers were required to walk around the room to assist students with queries or technical difficulties. This meant that privacy was not as easy to ensure as with a paper questionnaire (in which students can cover their answers with an arm).
Group interviews with friends of PSs (see Chapter 3) touched on the acceptability of questionnaire completion. Some students raised concerns about privacy arising from the potential visibility to fieldworkers, teachers and other students:
I just found it more weird that there was people walking around, just looking at your computer, looking what you were doing as well sometimes.
Like, sitting next to people, they can easily just look at what you’re doing.
Oh, did you feel like you didn’t have . . . ? [Privacy.] . . . Did that have any impact, do you think, on what you were filling in or what answers you gave?
Nah, not really. I just answered it.
It was mostly the people around you . . . Could just easily look at your . . .
So, were friends looking at each others?
I don’t think they were but it was just the feeling that they could.
And then like the teachers an’ all that walking around an’ you were just kinda like ‘OK’ . . .
School 3, friends of PSs, mixed group
These students were not deterred from answering questions, which may have been in part because of confidence in the confidentiality of the survey:
As long as your name’s not gonna go anywhere [on it] it doesn’t really matter.
School 3, friends of PSs, mixed group
At the end of all the questionnaires, participants were asked ‘Is there anything at all you would like to tell us about the STASH project or this questionnaire?’ and the responses were coded post hoc. Of 1979 completed questionnaires, six participants made comments on confidentiality in the open-ended ‘additional comments’ section, including ‘Nothing is stopping anyone from looking at my screen’ and ‘let the pupils complete this survey in a more private manner so they don’t feel embarrassed or lie about their answers because others can see’.
Questionnaire comprehension and sensitivity
Most students interviewed for the process evaluation said that they thought the questionnaire was ‘pretty straightforward’ and ‘easy to understand’. Teachers were able to comment across a broader range of students, with one teacher (school 4) highlighting that the questionnaire was difficult for students with literacy issues:
There was a couple that we had to sit with ’cause their English isn’t great, which probably wasn’t the best environment to do it with, sitting in front of the class, ‘cause you were having to read out things that they possibly didn’t want to share in front of everybody.
School 4, contact teacher
Fieldworkers also noted that issues of literacy, English as a second language and learning support limited participation for a few students (schools 2–4).
The nature of the ‘quite personal questions’ raised concerns for some students, primarily focused on sexual behaviour questions. Concerns were also raised in relation to the SNA friendship module, in particular the fact that names of students appeared from a pre-populated class list from which respondents could select their friends. This was done to minimise errors in naming students but was perceived by students as ‘weird’:
What did you think of the questionnaire?
It was all right.
Yeah.
It was weird how you could, like, put in people’s names and then click it.
Kinda weird, yeah. And then just came up.
Yeah, and it just like came up.
Aye, just some of the questions were weird. Like, it was just kinda random. We weren’t really told what the questionnaire was about and then like you just see like all these questions, like weird. [What do you mean by weird?] Unusual, like. I wasn’t expecting it.
School 3, friends of PSs, mixed group
This sense of the unexpected was reiterated in interviews with teachers. One teacher said that some students ‘were a bit taken aback by some of the questions’, but attributed this to the fact that ‘they’ve never had that question put to them before’ and that they, nevertheless, ‘got their head down and got on with answering’ them (school 5, DHT). Another teacher commented that some students may have felt ‘timid, or a bit shy’ about the questions, but that the boys they supervised were ‘quite confident and wouldn’t be shy about those kind of things. So they filled it in . . . fine without any issues’ [school 6, contact teacher (CT)].
In the open-ended ‘additional comments’ question that concluded the questionnaire, there were 15 positive responses, mostly brief comments on having enjoyed the experience, such as ‘I enjoyed this’, ‘it was good’ and ‘it was interesting’. Negative comments were more numerous. Eleven comments were general in nature (e.g. ‘pointless’ and ‘weird’). Thirty comments expressed discomfort with the personal nature of the questions, for example ‘This is none of your business’, ‘It’s very personal’ and ‘. . . some questions are uncomfortable to answer’. Five comments were made relating to the questionnaire being insufficiently inclusive, noting for example the equivalence of ‘penis in a vagina’ with intercourse and a lack of options for those identifying as asexual. Five comments expressed concern about the inputting of postcodes (for calculation of the SIMD category) and friend names, querying whether or not the questionnaire could really be anonymous. Six students commented that the questionnaire was too long or that they needed more time to complete it. Ten queries or suggestions were made that were specific to questions (e.g. more ‘not relevant’ options or use of simpler language).
Fieldworkers reported some of the common queries they received. These included requests for meaning of some words (optimistic, self-esteem), queries about why they were being asked to give their postcode and some confusion about the question on data linkage.
Response rates at control, baseline and follow-up
Table 5 outlines the response rate for the control group, intervention group baseline and intervention group follow-up.
| School | Response rate, n/N (%) | ||
|---|---|---|---|
| Control | Intervention, time point | ||
| Baseline | Follow-up | ||
| 1 | 141/190 (74) | 147/198 (74) | 127/180 (71) |
| 2 | 112/129 (87) | 95/104 (91) | 88/101 (90) |
| 3 | 162/187 (87) | 175/193 (91) | 140/174 (80) |
| 4 | 41/55 (75) | 33/59 (55) | 23/48 (48) |
| 5 | 129/155 (83) | 124/145 (86) | 115/127 (91) |
| 6 | 111/148 (75) | 106/132 (80) | 107/114 (94) |
| Overall | 696/864 (80) | 680/831 (82) | 603/744 (79) |
In five schools, student response rates of approximately 80% at baseline and follow-up (green target > 70%).
The target response rate was met with ease in all but one school (school 4). This school differed from the other schools in being much smaller, with the highest proportion of students eligible for FSM.
It became apparent that class lists (which provided the denominator) were not always up to date, as they were often received a few weeks into the school term. This meant that a school leaver might appear on the class list and a new student might be missing. Contact teachers explained that there are students who appear on class lists, but do not attend school on a regular basis, either because of truancy or because they are engaged with other local authority education or social services. Comparing Tables 4 and 5, it is notable that the three schools with indices indicative of higher socioeconomic deprivation tended to have response rates below the average across schools. This pattern is possibly explained by a higher proportion of non-attenders in these schools.
Loss to follow-up in intervention group: differences in intervention students who did and did not complete the follow-up questionnaire
Across all schools, 81.2% of students completing the baseline survey also completed the follow-up. Six parents opted for their child to leave the study (three in the control group and three in the intervention group) and three students declined to complete the questionnaire.
Table 6 shows differences in sociodemographic and educational profile, and sexual experience between students who did and did not complete the follow-up survey. As only three students opted out of the survey, completion at both time points primarily reflects the extent to which students were in attendance and available to complete the questionnaire. Young women were more likely to complete the follow-up questionnaire than young men. Students from lower socioeconomic backgrounds were less likely to complete the follow-up questionnaire and this was evident for all measures of socioeconomic status: SIMD, FSM eligibility and home ownership. Educational attainment also differed between the groups. Those followed up were more likely to be doing National 5 qualifications (Scottish equivalent of English General Certificate of Secondary Education) than a mix of National 5 and lower-level qualifications, or just lower-level qualifications. They were also less likely to be leaving school early [in Scotland students have the option to leave in S4 after they reach 16 years, or at the end of secondary 5 (S5) or secondary 6 (S6)].
| Baseline characteristic | All | Completed follow-up | Did not complete follow-up | |
|---|---|---|---|---|
| Gender | Nobs (Nmiss) | 677 (3) | 549 (3) | 128 (0) |
| Male, n (%) | 296 (43.7) | 225 (41.0) | 71 (55.5) | |
| Female, n (%) | 369 (54.5) | 313 (57.0) | 56 (43.8) | |
| Transgender/non-binary/other, n (%) | 12 (1.8) | 11 (2.0) | 1 (0.8) | |
| SIMD | Nobs (Nmiss) | 449 (33) | 368 (7) | 81 (2) |
| Quintile 1 (most deprived), n (%) | 71 (15.8) | 46 (12.5) | 25 (30.9) | |
| Quintile 2, n (%) | 95 (21.2) | 78 (21.2) | 17 (21.0) | |
| Quintile 3, n (%) | 73 (16.3) | 60 (16.3) | 13 (16) | |
| Quintile 4, n (%) | 83 (18.5) | 70 (19.0) | 13 (16) | |
| Quintile 5 (least deprived), n (%) | 127 (28.3) | 114 (31.0) | 13 (16) | |
| FSM | Nobs (Nmiss) | 675 (5) | 548 (4) | 127 (1) |
| No, n (%) | 588 (87.1) | 492 (89.8) | 96 (75.6) | |
| Yes, n (%) | 87 (12.9) | 56 (10.2) | 31 (24.4) | |
| Type of residence | Nobs (Nmiss) | 675 (5) | 547 (5) | 128 (0) |
| House/flat owned by family, n (%) | 447 (66.2) | 390 (71.3) | 57 (44.5) | |
| Other, n (%) | 228 (33.8) | 157 (28.7) | 71 (55.5) | |
| Number of examinations in S4 (categories)a | Nobs (Nmiss) | 608 (1) | 500 (0) | 108 (1) |
| National 5 only, n (%) | 413 (67.9) | 365 (73) | 48 (44.4) | |
| National 4 only, or National 4 and National 5, n (%) | 195 (32.1) | 135 (27) | 60 (55.6) | |
| Age (years) | Nobs (Nmiss) | 673 (7) | 545 (7) | 128 (0) |
| Mean (SD) | 15.3 (0.5) | 15.3 (0.5) | 15.3 (0.4) | |
| Median (Q1, Q3) [range] | 15.3 (15.0, 15.6) [14.6–18.7] | 15.3 (15.0, 15.6) [14.6–18.7] | 15.2 (15.0, 15.5) [14.7–17.8] | |
| Intention to leave school | Nobs (Nmiss) | 678 (2) | 550 (2) | 128 (0) |
| End of S4/Christmas S5/end of S5, n (%) | 151 (22.3) | 95 (17.3) | 56 (43.8) | |
| End of S6, n (%) | 427 (63.0) | 374 (68.0) | 53 (41.4) | |
| Do not know, n (%) | 100 (14.7) | 81 (14.7) | 19 (14.8) | |
| Religiosity | Nobs (Nmiss) | 668 (12) | 542 (10) | 126 (2) |
| Very/quite important, n (%) | 100 (15.0) | 79 (14.6) | 21 (16.7) | |
| Not very/not at all important, n (%) | 568 (85.0) | 463 (85.4) | 105 (83.3) | |
| Ethnicity | Nobs (Nmiss) | 676 (4) | 548 (4) | 128 (0) |
| White Scottish/British, n (%) | 611 (90.4) | 497 (90.7) | 114 (89.1) | |
| White, but not Scottish/British, n (%) | 24 (3.6) | 21 (3.8) | 3 (2.3) | |
| Asian, n (%) | 17 (2.5) | 14 (2.6) | 3 (2.3) | |
| African/Caribbean/black, n (%) | 10 (1.5) | 6 (1.1) | 4 (3.1) | |
| Other/mixed, n (%) | 14 (2.1) | 10 (1.8) | 4 (3.1) | |
| Identity | Nobs (Nmiss) | 674 (6) | 546 (6) | 128 (0) |
| Heterosexual/straight, n (%) | 597 (88.6) | 486 (89.0) | 111 (86.7) | |
| Gay or lesbian, n (%) | 16 (2.4) | 14 (2.6) | 2 (1.6) | |
| Bisexual, n (%) | 34 (5.0) | 24 (4.4) | 10 (7.8) | |
| Other, n (%) | 11 (1.6) | 9 (1.6) | 2 (1.6) | |
| Rather not say, n (%) | 16 (2.4) | 13 (2.4) | 3 (2.3) | |
| Ever experienced oral sex? | Nobs (Nmiss) | 643 (37) | 523 (29) | 120 (8) |
| Yes, n (%) | 134 (20.8) | 95 (18.2) | 39 (32.5) | |
| No, n (%) | 509 (79.2) | 428 (81.8) | 81 (67.5) | |
| Ever experienced vaginal sex? | Nobs (Nmiss) | 638 (42) | 519 (33) | 119 (9) |
| Yes, n (%) | 98 (15.4) | 62 (11.9) | 36 (30.3) | |
| No, n (%) | 540 (84.6) | 457 (88.1) | 83 (69.7) | |
There were also differences in sexual experience between those who did and did not complete follow-up. Students who did not complete follow-up were more likely to have experienced both oral sex and vaginal sex at baseline than those who were followed up.
Sample characteristics of intervention, control and follow-up groups
Table 7 shows the baseline characteristics of the sample, split by study group. The primary comparison of interest is between follow-up and control, as these are the study groups that we mainly wish to compare. There was an imbalance in gender: a higher proportion of female students in the follow-up group than in the control group. There were no marked differences between the follow-up group and the control group for any other baseline characteristics.
| Baseline characteristic | Baseline | Follow-up | Control | |
|---|---|---|---|---|
| Age | Nobs (Nmiss) | 673 (7) | 600 (11) | 686 (10) |
| Mean (SD) | 15.3 (0.5) | 15.9 (0.5) | 15.8 (0.4) | |
| Median (Q1, Q3) [range] | 15.3 (15.0, 15.6) [14.6–18.7] | 15.8 (15.6, 16.1) [15.1–19.2] | 15.8 (15.5, 16.0) [14.2–18.2] | |
| Gender | Nobs (Nmiss) | 677 (3) | 607 (4) | 691 (5) |
| Male, n (%) | 296 (43.7) | 247 (40.7) | 346 (50.1) | |
| Female, n (%) | 369 (54.5) | 342 (56.3) | 335 (48.5) | |
| Transgender/non-binary/other, n (%) | 12 (1.8) | 18 (3.0) | 10 (1.4) | |
| SIMD | Nobs (Nmiss) | 449 (9) | 393 (14) | 457 (8) |
| Quintile 1 (most deprived), n (%) | 71 (15.8) | 67 (17.0) | 76 (16.6) | |
| Quintile 2, n (%) | 95 (21.2) | 78 (19.8) | 92 (20.1) | |
| Quintile 3, n (%) | 73 (16.3) | 66 (16.8) | 62 (13.7) | |
| Quintile 4, n (%) | 83 (18.5) | 76 (19.3) | 76 (16.6) | |
| Quintile 5 (least deprived), n (%) | 127 (28.3) | 106 (27.0) | 151 (33.0) | |
| FSM eligibility | Nobs (Nmiss) | 675 (5) | 602 (9) | 687 (9) |
| No, n (%) | 588 (87.1) | 531 (88.2) | 603 (87.8) | |
| Yes, n (%) | 87 (12.9) | 71 (11.8) | 84 (12.2) | |
| Type of residence | Nobs (Nmiss) | 675 (5) | 605 (6) | 690 (6) |
| House/flat owned by family, n (%) | 447 (66.2) | 421 (69.6) | 464 (67.2) | |
| Other, n (%) | 228 (33.8) | 184 (30.4) | 226 (32.8) | |
| Number of examinations in S4 (categories) | Nobs (Nmiss) | 608 (1) | 570 (7) | 639 (8) |
| National 5 only, n (%) | 413 (67.9) | 360 (63.2) | 361 (56.5) | |
| National 4 only, or National 4 and National 5, n (%) | 195 (32.1) | 210 (36.8) | 278 (43.5) | |
| Religiosity | Nobs (Nmiss) | 668 (12) | 605 (6) | 681 (15) |
| Very/quite important, n (%) | 100 (15.0) | 97 (16.0) | 95 (14.0) | |
| Not very/not at all important, n (%) | 568 (85.0) | 508 (84.0) | 586 (86.0) | |
| Ethnicity | Nobs (Nmiss) | 676 (4) | 605 (6) | 688 (8) |
| White Scottish/British, n (%) | 611 (90.4) | 547 (90.4) | 608 (88.4) | |
| White, but not Scottish/British, n (%) | 24 (3.6) | 20 (3.3) | 26 (3.8) | |
| Asian, n (%) | 17 (2.5) | 18 (3.0) | 27 (3.9) | |
| African/Caribbean/black, n (%) | 10 (1.5) | 9 (1.5) | 12 (1.7) | |
| Other/mixed, n (%) | 14 (2.1) | 11 (1.8) | 15 (2.2) | |
| Sexual identity | Nobs (Nmiss) | 674 (6) | 598 (13) | 674 (22) |
| Heterosexual/straight, n (%) | 597 (88.6) | 527 (88.1) | 600 (89.0) | |
| Gay or lesbian, n (%) | 16 (2.4) | 15 (2.5) | 19 (2.8) | |
| Bisexual, n (%) | 34 (5.0) | 31 (5.2) | 39 (5.8) | |
| Other, n (%) | 11 (1.6) | 25 (4.2) | 16 (2.4) | |
| Rather not say, n (%) | 16 (2.4) | 0 (0.0) | 0 (0.0) | |
Chapter 5 STASH study intervention feasibility and acceptability
This chapter assesses the acceptability of the STASH study to students, teachers and parents, including whether or not the relevant trial progression criteria were met. We defined acceptability as the degree to which the participants deemed the STASH study intervention ‘appropriate, based on anticipated or experienced cognitive and emotional responses to the intervention’. 119 We also measured uptake and completion of the PS role as a more objective measure of acceptability. 119
We draw on data from structured observations, semistructured interviews with students and staff, PS training evaluations, the PS online questionnaire, activity observations, the project monitoring log and the follow-up questionnaire (see Chapter 3 and Report Supplementary Material 4). Differences by school or by gender are highlighted when relevant.
Significantly, in terms of feasibility and acceptability, no harms (as defined in Chapter 3) were reported in the course of the study.
Acceptability of the STASH study to peer supporters
Recruitment and retention of peer supporters
Students receiving the most nominations from their peers (roughly the top 25% of year group, stratified by gender) were invited to the STASH study recruitment meeting (see Chapter 2). Across schools, an average of 87% of those nominated attended the meeting and 52% of those nominated (63% of those attending the meeting) were trained. Of those trained, 97% fulfilled the requirements of the role, defined as posting three or more STASH study messages on Facebook or having two or more face-to-face conversations about the STASH study, and attending two or more follow-up sessions (Table 8). In relation to progression criterion 1, > 50% of nominees were trained in only three of the six schools, so the green and amber targets were not reached. However, 97% of trained PSs fulfilled the role – 100% of those trained in four of six schools – meaning that the green target for progression criterion 2(a) was far surpassed.
| School | Total nominees, n (% of year) | Nominees attending recruitment meeting (%) | Nominated students trained as PS, n (% of year) | Trained PSs who fulfilled role (%) |
|---|---|---|---|---|
| 1 | 45 (23) | 71 | 58 (13) | 96 |
| 2 | 29 (28) | 90 | 45 (13) | 100 |
| 3 | 42 (22) | 79 | 45 (10) | 100 |
| 4 | 16 (27) | 100 | 56 (15) | 100 |
| 5 | 35 (24) | 83 | 77 (18) | 85 |
| 6 | 30 (23) | 97 | 33 (8) | 100 |
| Average | 33 (25) | 87 | 52 (13) | 97 (n = 99) |
In three of six schools, > 50% of nominees were recruited and trained (amber target > 50% in four schools).
Progression criterion 2a: green target achievedIn four of six schools, 100% of trained PSs completed the role (green target > 60% in four schools).
As progression criterion 1 was not met, we did a sensitivity check to see if students accepting the role differed from those who did not, in terms of the number of nominations they received. We found that students accepting and completing the role received 15.6 nominations from their peers, whereas those who did not take up the role received an average of 13.5 nominations. This suggests that students receiving more nominations were slightly more likely to take up the role and means that had we invited the top 21% (as opposed to the top 25%), we may have performed better on this progression criterion.
Role uptake and completion was slightly higher among young women. There were slightly more young men at the recruitment meeting (52.4%), but slightly more young women trained (54.8% young women, 104 students) and completing the role (56.6% young women, 99 students). In terms of acceptability across schools, observational and project monitoring data suggested that variation primarily reflected differences in levels of school support and buy-in to the intervention (e.g. HT presence at recruitment meeting, provision to students of clear information about where and when recruitment meetings would take place). There were small differences in engagement by gender, with slightly more young women than young men reporting all the key PS activities.
Motivation to participate
The most commonly cited reasons for attending training (student evaluation form, n = 104) were curiosity (27%), benefit to CV (21%) and fun (19%). The main reasons for remaining engaged throughout the intervention (PS questionnaire, n = 88) were learning useful information (44%) and viewing the project as fun (34%). These motivations were echoed in interviews, for example ‘I thought it’d be good to learn about it as well, but it’d also be quite fun’ (school 4, PS boy). In one group interview, PSs suggested that some students ‘went for the free food but . . . then everybody, I think, enjoyed it, like, so it was an experience’ (school 5, PS girl, mixed group).
When asked why they thought that some friends had decided not to take up the role, PSs cited ‘feeling uncomfortable’ and simple disorganisation and forgetting to ‘hand their letter in fast enough’ (school 4, PS boys). In terms of the latter, schools played a vital role in helping ensure that student disorganisation (e.g. in not returning parental consent forms) did not preclude participation. Particular schools were observed putting in extra effort, such as phoning parents and carers and obtaining verbal consent if a PS had forgotten their form.
Reasons for reducing involvement or withdrawal from the STASH study
Twelve PSs said that their level of involvement tailed off towards the end (PS questionnaire, 15%). The most common reasons were not wanting to miss classes (five students) and frustration with technical problems (three students). These students had nevertheless fulfilled the role’s minimum requirements. Although we were unable to obtain PS questionnaires from the five students who did not complete the role, informal conversations with PSs, trainers and teachers suggested that one felt uncomfortable with other PSs and the remainder were discouraged by timetable conflicts.
Factors associated with peer supporter engagement in the STASH study
Recruitment
Recruitment meetings consisted of one or two of the trainers hosting an information session during class time, usually in a classroom or assembly hall. Speaking with a PowerPoint® presentation (Microsoft Corporation, Redmond, WA, USA), trainers provided an overview of why students had been invited and what the project would involve. The trainers emphasised that students had been invited because they had been nominated as influential by their peers. We observed four recruitment meetings to capture student engagement. In each, there was initial curiosity, as students did not know why they were there. Engagement appeared greater in schools in which senior staff were present and encouraging attention, trainers were more confident and enthusiastic, and the group was not too large or dominated by one strong character. For example, a large and rowdy group of potential recruits in school 3 – in combination with a trainer who seemed relatively less confident in delivery of the session – created a challenging situation, which saw a relatively low training uptake (45% of attendees). In contrast, a much smaller group in a smaller school (school 4) were familiar with each other and with the trainer (the school having previously participated in ASSIST). The trainer emphasised the fun aspect of the project, students appeared to engage more readily and uptake was higher (56%). The highest uptake occurred in school 5 (77%), in which the HT attended the session and the trainer gave a highly persuasive presentation (this session was not formally observed, but was witnessed by a member of the research team).
The majority of students remained fairly impassive during the meetings, although there were murmurs of excitement when they were told that they were there because they had received the most nominations from their peers. The news that they would be trained to talk to their peers about sexual health appeared to elicit more reaction, with responses ranging from grimaces to giggles. Various questions were raised by PSs, including why nomination as ‘influential’ meant that they needed to learn about sexual health and whether or not they were perceived as sexually active. Trainers reassured them that this was not the case.
Peer nomination appeared to contribute to students’ willingness to participate, supporting a key assumption of our initial programme theory. Some were ‘surprised’ to have been nominated as they ‘just didn’t think many people would put [their] name down’, but were flattered ‘that [ . . . ] other people had thought of me’ (school 4, PS girl). Others were humorous in claiming that the nomination confirmed what they already suspected: ‘I wasn’t surprised . . . I’m an influential guy, you know?’ (school 6, PS boys).
Peer supporter training
The 2-day training took place at a local hotel. Each session was facilitated by at least two trainers, using a mix of plenary sessions, small group work and activities. All students who began training completed it, bar one withdrawal due to illness. Group size seemed to influence engagement, with the largest group of trainees (n = 27) proving most challenging to keep on task. Owing to the impracticalities of switching between the central horseshoe and ‘café-style’ tables, most sessions for this school had to be completed in small groups, which had an impact on focus in less interactive sessions. In interviews, the trainers suggested that a maximum of 20 students would be preferable.
An appropriate training space was also crucial. Owing to a booking problem in one venue, two smaller rooms were provided, one of which had (poor) Wi-Fi. This necessitated repeated moving between rooms which, according to observations and trainer reports, disrupted the training flow, made it challenging to maintain focus and limited website access (necessitating PSs viewing this at home).
Students reported that they enjoyed the training, citing the ‘nice environment’ the trainers created, the fact that ‘everyone was, like, getting on [and] there wasn’t any awkwardness’, balance between learning and fun and avoidance of ‘information overload’ (school 3, mixed group).
Trainer–trainee rapport was also a significant facilitator of engagement, with students valuing the trainers being ‘good at having a laugh with us’ (school 4, PS girls). School staff also noted a positive impact of this relationship and the trainers being ‘approachable’:
I thought they had a really good rapport with the kids, and they talked to them in a way they needed to talk to them to get them on board, to get them discussing.
School 6, contact teacher 1
Although school staff initially had concerns about some students disrupting the project, observations suggested that the trainers were largely able to manage any challenging personalities in a way that fostered engagement. Indeed, the trainers noted that vocal students could sometimes stimulate group interaction, suggesting that a lively character ‘here and there does help move things along’ (trainer 1).
Trainers noted a need to ‘warm up’ the group first thing each day and that, although it was initially ‘like trying to get blood out a stone’ for some groups, taking time to warm up meant ‘they became a lot better and were really quite vocal’ (trainer 1). Observational data suggested that the small group work, alongside other trainer strategies (e.g. mixing friendship groups, dynamic games, humour) maintained student engagement once established and promoted interaction across the group.
Follow-up meetings and peer supporter activities
The six in-school follow-ups took place in class time and typically comprised trainers checking in on weekly or fortnightly activity and troubleshooting, plus an interactive activity on a STASH study topic (see Chapter 2). Attendance averaged 80%, varying slightly by week and school (Figure 7). The school with highest overall attendance had the smallest group of PSs (school 6 with 10 PSs) and the lowest overall attendance came from one of the two largest groups (school 1 with 26 PSs), suggesting that smaller groups may be simply easier to manage. School support (e.g. in reminding PSs about the meetings) appeared another potential explanation for the variation across schools.
FIGURE 7.
Peer supporter attendance at follow-up sessions. FU, follow-up.
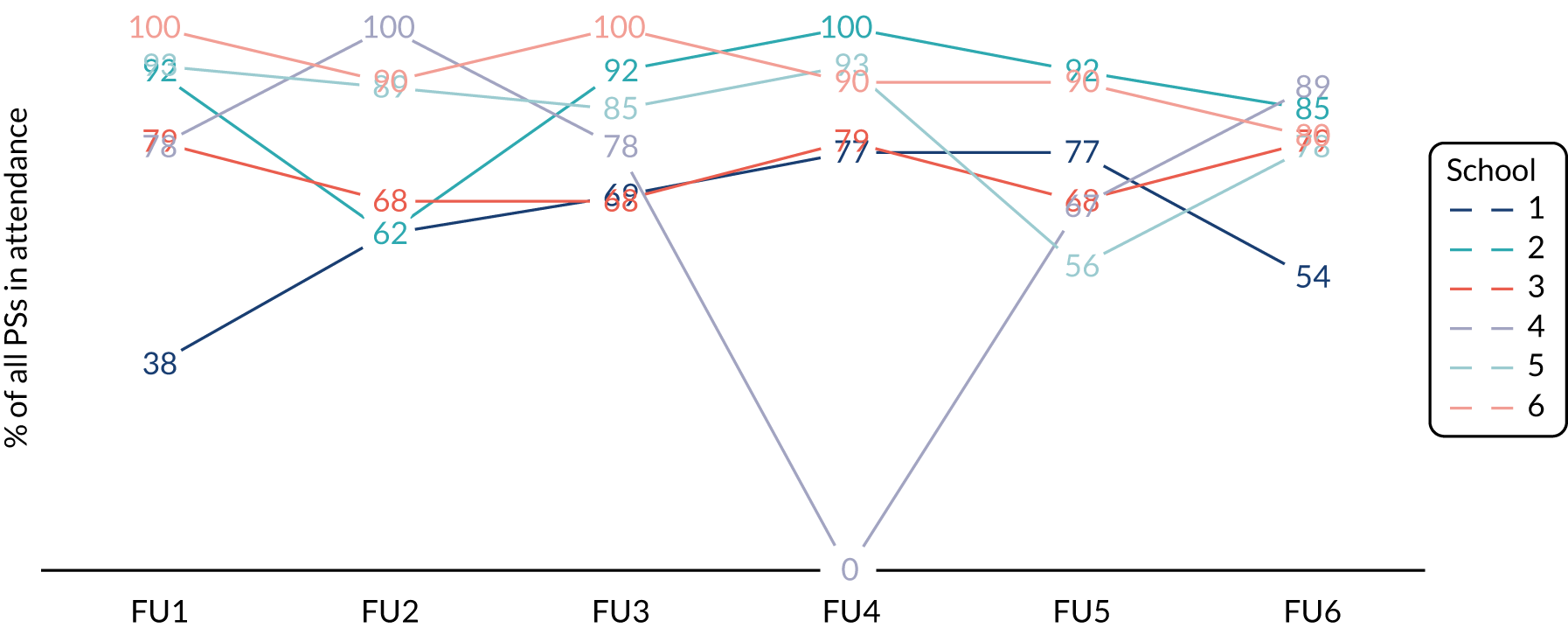
Most PSs found follow-ups ‘quite good’, worth missing classes for, useful as a reminder of their role and a top-up for key information:
It was a good refresh, ‘cause if we hadn’t had the follow ups then we [. . .] would’ve forgotten quite a lot and not know as much.
School 3, PS boy, mixed group
However, some felt that they were less interesting than the training, possibly affecting attendance:
I think everybody would be more involved if there was more activities at the follow-ups. [. . .] I think that’s maybe why people haven’t turned up so much ‘cause it’s . . . not as interactive.
School 5, PS girl, mixed group
In designing the feasibility study, we deliberately set follow-ups either weekly or fortnightly to explore any difference this might make. This was originally for three schools apiece, but changed to four schools weekly and two fortnightly when some sessions were rearranged at one school’s request. Qualitative and monitoring data suggested that students were satisfied with either follow-up, that regular spacing and reminders were important and that sufficient time between follow-ups also facilitated engagement, giving PSs time to share messages:
It was all so much more information and [. . .] it was always spread out so we had enough time to post things.
School 4, PS girl
A practical consideration related to the use of Facebook by trainers to communicate reminders to PSs. A lack of scheduling clarity – particularly for Facebook non-users and when schools had requested timetable amendments – had an impact on attendance. Some students did not know when follow-up sessions were or only found out at the last minute, particularly in school 3, which had the lowest proportion of Facebook users (and relatively low follow-up attendance).
Observational data also highlighted a range in trainers’ ability to maintain engagement and rapport, including using students’ names and apparent familiarity with session materials, which led to some variation in what was delivered and how (see Chapter 6).
In schools 5 and 6, PSs suggested that conflict with popular examination subjects may also have contributed to attendance drop-off, particularly when follow-up sessions were scheduled repeatedly against the same academic subjects. Although timetable conflicts made it challenging to participate in follow-ups, this did not always equate to lower overall engagement. For example, a school 4 PS who reported a timetable conflict was nevertheless one of the highest engagers on Facebook and contributed significantly to the follow-up sessions that he did attend.
Extent to which peer supporters liked the role
In all six schools, > 75% of PSs liked the role (green target: 60% in four schools).
The intervention was highly acceptable to PSs, with 85% of PSs reporting in the PS questionnaire that they liked the role [94% girls, 71% boys; range across schools 75% (school 1) to 100% (schools 3 and 4)]. Progression criterion 2b was therefore met with ease.
Overall, the PSs interviewed were positive about the STASH study, with common comments including ‘it was quite a good experience’ and ‘I think we’ve been well informed’. There was a sense in interviews that the role became more comfortable as they gained skills and experience. Although they had initially expected to feel ‘awkward speaking to other people about it’, they eventually felt that ‘it wasn’t as if it was something totally new that we were talking about, so, it wasn’t really a big jump . . .’ (school 4, PS girls). Engagement was also facilitated by group cohesion, which emerged in all schools to some degree. This was typically about familiarity and a sense of a shared experience, rather than friendships with other PSs. Boys from school 6, for example, felt that if the training had been ‘with 12 total strangers it wouldn’t have been that good a laugh’ and that being ‘with . . . I wouldn’t say pals, but folk that you kinda get along with, then . . . you’re a wee bit more laid-back in what you say and you know that it’s not gonna offend anybody’ (school 6, PS boy).
Peer supporters described the broader benefits of their involvement in the project as including an increase in their comfort levels in discussing sex and relationship issues, the additional learning around these topics, and the information and skills – ‘mental preparation’ (school 4, PS girl) – that this provided them with for the future. PS questionnaire data supported these findings, with 86% of PSs saying that the role would benefit their CV and 94% saying learning from the STASH study would help them protect themselves in the future. Some also noted that participation in the intervention had made them ‘more sociable’ and that being a PS was a ‘good life skill’ (school 3, PS mixed group), whereas others highlighted a broad benefit of showing what information and resources are ‘out there’ (school 6, male friend), highlighting a potential contribution to young people’s online sexual health literacy.
Acceptability of time commitment
Around half of the PSs (52%) reported spending < 30 minutes per week on STASH study activities (posting Facebook messages or talking about the STASH study, excluding follow-up meetings); 29% spent 30–60 minutes and the rest spent > 1 hour (with two PSs spending > 3 hours). The majority (84%) found the amount of weekly time they spent on the STASH study to be acceptable, with 7% saying that it was too much and 9% saying that it was too little. Most (61%) reported the number of weeks they spent as a PS to be ‘just right’. There was no clear pattern in views on intervention length according to whether the PS had weekly or fortnightly follow-ups.
Acceptability of online and social media components to peer supporters
For the most part, PSs reported accessing the STASH study website at home alone (51%) or in school with others (44%). Most (84%) PSs liked how the website looked and found it easy to navigate (64%). The majority (70%) found it easy to post messages from the website to Facebook and 87% found it easy to direct friends to the website. Eight per cent (n = 7) reported that their friends had disliked the STASH study messages or website.
The use of social media use in the STASH study was broadly acceptable to PSs, once they knew that posts would be made in a closed group. This was indicated by general comments like ‘it was actually alright’ (school 6, PS girl). There were mixed views on the relative merits of social media compared with face-to-face communication. Some felt that it was ‘a good way to get across to other people in our year’ (school 4, PS girl) and that there was enough flexibility to allow them to feel comfortable about who was in their Facebook group. Others felt that the use of Facebook, specifically, had constrained the project by limiting its perceived kudos (see Chapter 6 for associated limitations to intervention reach). A benefit of using social media was that it generated interest in sex and relationships information on the internet and social media, potentially enhancing digital literacy and use of the internet as a source of advice:
. . . before STASH I wouldn’t really pay much attention to it. But now I would, after learning about it. [. . .]
It’s because we’ve been trained . . . [. . .] If I wasn’t a PS and I got a notification, I probably would read the first couple of lines and then just swipe off. [. . .] Whereas, ‘cause I’ve been told about it face to face in an actual training session, I’d probably be more likely to like read it now. Be more interested.
School 3, PS mixed group
In general, interviewees seemed to take the view that although online communication bypassed awkwardness or embarrassment, face-to-face conversations (when engaged in) allowed them to expand on or explain in more detail about the posts they had shared.
Acceptability compared with usual sex and relationships education
Peer supporters found the STASH study more relevant (71%), helpful (76%) and interesting (75%) than their usual classroom SRE. Relative advantages included depth of information, with PSs saying that ‘it was good for us to have that knowledge, ‘cause it’s not really something that’s massively spoken about in school’, beyond the basics of ‘use protection and be safe’ (school 4, PS girl). PSs also felt that it bypassed the awkwardness of classroom SRE:
I think the teachers find it quite awkward, talking about it.
Yeah. They find it more awkward than we do. [. . .] And it’s like you’re not embarrassed to ask these questions [in STASH study], because you don’t have a bunch of people from your class that you’re maybe not entirely comfortable with.
School 4, PS girls
Acceptability of the STASH study to the wider year group
Students were defined as ‘exposed’ to the STASH study if they were a PS or reported one or more of the following in the follow-up questionnaire:
-
shown the STASH study website by a PS or accessed it themselves
-
joined a Facebook group, viewed posts or followed links
-
talked to friends about the STASH study Facebook posts or talked to/asked a PS about a STASH study topic.
In this section, we focus on the 268 students (43.9% of all S4 students) who were not a PS but reported one or more of the above exposures in the follow-up questionnaire (see also Chapter 6).
Over 70% of exposed students in all six schools agreed that the STASH study was acceptable (green target: > 60% in four schools).
Across all schools, the majority of exposed students reported that the way the STASH study was run was acceptable (74.5%) and that the information provided was acceptable (78.2%). Acceptability was higher among young women than young men (76.7% vs. 70.1% for delivery and 81.5% vs. 73.2% for information, respectively). All six schools surpassed the green target of 60% for acceptability, meaning that progression criterion 3a was easily met.
Peer supporters perceived that their friends viewed the STASH study positively (87% said their friends did not get fed up with them talking about it). In interviews, friends themselves reported the delivery of the STASH study as broadly acceptable. Some friends said they grew ‘more confident talking to [the PS]’. This was partly because they observed the PS themselves growing in confidence, and partly a recognition of the training that the PS had received:
. . . it’d be weird if they just came up and started talking about that [. . .] But, now that they’ve been taught about it, it’s OK, you can listen to them a bit more, ‘cause you know that they know what they’re talking about.
School 4, female friends
In the follow-up questionnaire, among students who had seen the website, 89% agreed that they liked the way it looked and 79% said that they found the information useful. Of students who were members of the Facebook group, 60.2% agreed that they were happy to be. In interviews, non-PS reactions to receiving STASH study posts via Facebook ranged from openness and interest to indifference. A few non-PSs recalled initial surprise at seeing the early posts, but quickly remembered having been told about the STASH study and viewed the messages in that light. One student described how the posts stood out as different:
It made you read it, ‘cause you don’t really see that.
Male, non-PS
Conversely, students in one mixed-gender interview group did not find the content ‘weird’ or ‘unusual’, indicating instead that ‘[t]hey just put it in the chat an’ we talk about it’ (female non-PS, mixed-gender interview group). Other students said that the content was not of immediate interest to them because they felt that they already had sufficient knowledge, whereas others suggested that sexual health content had limited appeal compared with other content on social media. A few students who were members of multiple groups expressed frustration with the volume of post notifications.
There were mixed views from friends whether online or face-to-face interaction was preferable. Some saw the opportunity to engage online as less awkward, whereas others preferred face-to-face conversation. The majority appeared to favour a combination, given that ‘social media’s a thing that a lot of people use’ and that if ‘you all see the same post, you might end up, like, having a conversation about it’ (school 6, male friend). To the extent that non-PSs registered and responded positively to messages, it appeared important that messages were sent by someone they knew and were seen by others in the group, such that there were opportunities for discussion.
For those who viewed Facebook posts, there was an appreciation of the integration of humour with serious information, which ‘made it funny but like . . . you got the information across. So it’s like a bit of both’ (school 4, female friends).
There was a sense among some friends that Facebook was an acceptable platform for the project, but students in all groups suggested that use of additional or alternative platforms, particularly Instagram, might enhance acceptability. For some, the use of Facebook had limited their engagement, as this was not typically a platform they used.
Perhaps unsurprisingly, exposed students in the wider year group viewed the intervention less favourably than PSs, as they did not participate in key elements, such as the training. Compared with usual SRE, about half said that the STASH study was just as relevant (51.5%, with 20.8% finding it more relevant), helpful (50.2%, with 17.5% finding it more helpful) and interesting (51.6% ,with 12.4% finding it more interesting). These findings were supported in interviews with PSs’ friends. Some felt that the STASH study was ‘a bit more in-depth [. . .] than it is in school ‘cause they just cover it briefly and move onto the next thing’ (school 4, female friends), whereas others felt that the STASH study covered similar ground to school lessons, namely regarding ‘all the infections’ (school 6, male friends).
Acceptability of the trainer role
Trainers maintained a visible presence in PS Facebook groups, to offer support, monitor activity and pick up on any misinformation or inappropriate behaviour. This was explained at training and PSs were asked to add the trainer immediately on creating their groups.
Of 71 PSs who completed the PS questionnaire and said that they used Facebook for the STASH study, 59% were glad to have the trainer in their group, with girls notably more accepting of this than boys (73% vs. 36%, respectively). Forty per cent indicated that they had asked the trainer a question via Facebook and 8% said they had contacted them about something private. In interviews, PSs said that they were conscious of the trainers’ monitoring role. Although this too was viewed as acceptable, there was a sense from some that their presence may have inhibited other students from engaging, with friends who did not know the trainers, potentially ‘scared to say some things’ and choosing not to ask questions because ‘this stranger’s in the group that I don’t know’ (school 5, PS girl).
The trainer–student relationship was expected to make a key contribution as per our programme theory, and observational data suggested a broadly high level of rapport throughout. This was borne out in the interviews, in which (particularly female) PSs were very positive about the trainers and their approach:
They were really nice and like worked well with us. Like, [. . .] they were patient and . . . just . . . good.
School 3, PS girl
The trainers themselves found their role acceptable and were enthusiastic about the project. The trainers were strongly invested in the STASH study, having co-designed intervention content with the research team (see Chapter 2). They valued their ongoing role in refining and optimising, including ‘the fact that we sat down together and tweaked [the content] before we went [to the training] and after’ (trainer 1) to review the sessions. Beyond this, they were satisfied with the overall running, communication and expectations of them.
The trainers felt that their continuing presence at each school facilitated greater rapport with students and this meant that PSs felt more comfortable approaching them with queries or concerns. One trainer commented that being seen as ‘a constant’ also facilitated engagement online:
I think they just feel a sense of a connection more. [. . .] I don’t think they feel as valued if somebody’s jumped in and out [. . .] [They think] ‘So you’ve something better to do today? Well, why should I be here?’
Trainer 1
The STASH study required some degree of social media literacy of the trainers. Only one of the three trainers was fully comfortable with Facebook, and thus took on most of the online monitoring and communication. Although the trainers highlighted that monitoring high volumes of PS posts from the STASH study trainer account had been complicated, the work had played an important part in keeping PSs engaged and making them feel valued:
I think it’s about keeping on top of it, and making sure that the PS know that you’re there for them.
Trainer 3
Acceptability of the STASH study among stakeholders
No major acceptability issues were identified via the process evaluation or in general project communication with schools.
No major acceptability issues raised (green target: no major acceptability issues raised).
Progression criterion 3c: green target metOne PS (1.1%) reported that their parents were unhappy about them being a PS (green target: < 15% parents/carers unhappy).
Data on acceptability to parents and carers were collected indirectly via PSs and teachers. One student reported in the PS questionnaire that their parents or carers were unhappy about them being a PS and, therefore, easily meeting the target of < 15%. This meant that both criteria 3b and 3c were met. In interviews, four students described any direct comment from parents or carers, including queries as to why S4 students were targeted:
. . . she was just in shock, she was like, ‘why are they teaching 15-year-olds this?’
See, my mum had that [question] at first, why it is our year that was targeted. Because obviously it’s still against the law and my mum couldn’t understand why they were doing it with my year.
I think it’s kinda good that they’re targeting our [year] because it’s like we’re getting to that age . . .
School 6, PS girls
Another PS described how his mum encouraged him to participate:
My mum’s pretty much the one that told me to do it. [. . .] So then, obviously, she was asking lots about it. She thought [the website] was good, [that] it was good for like people that are younger to be able to see all this.
School 3, PS boy
Although teachers were initially concerned about how parents might react, particularly to the intervention’s social media component, none reported any actual complaints.
Peer supporters reported that their teachers were largely positive or neutral towards the STASH study. Most felt supported by the STASH study contact teacher (71%) and 46% agreed, or neither agreed nor disagreed (43%), that their teachers were happy they were a PS. There was some variation by school (Figure 8), with no students in school 6 agreeing that their teachers were happy that they were a PS (78% neither agreed nor disagreed) and a relatively high proportion in school 5 agreeing that they were. Again, this may reflect relative levels of ‘buy-in’ from schools, which (as noted earlier) was higher in school 5 and lower in school 6.
FIGURE 8.
Peer supporter views on contact teacher support and extent to which teachers were happy with them undertaking the role.
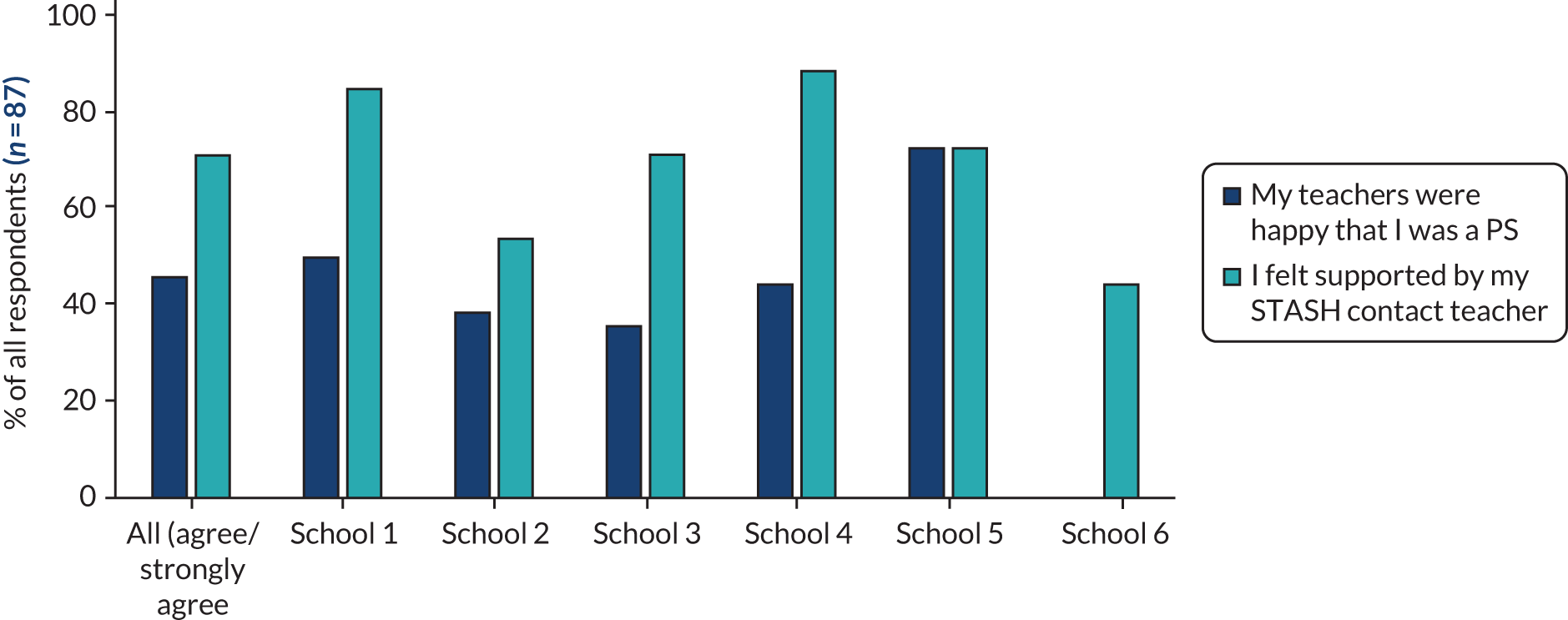
Most school staff interviewed found the intervention acceptable, particularly when they saw it as offering ‘leadership opportunities’ and when they supported the ‘ethos that [sex is] something that we’re not embarrassed to talk about’ (school 3, DHT). Common to other schools, the same DHT was positive about the trainers having ‘a really good handle on the kids’, who she believed ‘would have felt that they were respected and listened to’.
Staff, likewise, noted the significance of trainers maintaining rapport and being ‘inclusive of the group’:
. . . they definitely had the right idea. If you go too heavy with these things [. . .] then sometimes you then just create the stigma or the barrier that you’re trying to get rid of in the first place. I thought the staff dealt with that really well.
School 4, DHT
Another noted that the ‘excellent’ quality of delivery and appropriate tone of the intervention had enabled trainers to ‘get a lot of information into a short space of time’ (school 5, CT). These comments echo the evaluations of the training days, in which the various components of the training were consistently described by school staff as ‘good’ or excellent’.
Of eight staff members interviewed, only one raised any notable concerns, and these related primarily to the capacity of that school to participate in such an intervention. This school was the smallest of the six, and we included it as a ‘case study’ to capture potential issues associated with small size. The original contact teacher went on sick leave, and the senior staff member who took over had not been involved in the original decision to participate. Although perceiving the project to be well organised and flexible, this teacher had reservations about taking part in STASH, partly because the school was undergoing a significant transition. In interview, the teacher talked about a late timetable change by the school, which meant follow-up sessions clashed with an examination class and ‘created a bit of a monster’ with regard to satisfying staff and students that they would not miss important class time. He valued the fact that ‘as far as delivery [was concerned], there was no expectation on us’. However, he remained somewhat sceptical of the intervention, maintaining that participation created ‘pressures across the school because of something that, in theory, directly only impacts nine kids’ (school 4, DHT).
There was a fairly consistent view across school staff interviews that, whatever attempts might be made, S4 is a very challenging year for any additional activities to fit into and that the ‘big commitment’ required took ‘a big chunk out of their [examination subject] lessons that they then have to catch up on’ (school 6, CT 2).
Teachers who were in a position to compare the STASH study with SRE in their school (about half the sample) saw the STASH study as offering an update to materials that students had suggested were out of date. The relatively relaxed STASH study environment was also highlighted as facilitating students asking ‘sensible questions [. . .] about risk-taking behaviour’:
I wondered if they found that easier to ask those questions because it was people that they were meeting in that context, not teachers that they would . . . they certainly wouldn’t ask me those questions.
School 3, DHT
In one school, it was suggested that the STASH study content was ‘very similar’ to what the school currently delivered, which was taken as validation that they were doing something right:
There was quite a bit of crossover, which was quite nice, actually, for me to think what we’re teaching is actually still relevant to the youth of today.
School 5, CT
The school’s higher level of buy-in to the STASH study may be because the school was already invested in effective SRE.
In terms of broader impact, teachers noted the combined growth in ‘young people’s awareness about sex education’, along with the fact that the STASH study had ‘developed confidence [and] given them an opportunity to develop leadership skills’ (school 5, DHT). The benefit of improved confidence was particularly highlighted in school 5, with a contact teacher also noting ‘how articulate, vocal’ one male PS had become, as well as improvements among the girls:
Some of those skills were already there. But again, them delivering a presentation to their peers? If you’d asked them that at the start, I reckon you’d have got one, maybe two. [. . .] 10? 10! [Laughs] So yeah, clearly an important skill set that they’ve gained.
School 5, CT
Acceptability of continued participation
Despite the practical challenges noted earlier, all bar one school was keen to continue involvement in the STASH study in future years. A few (male) PS interviewees expressly said that they were unlikely to extend their involvement in the STASH study, whereas most expressed interest in continuing to share messages and, potentially, in collaborating with PSs from other schools:
Because then you could share ideas and show what you’d done and then maybe even add them to your Facebook group.
It’d be a good way to make new friends and that . . . ‘cause [. . .] you’ve got something in common.
School 6, PS girls
Post intervention, the Edinburgh & Lothians Health Foundation (which funded the intervention costs) allowed the team to use a small underspend to continue to support the PS activities. The PSs in three schools were supported by Fast Forward to set up a lesbian, gay, bisexual, transgender club, run STASH drop-in sessions, support an ongoing Healthy Respect drop in and establish links with community groups. This work continued for about 1 year after the end of the STASH intervention.
Chapter 6 Intervention fidelity, reach and exposure
This chapter presents results on the STASH study intervention fidelity, reach and exposure, and progression with criterion 1 (regarding the feasibility of implementing the STASH study). Specifically, we examined if PSs carried out intervention activities as intended (fidelity); the extent to which they and non-PSs interacted with different elements of the intervention (exposure); and the extent to which the whole year group came into contact with the intervention (reach). The exploration of fidelity, exposure and reach was designed to identify barriers to and facilitators of successful implementation, and enable us to interrogate hypothesised mechanisms of action in the STASH study programme theory (see Chapter 9).
Fidelity: did the peer supporters fulfil their role as intended?
We examined the extent to which PSs carried out the role as intended in the intervention design and as instructed at the PS training sessions. The role involved setting up ‘secret’ Facebook groups; inviting friends to join these groups; posting messages from the STASH study website; having face-to-face conversations about sexual health topics; and directing friends to the STASH study website (see Chapter 2, The STASH study intervention design for the feasibility trial). For the most part, PSs fulfilled the role as intended.
Peer supporter activity in the STASH study Facebook groups
Table 9 gives an overview of PS activity. Figures reported on the number of Facebook group members exclude the PSs who created that group and the STASH study trainer. Of 104 trained PSs, 87 used Facebook to share STASH study messages. The remaining 17 PSs used only face-to-face conversation. Facebook groups comprised an average of 12 members. Group membership remained largely stable over the intervention period (four groups gained and two lost one member). Most groups (65 of 87) were mixed gender, whereas 16 were all male and seven were all female. Seventy-five groups included non-PS friends (i.e. other S4 students from the year, hereafter ‘friends’) with an average of nine friends. This suggests good potential for messages to reach beyond the PSs.
| School | Used FB for the STASH study (%) | Average FB group members (n) | Average non-PS FB group members (n) | Posted three or more messages (%) | Average posts per PS (n) | Total posts per school (n) | Average face-to-face conversations per PS (n)a | Had three or more conversations about the STASH study (%)a |
|---|---|---|---|---|---|---|---|---|
| 1 | 96 | 20 | 12 | 95 | 16 | 388 | 4 | 80 |
| 2 | 92 | 9 | 6 | 92 | 19 | 230 | 5 | 85 |
| 3 | 42 | 6 | 4 | 29 | 7 | 78 | 12 | 100 |
| 4 | 100 | 7 | 1 | 100 | 12 | 109 | 8 | 100 |
| 5 | 89 | 15 | 9 | 70 | 15 | 348 | 5 | 79 |
| 6 | 90 | 15 | 11 | 89 | 21 | 190 | 4 | 67 |
| Total/average | 84 | 12 | 7 | 77 | 15 | 1343 | 6 | 84 |
Peer supporters posted 1343 STASH study-related messages over the intervention period, averaging 15 posts per Facebook-using PS. There were 746 recorded reactions to posts – ‘likes’, comments and shares, excluding flippant or unrelated comments, and comments from the STASH study trainers – averaging nine per Facebook-using PS. The majority of PSs (77%) posted at least three messages. Relatively few (n = 15) direct messages were sent to STASH study trainers by PSs, and only two of those were sexual health specific (the majority related to technical issues).
A Facebook Analytics report (using data from the bespoke API, which allowed users to log in to the STASH study website via Facebook) indicated 146 unique visitors to the website via the API. As only 87 PSs were using Facebook to log in to the website, this suggests a number of repeat logins by PSs. PSs who logged in via Facebook made a total of 408 site visits.
Figure 9 illustrates the temporal spread of message-sharing activity by PSs who were logged into the website via the Facebook API. Activity was relatively consistent over time, with spikes particularly around follow-up sessions. The graph does not capture all posting activity, because technical problems prompted many PSs to screenshot messages and post without using the API’s copy and share function. The PS questionnaire data (n = 88) suggested that 18% had problems logging into the website (via the API) and 37% had difficulties trying to share from the website to Facebook. Although this highlights a functionality issue, and a potential barrier to full participation, it also demonstrates the capacity and willingness of PSs to adapt and get around technical issues. Most PSs (57%) disagreed that they preferred to put messages into their own words rather than use words from the STASH study website, suggesting a preference for using the provided messages, rather than creating their own.
FIGURE 9.
The STASH study website message-sharing activity (by PSs logged in via Facebook API).
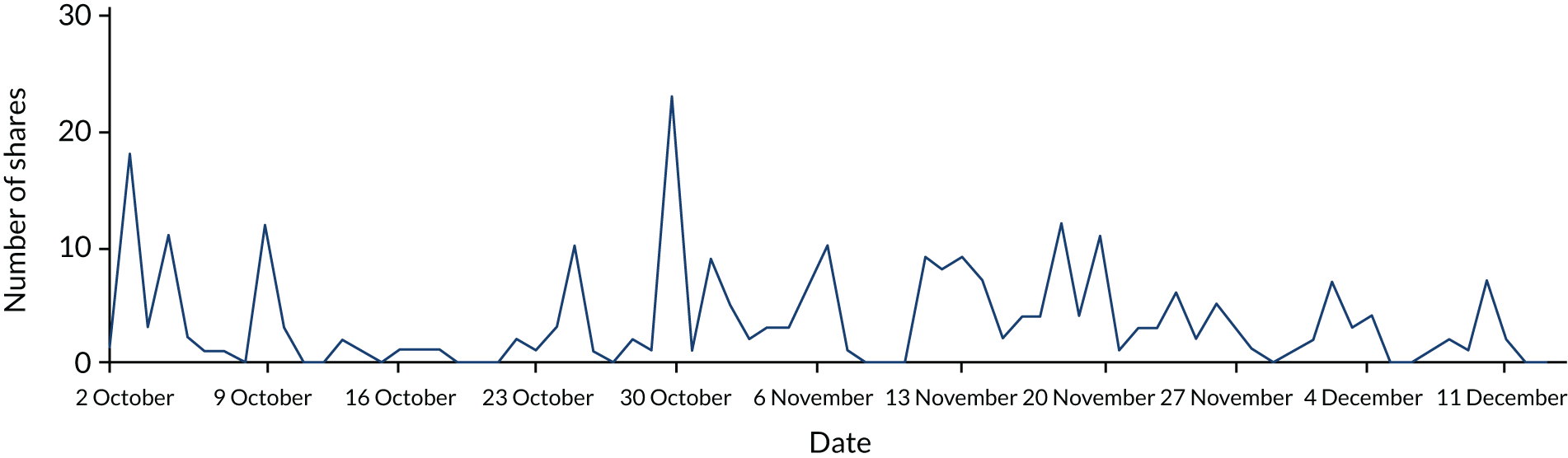
Peer supporters reported that Facebook may have served as a barrier to fidelity (and exposure). Of PSs using Facebook, 13% said that some of the people they wanted to join their group were not on Facebook (ranging from zero in school 4 to 21% in school 5) and 30% of all PS participants agreed that ‘people I wanted to join my group hardly ever use Facebook’ (ranging from zero in school 4 to 83% in school 3). This was more commonly reported by young men than young women (39% vs. 24%, respectively).
Facebook activity varied by school and by individual PS (see Table 9). For example, school 3 had the fewest PSs who primarily used Facebook (42%), but the highest average (self-reported) face-to-face conversations (12 per PS, twice the average for all schools). In interviews, PSs at school 3 said that their friends were ‘hardly using’ Facebook. Some PSs at school 3 and their friends said that they had mobile app notifications switched off, and thus were not aware of new posts. Conversely, PSs at school 4 reported relatively few face-to-face conversations, but had a higher proportion of PSs using Facebook (90%), higher Facebook group membership (including more non-PS members), more posts per PS and no PS reporting that their friends did not use Facebook. The reasons underlying variation in social media use by school were difficult to determine in this small sample, but could relate to emergent subcultures within schools, in which friendship groups go with one platform or another.
Although friends interviewed knew that the STASH study Facebook groups had been set up, and some knew that there was a website, not all said that they had engaged in-depth with the topics or messages (or were not willing to say so in a group interview context). This varied slightly among interview groups, with some friends more aware of some STASH study topics and able to discuss specific messages around, for example, ‘consent’ and ‘kinds of infections’ (school 4, female friends). These participants also noted ‘links to YouTube videos and stuff’, although typically said that they had ‘never really looked’ at these or other external links, a finding echoed elsewhere by male and female participants. We had initially expected signposting to external sources to be useful (see Chapter 2), but these data suggest that the ‘ask’ of non-PS participants (following a link from a STASH study message to an external site) might be too much. The process evaluation data confirmed that we were right to replace much of the signposting and text-heavy messages with primarily visual messages (memes, infographics), as these were more positively received, with participants noting that these stood out and ‘. . . were cheesy but alright . . .’ and ‘intrigued me more’ (school 6, friends mixed group).
Peer supporter engagement in face-to-face conversations
Most of the PS questionnaire participants (86%) said that they had talked with friends about STASH study topics, with 85% of these participants reporting at least three conversations (see Table 9). There was some variation across schools, with 100% of PSs in school 3 (low level of Facebook use) reporting at least three conversations, but only 67% of PSs reporting at least three conversations in school 6. Overall, more young women (86%) than young men (83%) reported having three or more STASH study conversations with friends. This included 76% of PSs (80% of girls, 72% of boys) who had advised a friend on where to seek help on sex and relationships.
Interviews explored in more detail how PSs engaged friends in face-to-face conversations. One PS described his conversations as follows:
[I was] just saying how they can see everything on the website, and I obviously showed them [. . .] and then it was just about, like, sexual health and keeping yourself safe in all these different situations, and not just about having sex. It was about the stuff behind it like consent and all that.
School 3, PS boy
Most friend interviewees also said that the conversations they had with a PS were quite general, about the fact that they were attending STASH study meetings and not necessarily much about STASH study topics per se:
Every now and then there was a ‘we done this, it was like this, and then this was said’ [. . .] But there wasn’t really that much [discussion].
School 6, male friend
Friends of PSs did seem aware of what the PSs had been asked to do, ‘Talking to people. If people are, like, worried about something’ and most had a general sense that the STASH study was about STIs, ‘diseases and stuff’ and ‘safer sex’, suggesting some diffusion of the STASH study messages.
Extent to which peer supporters were representative of the year group
Table 10 presents baseline characteristics (n = 680) by intervention group: trained PSs (regardless of whether or not role completed), nominees (peer nominated and invited to recruitment meeting, but did not attend training) and other students (neither nominated nor trained). In general, the nomination process identified students from higher socioeconomic backgrounds than other students, but the nominees who actually took up the role (the PSs) tended to be similar to other students on most of these indicators (specifically SIMD quintile, FSM and home ownership). Both nominees and PSs reported higher academic attainment. There was little difference in ethnicity, religiosity and sexual orientation between the three groups. The 50 : 50 gender split for nominees reflected gender stratification by the research team in selecting nominees; however, uptake of the role reflected the actual gender split of students in the year group (a preponderance of females).
| Baseline characteristic | All | PS | Nominated/invited | Other student | |
|---|---|---|---|---|---|
| Gender | Nobs (Nmiss) | 677 (3) | 97 (0) | 80 (1) | 500 (2) |
| Male, n (%) | 296 (43.7) | 41 (42.3) | 40 (50.0) | 215 (43.0) | |
| Female, n (%) | 369 (54.5) | 55 (56.7) | 39 (48.8) | 275 (55.0) | |
| Transgender/non-binary/other, n (%) | 12 (1.8) | 1 (1.0) | 1 (1.2) | 10 (2.0) | |
| SIMD | Nobs (Nmiss) | 449 (231) | 72 (25) | 59 (21) | 318 (182) |
| Quintile 1 (most deprived), n (%) | 71 (15.8) | 9 (12.5) | 4 (6.8) | 58 (18.2) | |
| Quintile 2, n (%) | 95 (21.2) | 15 (20.8) | 10 (17.0) | 70 (22.0) | |
| Quintile 3, n (%) | 73 (16.3) | 9 (12.5) | 8 (13.6) | 66 (17.6) | |
| Quintile 4, n (%) | 83 (18.5) | 18 (25.0) | 12 (20.5) | 53 (16.7) | |
| Quintile 5 (least deprived), n (%) | 127 (28.3) | 21 (29.2) | 25 (42.3) | 81 (25.5) | |
| FSM eligibility | Nobs (Nmiss) | 675 (5) | 97 (0) | 81 (0) | 497 (5) |
| No, n (%) | 588 (87.1) | 82 (84.5) | 74 (91.4) | 432 (86.9) | |
| Yes, n (%) | 87 (12.9) | 15 (15.5) | 7 (8.6) | 65 (13.1) | |
| Residence type | Nobs (Nmiss) | 675 (5) | 97 (0) | 80 (1) | 498 (4) |
| House/flat owned by family, n (%) | 447 (66.2) | 69 (71.1) | 65 (81.2) | 313 (62.9) | |
| Other, n (%) | 228 (33.8) | 28 (28.9) | 15 (18.8) | 185 (37.1) | |
| Number of examinations in S4 (categories) | Nobs (Nmiss) | 608 (1) | 94 (0) | 75 (1) | 439 (0) |
| National 5 only, n (%) | 413 (68.0) | 79 (84.0) | 63 (84.0) | 271 (61.7) | |
| National 4 only or National 4 and National 5, n (%) | 195 (32.0) | 15 (16.0) | 12 (16.0) | 168 (38.2) | |
| Religiosity | Nobs (Nmiss) | 668 (12) | 95 (2) | 81 (0) | 492 (10) |
| Very/quite important, n (%) | 100 (15.0) | 12 (12.6) | 10 (12.3) | 78 (15.9) | |
| Not very/not at all important, n (%) | 568 (85.0) | 83 (87.4) | 71 (87.7) | 414 (84.1) | |
| Ethnicity | Nobs (Nmiss) | 676 (4) | 97 (0) | 80 (1) | 499 (3) |
| White Scottish/British, n (%) | 611 (90.4) | 92 (94.8) | 74 (92.5) | 445 (89.2) | |
| White, but not Scottish/British, n (%) | 24 (3.6) | 2 (2.1) | 1 (1.2) | 21 (4.2) | |
| Asian, n (%) | 17 (2.5) | 1 (1.0) | 1 (1.2) | 15 (3.0) | |
| African/Caribbean/black, n (%) | 10 (1.5) | 2 (2.1) | 2 (2.5) | 6 (1.2) | |
| Other/mixed, n (%) | 14 (2.1) | 0 (0.0) | 2 (2.5) | 12 (2.4) | |
| Sexual identity | Nobs (Nmiss) | 674 (6) | 97 (0) | 81 (0) | 496 (6) |
| Heterosexual/straight, n (%) | 597 (88.6) | 88 (90.7) | 73 (90.1) | 436 (87.9) | |
| Gay or lesbian, n (%) | 16 (2.4) | 3 (3.1) | 3 (3.7) | 10 (2.0) | |
| Bisexual, n (%) | 34 (5.0) | 3 (3.1) | 4 (4.9) | 27 (5.4) | |
| Other, n (%) | 11 (1.6) | 0 (0.0) | 0 (0.0) | 11 (2.2) | |
| Rather not say, n (%) | 16 (2.4) | 3 (3.1) | 1 (1.2) | 12 (2.4) | |
Extent to which peer supporters reached their social network
We used SNA to evaluate the potential for diffusion of STASH study messages across the S4 year group via social network friendship ties (see Chapter 3 and Appendix 3). SNA data were generated from the ‘friendship modules’ in the baseline and follow-up questionnaires, and are distinct from friendships denoted by Facebook group membership and other PS activity. SNA friendship ties were mapped using data from all students for each of the six S4 year groups prior to the intervention.
Describing the school networks (pre intervention)
Four of the six school networks formed a single component; that is, every student in these schools had a path of ties connecting them to every other student in the network (S4 year group). Schools 4 and 6 had disconnected components, meaning that some students had no links to the rest of the year group. On average, students were separated by five or six steps (degrees of separation), with the exception of school 4, in which this average was three steps. Students averaged seven friendship ties (SD 3.8, range 1–19). This included both ingoing ties towards the node (i.e. others that had named that student as a friend) and outgoing ties from the node (friends that student had named). Network density – the proportion of actual ties from all possible ties in the network – ranged from 2% to 5%. This suggests a fairly low level of cohesion,90 although that may also reflect that students were able to name only up to six friends, and could include non-school friends in their list.
We used a stochastic actor-orientated model (see Chapter 3 and Appendix 4) to analyse change in the year group networks over time. Analysis was undertaken on students completing the friendship module at baseline and follow-up, and used data from five schools. School 4 was excluded because of a low Jaccard coefficient. This coefficient can be considered as a measure of stability: a low value means that the turnover in the network is too high to consider the data as evolving, limiting the possibility to apply RSiena (simulation investigation for empirical network analysis). For all other schools we found good values of Jaccard coefficient, ranging between 0.27 and 0.35.
Results showed that friendship ties tended to be reciprocated and two friends were likely to share the same friends. ‘Popular’ students (those most frequently named as friends) did not necessarily receive or make many more friendships over time. However, students who named more friends at baseline were more likely to add more friends at follow-up. We found that young women tended to name more friends than young men (Figure 10a) and, overall, there was a preference for same-gender friends (see Figure 10c). Level of sexual experience did not appear to be related to friendship ties (i.e. students did not tend to name friends with similar levels of sexual experience). Finally, friends were more similar at follow-up than at baseline in their assessment of STI risk with inconsistent condom use, but not in their self-assessed confidence to refuse sex without a condom.
FIGURE 10.
Gender influence in the selection of named friends. Values are log-odds (95% CI). (a) The difference in number of friends named between boys and girls; (b) the gender difference in ‘popularity’; and (c) the similarity (homophily) between friends by gender. RE, random-effects model.
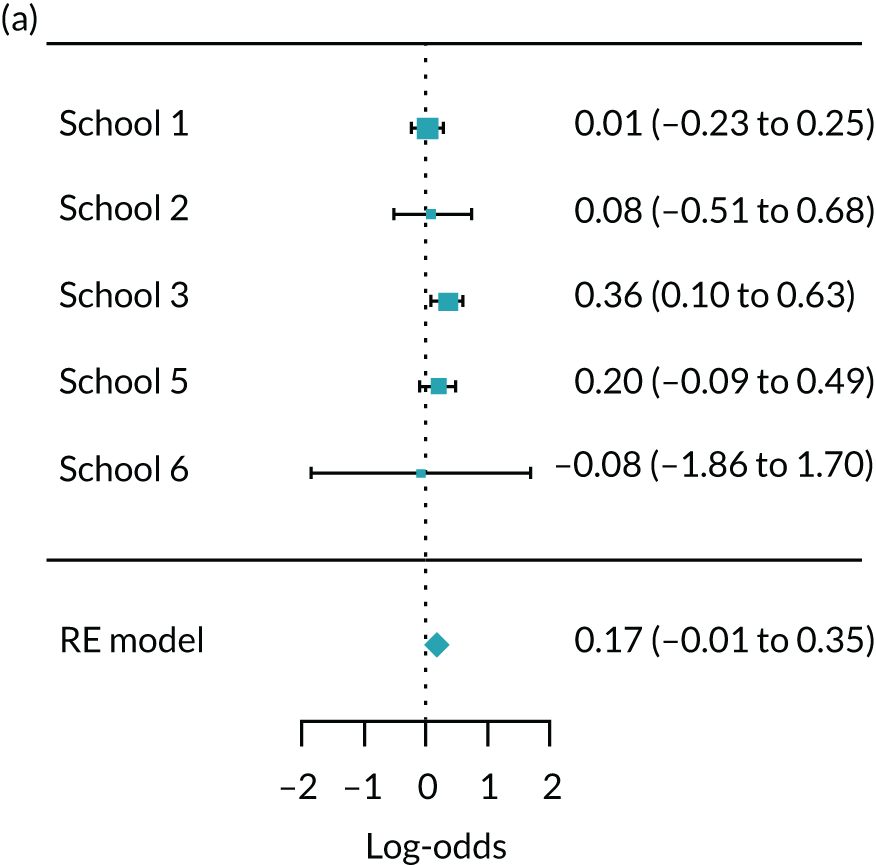

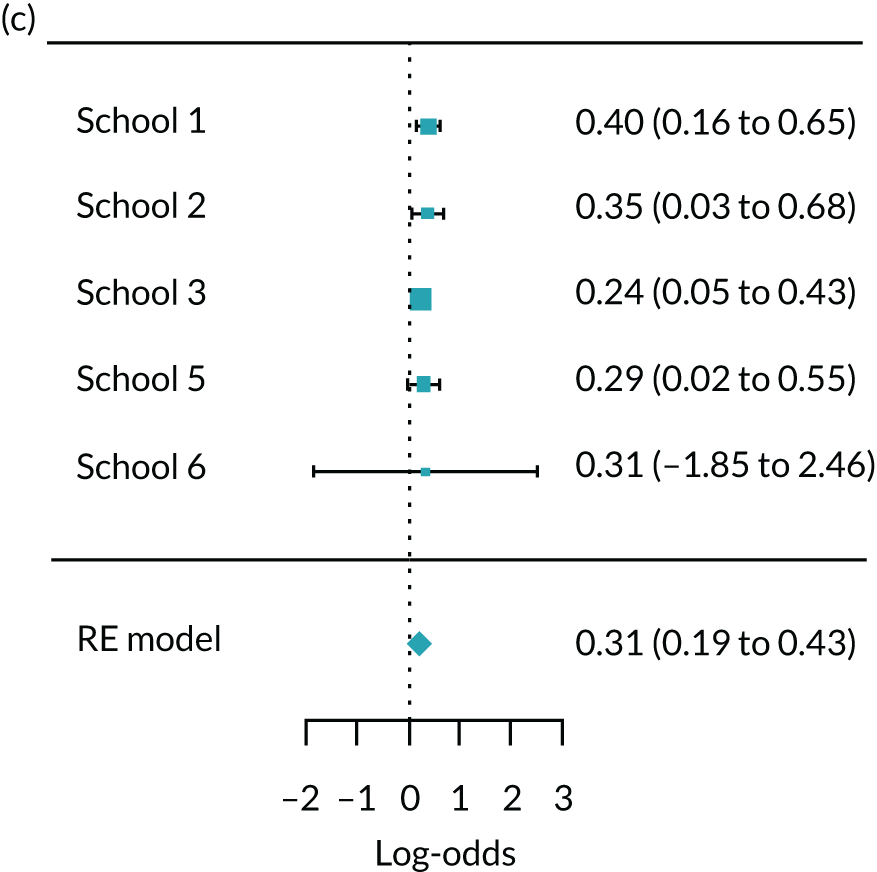
Peer supporter distribution in friendship clusters
We investigated the distribution of PSs across friendship clusters. The presence of clusters represents a potential barrier to message diffusion because they suggest a level of segregation that those outside the cluster can find difficult to access. Therefore, PS presence across clusters is desirable. In Figure 11, nodes (circles) represent students and links among them indicate friendship ties. Friendship clusters (identified by using the Girvan–Newman cluster detection algorithm; see Chapter 3) are highlighted in different colours and represent groups of students with many reciprocal ties (dense connections). PSs are highlighted blue. The extent to which PSs were distributed across friendship groups varied between 33% and 80%. PSs were present in one-third of subgroups in school 4, in 45% in school 6, in half of subgroups in schools 1, 5 and 3, and in the majority of subgroups in school 2. This is consistent with findings from ASSIST40 (in which PSs were present in 50–60% of clusters) and suggests that PSs had reasonable potential to reach across the network, with some variation by school.
FIGURE 11.
Peer supporter distribution in friendship subgroups by school. (a) School 1; (b) school 2; (c) school 3; (d) school 4; (e) school 5; and (f) school 6. Nodes (circles) represent students; links among them indicate friendship ties. Friendship clusters are highlighted in different colours; solid blue circles are PSs.
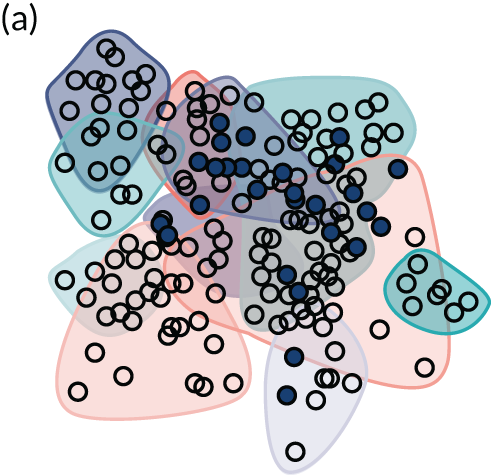
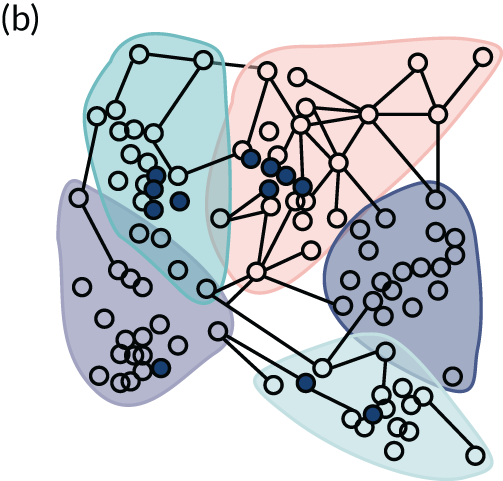
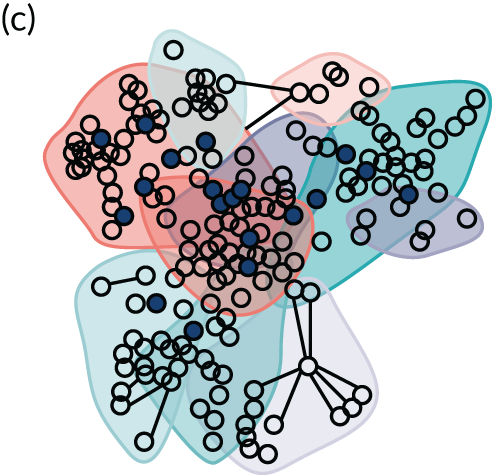
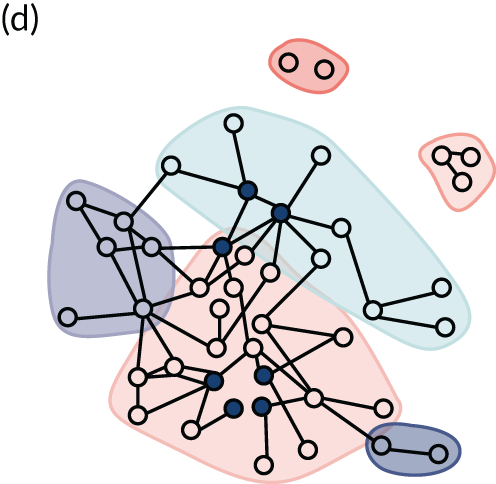
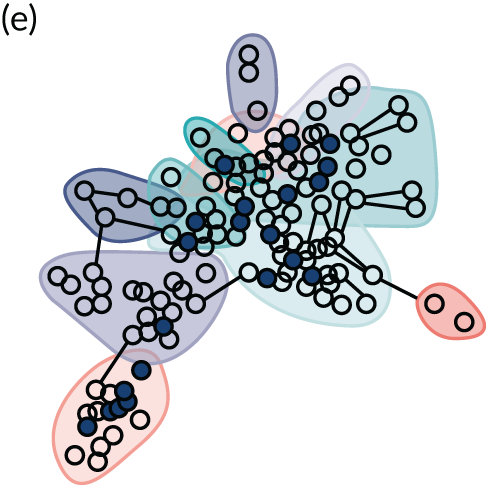
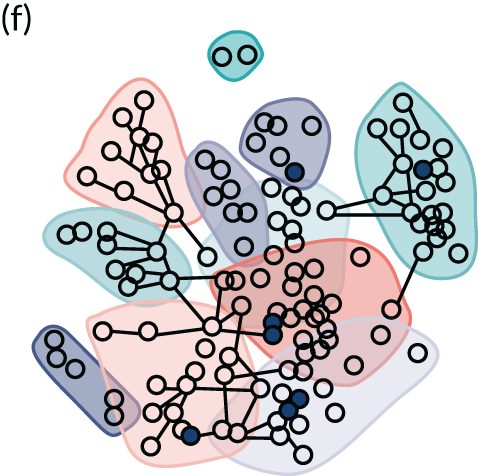
The direct reach measure indicates that, overall, one-third of students (34%, n = 302) were directly connected to a PS. Schools 1 and 3 had the largest proportion of students directly connected to a PS (52%), whereas the smallest proportion was in school 6 (7%).
Peer supporter reach by Facebook groups
We also examined PS friend connections in the STASH study Facebook groups. In Figure 12, PSs are indicated in orange and friends who were at least in one Facebook group in light blue. In schools 1 and 5, 53% of students (excluding PSs) were members of a STASH study Facebook group (n = 90 and n = 71, respectively). In school 2, 37% (n = 37) of students were linked on Facebook, whereas in school 6 this was 25% (n = 31). Few students were connected through Facebook in school 3 (9%, n = 16) and 4 (2%, n = 1). As described in Peer supporter activity in the STASH study Facebook groups, PSs in school 3 tended to use face-to-face interactions rather than Facebook. School 4 encountered additional challenges in implementing the STASH study, which seems to be reflected here in the minimal reach beyond the PS.
FIGURE 12.
Peer supporter distribution in Facebook memberships by school. (a) School 1; (b) school 2; (c) school 3; (d) school 4; (e) school 5; and (f) school 6. PSs are indicated in orange and friends who were at least in one Facebook group in light blue.
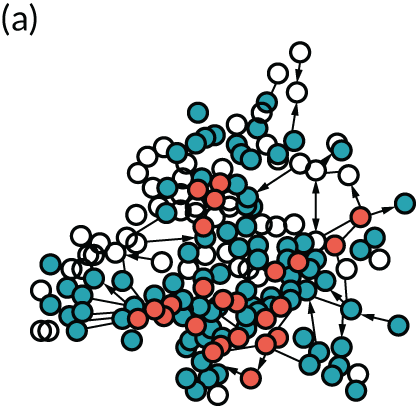
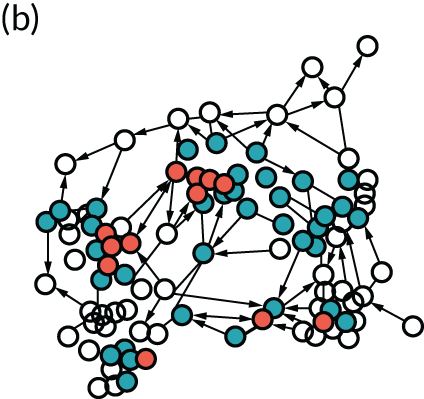
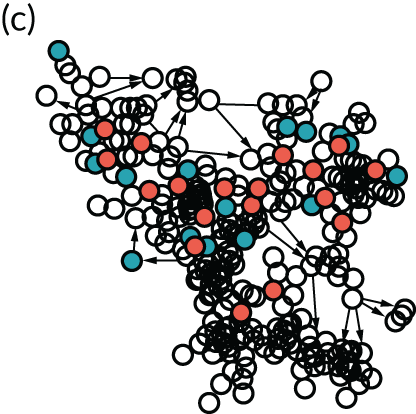
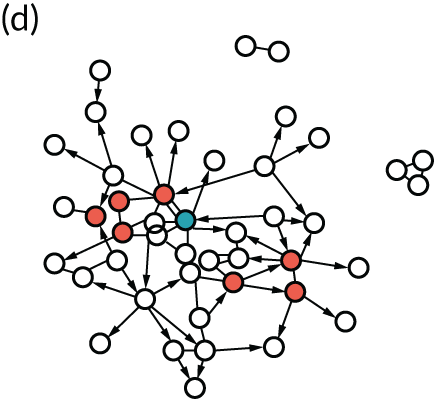
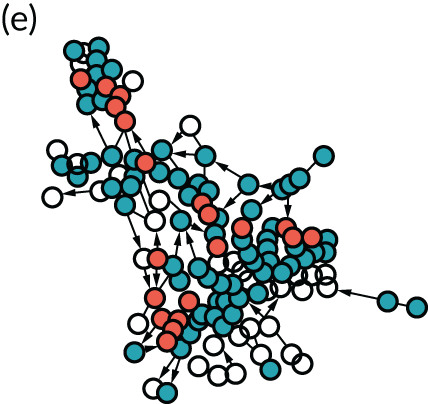
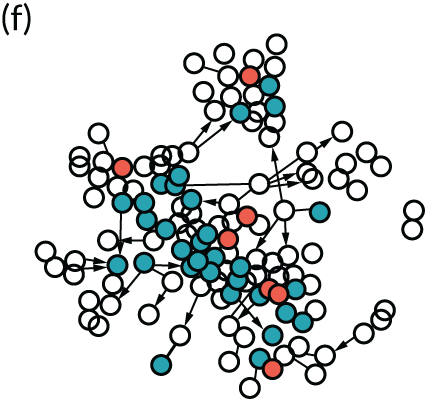
Comparison of peer supporter network position with nominees who did not take up the role and other students
Comparison with those nominated and invited, who did not take up the role
We compared the network position of students who trained as PSs with those who were nominated but declined the role. To see if there were differences in centralities between the two groups, we used the permutation-based t-test procedure in UCINET version 6.6 (Analytic Technologies, Lexington, KY, USA), a type of inferential test specifically designed for network data that are not statistically independent. The number of friendship module nominations received (indegree centrality) varied only slightly between nominees and PSs [5.3 (SD 2.4) nominations vs. 5.1 (SD 2.5) nominations, respectively], and the difference in means was not significant (p = 0.492). The two groups were also similar when taking into account the network centrality of their friends [eigenvector centrality score 0.042 (SD 0.15) for nominees and 0.045 (SD 0.17) for PSs, with a high p-value of 0.889]. The proportion of the year group that PSs could potentially reach in two steps (two-step reach centrality) ranged from 9% of students in school 1 to 60% of students in school 4. Across schools, the mean number of students reached was 27 (SD 7.9) for PSs and 24 (SD 8.6) for nominees. A two-tailed test indicates a difference of –2.737 (p = 0.03). We can therefore conclude that, on average, nominees who declined the role could potentially reach fewer students in two steps than the trained PSs. These results suggest that PSs were similar in terms of friendship ties to those who were nominated and invited but did not take up the role, except that they had better two-step reach centrality. This has implications for progression criterion 1, as it suggests that, despite a lower proportional uptake, we were able to recruit a cadre who were as well positioned (or more so) as those who did not take up the role.
Comparison of network position between peer supporters and other students
Across all schools, PSs had greater potential to reach across networks than students who were not nominated (‘other students’). The average number of incoming ties (indegree) was higher for PSs: they were named as a friend on average 5.3 times (SD 4) compared with 3.5 (SD 2.2), with a p-value of 0.0001 for the two-tailed test. We can therefore conclude that there was a difference in centrality between the two groups. Similarly, PSs had potential to reach 27% of students in two steps, whereas other students had potential to reach only 20% (p = 0.0001). However, means calculated via eigenvector centrality were no different between PSs and other students [0.04 (SD 0.17) and 0.03 (SD 0.12), respectively], with a high p-value (p = 0.1677). This suggests that there was no difference in the extent to which PSs and non-PSs were connected to ‘popular’ (well-connected) others in the network.
Participant perceptions of reach and representativeness
In terms of intervention actors viewing selection of PSs as fair and coherent,60 a perception of effective reach and representativeness of PSs by participants is important. Overall, PSs were viewed as representing a broad range of students. In interviews, PSs largely suggested that the group offered reasonable representation of their year, noting ‘It was a good mix of different groups’ and ‘pretty much every group was covered’ (school 3, PS boy). Friends of PSs suggested a similar view:
Yeah, there’s one [PS] for every friend group, if you know what I mean.
School 4, female friend
School staff concurred with this view, with both school 4 teachers, for example, noting a ‘real mixed bag of pupils’. PSs also perceived that they had potential to reach across the year (perhaps more so than was suggested by the SNA):
. . . do you think there’s anyone in your year that would be missed out?
I think our year is so small anyway that everyone’s kind of friends with everyone, so . . . [Yeah.] So, like, everyone got the information about it.
School 4, PS girls
Among friends of PSs, a perception that more students should have been ‘involved’ belied a possible lack of comprehension about the mechanism of change (PSs as conduits of messages), with possible impact on coherence of the intervention for some students:
I think if more people were, like, involved in it, it would . . .
Work better.
Like, maybe the whole year instead of just a group of them, because the more people know about it.
School 5, friends, mixed group
Potential for ‘contamination’ beyond secondary 4 groups
Sharing of STASH study messages with young people (aged > 14 years) in other schools may be regarded as a positive impact of the intervention. However, it could also represent ‘contamination’ in the context of a future trial in which intervention and control schools are in close proximity. Across all six schools, 80% of friends named in the friendship module were from S4 at that school. In five schools, the proportion of named friends from outside S4 was < 10%. The exception was school 3, in which 61% of friends were from outside S4 (a relatively high proportion, which could be explained by factors such as a greater proportion of friends in other year groups). With regard to message reach beyond intervention schools, 25% of PSs across all schools said that they had shared STASH study messages with students outside their school, ranging from 8% (school 2) to 40% (school 1). Most PSs who shared in this way did so once or twice. These findings indicate some potential for both influence and contamination beyond intervention schools.
Differences between exposed and unexposed students
Using data from the follow-up questionnaire, students were categorised by exposure to the STASH study intervention as follows:
-
trained PS
-
exposed non-PS student who had:
-
been shown the STASH study website by a PS or accessed it themselves
-
joined, viewed posts or followed links in a STASH study Facebook group
-
talked to friends about STASH study Facebook posts
-
talked to or asked a PS about a STASH study topic
-
-
unexposed: non-PS student who did not meet any above condition
-
unknown: non-PS student who did not complete the follow-up questionnaire (meaning exposed or unexposed status could not be assigned).
Among students for whom baseline data were available, 97 (14%) of the 677 students were trained as PSs, 241 (36%) were exposed to the intervention (non-PSs) and 224 (33%) were unexposed. A total of 118 (17%) students did not complete the follow-up questionnaire and so their exposure status was unknown.
Among students completing the follow-up questionnaire (although not necessarily the baseline), 58.1% (n = 611) of the year group reported exposure to STASH study activities (including PSs). Exposure was higher for young women (62.6%, n = 342) than for young men (53.4%, n = 247).
Sample characteristics by level of exposure to the STASH study
Table 11 shows baseline characteristics by exposure. PSs and exposed students were more likely than unexposed students to be female. There were no differences across exposure group by area deprivation (SIMD) or residence type, but PSs had higher FSM eligibility than the other two groups. There was a gradient in academic attainment, with a greater proportion of PSs studying for National 5 qualifications, followed by exposed and then unexposed students. There was little difference between exposure groups in terms of ethnicity, age, religiosity and sexual orientation. There was some suggestion of a gradient in terms of sexual experience, with PSs more likely to report sexual experience, followed by exposed and then unexposed students. This suggests that the intervention may have reached the groups for whom STASH study information was most immediately relevant.
| Baseline characteristic | PS | Exposed | Unexposed | |
|---|---|---|---|---|
| Demographic | ||||
| Gender | Nobs (Nmiss) | 97 (0) | 240 (1) | 222 (2) |
| Male, n (%) | 41 (42.3) | 87 (36.2) | 103 (46.4) | |
| Female, n (%) | 55 (56.7) | 150 (62.5) | 112 (50.5) | |
| Other, n (%) | 1 (1.0) | 3 (1.2) | 7 (3.2) | |
| SIMD | Nobs (Nmiss) | 72 (25) | 172 (68) | 144 (78) |
| Quintile 1 (most deprived), n (%) | 9 (12.5) | 25 (14.5) | 17 (11.8) | |
| Quintile 2, n (%) | 15 (20.8) | 38 (22.1) | 27 (18.7) | |
| Quintile 3, n (%) | 9 (12.5) | 33 (19.2) | 23 (15.9) | |
| Quintile 4, n (%) | 18 (25.0) | 29 (16.9) | 27 (18.7) | |
| Quintile 5 (least deprived), n (%) | 21 (29.2) | 47 (27.4) | 50 (34.7) | |
| FSM eligible | Nobs (Nmiss) | 97 (0) | 240 (1) | 221 (3) |
| No, n (%) | 82 (84.5) | 219 (91.2) | 197 (89.1) | |
| Yes, n (%) | 15 (15.5) | 21 (8.8) | 24 (10.9) | |
| Residence type | Nobs (Nmiss) | 97 (0) | 239 (2) | 221 (3) |
| House/flat owned by family, n (%) | 69 (71.1) | 168 (70.3) | 157 (71.0) | |
| Other, n (%) | 28 (27.9) | 71 (29.7) | 64 (29.0) | |
| Examination qualification level | Nobs (Nmiss) | 94 (0) | 222 (0) | 194 (0) |
| National 5 only, n (%) | 79 (84.0) | 160 (72.1) | 135 (69.6) | |
| National 4 only or National 4 and National 5, n (%) | 15 (16.0) | 62 (27.9) | 69 (30.4) | |
| Religiosity | Nobs (Nmiss) | 95 (2) | 237 (4) | 220 (4) |
| Very/quite important, n (%) | 12 (12.6) | 32 (13.5) | 35 (15.9) | |
| Not important, n (%) | 83 (87.4) | 205 (86.5) | 185 (84.1) | |
| Ethnicity | Nobs (Nmiss) | 97 (0) | 239 (2) | 222 (2) |
| White Scottish/British, n (%) | 92 (94.8) | 220 (92.1) | 195 (87.8) | |
| White, but not Scottish/British, n (%) | 2 (2.1) | 9 (3.8) | 10 (4.5) | |
| Asian, n (%) | 1 (1.0) | 5 (2.1) | 8 (3.6) | |
| African/Caribbean/black, n (%) | 2 (2.1) | 1 (0.4) | 3 (1.4) | |
| Other/mixed, n (%) | 0 (0.0) | 4 (1.7) | 6 (2.7) | |
| Sexual identity | Nobs (Nmiss) | 97 (0) | 240 (1) | 219 (5) |
| Heterosexual/straight, n (%) | 88 (90.7) | 215 (89.6) | 191 (87.2) | |
| Gay or lesbian, n (%) | 3 (3.1) | 6 (2.5) | 6 (2.7) | |
| Bisexual, n (%) | 3 (3.1) | 10 (4.2) | 12 (5.5) | |
| Other, n (%) | 3 (3.1) | 9 (3.7) | 10 (4.5) | |
| Sexual experience | Nobs (Nmiss) | 91 (6) | 242 (0) | 229 (0) |
| None, n (%) | 39 (42.8) | 115 (47.5) | 120 (52.4) | |
| Kissing/touching genitals, n (%) | 32 (35.2) | 85 (35.1) | 62 (27.1) | |
| Oral or vaginal sex, n (%) | 20 (22.0) | 42 (17.4) | 47 (20.5) | |
| Connectedness and engagement with school | ||||
| I feel close to people in the school | Nobs (Nmiss) | 97 (0) | 241 (0) | 220 (4) |
| Agree, n (%) | 80 (82.5) | 187 (77.6) | 173 (78.6) | |
| Disagree, n (%) | 17 (17.5) | 54 (22.4) | 47 (21.4) | |
| I try hard in school | Nobs (Nmiss) | 97 (0) | 240 (1) | 220 (4) |
| Agree, n (%) | 86 (88.7) | 224 (93.3) | 201 (91.4) | |
| Disagree, n (%) | 11 (11.3) | 16 (6.7) | 19 (8.6) | |
We examined student perceptions of school climate (e.g. perceived fairness, student–teacher trust, encouragement of participation) and compared across exposure groups to examine whether or not the peer nomination process selected students with a more positive perception of their school. Differences were small and seemed unlikely to be significant. In Table 11, we highlight two key measures: (1) perceived connectedness to others at school and (2) trying hard at school. Perhaps as expected, given the peer nomination process, PSs reported feeling closer to others at school than other students, but if anything they were less likely to say they tried hard at school.
Exposure to STASH study-related conversations
We examined data on students’ conversations about STASH study-related topics as a means of assessing any change between baseline and outcome that may have reflected diffusion of STASH study messages. Table 12 shows the proportion of students at baseline who reported talking about STASH study-related topics, by exposure, and the change in the proportions at follow-up. At baseline, PSs were more likely than other students to report conversations about all STASH study-related topics, and had greater increases in discussions about body and looks and STIs than other students. However, conversations about almost all of the topics increased regardless of exposure.
| Topic | PS | Exposed | Unexposed | |
|---|---|---|---|---|
| Talked to friends | Nobs (Nmiss) | 96 (1) | 239 (2) | 215 (9) |
| Your body and looks | Baseline, n (%) | 52 (54.2) | 128 (53.6) | 94 (43.7) |
| Change, % | 13.6 | 5.3 | 5.7 | |
| What makes a good or bad relationship | Baseline, n (%) | 67 (69.1) | 126 (53.2) | 98 (45.6) |
| Change, % | –2.4 | 8.3 | 5.2 | |
| Knowing if you are ready for sex | Baseline, n (%) | 35 (36.5) | 57 (24.1) | 48 (22.3) |
| Change, % | 4.6 | 5.9 | 2.7 | |
| STIs | Baseline, n (%) | 26 (27.1) | 35 (14.8) | 45 (21.0) |
| Change, % | 15.1 | 6.2 | 1.8 | |
| Sexting or pornography | Baseline, n (%) | 43 (45.3) | 67 (28.3) | 52 (24.4) |
| Change, % | –0.9 | 6.2 | 6.2 | |
Chapter 7 Development and testing of measures
This chapter describes the development and testing of intervention outcome measures. These were categorised as potential primary outcomes and potential secondary outcomes. We collected data to investigate response rates to the various question types and to assess the utility of the measures for a future trial.
Secondary outcomes are presented descriptively and, in some cases, with measures of reliability of combined question banks. The data generated by these measures are not intended as an assessment of effectiveness of the intervention, rather they provide guidance on the most useful outcomes to take forward to the definitive trial.
Group definitions
Study group was defined as:
-
baseline (study participants assessed prior to the start of the intervention)
-
follow-up (study participants assessed at the end of the intervention towards the end of the school year)
-
control (previous year’s S4, assessed towards the end of the school year).
Exposure to the STASH study intervention was predefined (for follow-up students only) as:
-
trained PS
-
exposed (i.e. a non-PS student who has been ‘exposed’ in one or more of the following ways: received at least one message via social media, had at least one conversation or visited the STASH study website).
Primary outcome measures
-
Have you ever experienced oral sex?
-
When was the most recent time you had oral sex? (Within the last 6 months or more than 6 months.)
-
In the last 3 months, how many different people have you had oral sex with?
-
And how many of them did you have oral sex with without using a condom or dental dam?
-
-
The last time you had oral sex, was a condom or dental dam used?
-
Have you ever had sexual intercourse (penis in vagina)?
-
When was the most recent time you had sexual intercourse (penis in vagina)? (Within the last 6 months or more than 6 months.)
-
How many times in the last 3 months have you had sexual intercourse (penis in vagina)?
-
In the last 3 months, how many different people have you had sexual intercourse with?
-
And with how many did you have sexual intercourse without using a condom?
-
-
How often was a condom used when you had sexual intercourse in the last 3 months? (Always, often, sometimes, never.)
-
The last time you had sexual intercourse, was a condom used? (Yes, no.)
For the full range of potential primary outcome measures from the follow-up questionnaire, see Report Supplementary Material 5.
Principal component analysis on potential primary outcomes
Principal component analysis was carried out on the full range of potential primary outcomes on follow-up and control data sets (as listed in Primary outcomes). The main items that loaded onto the first principal component were the number of different partners in the last 3 months and number of partners with whom a condom or dental dam was not used, explaining around 20% of the variability in the sample. Main items loading onto the second principal component were use of a condom at last sex and how often a condom was used in the last 3 months. These explained 18% of the variance in the sample.
The first principal component did not make good sense as a composite outcome, particularly as it was restricted to those who reported having had oral sex or vaginal sex. The second was a more sensible composite, as it contained a greater amount of information on an important outcome, condom use, but it explained < 20% of the variance in the sample.
In general, the PCA of the potential primary outcomes did not provide any strong indications of a data-driven choice of primary outcome. The results were not used further in defining the primary outcome to take forward in the definitive trial.
Descriptive statistics for primary outcomes
Table 13 presents the summary statistics for all of the potential primary outcomes, overall and for the three study groups (baseline, follow-up and control). The rates of ever having had oral or vaginal sex would be expected to increase from baseline to follow-up (due to maturation effects), but would be broadly comparable in the follow-up and control groups, as group members completed the questionnaires at approximately the same time in their school education and were the same age (see Chapter 4 and Table 7).
| Primary outcome | All | Baseline | Follow-up | Control | |
|---|---|---|---|---|---|
| Oral sex ever | Nobs (Nmiss) | 1883 (104) | 643 (37) | 573 (38) | 667 (29) |
| Yes, n (%) | 496 (26.3) | 134 (20.8) | 167 (29.1) | 195 (29.2) | |
| No, n (%) | 1387 (73.7) | 509 (79.2) | 406 (70.9) | 472 (70.8) | |
| Most recent oral sex | Nobs (Nmiss) | 489 (7) | 132 (2) | 164 (3) | 193 (2) |
| Last 6 months | 383 (78.3) | 108 (81.8) | 122 (74.4) | 153 (79.3) | |
| More than 6 months | 106 (21.7) | 24 (18.2) | 42 (25.6) | 40 (20.7) | |
| Oral sex for first time in last 6 months | Nobs (Nmiss) | 372 (11) | 103 (5) | 121 (1) | 148 (5) |
| Yes, n (%) | 135 (36.3) | 43 (41.7) | 37 (30.6) | 55 (37.2) | |
| No, n (%) | 237 (63.7) | 60 (58.3) | 84 (69.4) | 93 (62.8) | |
| Use of condom/dental dam at last oral sex | Nobs (Nmiss) | 364 (19) | 102 (6) | 118 (4) | 144 (9) |
| Yes, n (%) | 53 (14.6) | 20 (19.6) | 14 (11.9) | 19 (13.2) | |
| No, n (%) | 311 (85.4) | 82 (80.4) | 104 (88.1) | 125 (86.8) | |
| Main reason for no condom/dental dam at last oral sex | Nobs (Nmiss) | 296 (15) | 78 (4) | 102 (2) | 116 (9) |
| Got carried away and forgot, n (%) | 48 (16.2) | 15 (19.2) | 18 (17.6) | 15 (12.9) | |
| Did not have one to hand, n (%) | 67 (22.6) | 23 (29.5) | 28 (27.5) | 16 (13.8) | |
| I/my partner did not think it was necessary, n (%) | 120 (40.5) | 25 (32.1) | 40 (39.2) | 55 (47.4) | |
| I/my partner did not know how to use one, n (%) | 1 (0.3) | 0 (0.0) | 1 (1.0) | 0 (0.0) | |
| I/my partner did not want to use one, n (%) | 33 (11.1) | 9 (11.5) | 10 (9.8) | 14 (12.1) | |
| We had one but it broke, n (%) | 5 (1.7) | 0 (0.0) | 1 (1.0) | 4 (3.4) | |
| Other, n (%) | 22 (7.4) | 6 (7.7) | 4 (3.9) | 12 (10.3) | |
| Vaginal sex ever | Nobs (Nmiss) | 1868 (119) | 638 (42) | 569 (42) | 661 (35) |
| Yes, n (%) | 371 (19.9) | 98 (15.4) | 120 (21.1) | 153 (23.1) | |
| No, n (%) | 1497 (80.1) | 540 (84.6) | 449 (78.9) | 508 (76.9) | |
| Most recent vaginal sex | Nobs (Nmiss) | 369 (2) | 97 (1) | 119 (1) | 153 (0) |
| Last 6 months, n (%) | 290 (78.6) | 74 (76.3) | 94 (79.0) | 122 (79.7) | |
| More than 6 months, n (%) | 79 (21.4) | 23 (23.7) | 25 (21.0) | 31 (20.3) | |
| Vaginal sex for first time in last 6 months | Nobs (Nmiss) | 287 (3) | 73 (1) | 94 (0) | 120 (2) |
| Yes, n (%) | 100 (34.8) | 30 (41.1) | 29 (30.9) | 41 (34.2) | |
| No, n (%) | 187 (65.2) | 43 (58.9) | 65 (69.1) | 79 (65.8) | |
| Use of condom at last vaginal sex | Nobs (Nmiss) | 284 (6) | 72 (2) | 94 (0) | 118 (4) |
| Yes, n (%) | 125 (44.0) | 35 (48.6) | 38 (40.4) | 52 (44.1) | |
| No, n (%) | 159 (56.0) | 37 (51.4) | 56 (59.6) | 66 (55.9) | |
| Main reason for no condom at last sex | Nobs (Nmiss) | 147 (12) | 36 (1) | 55 (1) | 56 (10) |
| Got carried away and forgot, n (%) | 30 (20.4) | 7 (19.4) | 13 (23.6) | 10 (17.9) | |
| Did not have one to hand, n (%) | 36 (24.5) | 9 (25.0) | 15 (27.3) | 12 (21.4) | |
| I/my partner did not think it was necessary, n (%) | 18 (12.2) | 3 (8.3) | 7 (12.7) | 8 (14.3) | |
| I/my partner did not know how to use one, n (%) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| I/my partner did not want to use one, n (%) | 15 (10.2) | 3 (8.3) | 4 (7.3) | 8 (14.3) | |
| We had one but it broke, n (%) | 2 (1.4) | 1 (2.8) | 0 (0.0) | 1 (1.8) | |
| Both got tested for STIs and had another form of contraception, n (%) | 36 (24.5) | 10 (27.8) | 13 (23.6) | 13 (23.2) | |
| Other, n (%) | 10 (6.8) | 3 (8.3) | 3 (5.5) | 4 (7.1) | |
| Frequency of condom use for vaginal sex (last 3 months)? | Nobs (Nmiss) | 209 (4) | 92 (2) | 117 (2) | |
| Always, n (%) | 60 (28.7) | 28 (30.4) | 32 (27.4) | ||
| Often, n (%) | 27 (12.9) | 9 (9.8) | 18 (15.4) | ||
| Sometimes, n (%) | 40 (19.1) | 18 (19.6) | 22 (18.8) | ||
| Never, n (%) | 82 (39.2) | 37 (40.2) | 45 (38.5) | ||
| Ever anal sex? | Nobs (Nmiss) | 1217 (90) | 0 (0) | 563 (48) | 654 (42) |
| Yes, n (%) | 85 (7.0) | 0 (0) | 29 (5.2) | 56 (8.6) | |
| No, n (%) | 1132 (93.0) | 0 (0) | 534 (94.8) | 598 (91.4) | |
| Most recent anal sex?a | Nobs (Nmiss) | 82 (3) | 0 (0) | 27 (2) | 55 (1) |
| Last 6 months, n (%) | 52 (63.4) | 0 (0) | 16 (59.3) | 36 (65.5) | |
| More than 6 months, n (%) | 30 (36.6) | 0 (0) | 11 (40.7) | 19 (34.5) | |
| Always practising safe sex | Nobs (Nmiss) | 1861 (126) | 637 (43) | 566 (45) | 658 (38) |
| No, n (%) | 216 (11.6) | 48 (7.5) | 72 (12.7) | 96 (14.6) | |
| Yes, n (%) | 1645 (88.4) | 589 (92.5) | 494 (87.3) | 562 (85.4) | |
Table 13 shows that the rates of ever having had oral sex were very similar between the control and follow-up groups. A lower proportion of those in the follow-up group than of those in the control group had oral sex for the first time in the last 6 months. The rates of condom and dental dam use were similarly low in both groups, at 12–13%, with the most common reasons being that students did not think it was necessary or they did not have one to hand. Most students who had oral sex did so with only one person, rendering the measure ‘number of oral sex partners’ uninformative as an outcome.
The rate of ever having had vaginal sex was 2% lower in the follow-up group than in the control group, with an increase of just under 6% from baseline. Almost 80% of those who reported having had sex had done so in the last 6 months in both groups, the proportion having had sex for the first time in that period being slightly lower in the follow-up group (31%) than in the control group (34%). These observations suggest that the STASH study may be potentially associated with a slightly lower rate of first-time sex among S4 students. Among those who reported having had vaginal sex in the last 6 months, use of a condom at most recent sex was slightly lower in the follow-up group (40.4%) than in the control group (44.1%). The main reasons cited for not using a condom were that students did not think it was necessary, they got carried away and forgot, or they had both been tested for STIs and had another form of contraception. The follow-up group were 3% more likely to have always used a condom when they had sex in the last 3 months, although the percentage who always or often used a condom was similar across the follow-up and control groups, at around 40%. Most students who had had vaginal sex had done so with only one person.
Suitability of primary outcomes
There was much discussion between the TMG and TSC regarding the identification of a suitable primary outcome for any future evaluation. Sexual activity and condom use are clearly important outcomes, which is why they were included as indicative outcomes in this study. However, when considered separately, they provide only partial coverage of the potential impact of the intervention on safe sexual behaviour. Condom use on its own is of limited utility as it is asked only of the subset of the sample who have had sex. The TMG recommended that both dimensions of sexual behaviour (sexual activity and condom use) should contribute to the primary outcome.
A further point of discussion concerned anal sex. This was not originally included in the list of primary outcomes, but it was noted (see Table 13) that the rate of anal sex in the follow-up group was 3.4% lower than in the control group, and the follow-up students were also less likely to have had anal sex in the last 6 months. As this outcome had a low incidence, this was felt to be a considerable drop. The TMG agreed that a reduction in anal sex would be a positive outcome of the intervention, as it is the riskiest practice in terms of STIs120 and as anal sex in young people is associated with coercion. 121 The TMG, in discussion with the TSC, also agreed that oral sex should be dropped from the composite measure because it is much less risky in terms of STIs120 and there is significant resistance to condom and dam use in oral sex. 122 Our data (see Table 13) confirmed that condom and dam use is much less common for oral sex (14.6% at last occasion of oral sex vs. 44% for vaginal sex). Although messages about condom and dam use for oral sex would be retained in the future intervention, we agreed that both intervention and outcome should focus on the practices with highest risk. This supports simpler messaging, which we found key to PS role effectiveness. In addition, it focuses the intervention on outcomes with the strongest potential for improvement.
The TMG therefore agreed to take forward a composite ‘always practising safe sex’ variable to the definitive trial. This would be defined as, ‘no condomless (vaginal or anal) sex in last 6 months’.
This means that students who were not having sex would also be considered to be safe from STIs (i.e. no sex equals no risk), as would those who were having (vaginal or anal) sex but always used a condom. To ensure consistency and inclusion of both heterosexual and same-sex relationships, it was agreed that the inclusion of anal sex in the ‘safer sex’ outcome should be on the basis that it could be happening, but would always involve condom use. We did not ask students in the current study whether or not they used a condom in anal sex, only whether or not they were having anal sex at all. We also use a 3-month period for reporting condom use in vaginal sex. Therefore, the composite primary outcome variable reported in this study is ‘always practising safer sex’ but is defined as ‘no condomless vaginal sex in the last 3 months and no anal sex in the last 6 months’.
The results from the current study suggest that this composite measure is likely to have greater utility than any of the individual outcomes, as it allows inclusion of everyone in the sample, and as both delaying sex and ensuring that sex is always protected are the safest ways to avoid STIs and unplanned pregnancy. The composite primary outcome is likely to be more sensitive to change because it is measured in more people than contraception use, which is relevant only to those who are having sex. The time marker of 6 months is consistent with the individual outcomes that were measured in this study and allows assessment of the impact of the STASH study intervention, as the study could not have affected behaviour prior to its start.
Therefore, a row is included at the bottom of Table 13 to show the rates of students ‘always practising safer sex’ in the current study and this is the variable that will be taken forward to the formal primary outcome analyses. The rate of this outcome is about 2% higher in the follow-up group than in the control group.
Primary outcome by study group
The difference in the primary outcome ‘always practising safe sex’ between the follow-up and control groups was estimated using a logistic regression model, adjusting for the clustering by school. The overall OR for the rate of ‘always practising safe sex’ for follow-up compared with control students was 1.18 (95% CI 0.85 to 1.64; p = 0.33). In other words, the prevalence of safe sex was 18% higher among students in the intervention year than among students in the control year. The difference was not significant, as the study was not powered to show a difference in outcomes, but the results are suggestive of a potential positive outcome for the intervention.
As there were more young men in the control group than in the follow-up group, the model was fitted separately for males and for females. Among males, the OR was 1.07 (95% CI 0.67 to 1.73; p = 0.78), whereas among females the OR was 1.37 (95% CI 0.85 to 2.21; p = 0.20). Therefore, there was a larger impact on the safe sex practices of young women than of young men. The interaction between gender and study group was statistically non-significant (p = 0.48), again because the study was not powered to show this. The difference in magnitude of the OR was considered scientifically significant.
In our statistical analysis plan (see Report Supplementary Material 5), we proposed analysis of whether or not there were any differences in primary outcome according to exposure to the intervention (PSs, students reached by PSs and unexposed students). The subgroup sample size for all outcomes was too small to offer a reliable picture. We present the analysis in Appendix 4 for information, but suggest a high level of caution in any interpretation of the data.
Information on the proposed composite primary outcome relevant to a future sample size calculation
The ICC was estimated from models fitted to the composite primary outcome with a random effect for school and no fixed effects. Owing to the small sample size, these ICC estimates were imprecise, with wide CIs. The ICC estimated from the model including all students in the follow-up and control groups was 0.0198, whereas the individual models for the follow-up and control groups estimated the ICC as 0.0066 and 0.0332, respectively. Although set out as a study objective, we opted not to propose a sample size calculation for a definitive trial based on our estimate of the effect on primary outcome from this study. This is consistent with recent guidance,95 as (1) our estimate is highly imprecise and yet any sample size calculation would be highly sensitive to it and (2) other sources of evidence should inform the specification of a difference to detect, including the value of the effect relative to intervention cost.
Secondary outcomes
A variety of potential secondary outcomes are considered here and are summarised into particular domains, each represented by a question bank in the evaluation questionnaires.
To assess reliability of each question bank as a whole, Cronbach’s alpha was calculated (when appropriate) from the control group data and is presented for each set of questions.
Ranges of response rates are given for each question bank and by study group. These represent the proportions of students who answered each question, out of those who completed any of the questionnaire at the relevant time point (and, in some cases, would be expected to have answered the question, following a particular response to a previous question).
As mentioned above, the exploratory and descriptive analysis of these outcomes is intended to provide a guide to their utility for a future, definitive trial of the STASH study, and not as evidence of effectiveness (or lack thereof) of the intervention arising from the current feasibility study.
The data are presented without CIs and the analyses are descriptive because there was no intention or statistical power to test for differences between groups. Planned analysis by exposure was done but is not presented because the sample size was too small for reliable interpretation.
Knowledge
The knowledge questions asked in the questionnaire were as follows (with correct answers in brackets, note ‘do not know’ was considered an incorrect answer):
-
With a condom on, a guy should wait until the penis is soft before pulling out after ejaculation (false).
-
You can make an effective dental dam by cutting up a condom (true).
-
If you get chlamydia you will know because you will have symptoms (false).
-
It is against the law for two 15-year-olds to have sex with each other (true).
-
If someone aged < 16 years goes to the doctor for a STI test or pregnancy test, the doctor has to tell their parents (false).
-
All STIs can be treated with antibiotics (false).
-
A girl cannot get pregnant if the guy pulls out (withdraws) before ejaculation/cumming (false).
-
If you use a lubricant with a condom it should be oil based [e.g. Vaseline® (Unilever UK Limited, Surrey, UK), massage oil] (false).
-
A girl’s clitoris is inside the vagina (false).
The ‘where to go’ knowledge questions were as follows:
-
where to get free condoms
-
where to get emergency contraception
-
where to get free contraception
-
where to get advice on sex.
The Cronbach alpha of the knowledge question bank as a whole was 0.70, whereas for the ‘where to go’ question bank it was 0.86.
Study group
The response rates to the knowledge questions were similar across the study groups, ranging from 90% to 98% at baseline, from 88% to 96% at follow-up and from 91% to 97% among the control students.
Figure 13 shows the percentage of the control and follow-up groups with the correct answer for each of the knowledge questions listed above. Lines between control and follow-up group are drawn for ease of comparison and do not indicate change over time. The graphs show that knowledge was generally higher in the follow-up group for both knowledge and knowing where to go for contraception and advice. Of particular note is knowledge question 2, which 8% of control students answered correctly, compared with 25% of follow-up students, and knowledge question 5, which 51% of control students answered correctly, compared with 64% of follow-up students. Both of these relate to key intervention messages. Correct responses to question 4 showed a decrease from the control group (72% correct) to the follow-up group (66%), which may have been due to some confusion around the term ‘sex’. Specifically, PSs were trained to think more broadly about what counts as sex (i.e. it is not just vaginal intercourse) and this may have led to confusion about which types of sex were against the law. This will be addressed in the terminology used for sex in the definitive trial questionnaire.
FIGURE 13.
Rates of correct answers to (a) knowledge and (b) ‘where to go’ questions for the control and follow-up groups. Lines are drawn for ease of comparison and do not indicate change over time, each line represents an individual question.
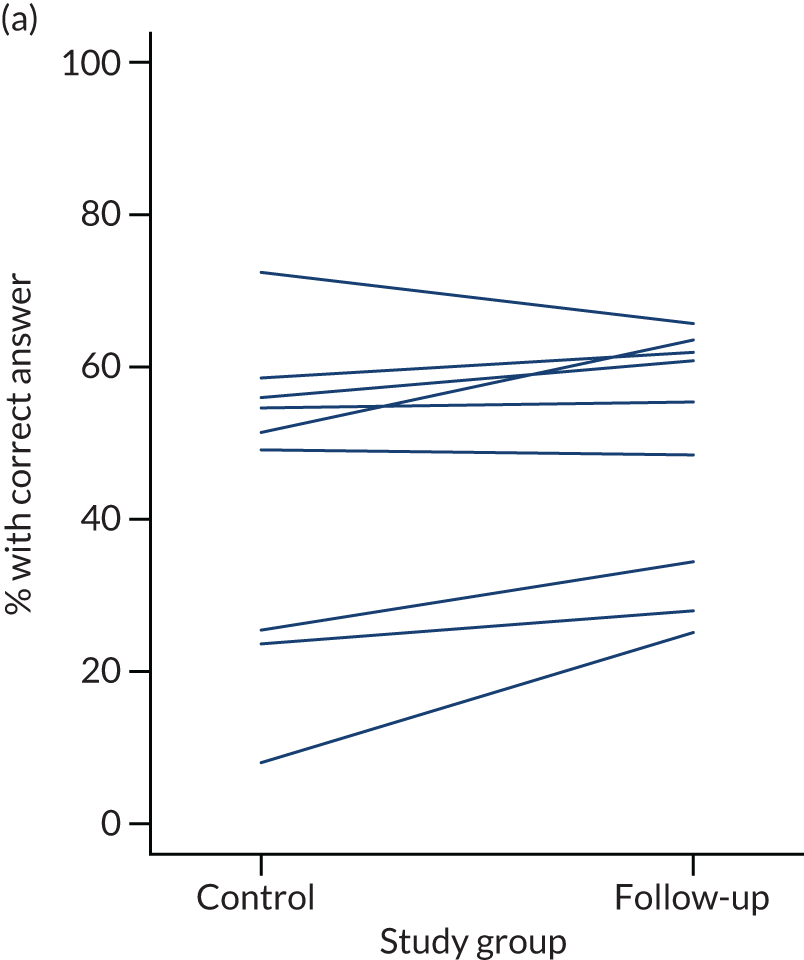
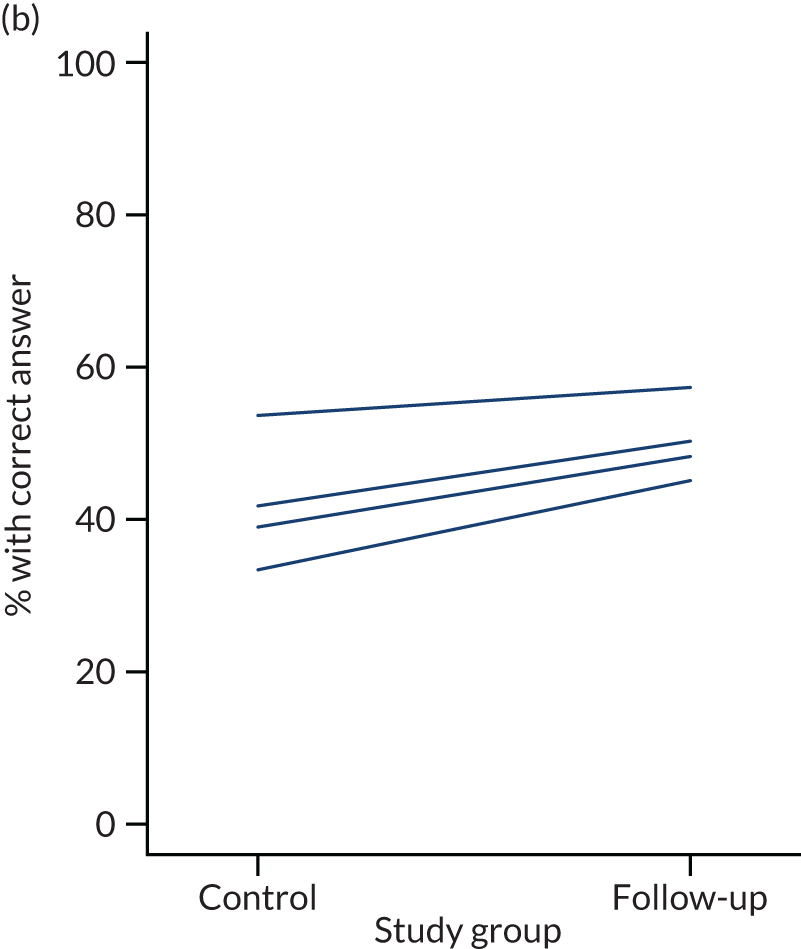
Across the nine knowledge questions, the proportion of students getting at least six questions correct was 25% in the control group and 36% in the follow-up group.
Attitudes and norms
A comparison of attitudes and norms across follow-up and control groups is shown in Figure 14. The items were as follows (the positive attitude responses are in brackets):
-
It is OK for someone who is not your boyfriend or girlfriend to ask you to send a nude pic of yourself (disagree).
-
The sex shown in pornography is similar to sex in real life (disagree).
-
Keeping a partner happy is a good reason to have sex (disagree).
-
It is not OK to have sex with someone who is very drunk (agree).
-
As long as you use a condom some of the times you have sex, your risk of getting a STI is very low (disagree).
FIGURE 14.
Percentage of (a) control and intervention students reporting positive sexual attitudes and (b) students reporting a positive change in attitudes by intervention exposure. Each line represents an attitude. Lines are drawn for ease of comparison and do not indicate change over time.
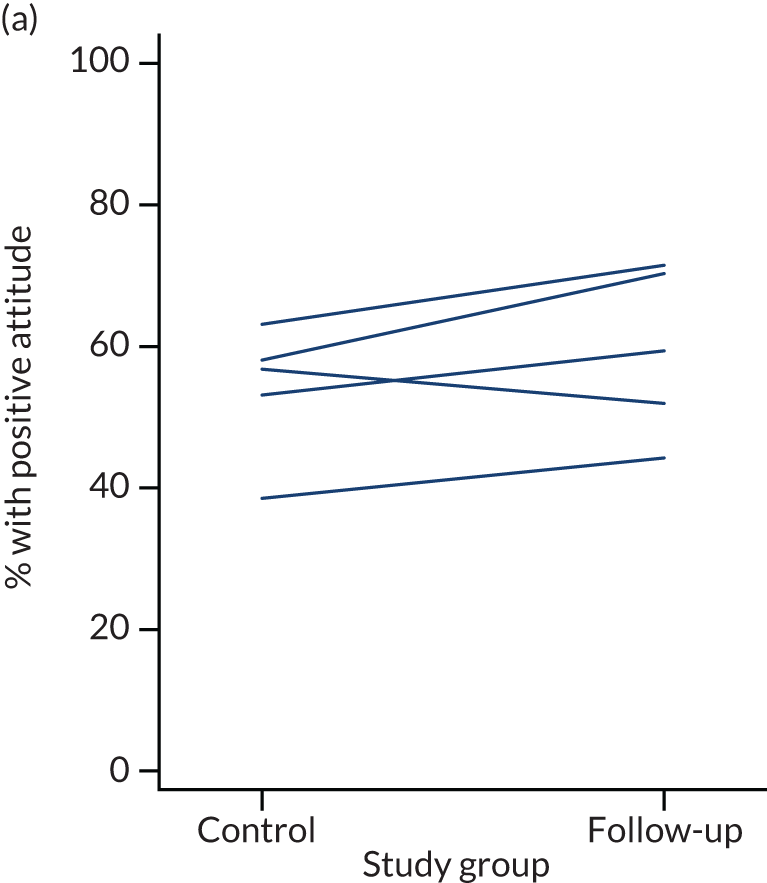
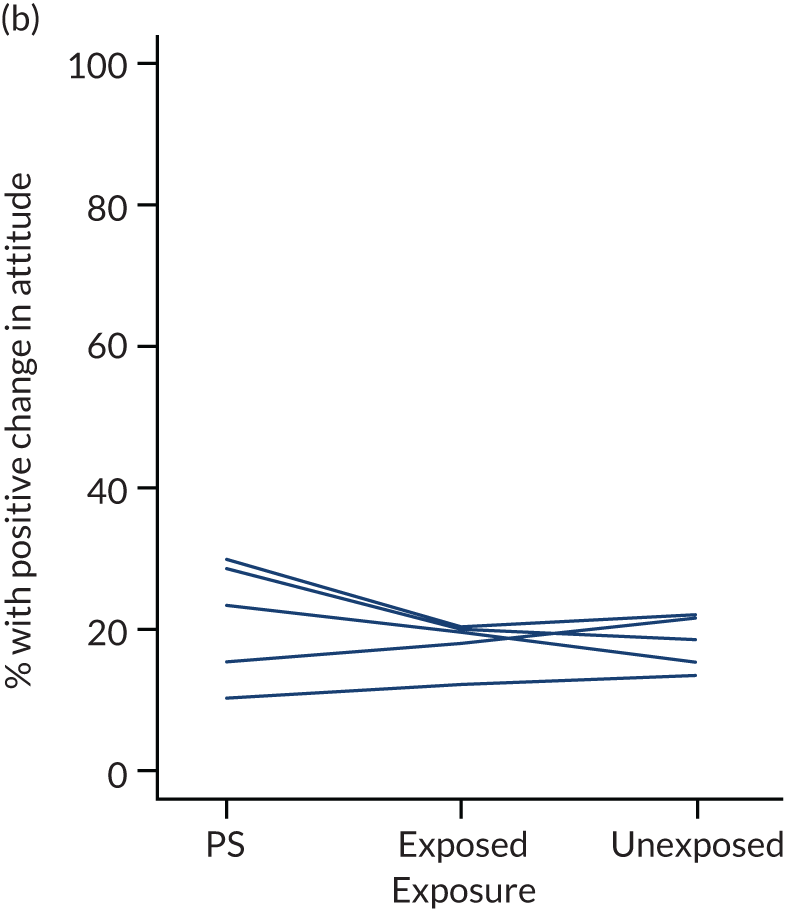
The response rates to the attitude and norm questions were similar across the study groups, ranging from 96% to 98% at baseline, from 95% to 96% at follow-up and from 96% to 97% among the control students.
The rates of adherence to positive attitudes and norms were slightly higher among follow-up students than among control students, with the exception of question 1, which was lower for follow-up students. The Cronbach alpha of the attitude question bank, as a whole, was 0.52.
We found no difference between follow-up and control students with regard to overestimation of the proportion of sexually active students in their year group (half of both follow-up and control students thought that more than one-third of students in their year were sexually active; the actual figure was 20%).
Confidence
The confidence question bank asked, ‘How confident are you that you could:’
-
‘get condoms of your own?’
-
‘put a condom on yourself or a partner?’
-
‘refuse to have sexual intercourse if they won’t use a condom?’
-
‘recognise when a partner doesn’t want to do something sexual?’
-
‘tell a partner that you don’t want to take part in a sexual activity?’
-
‘tell or show a partner what sexual activities you like or dislike?’
Response options were very confident, quite confident, unsure, not very confident, and not at all confident. These were recoded as a binary variable: confident (very, quite) versus other. Follow-up students were asked questions 1–3 at both baseline and follow-up, whereas the other questions were asked only at follow-up. The response rates to the confidence questions were high across the study groups, with 100% completion of the baseline questions, 86–98% completion at follow-up and 98–99% completion among the control students. The Cronbach alpha for the question bank, as a whole, was 0.77.
Generally, confidence was similar or slightly lower among students at follow-up than among control students. An exception was question 3 – refusing to have sex if a partner will not use a condom – for which follow-up students were more confident than control students (73.4% of follow-up students confident vs. 67.7% of control students confident).
Relationship well-being
A bank of items asking about relationship well-being was designed specifically for the STASH study, after we failed to identify any suitable measures of relationship well-being in young people. PCA was carried out on the seven relationship well-being indicators to assess whether or not a summary score could be constructed. The relationship indicators were (with the answer representing a healthy relationship in brackets):
-
They get very angry with me (not often/never).
-
We do sexual activities that I do not feel comfortable with (not often/never).
-
They get jealous and want to know what I’m doing and who I’m with (not often/never).
-
I tell them how I really feel (often/all the time).
-
I feel happy when we are together (often/all the time).
-
I feel comfortable talking about sexual things with them (e.g. whether to do something sexual, using condoms, sexual activities I like) (often/all the time).
-
They respect my opinions and ideas (often/all the time).
Only students who were in a relationship were asked to answer the questions. The response rates for the relationship indicators were similar across the study groups, with a 97–100% completion rate at baseline, a 98–99% completion rate at follow-up and a 98–99% completion rate among control students.
The PCA showed that there were two clusters of questions: questions 1–3 and questions 4–7. Together, these two clusters explained > 63% of the variability in the data and this was consistent whether the analysis was carried out on the control data alone, the follow-up data alone or both combined. The Cronbach alpha for the first measure (questions 1–3) was 0.66, whereas for the second measure (questions 4–7) it was 0.79. The question bank overall had a Cronbach alpha of 0.66. Future validation work on the measure could consider dropping the first subscale (items 1–3) to give a four-item measure of positive relationships. This four-item measure correlated as expected with distress about sex life [those reporting higher well-being were less likely to report distress about their sex life: OR 0.882 (95% CI 0.788 to 0.987); p = 0.029]. Interestingly, those with higher relationship scores were less likely to report safe sex (OR 0.869, 95% CI 0.786 to 0.961; p = 0.006), perhaps because they were in a longer-term relationship and were using another form of contraception.
As well as summarising the individual indicators, we included these two subscales of relationship well-being. These were calculated as a sum of the constituent question scores, with the question options ‘all of the time/often/sometimes/not often/never’ being given scores of 0–4 for the first (negative) measure and 4–0 for the second (positive) measure. The range for each could therefore be from 0 (unhealthy) to 12 (healthy) for the negative measure and 0 (unhealthy) to 16 (healthy) for the positive measure.
Generally, the rates of the indicators of a healthy relationship among follow-up students were similar to, or slightly higher than, rates among control students. The subscales of relationship well-being were very similar between the groups, with the control mean for the negative scale being 9.1 (SD 2.5), the follow-up mean being 9.1 (SD 2.7), and the control and follow-up means for the positive measure being the same, at 13.5 (SD 2.8).
Other secondary outcomes
Scores on the SWEMWBS measure of mental well-being101 had response rates of 99% at baseline, 90% at follow-up and 98% among the control students. Well-being scores were similar between the study groups [control mean score 21.0 (SD 4.6), follow-up mean score 21.3 (SD 4.2)]. As one of our hypothesised outcomes for the trial was increased well-being among PSs, we looked at differences in well-being by exposure (PSs, exposed students and non-exposed students) but found no differences in scores [mean total score for PSs 20.8 (SD 4.7), mean total score for exposed students 20.8 (SD 4.6) and mean total score for unexposed 21.2 (SD 4.7)].
The response rate for distress about sex life was 92% at baseline, 91% at follow-up and 95% among controls. The proportion of students distressed about their sex life was low across the study population, with 8.2% reporting distress in the follow-up group compared with 10.3% in the control group.
The response rates for the social media use questions were 90–92% at baseline, 90–91% at follow-up and 94% among controls. Cronbach’s alpha for the question bank was 0.78. Rates of using social media to view sexual images or to send, receive or be asked for nude or sexual pictures or videos were slightly lower in the follow-up group than in the control group. Rates of sharing a nude or sexual picture of someone else were very low and almost identical between the control (5.2%) and follow-up (5.0%) groups. The proportion of students reporting that they had used the internet or social media to find information about sexual health was slightly higher in the follow-up group (18.4%) than in the control group (15.4%).
The response rates to the questions about finding it easy to talk to parents, friends and partners about sex were 90–97% at baseline, 89–96% at follow-up and 93–96% among controls. The Cronbach alpha for this question bank was 0.5, suggesting poor correlation between comfort communicating with parents and communicating with friends and partners. The rates of students finding it easy to talk about sex was very similar in the control and follow-up groups (parents: control 17.6% vs. follow-up 19.3%; friends: control 58.3% vs. follow-up 59.5%; partners: control 30.6% vs. follow-up 28.9%), with students being most likely to talk to friends.
Questions assessing sexual competency at first sex were asked of the control group, but not of the follow-up group. This was an adaptation of a measure used in the National Survey of Sexual Attitudes and Lifestyles. 99 These measures were summarised as being the right time, both partners being equally willing, contraception being used and a positive reason for having had sex. The response rates were around 94% for these items. PCA showed that there were two clusters among these measures, explaining 70% of the variance in the data. The first cluster was the right time and equal willingness, and the second cluster was use of contraception and a positive reason for having sex. The Cronbach alpha was 0.53 for the first cluster and 0.63 for the second cluster. These may therefore be useful for taking forward as overall measures of sexual competence in the definitive trial. At follow-up, we asked the item on willingness and regret, plus a new one on alcohol and drug use. These items were asked about last sex rather than first sex (to increase the potential number of participants for whom this question would be relevant). The Cronbach alpha for these three items was 0.66, suggesting good utility in a definitive trial.
Effect modifiers
Aside from gender, as previously discussed, various potential effect modifiers of the difference between the follow-up and control groups in the composite primary outcome variable were investigated.
Although none of the interactions with study group reached statistical significance, those which showed potential differences in magnitude were:
-
FSM [yes, OR 1.21 (95% CI 0.85 to 1.73); no, OR 0.92 (95% CI 0.37 to 2.30)]
-
ethnicity [white Scottish/British, OR 1.14 (95% CI 0.80 to 1.61); other, OR 1.54 (95% CI 0.54 to 4.36)]
-
educational attainment [six or more National 5s, OR 1.53 (95% CI 0.92 to 2.55); other, OR 0.91 (95% CI 0.59 to 1.41)]
-
religiosity [very/quite important, OR 1.57 (95% CI 0.63 to 3.90); not important, OR 1.11 (95% CI 0.78 to 1.59)]
-
number of friends having sex [all/most/some, OR 1.14 (95% CI 0.74 to 1.74); a few/none, OR 1.70 (95% CI 0.86 to 3.36)]
-
number of friends who drink alcohol regularly [all/most/some, OR 1.25 (95% CI 0.84 to 1.87); a few/none, OR 1.92 (95% CI 0.87 to 4.23)].
This indicates that the intervention potentially was more effective on behaviour among students on FSM, non-white Scottish/British students, those with higher educational attainment, those to whom religiosity was important and those with peer groups who were less likely to report risky behaviours.
These are therefore variables that should be collected in the definitive trial, to ensure that these potential effect modifiers can be assessed rigorously.
Acceptability of data linkage
We explored the acceptability and feasibility of measuring a biological outcome in the longer term via linkage of student questionnaires to routine health service data on STI diagnosis. To assess acceptability, students were asked a question about data linkage at each survey administration. At follow-up, the question was worded as follows:
In the future it would be useful to link the answers you’ve given us today with information about you that health professionals (doctors, nurses) in the NHS (National Health Service) collect.
This might help us to see if taking part in the STASH study might improve future health.
To link this information we need to get your name, address and date of birth from your school so that it can be linked to your NHS data.
Your details would be kept strictly confidential the linked data would be anonymised (will not identify you) and would only be used for research.
We would like to ask for your consent to link your NHS record with your questionnaire answers.
No, I don’t give my permission 1
Yes, I give my permission 2
In the control year, 280 (43%) students said that they would be willing to give permission for access to their records. In the intervention year, 332 (53%) students said they would be willing at baseline and 352 (66.5%) students said they would be willing at follow-up. Greater willingness at follow-up may be related to higher levels of awareness (and possibly trust) in the study, but is also likely to be because of improved wording with each questionnaire iteration. The question was increasingly simplified and less hypothetical, which may have an impact on acceptability. It is also worth noting that there were slightly more missing data at follow-up, with 82 students not completing the question, compared with 59 students at baseline and 46 control students.
With further improvement in wording, it may be possible to achieve an acceptability of about 70%, which could make data linkage feasible. However, linkage to biological outcomes would be difficult for three reasons. First, prevalence of STIs is low, requiring a large sample to detect a difference. At age 18–19 years, the population prevalence of chlamydia is 4.7% in women and 0.5% in men. 2 Second, linkage to health-care records would pick up only individuals attending a clinic for STI testing and would miss individuals with asymptomatic STIs who do not present. If the STASH study is effective in raising awareness of STIs then participants might be more likely to seek help, making differences in diagnosis difficult to interpret. Third, there are limitations to data sources. At present, in Scotland, data on STI diagnosis are captured in the National Sexual Health System. A unique Community Health Index (CHI) patient identifier number is currently recorded for only a proportion of patients, leading to incomplete data. An alternative option would be to link to abortion and pregnancy before age 18 years as a proxy for unsafe sex, but this is not ideal for an intervention primarily addressing STIs, particularly as unplanned pregnancy is declining,123 whereas STIs are not. 124
Summary of key findings
Primary outcome (behaviour)
-
The suggested primary composite outcome for the definitive trial is ‘always practising safe sex,’ defined as ‘no condomless (vaginal or anal) sex in last 6 months’.
-
There was an increase in odds of the (modified) primary composite outcome of 18% following the intervention (compared with the previous year’s control group), with a larger effect among girls.
Knowledge
-
High response rates and high Cronbach’s alpha for the question banks.
-
Knowledge generally increased regarding both sexual health and where to go for contraception and advice, over baseline and compared with the control group.
-
There seemed to be some confusion around the law regarding 15-year-olds having sex with each other, which needs to be addressed in the delivery of the intervention.
-
Likely to be a useful measure in the definitive trial.
Attitudes
-
High response rates and moderate Cronbach’s alpha for the question bank.
-
Attitudes were generally observed to be more positive following the STASH study intervention than among control students.
-
May be a useful measure in the definitive trial.
Confidence
-
Generally high response rates but slightly lower among students not exposed to the intervention. High Cronbach’s alpha for the question bank.
Relationship well-being
-
Very high response rates and good Cronbach’s alpha, particularly for the ‘positive’ relationship well-being subscale.
-
Students had similar or slightly higher rates of healthy relationship indicators in the follow-up group than in the control group.
-
The composite relationship well-being scores were almost identical, both between the study groups and across exposure groups among follow-up students.
-
The relationship well-being measures may not be useful in the definitive trial, although the positive composite measure, in particular, may be useful more generally as an assessment of relationship well-being in research.
Other measures
-
Response rates were generally high for these measures.
-
Well-being scores were similar between study groups and by exposure.
-
Rates of distress about sex life were low and slightly lower among follow-up students than control students. There was little difference by exposure.
-
Rates of using social media or internet for positive purposes were slightly higher following the STASH study intervention than among controls, whereas use for negative purposes was slightly lower following the STASH study intervention than among controls.
-
Students found it easier to talk about sex with friends than parents or partners, and there was little difference between the study groups.
-
Sexual competency may be usefully assessed by two measures: one combining the right time to have sex and equal willingness, and the other combining use of contraception and a positive reason for having sex.
-
Well-being scores, distress about sex life, social media use and ease of talking about sex did not show strong utility for the definitive trial. Sexual competency at last sex may have some utility.
Data linkage
Around two-thirds of students at follow-up were willing to provide permission to access their health records, but at this point linkage to STI diagnosis does not seem feasible.
Chapter 8 Health economic analysis
This chapter addresses the key components of a future economic evaluation and reports on the piloting of data collection methods.
Cost of the STASH study
Table 14 provides a summary of the total cost of the STASH study intervention. On average, teachers spent 23.5 hours per school on planning and organisation associated with the STASH study intervention, including attending the training, at a cost of £545 per school or £3270 in total over six schools. The bottom-up costing of £545 for organisation and delivery was very similar to a payment of £500 paid per school by the trial as compensation for teacher time to attend the training. The compensation payment was omitted from the calculation, as this would be double counting.
| Cost item | Cost (£) |
|---|---|
| Training of peer educators: venue hire | 3040 |
| In-school recruit sessions: trainer time | 600 |
| Fee for trainers to conduct training | 5737 |
| Fee for trainers: weekly support meetings, communication with PSs via social media | 7200 |
| Travel to and from training: peer educators and trainers | 1696 |
| Subsistence during training (snacks and lunch) | 4003 |
| Teacher time spent in organising sessions and training | 3270 |
| Total cost for 611 students | 25,546 |
| Average cost per school | 4258 |
| Cost per student | 41.81 |
Time spent on the STASH study reported by teachers varied by school from 8 hours to 39 hours, or from a cost of £185.92 for teacher time per school to £906.36. Once the costs of teacher time were included, the total average cost per student ranged from £38.28 to £45.36 (assuming 8 hours or 39 hours per school, respectively). School sizes also differed, with the smallest school having 46 students per year and the largest having 183 students per year. Assuming similar fixed costs regardless of school size, the average cost per student for a smaller school is £92.56 and for a larger school is £23.27.
The costs shown in Table 14 are exclusive of intervention design and preparation carried out by research team (design of website, design of training manual and training of trainers).
Cost of sexually transmitted infection-related resource use by STASH study participants
Descriptive statistics for sexual health-related resource use and rates of missing data are reported in Table 15. For the intervention year, means (number of visits, purchases, etc.) are reported both for numeric data (mean) and as imputed means, which included numeric responses plus imputed numbers where free text had been given instead of a number (e.g. ‘several times’ or ‘a few’). Overall, the number of missing data was relatively small (4.9–10%), with higher rates seen in the intervention group. Condoms from the NHS were the most common resource used, with 12% (n = 70) using condoms in the control group and 8.8% (n = 45) using condoms in the intervention group.
| Sexual health resource use | Control (N = 696) | Intervention follow-up (N = 611) | |
|---|---|---|---|
| Sexual health clinic | Yes, % (n) | 8.1 (49) | 5.7 (30) |
| Mean number of visits (SD)a | 2.3 (3.0) | 2.5 (1.5) | |
| Imputed, mean (SD)b | 2.3 (1.11) | ||
| Missing, % (n) | 5.9 (41) | 9.8 (59) | |
| School nurse | Yes, % (n) | 0.6 (4) | 1.5 (8) |
| Mean number of visits (SD)a | 1.5 (1.3) | 1 (0) | |
| Imputed, mean (SD)b | 1 (0) | ||
| Missing, % (n) | 6.5 (45) | 10.0 (61) | |
| GP | Yes, % (n) | 3.6 (23) | 3.6 (19) |
| Mean number of visits (SD)a | 1.7 (1.7) | 1.7 (1.1) | |
| Imputed, mean (SD)b | 1.3 (0.7) | ||
| Missing, % (n) | 5.9 (41) | 9.5 (58) | |
| Practice nurse | Yes, % (n) | 1.4 (9) | 2.8 (15) |
| Mean number of visits (SD)a | 1.8 (1.2) | 1.2 (0.4) | |
| Imputed, mean (SD)b | 1.1 (0.4) | ||
| Missing, % (n) | 6.3 (44) | 9.8 (59) | |
| Condoms (NHS) | Yes, % (n) | 12 (70) | 8.8 (45) |
| Mean number of purchases (SD)a | 7.6 (18.1) | 4.1 (7.1) | |
| Imputed, mean (SD)b | 3.7 (6.1) | ||
| Missing, % (n) | 4.9 (34) | 9.2 (56) | |
| Condoms (out of pocket) | Yes, % (n) | 6.3 (39) | 4.9 (26) |
| Mean number of purchases (SD)a | 9.7 (26.2) | 3.8 (7.1) | |
| Imputed, mean (SD)b | 3.5 (6.4) | ||
| Missing, % (n) | 6.0 (42) | 9.3 (57) | |
| Other contraception | Yes, % (n) | 7.4 (45) | 8.2 (42) |
| Mean number of purchases (SD)a | 2.6 (8.18) | 1.5 (0.88) | |
| Imputed, mean (SD)b | 1.7 (0.75) | ||
| Missing, % (n) | 6.2 (43) | 9.7 (56) | |
| Pregnancy test (NHS) | Yes, % (n) | 2.8 (18) | 1.7 (9) |
| Mean number of tests (SD)a | 1.1 (0.58) | 1.5 (0.8) | |
| Imputed, mean (SD)b | 1.4 (0.7) | ||
| Missing, % (n) | 5.9 (41) | 10.0 (61) | |
| Pregnancy test (out of pocket) | Yes, % (n) | 4.0 (25) | 1.5 (8) |
| Mean number of tests (SD)a | 4 (13.0) | 1.9 (1.7) | |
| Imputed, mean (SD)b | 1.6 (1.4) | ||
| Missing, % (n) | 5.6 (39) | 10.0 (61) | |
| STI test | Yes, % (n) | 1.7 (11) | 1.5 (8) |
| Mean number of tests (SD)a | 6.5 (15.7) | 1.6 (1.3) | |
| Imputed, mean (SD)b | 1.4 (1.1) | ||
| Missing, % (n) | 5.5 (38) | 10.0 (61) | |
| Emergency contraception | Yes, % (n) | 3.3 (21) | 3.0 (16) |
| Mean number of purchases (SD)a | 1.5 (1.3) | 1.4 (0.8) | |
| Imputed, mean (SD)b | 1.3 (0.8) | ||
| Missing, % (n) | 6.0 (42) | 10.0 (61) | |
The total adjusted cost per student of sexual health services was £30.87 in the control group (95% CI £18.68 to £43.24) and £15.64 in the intervention group (95% CI £2.14 to £29.04), with a total cost saving of £15.23 (95% CI –£30.38 to –£0.08; bootstrapped estimate –£12.77, 95% CI –£31.59 to £6.05). When out-of-pocket costs were included, the total mean cost per student in the control group was £32.88 (95% CI £20.61 to £45.31) and £16.06 (95% CI £2.43 to £29.58) in the intervention group, with a total mean cost saving per student of £16.82 (95% CI –£32.40 to –£1.24; bootstrapped estimate –£16.95, 95% CI –£35.75 to £1.85).
When the cost per student of the STASH study intervention (£41.81) is added to the average cost savings per student for sexual health services, the total cost of the intervention is £24.99 per student.
Combining costs for all students with the ‘always safe sex’ outcome, for each additional student classified as ‘always safe sex’ this corresponds to an average cost saving of –£85.72 (95% CI –£107.56 to –£63.88).
Measurement of quality of life and cost-effectiveness
Descriptive statistics for the CHU-9D are reported in Table 16. Young women and students identifying as ‘other’ had significantly lower utility scores than boys, with an average utility decrement of –0.068 (95% CI –0.081 to –0.056) for young women compared with young men, and –0.114 (95% CI –0.162 to –0.066) for students who identify as ‘other’ compared with young men. Students who identified as gay, lesbian, bisexual or other also had significantly lower utility scores than those who identified as heterosexual. There was no difference in utility scores between students eligible for FSM and those ineligible (our marker for potential socioeconomic deprivation).
| Variable | Value | Mean utility (95% CI) | Significance |
|---|---|---|---|
| Gender | Male | 0.849 (0.840 to 0.859) | |
| Female | 0.781 (0.773 to 0.789) | p < 0.0001 | |
| Other | 0.736 (0.688 to 0.783) | p < 0.0001 | |
| FSM | Yes | 0.815 (0.797 to 0.833) | |
| No | 0.809 (0.802 to 0.816) | p = 0.540 | |
| Sexual orientation | Heterosexual | 0.824 (0.817 to 0.830) | |
| Gay or lesbian | 0.707 (0.670 to 0.744) | p < 0.0001 | |
| Bisexual | 0.716 (0.691 to 0.742) | p < 0.0001 | |
| Other | 0.682 (0.648 to 0.717) | p < 0.0001 |
Mean unadjusted utilities derived from the CHU-9D at each time point are reported in Table 17. There was no significant difference between control and intervention year group utility scores at follow-up in the adjusted multilevel model, including imbalances in gender (–0.010, 95% CI –0.035 to 0.015; bootstrapped estimates –0.010, 95% CI –0.022 to 0.002).
| Utility score | Control (n = 636) | Intervention time point | |
|---|---|---|---|
| Baseline (n = 615) | Follow-up (n = 561) | ||
| CHU-9D, mean utility (SD) | 0.821 (0.123) | 0.804 (0.131) | 0.801 (0.131) |
To investigate the reliability of the CHU-9D as a measure of student health-related quality of life, we investigated whether or not it was positively associated with other measures of well-being and self-esteem, as hypothesised. The CHU-9D had a significant positive correlation with the SWEMWBS measure of well-being (0.46, p < 0.0001). For every 1-point increment on the SWEMWBS, there was a corresponding 0.014 (95% CI 0.013 to 0.015) gain in utility on the CHU-9D.
There was also a significant decrease in utility for each step away from ‘strongly agree’ response options for the three measures of self-esteem. For the item ‘I like myself’, there was a utility decrement of –0.047 (95% CI –0.052 to –0.042) for each step from ‘strongly agree’ to ‘strongly disagree’. For the item ‘Most of the time, I like the way I look’, there was a utility decrement of –0.042 (95% CI –0.047 to –0.037) for each step from ‘strongly agree’ to ‘strongly disagree’. For the item ‘I have high self-esteem’, there was a utility decrement of 0.042 (95% CI –0.046 to –0.037) for each step from ‘strongly agree’ to ‘strongly disagree’.
There was no significant relationship between the CHU-9D utility scores and the proposed primary outcome of ‘always safe sex’ (increase of 0.003 in CHU-9D utility scores for each additional case of ‘always safe sex’, 95% CI –0.017 to 0.022; p = 0.775).
Incremental cost-effectiveness ratio, cost-effectiveness acceptability curve and cost-effectiveness plane
The incremental cost-effectiveness ratio for the intervention compared with current practice from the health-care cost perspective is £1303 (–12.77/–0.010) per 1-point gain in utility. Including out-of-pocket costs, it is £1715 (–16.95/–0.010). This is dominated by the control group if the cost of the STASH study intervention is introduced (additional cost per student of £24.99 and a utility loss of –0.010). The cost-effectiveness plane is reported in Figure 15. As most of the values sit in the south-west quadrant, where the intervention costs less but also results in a lower utility, the resulting cost-effectiveness acceptability curve (Figure 16) is difficult to interpret. There is a 93% probability that the intervention is cost-effective for very low values (close to £0) of willingness to pay for a utility, but a 2% probability for a willingness to pay > £6500. The probability of cost-effectiveness decreases as willingness to pay increases because, as willingness to pay for utility increases, the reduction in utility for the intervention year plays a greater role in the probability of cost-effectiveness than in the cost savings.
FIGURE 15.
Cost-effectiveness plane for all costs, including the cost of STASH study, out-of-pocket costs and NHS costs for intervention year compared with control year.
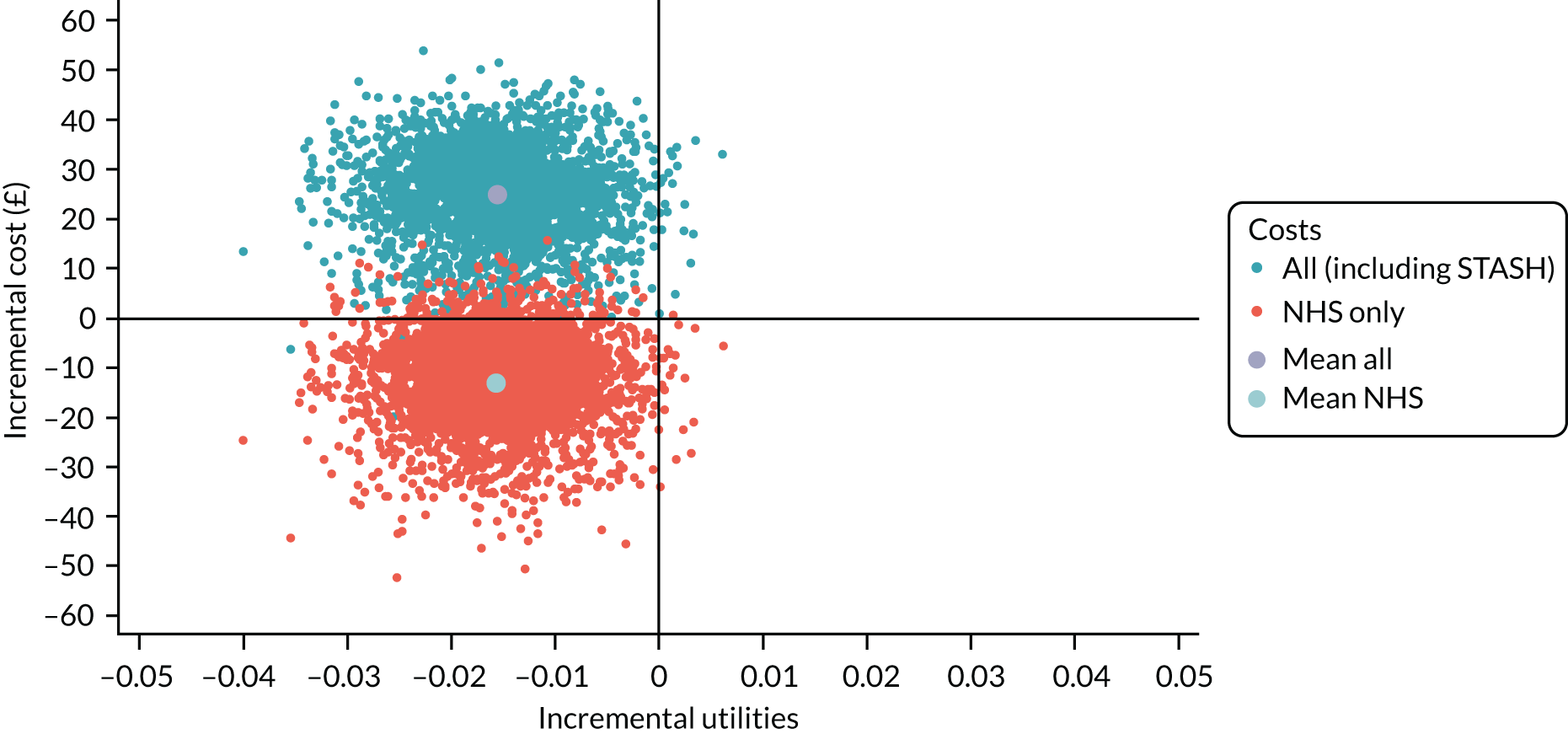
FIGURE 16.
Cost-effectiveness acceptability curve of NHS costs, out-of-pocket costs and intervention costs for intervention year compared with control year. Int, intervention; OOP, out of pocket.
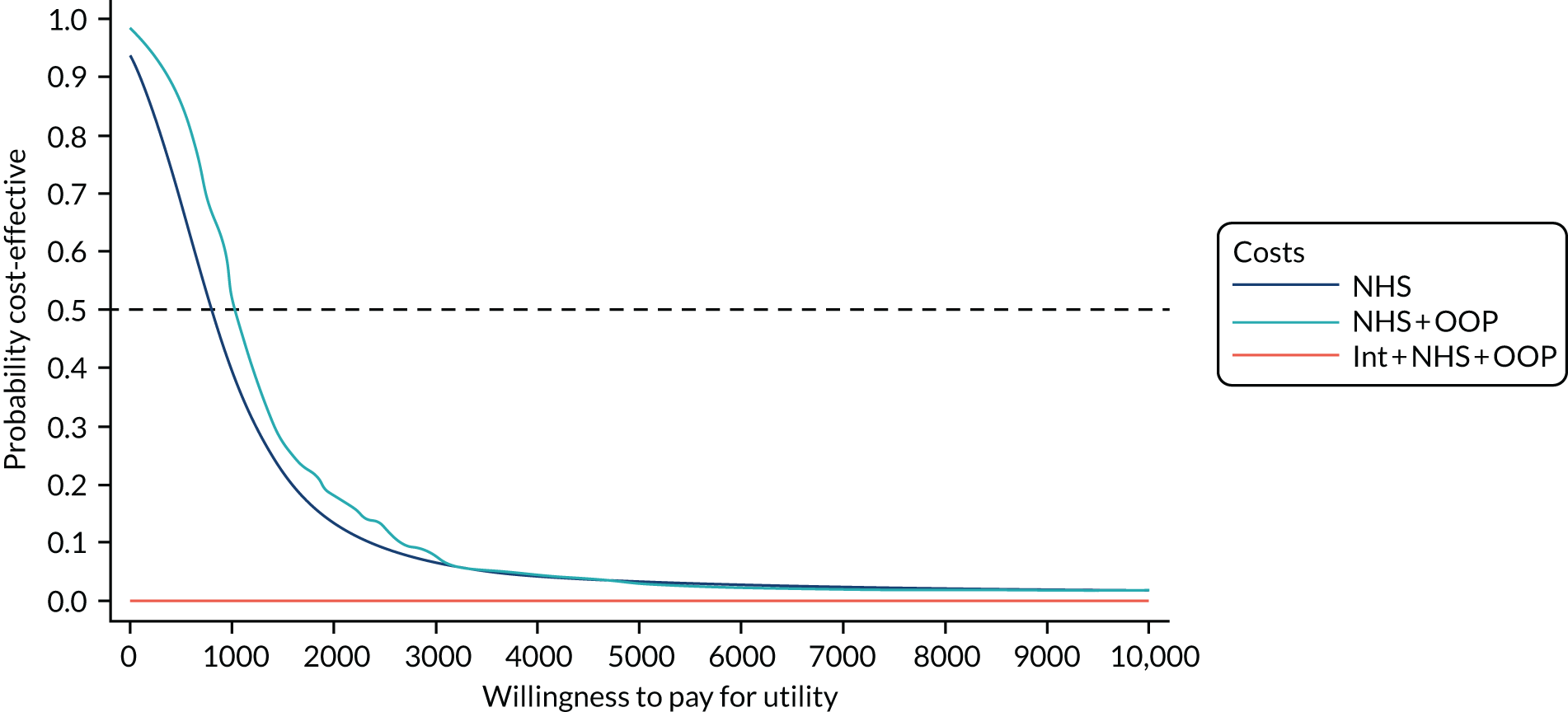
If the proposed primary outcome of ‘always safe sex’ was used instead of the CHU-9D, the cost per additional person having ‘always safe sex’ would be £1315, assuming that 85% of students had ‘always safe sex’ in the control group and 87% of students had ‘always safe sex’ in the intervention group, and a cost per student of the intervention of £24.99 compared with the cost savings.
Subgroup analysis
For young men, there was a difference in utility of 0.008 (95% CI –0.025 to 0.042) for the intervention year compared with the control year, with an average cost saving per student of –£10.78 (95% CI –£38.63 to £17.07) for NHS only costs, an average cost saving per student of –£17.78 (95% CI –£46.12 to £10.57) when out-of-pocket costs are included and a mean total of £24.03 per student when the cost of the intervention is added. This corresponds to an incremental cost-effectiveness ratio of £3004 (24.03/0.008) per 1-point change in utility.
For young women, there was a utility decrement of –0.036 (95% CI –0.077 to 0.005) for the intervention year compared with the control year, with an additional cost of £15.61 (95% CI –£8.50 to £39.71) for NHS costs and £15.65 when out-of-pocket costs are included (95% CI –£8.59 to £39.89). The intervention is dominated by the control.
Interpretation of findings
The total cost of the STASH study intervention was approximately £42 per student or £4258 per school for a year group of approximately 100 students. This varied from £23 per student to £93 per student, dependent on the number of students in a year group. In comparison with school size, assumptions about the duration of time teachers spent on the preparation and delivery of the STASH study intervention had less of an impact on potential costs (£38–45 per student). It is possible that the cost of the intervention could be reduced if taken to scale, for example by reducing costs of travel or meals, to result in a lower cost per student.
It was feasible to collect STI health-care resource use data from students. Costs of sexual health services were significantly lower for students in the STASH study intervention year than for control students, with a cost saving of £15.23 per student to the NHS and £16.82 if out-of-pocket costs are included. These data should be interpreted with caution, given that this is a feasibility trial and also because some of these costs relate to preventative behaviours that might represent a saving to the NHS in the longer term. The net mean total cost per student was therefore £25 when NHS cost saving and out-of-pocket costs were incorporated. This was mostly due to a reduction in condom use and pregnancy tests. The reduction in condom use might be because the proportion of students having sex in the past 6 months was lower in the intervention year than in the control year, although the difference is small (19% in control and 17% in intervention) (see Chapter 7). The reduced use of pregnancy tests in the intervention year may be because of an increase in safe sex in the intervention year, although again the difference is small (85% ‘always have safe sex’ in the control group and 87% in the intervention group) (see Chapter 7).
The analysis included costs that occurred over the duration of the trial only. Looking at within-trial costs for all students in the study, each additional case of ‘always safer sex’ corresponded to a reduced cost to sexual health services of £86. Over a longer time horizon, additional cost savings could accrue via reductions in STIs and unintended pregnancies that were not captured over the duration of this intervention.
It was feasible to collect CHU-9D data and we found hypothesised significant relationships with the variables expected (well-being and self-esteem). However, there was no relationship with the proposed primary outcome of ‘always safe sex’.
The small, non-significant, reduction in CHU-9D in the intervention year makes the cost-effectiveness of the intervention difficult to interpret in the standard cost per QALY gained framework recommended by NICE. The suitability of using the CHU-9D to calculate QALYs in a future evaluation of the STASH study is questionable. A key issue for a cost-effectiveness analysis as cost per outcome gained, is that it is hard to envisage what an appropriate effectiveness outcome would be, as costs per STI or averted unplanned pregnancy are difficult to interpret. Averted unplanned pregnancies can have significant long-term savings, with an estimated 10-year cost saving of £23,909 per pregnancy averted (including the cost of health care, social security benefits and child education costs). 125 Calculating the cost of STI prevention is more complex because different STIs have different costs and consequences. Furthermore, STIs can be transmitted to other individuals, resulting in additional costs to the system. A systematic review and 1-year statistical model of the costs and QALYs of behavioural interventions to prevent STIs in young people aged 13–19 years found that for a cohort of 1000 boys and 1000 girls a behavioural intervention would avert three STI cases, with an additional 0.5 of a QALY. 25 Owing to data limitations and uncertainty around intervention effect size, the authors considered the findings purely illustrative and they were unable to project effectiveness or cost beyond the 1-year time horizon.
The results of public health interventions for which the costs occur in different parts of the system can make policy decisions challenging. For instance, in Scotland, third-sector partners and NHS boards are responsible for ensuring that schools are adequately equipped to teach relationship, sexual health and parenthood education. 126 As a result, all parties in the system have a vested interest in ensuring suitable sexual health education. In England, schools are responsible for delivering SRE,127 with discretion as to how they achieve this. Meanwhile, provision of sexual health services falls within the budget of local authorities, contraception costs can fall within both local authority budgets and the NHS, and the costs of unintended pregnancies falls across NHS, local authorities and the Department of Work and Pensions (if social security benefits are included). To understand the relative impact of sexual health education in schools on each of these government departments, it is recommended that costs and benefits to different sectors are reported separately,108 and that a cost–consequences analysis may be more appropriate, although this is not the option preferred by NICE. 106 Return on investment, reporting all costs to publicly funded organisations and budget impact analysis, when the costs to specific payers and service providers are reported separately, are other potential options. A budget impact analysis may be attractive given the potential cost savings to the NHS. Different models could be explored, in which the intervention is delivered at a lower cost to schools and no cost to local government. There is no perfect option for analysis of the cost perspective, and the choice will involve a trade-off between capturing all relevant costs but providing no specific answer to any one decision-maker (societal analysis), or specificity to one decision-maker but not capturing costs to other affected stakeholders (health-care cost perspective).
An alternative approach is to model long-term outcomes of STIs and unintended pregnancies related to increases in safe sex. This may be more appropriate to capturing the impact of the STASH study intervention on both costs and consequences. Such a model would allow for cost-effectiveness as cost per QALY to be calculated by including the disutility of STIs in the model. A decision model was beyond the scope of this project, but would be a useful component in a future evaluation of the STASH study.
Any future evaluation will need to collect sufficient, relevant data to facilitate a range of analysis options, so that the results can be reported in ways that are useful to different audiences, including schools, local authorities, the NHS and national policy-makers, such as the Scottish Government and NICE.
Chapter 9 Key findings and recommendations
The STASH study intervention was feasible to implement in six Scottish schools with varying levels of deprivation and educational attainment. It was highly acceptable to the students, staff and trainers involved. This chapter presents key findings against the study objectives.
Key findings against study objectives
Objective 1
Finalise the design of a school-based STI prevention intervention, in which influential PSs use online social networks and face-to-face interactions to influence norms, knowledge, competence and behaviour, and promote use of sexual health services.
We met the first objective via reviews of literature and sex education resources; intensive consultation with young people and professional stakeholders (patient and public involvement); co-production and optimisation of a website of curated resources and a training manual; and an intervention pilot. Intervention development work identified key motivations for schools in terms of meeting national targets for health and well-being, and providing leadership opportunities for senior students. Our consultations and pilot affirmed that the peer nomination process used in ASSIST would be palatable to students and staff, but that we might need to overinvite students (25% of the year group rather than 17.5%) to the recruitment meeting, to train 15% of the year group as PSs (the proportion deemed critical in ASSIST). 67
In response to discussions with stakeholders regarding the sensitivity of the topic, we developed additional nomination questions focused on trust and listening skills to pilot alongside the original ASSIST questions (focused on respect and leadership). Most development activities contributed to the design of a curated set of shareable digital resources (housed on the STASH study website) and a bespoke training manual. Over various iterations, the STASH study website became increasingly visual and decreasingly reliant on text and signposting to other websites (as students in the pilot rarely clicked on these links).
The PS role crystallised incrementally in response to ideas from young people and stakeholders, as well as learning from the pilot. The role was eventually clarified as information giving, attitude influencing, promoting the website and signposting to sexual health services. Professional stakeholders were clear that the PSs would require training on handling sensitive disclosures and that they should be advised to avoid a counselling role. A PS charter was created to signal to PSs the responsibility inherent in the role.
The STASH study sought to adapt to contemporary modes of social interaction by introducing a social media option for dissemination of messages. A review of current platforms identified Facebook as the only one to meet the project requirements of closed and private groups and ability to interface with a website. Consultations with young people established that Facebook was not a first choice of platform for young people, but nevertheless it was widely used and broadly acceptable. A key design feature, initiated in response to concerns of teachers, was to stipulate that the STASH study trainers would monitor and support online activities via membership of each PS Facebook group. Development activities, and particularly the pilot, highlighted the need to increase awareness of the STASH study across school staff and year group students, but suggested a flexible approach, allowing each PS team to decide a course of action appropriate to their school.
Objective 2
Assess the recruitment and retention of PSs, as well as feasibility and acceptability of the intervention among PSs, participants and key stakeholders.
We anticipated that role uptake would be lower than in ASSIST57 and the ASSIST extensions128 because we were delivering the intervention on a more sensitive topic to a year group undertaking public examinations. Across the six schools, 52% of nominated students (63% of those attending the recruitment meeting) were trained. Variation across schools (a high of 77% in school 5 and a low of 33% in school 6) was consistent with process evaluation findings of variable levels of school buy-in and support of the intervention, as well as variation in the quality of the ‘pitch’ given by trainers at the recruit meeting. Role retention was very high, with 97% of PSs fulfilling the role (defined as posting three or more STASH study messages on Facebook or having two or more conversations and attending two or more follow-up sessions). The intervention was highly acceptable to PSs (85% said they liked the role), more so to young women (94%) than to young men (71%).
The majority of PSs liked the STASH study website and found it easy to navigate and share messages. The STASH study appeared to achieve a good balance between allowing flexible engagement and ensuring trainer monitoring and support.
Over 70% of PSs said that they found the STASH study more relevant, helpful and interesting than their usual SRE lessons. Of the other students engaging with STASH study messages via the PSs (exposed students), 74% thought that the way the STASH study was run was acceptable and 78% thought that the information provided was acceptable. Again, acceptability was higher for young women than for young men. We did not interview parents directly, but only one student reported that their parent was unhappy about them being a PS.
The eight staff members interviewed were positive about the ethos of the STASH study, the leadership opportunities it afforded, the rapport between trainers and PSs, and the high-quality training. Staff acknowledged the additional workload involved in delivering the STASH study intervention and the challenges for students in terms of missing classes for training and follow-up sessions. One teacher raised concern about school capacity to deliver the intervention. His concerns related as much to the burden of the evaluation as the intervention, and partly reflected that the school was undergoing a major transition at the time.
Objective 3
Assess the fidelity and reach of intervention delivery by trainers and PSs, including barriers to, and facilitators of, successful implementation.
The STASH study was implemented with excellent fidelity. All nomination exercises, recruitment sessions, external trainings and 35 of 36 follow-up sessions were delivered as planned. Attendance at follow-up sessions was high (average 80%), particularly given that this was an examination year. The PSs were highly active on social media, sharing 1343 messages from the STASH study website to their Facebook groups over the course of the intervention period (5 weeks in three schools and 10 weeks in the other three schools). On average, PSs reported six face-to-face conversations about the STASH study with their friends.
Social network analysis showed that students trained as PSs were well positioned across their year group friendship networks. They had greater potential to reach across their year group than students who were not nominated (5.3 incoming friendship ties vs. 3.5 for non-nominated students). PSs were also well distributed across friendship clusters, ranging from presence in one-third of friendship groups in one school to four-fifths in another. Across all schools, PSs had direct friendship ties to one-third of students.
The intervention had good reach across the S4 year group, with 58% (n = 611) of students at follow-up reporting some level of exposure (trained as a PS, visited the website or member of a Facebook group, or had a conversation with a PS). Young women were more likely to report exposure than young men (63% vs. 53%, respectively). Educational attainment and sexual experience at baseline both appeared linked to likelihood of exposure, but not socioeconomic deprivation, ethnicity, religiosity or sexual orientation. Key facilitators identified were buy-in and support from schools; visibility of the STASH study intervention to the rest of the year group and school; good rapport at training; high-quality training; regular direct communication between trainers and PSs via Facebook, including reminders for follow-up meetings; the use of private and closed groups to give PSs control over message sharing; and well-planned and regularly spaced follow-up sessions that included an interactive activity, as well as progress check.
Key barriers identified were reliance on schools for scheduling of activities; academic pressures, such that follow-ups scheduled during class time were difficult for some teachers and students; technical issues with the website (these were small in number); infrequent use of Facebook among some students; low levels of awareness of the intervention across the rest of the school; low levels of intrinsic motivation of non-PSs to engage with PS activities; and poorer engagement by young men compared with young women, probably due to higher embarrassment and less maturity in discussing sexual health issues.
Objective 4
Refine and test the programme theory and theoretical basis of the intervention.
We used the feasibility trial to test the STASH study programme theory, leading to a refined theory in which mechanisms of change, conditions of success and context were more clearly articulated (Figure 17). We also explored ways to visualise the theory to reflect the dynamic interaction of intervention components in a format accessible to stakeholders and delivery partners (Figure 18). Figure 17 shows the version of the programme theory following the feasibility trial, but prior to the full analysis of the results. Figure 17(a) shows the full logic model from problem identification to outcomes and Figure 17(b) ‘explodes’ the intervention component to detail the conditions of successful implementation and mechanisms of action. In comparison to the post-pilot, pre-feasibility trial programme theory, the version showing in Figure 17 has a number of key refinements. It more clearly sets out the theoretical underpinnings of the trial at micro, mid and macro level. It articulates the mechanisms of change for key actors in the intervention and it more clearly establishes the conditions of successful implementation, linking these to their respective intervention components. In addition, we refined our expectations of the key intermediate and end outcomes. We added competence at last sex (equally willing, no regret, no alcohol) and ease of talking about sex as intermediate outcomes, we moved relationship well-being to the end outcomes, and we added confidence and well-being among PSs as an end outcome. These refinements to the end outcomes emerged from discussion – with the TMG, TSC and project stakeholders – about the importance of recognising the wider potential impact of the trial beyond STI prevention. Although we captured qualitatively the broader psychosocial benefits for PSs, our measures of well-being (at least in this small sample) did not pick this up. Similarly, our new measure of relationship well-being was unable to detect a difference between intervention and control groups (see Objective 6).
FIGURE 17.
The STASH study programme theory: feasibility trial stage. (a) Full programme theory; and (b) details of conditions of successful implementation and mechanisms of action. TDF, theoretical domains framework. Reproduced from Forsyth et al. 62 This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/. The figure includes minor additions and formatting changes to the original figure.
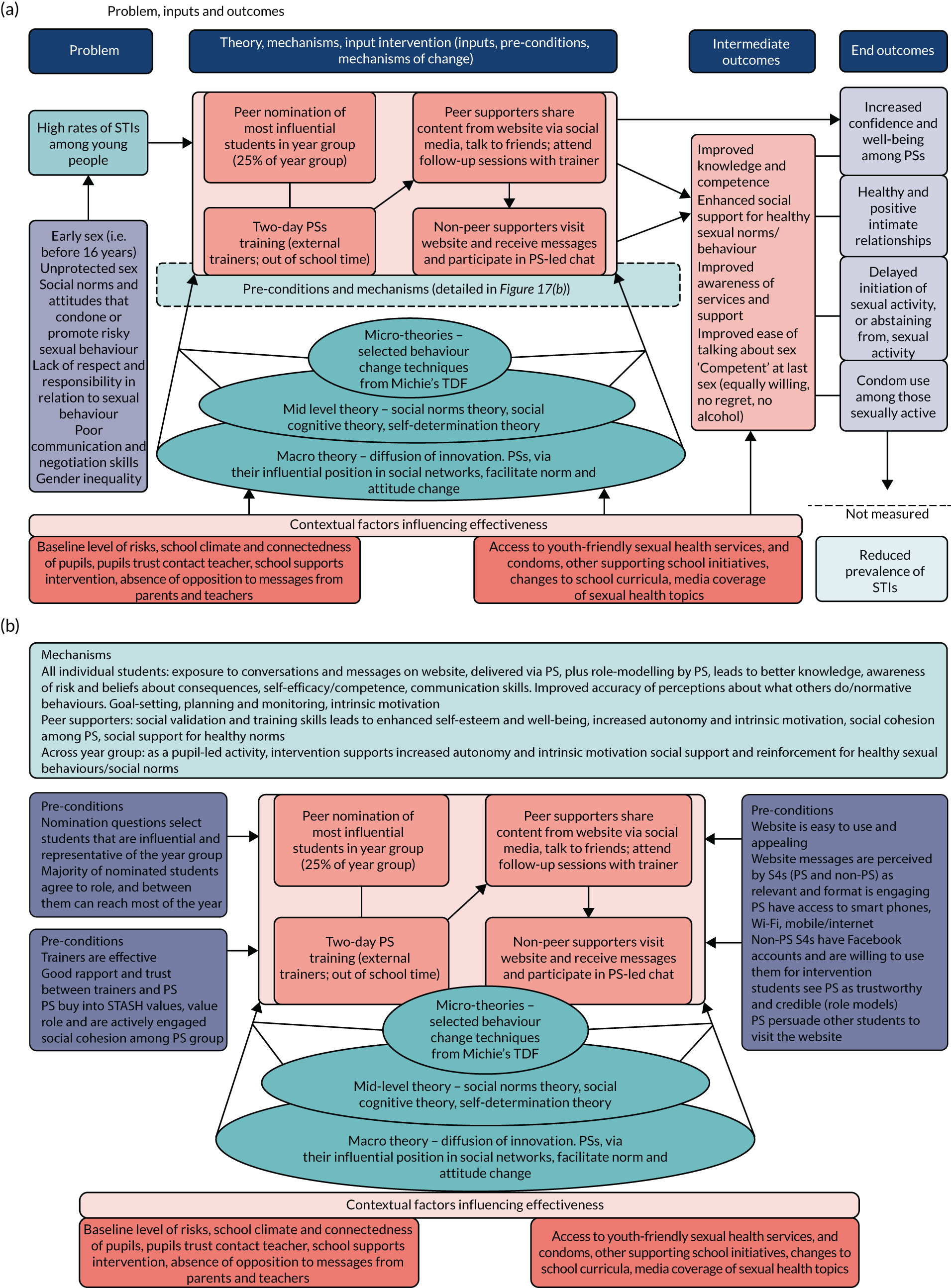
FIGURE 18.
An alternative visualisation of the programme theory designed primarily to explain the STASH study to stakeholders (using an animation to highlight different stages). The visualisation highlights the conditions and mechanisms relevant to each intervention stage.
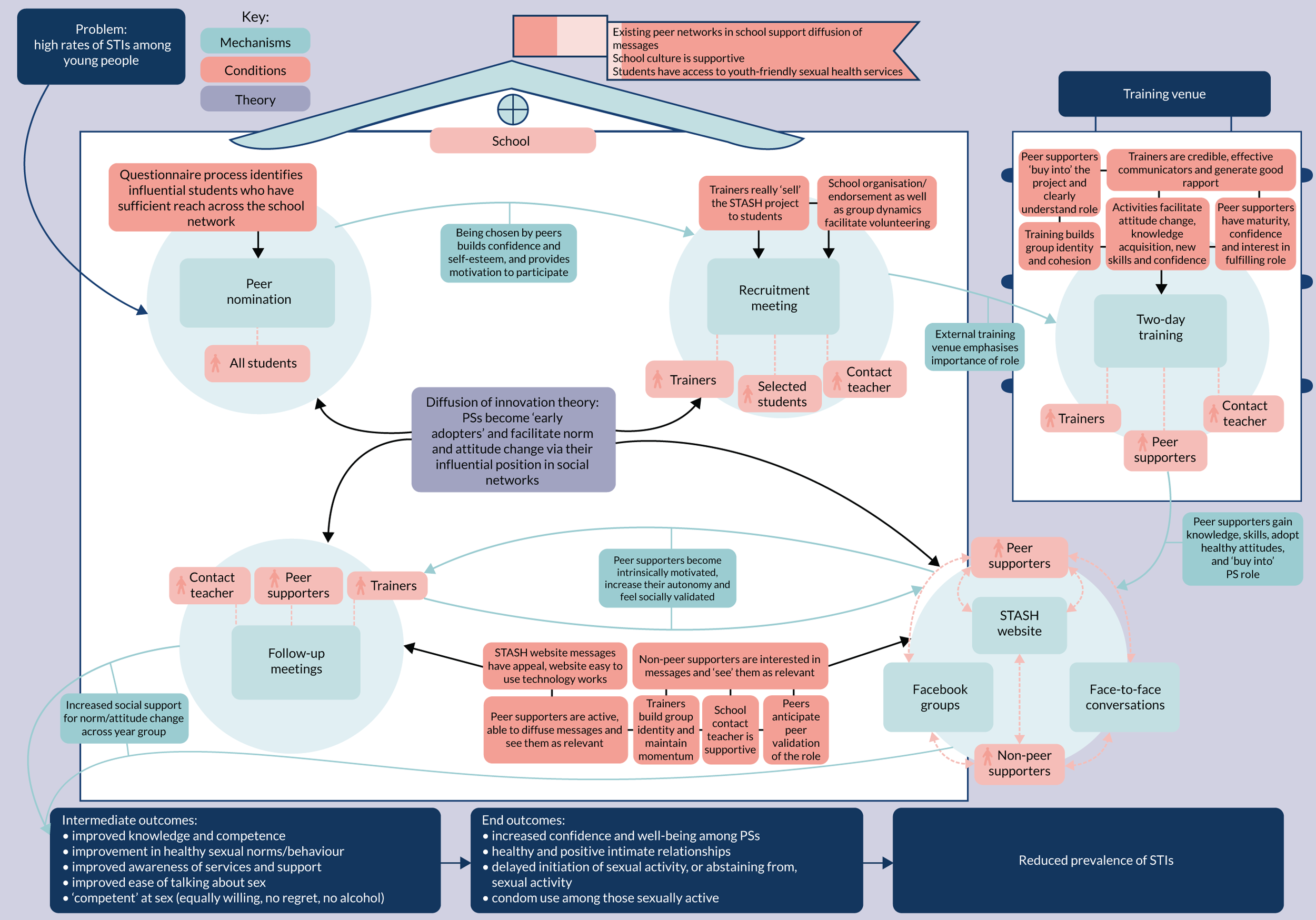
Our analysis of the feasibility trial data largely confirmed that the programme theory presented in Figure 17 adequately captured the preconditions of success and contextual factors influencing effectiveness. In general, the key conditions were met, with variability across schools. Some conditions were harder to meet than others.
The feasibility trial was able to interrogate the mechanisms of change to some extent (see Figure 17). Table 18 shows the mechanisms in a separate box, alongside key evidence from the study relating to that mechanism and suggested revisions to the hypothesised mechanisms for a future version of the programme theory. The more challenging mechanisms were those dependent on PS delivery of activities (the aspect of the intervention over which we had least control). In particular, there appeared a limit to which the PS felt socially validated in the role by their peers (they appeared neither validated nor disproved of). A key finding was that there appeared a limit to which non-PSs were interested in messages and saw them as relevant. Although the training led to enthusiasm and awareness of sexual health issues among PSs, it appeared difficult for them to generate the same level of interest among their friends via brief messages and conversations. As these conditions were only partially met, the extent to which the intervention supported autonomy and intrinsic motivation (a purported mechanism of change) is unclear.
| Mechanism | Summary of evidence | Recommendation |
|---|---|---|
| All students | ||
| Exposure to conversations and messages on website, delivered via PSs, plus role-modelling by PSs, leads to better knowledge, awareness of risk and beliefs about consequences, self-efficacy/competence and communication skills | Strong evidence of PS conversations and delivery of messages. Some evidence of role-modelling (e.g. modelling attitudinal norms and treating sexual health as important). Early indications of changes in knowledge and attitudes. Unclear picture regarding competence and communication skills | Retain as mechanisms |
| Improved accuracy of perceptions about what others do/normative behaviours | No change in per cent with accurate perception of how many others in the year are sexually active | Retain as mechanisms. Stronger focus on norms in future intervention content |
| Goal-setting, planning and monitoring. Intrinsic motivation | Did not assess goal-setting and planning, and this was not a strong focus of the intervention. Intrinsic motivation among all students seems unlikely | Consider whether or not to strengthen goal-setting and planning in training content |
| PSs | ||
| Social validation and training skills leads to enhanced self-esteem and well-being, increased autonomy and intrinsic motivation, social cohesion among PSs and social support for healthy norms |
PSs neither validated nor invalidated in role. Some evidence for increased autonomy, intrinsic motivation and social cohesion. This study was unable to pick up significant change in self-esteem and well-being. Owing to small numbers, this study did not investigate increased support for healthy norms among PSs as a group PSs did gain confidence/self-efficacy following the training and the process evaluation suggested that this was important |
Retain as mechanisms. Employ stronger qualitative assessment of social support for healthy norms in future evaluation Add increase confidence/self-efficacy |
| Across year group | ||
| As a pupil-led activity, intervention supports increased autonomy and intrinsic motivation. Social support and reinforcement for healthy sexual behaviours/social norms | Some evidence of increased autonomy. Evidence suggested weak intrinsic motivation among non-PSs | Remove ‘intrinsic’ from ‘increased intrinsic motivation’ to consider broader range of motivations. Otherwise, retain the mechanisms |
Diffusion of innovations theorists suggest five stages in the adoption of new behaviours (knowledge, persuasion, decision, trial and adoption). 129 Owing to variation in the pace at which people move through the stages of adoption, considerable time can elapse between first and last adopters, even for clearly advantageous behaviours. 24 The theory suggests that the rate at which a new idea or behaviour is adopted depends, among other things, on the past experiences and needs of potential adopters. 59,129 A challenge for sexual risk reduction messages in mid-adolescence is that only a proportion of students are sexually active [approximately 20% reported vaginal or oral sex in this study (see Table 11)]. The ‘potential adopters’ of new messages on sexual behaviour may be relatively small (particularly as some of those who are sexually active are already practising safer-sex behaviours). The STASH study messages were wide-ranging in recognition of this variation among the target group; even so, students who were not sexually active may have simply decided that the STASH study was less personally relevant to them.
Given that sexual experience and ‘readiness’ for messages about sexual health will always be variable within a S4 student year group, it is worth reinterrogating our programme theory to ask whether or not supporting increased autonomy and intrinsic motivations is (1) realistic and (2) an essential mechanism of change. The architects of self-determination theory, Ryan and Deci,83 describe how social and environmental factors can facilitate or undermine intrinsic motivation (cognitive evaluation theory,83 a subtheory within self-determination theory). In the STASH study, PSs were able to create their own groups, and to choose which messages to share, how and with whom, and non-PSs had full autonomy over if and how they engaged with messages. The practice and ethos of the STASH study was thus autonomy supportive, particularly in comparison with more controlled didactic classroom-based methods. What seems less clear is whether or not this autonomy led to intrinsic motivation. Interestingly, the top two motivations cited for PSs continuing in the project were ‘learning information’ and ‘fun’ (see Chapter 5, Motivation to participate), and not extrinsic rewards, such as benefit to CV, indicating some level of intrinsic motivation among the PS group. Among non-PSs, intrinsic motivation to engage with the topic appeared low, but it is worth questioning whether or not this is a realistic expectation across the year group, and whether or not it is essential as a mechanism of change. It is possible that norms can be diffused across a peer network with relatively low levels of intrinsic motivation to engage with the intervention. Therefore, in the next iteration of the programme theory, increased intrinsic motivation should perhaps be limited to PSs and not the year group as a whole. In Recommendations for future evaluation, we also suggest ways to enhance non-PS engagement in the intervention.
Objective 5
Enhance understanding of the potential of social media, when used by influential peers, to diffuse norm change and facilitate social support for healthy sexual behaviour.
The students interviewed in the STASH study engaged with social media for primarily social reasons, using a range of platforms. Social ‘gossip’ unfolded seamlessly across online and offline spaces, such that not keeping up online could mean missing key developments in social events. Non-PS student reactions to receiving STASH study posts via Facebook ranged from openness and interest to indifference. Some saw the opportunity to engage online as less awkward, whereas others preferred face-to-face conversation or a mix. To the extent that non-PSs registered and responded positively to messages, it appeared important that messages were sent by someone they knew and seen by others in the group, such that there were opportunities for discussion. In other words, the offline social context was key in both legitimising and augmenting online messages.
The process evaluation confirmed findings of the intervention development stage in suggesting a strong preference for humorous, colourful, eye-catching images, with as little text as possible. The opportunity to share messages within a private group rather than on a general profile page was key to feeling comfortable, and PSs were discerning about who they invited. Issues of stigma and unease at being linked to sexual health content, identified in previous social media interventions in sexual health,130,131 did not emerge as particular issues in the STASH study. This is most likely as a result of the use of private groups. A possible cost of this privacy is that STASH study interactions may have been viewed as parallel to, rather than embedded in, PSs’ usual online social interactions.
The presence of a trainer within the private groups appeared reassuring for many, although only a small number felt the need or wished to engage with them in this forum (primarily young women). In terms of practical considerations, the use of social media necessitates hiring trainers who are comfortable using it, and there are challenges in establishing a design that is sufficiently flexible to keep pace with constantly evolving platforms and technology.
Objective 6
Determine key trial design parameters for a possible future large-scale trial, including recruitment and retention rates, strategies, outcome measures, ICC and sample size.
All six schools were retained in the study. Response rates for the student surveys were 80% for the controls, and 82% at baseline and 79% at follow-up. Among the intervention year, 81.2% of students completing the baseline questionnaire also completed the follow-up questionnaire. Response rates were slightly lower than other recent school-based studies. 128,132 As parental opt-out (n = 6) and student non-consent (n = 3) were low, the response rate primarily reflected the number of students who attended school on survey days, and made it to the class in which the questionnaire was administered. There was a suggestion from teachers that the class lists (on which the denominator was based) were not always up to date and included students who did not regularly attend school. Our finding that students who did not complete the follow-up questionnaire were more likely to be male, from more deprived backgrounds and with lower educational entertainment highlights both the importance of conducting the STASH study in schools (where the fullest range of young people can be reached) and the methodological challenges of doing so.
We investigated a number of candidate primary outcomes, identifying a composite measure of ‘always practising safer sex’ as a potential primary outcome for the trial. We defined this as ‘No condomless (vaginal or anal) sex in the last 6 months’. A future intervention would seek to increase the proportion of students practising safer sex either by not having sex (the safest option) or by having sex but always using a condom. The odds of reporting always safer sex in this study were in a direction suggestive of benefit, although the study was not powered to demonstrate a significant difference. Like all self-report measures of sexual behaviour, this outcome is subject to social desirability bias and, to a lesser extent, recall bias. A further limitation is that it does not include unprotected oral sex and also does not account for situations in which two young people in a long-term monogamous relationship may have stopped using condoms following negative STI tests. These behaviours will be measured in the outcome questionnaire.
Delayed initiation or no sex and condom use are the most common outcomes in youth-targeted sex education interventions,3,31 but these are usually reported separately. Some studies use a measure of consistent condom use, whereas others focus on condom use at last sex. 3,31 For instance, the school-based ‘Safer Choices’ intervention had three separate primary outcomes: (1) delayed initiation of sexual intercourse, (2) frequency of sex with a condom among those reporting intercourse and (3) the number of sexual partners with whom students had condomless intercourse in the last 3 months (among those reporting intercourse). 133 Our composite outcome captures the first and second of these dimensions within a single measure. In a subsequent evaluation, we would not propose to measure the third dimension, because the rate of partner change within our time frame for follow-up is too low (an average of one partner) (see Chapter 7, Descriptive statistics for primary outcomes). Reviews of condom use measures in evaluating human immunodeficiency virus prevention show substantial heterogeneity in measurement, with no trend towards standardisation over time. 134 Condom use at last sex is the most common measure, followed by consistency of condom use; however, current recommendations do not suggest clear superiority of one over the other. 134 With respect to youth-targeted interventions, a challenge is that behavioural outcome measures can present an inconsistent picture. For instance, the STAND study found an increase in condom use at last intercourse, but negative changes in other outcomes (e.g. condom use in anal sex, unplanned pregnancy and STIs). 41
In terms of secondary outcomes, our question banks on knowledge and attitudes had high response rates. Reliability was good for the knowledge question bank (Cronbach alpha 0.7) and medium or low response rates for the question bank on attitudes (Cronbach alpha 0.52). Knowledge was higher, and attitudes more positive, in the intervention responses than in the control, suggesting potential benefit of the intervention (again, not powered for significance). The question bank on confidence had good response rates and reliability (Cronbach alpha 0.77); however, we found an inconsistent picture (control year higher on some items and follow-up on others), possibly reflecting that individual assessment may vary according to experience of trying a behaviour (such as negotiating condom use). If taken forward to a future trial, these measures should be limited to those with sexual experience. Our newly designed measure of relationship well-being had high reliability (Cronbach alpha 0.79) for the positive subscale in particular (measuring openness, happiness, comfort and respect) and correlated with related constructs (e.g. distress about sex life), but did not differentiate between control and intervention groups. This needs to be considered in the decision about whether or not to take this forward. Our adapted measure of sexual competence99 (willingness, regret, use of alcohol or drugs) has medium reliability (Cronbach alpha 0.66) and merits inclusion, but condom use should be added to the measure (as a key dimension of competence). The measure should also be asked of most recent sex, rather than first sex, to increase the number of students for whom the question is relevant.
Our analysis of potential effect modifiers suggested several that might affect the primary outcome and should be retained: FSM, ethnicity, educational attainment, religiosity, peer group sexual behaviour and alcohol use. Other modifiers did not demonstrate an association with the primary outcome and could possibly be omitted from the questionnaire going forward. These include self-regulation, parental monitoring, sexual attraction and importance of social media to social life.
Although a study objective, we ultimately opted not to propose a sample size calculation for a definitive trial at this stage. This is partly because the estimate of effect from this small sample is imprecise and yet any sample size calculation would be highly sensitive to it. The recent DELTA2 recommendations state that pilot trials are typically too small to form a reliable basis for a sample size calculation, although they can indicate a realistic target difference. 95 At the stage of designing a full-scale evaluation, we will follow the recent DELTA2 guidelines to calculate the sample size, basing it on a wider range of sexual health interventions and on an assessment of what would be considered meaningful to key stakeholders. 95 Evidence from previous school-based sexual health interventions suggests that any differences in behaviour are likely to be small;3 for instance, the effective and widely adopted ‘Safer Choices’ intervention found estimated OR effect sizes (intervention vs. control) of 0.83 for sexual initiation (non-significant), 0.63 for frequency of sex without a condom in last 3 months (p = 0.05) and 0.73 for number of sexual partners without a condom in last 3 months (p = 0.02). 133 In our case, an OR of 1.2 may be realistic for an outcome of ‘always safer sex’. In terms of what is considered meaningful, a drop in the primary outcome of a risk behaviour may be less important to educational stakeholders than improved well-being, and health sector stakeholders may be happy to accept a small change in primary outcome when other secondary outcomes (such as knowledge about where to seek help and self-efficacy in condom use) improve. Such considerations are key, particularly when only small changes in the primary outcome are realistic. A further consideration is the heterogeneity in measurement of primary outcomes for youth-focused STI prevention. The DELTA2 guidance recommends performing a sensitivity analysis to consider the effect of uncertainty in the estimate of the target difference. This study provides useful information to contribute to our review of existing literature: a control proportion of 0.854 for practising ‘always safer sex’ and an ICC estimate (based on follow-up and control students) of 0.0198.
Objective 7
Determine the key components of a future cost-effectiveness analysis and test data collection methods.
The total cost of the STASH study intervention was approximately £42 per student or £4258 per school for a year group of approximately 100 students. This varied from £23 per pupil to £93 per student, dependent on year group size. This suggests that the intervention may be more costly to deliver in smaller schools, a fact that should be borne in mind for future evaluation and roll-out. The question bank on sexual health-related resource use was completed well, with relatively low levels of missing data. We established that the CHU-9D was unsuited to calculating QALYs in the context of the STASH study because it was not associated with the primary outcome of always practising safer sex. This analysis confirmed our lack of theoretical expectation that the intervention would have an effect on the domains measured by the CHU-9D, making the CHU-9D an inappropriate and insensitive measure for any effects on well-being that might be achieved by the STASH study. Lower CHU-9D scores in the control arm made the resulting incremental cost-effectiveness ratios, cost-effectiveness acceptability curves and cost-effectiveness planes difficult to interpret. A possible approach for the economic evaluation in a future trial of the STASH intervention could be to model long-term outcomes of STIs and unintended pregnancies related to increases in safer sex, accounting for the disutility of a STI and unplanned pregnancy.
Objective 8
Establish whether or not pre-set progression criteria are met and if a larger-scale trial is warranted.
The study set seven progression criteria regarding the feasibility and acceptability of the intervention and evaluation. We adopted a traffic light system (green, amber, red), with green targets as follows:
-
In each of four schools, 60% of nominated students are recruited and complete the training.
-
In each of four schools, 60% of PSs complete the training, send three or more messages or have three or more conversations, and attend two or more follow-up meetings.
-
In each of four schools, 60% of PSs report that they ‘liked’ the role.
-
In each of four schools, 60% of students who are exposed to the STASH study agree that the intervention was acceptable.
-
No major acceptability issues raised.
-
Less than 15% of PSs report that their parents or carers were unhappy about them being a PS.
-
In each of four schools, achieve student response rates of > 70% at baseline and follow-up.
We met green targets with ease for all criteria bar the first. This first indicator (red) was discussed at length with the TSC, as stipulated in our protocol. At the trial outset, we agreed that in the case of amber or red, a mitigating strategy should be identified and continuation should be considered only if all other targets were green. Given that the green targets were easily surpassed for all other criteria, the TSC were supportive of continuation.
Although we did not achieve 60% role uptake among those nominated, we were still able to train 13% of the year group as PSs. This is just short of the 15% deemed critical in the popular opinion leader model of peer education on which ASSIST is based. 66 We achieved this partly by overinviting the top nominees (taking the top 25%, rather than the 17.5% invited in ASSIST). Nominees who took up the role received more nominations than those who declined to participate, suggesting that uptake was more likely among the more influential students. This suggests that we may have thrown the net a little wide and that inviting a smaller proportion to recruitment (for example 20%) might still achieve a critical mass of 15%, but with a higher proportional uptake among those invited. The number of friendship ties was broadly similar across those who did take up the role and those who did not take up the role, except that the trained PSs had higher two-step reach centrality (mean of 27 students reached in two steps vs. a mean of 24 students reached for those who did not take up the role). The PSs were well distributed across friendship clusters, with results similar to those in ASSIST. 40 PSs also had higher potential to reach across their network than non-nominated students, and were reasonably representative of their year group, being similar in terms of ethnicity, age, religiosity and sexual orientation, but slightly more academic and more likely to be eligible for FSM (a proxy for low-income household). PSs were slightly more likely to report some sexual experience at baseline, such that role uptake may have been related to perceived personal relevance of the topic and/or readiness to hear messages about sexual health.
The target of 60% was based on the experience of ASSIST and extensions of ASSIST67,128 [in which role uptake was high (> 90%)], but may have been set too high for the STASH study given the topic and age group of the students. Among younger students in ASSIST, the prospect of a 2-day training out of school provided a strong motivation, whereas in the STASH study this element received a mixed response, because of academic pressures. There is little evidence from peer-led sexual health interventions to guide decisions on an appropriate target for recruitment. Of five peer-led studies included in a recent European systematic review,32 none used peer nomination to select peer educators (two employed teacher selection, two asked for volunteers and one did not report the selection method). The USA-based STAND study41 is, to our knowledge, the only other youth-focused sexual health intervention to employ peer nomination. The STAND study41 was also a school-based study targeting 15- to 16-year-olds. Their peer nomination process identified 42 opinion leaders, of whom 21 were trained (50%), a very similar proportion to the STASH study. This suggests that 50% uptake may be a more reasonable target. Nonetheless, it is important to think about how we might improve uptake in the future. The target of 60% was far surpassed in one school (77%) and nearly met in two schools (58% and 56%), suggesting that more intensive work to prepare and support schools may be important. In establishing the appropriate proportion of nominees invited to the recruitment meeting, it will be important to identify the percentage (somewhere between 17% and 25%) that achieves the highest proportional uptake while still recruiting 15% of the year. Other possible mitigation strategies regarding the recruitment process are discussed in Recommendations for future evaluation.
Recommendations for future evaluation
Adaptation to the intervention
-
Further strategies to enhance awareness of the intervention in the year group and among school staff should be developed. Strategies employed in this feasibility trial included announcements in registration class, assemblies, bulletins and staff meetings. The PSs were given flexibility to ‘announce’ the project according to their preference. In practice, the effectiveness of these activities depended on the support they received from school staff. Going forward, the intervention might supplement these activities via a standard trainer-delivered SRE session, which would give key STI prevention messages and introduce both the project and the PSs. Such a session would help generate a more supportive context for PS activities, reducing the ‘surprise’ element of sexual health messages appearing in student social media threads. It would also reduce the inbuilt inequality of exposure being dependent on proximity to a PS and increase the coherence60 of the intervention for participants (in understanding why only a proportion of the year received training). The cost implications in terms of additional trainer time would need to be considered.
-
Uptake of the PS role could be improved in a number of ways. On average, 13% of nominees did not attend the recruitment meeting and so did not have a chance to consider participation. The importance of the recruitment session needs to be emphasised to schools, along with practical suggestions as to how they can support the process. For larger schools, in particular, it may be prudent to split the recruitment meeting into two sessions, on the basis that students may feel more comfortable in smaller groups. The second session would have an additional benefit of providing a mop-up for those who missed the first. We found that in addition to school support, the ‘pitch’ given at the recruitment meeting is very important. Equipping trainers to deliver a strong pitch, with a focus on the key motivators (identified as curiosity, benefit to CV and fun) may also help to increase uptake. Anonymous PS testimonies given in this study could be integrated into recruitment materials and if the STASH study is delivered in subsequent years within the same school, there would also be the option of inviting previously trained PSs to talk about their experience. This is likely to be both reassuring and motivating.
-
The study established social media as effective at diffusing intervention messages when used in conjunction with face-to-face elements. At a practical level, the social media element needs to be ‘future-proofed’ to cope with evolving engagement in social media and technological advances. In addition, the appropriate level of control over social media use requires confirmation. Ideally, PSs would have flexibility to engage with STASH study messages using a social media platform of their choice, giving them greater ownership and potential to tailor to the social media preferences of their friendship group. The absence of any untoward incidents in our study suggests that some loosening of control and enhanced flexibility may be justifiable and beneficial; however, this will require careful consideration and monitoring. On a practical level, updates to the website should aim for simplicity for users and minimisation of technical issues.
-
A challenge for the STASH study was the range and complexity of messages required to fully equip young people for positive sexual health and avoidance of STIs. This challenge was intensified by the wide range of sexual experience and existing knowledge across the year group, such that individuals differed in the messages they required and found relevant. Our literature review strongly supported a holistic intervention content (rather than a focus on STIs and risk)11–13 and flexibility for PSs to engage with messages according to their interest. Although beneficial in terms of ownership and engagement, this high level of choice was challenging for some PSs. In future, the intervention might supplement the curriculum with a set of streamlined, simple and memorable ‘basic set’ messages that PSs are encouraged to engage with as a minimum.
-
Any future roll-out of the intervention will need to address the gender bias in engagement. A finer-grained analysis of motivations to participate might identify particular motivators for young men that could be used to strengthen the appeal for them.
-
In terms of timetabling, the peer nomination process could be moved back to June (prior to summer break) so that the baseline questionnaire could be implemented as soon as schools return from the summer break. This would have an important additional benefit of giving more time for intervention delivery before the Christmas break. It is possible, although unlikely, that friendship networks change over the summer break, so this change may need to be piloted (e.g. by repeating the nomination survey in a single school).
-
Our health economics analysis suggests that delivery in a small school is potentially more costly.
-
In the longer term, the ideal implementation model for the STASH intervention could be an annual cycle of delivery for successive S4 year groups. Trained PSs moving into S5 and S6 (the final 2 years of secondary school) could support the PSs and deliver additional activities, such as supporting school drop-in clinics, facilitating SRE sessions for younger years and undertaking outreach. A wider implementation model such as this might facilitate embeddedness within schools and contribute to longer-lasting impact. After the study ended, the STASH trainers continued to work with PSs in several schools post intervention (e.g. to support the school drop-in clinic) and informal learning from this work will contribute to future discussion on intervention implementation.
-
A significant alternative adaptation to the model would be to train S6 students (aged 16–18 years) as PSs, rather than S4. The S6 students could use social media and face-to-face conversation to diffuse messages to their peers in S6 (and S4 and S5 if desired, as senior students are often in mixed year group classes), as well as facilitating classroom sessions with S4 students. The project could be delivered in a 3-year cycle, in which S4 students initially taught by S6 PSs eventually become trained PSs themselves. This approach could potentially address some of the limitations identified in this study. First, the older age group would be more palatable to schools because there is less academic pressure in S6 (the main public examinations are undertaken in S5) and students tend to have free periods in which follow-up sessions could be scheduled. Second, there would be a greater proportion of sexually active students for whom the STASH study messages feel personally relevant, thereby potentially addressing some of the identified challenges around intrinsic motivation. Third, an older age group would not require such close control and monitoring of social media use, enabling students to engage more flexibly with different social media platforms. Finally, in later school years, young men tend to ‘catch up’ in terms of reaching a level of maturity conducive to full engagement with the role. Although it could be argued that S6 is too late to prevent unsafe or unhealthy first sexual experiences, the fact that the STASH study is intended to augment rather than replace sex education justifies waiting until a greater proportion of the target group perceives the messages as personally relevant. In an English educational context, this would translate to the lower sixth year group. In schools with a separate sixth form, the intervention may need to take place later in the school year, as new friendship groups will need time to establish.
Adaptation to data collection methods
-
Administering the questionnaire was burdensome for schools and a future trial should consider ways to reduce this burden. A return to a paper-and-pen questionnaire is not suggested for reasons of data quality. 117,118 One option for a web-based survey, would be for the fieldwork team to carry mobile Wi-Fi ‘hotspots’, which would allow students to remain in class and complete the survey on their mobile phones. A pilot of this approach in another ongoing school-based study within our unit suggests that this is feasible (Equally Safe Research team, University of Glasgow, 2020, personal communication). A small number of tablets could be made available to students without phones or charge. This approach would reduce logistical difficulties and increase privacy. Survey administration may be easier for schools if there is a clearly identified back-up or support teacher for each contact teacher. This person should be present at all early planning meetings to ensure that they understand the study and can stand in effectively.
-
The questionnaire was slightly long, both for students undertaking it and for administration within a school period. Reducing the length of the questionnaire should be straightforward to achieve, as analysis of the outcome measures identified a number of items that can be omitted. We have identified specific ways to improve questionnaire wording and filtering. We could also do more to work with teachers to identify language issues ahead of time and put in place measures to support students on a school-by-school basis.
-
The questionnaire was experienced as intrusive by some students. This is, to some extent, inevitable in a survey on attitudes and behaviour related to sex. Although we were careful to explain the questionnaire topic in the participant information sheet, and at the start of the questionnaire, we could expand the introduction to the survey on the fieldworker script. A stronger explanation as to why we need to collect the data could be provided, focusing particularly on the questions that raised concern about confidentiality, such as the postcode and friendship module. Reassurances could be repeated throughout the questionnaire. At follow-up, an additional explanation should state the reasons for repeating the same questions, as higher levels of missing data at follow-up may reflect students feeling that they have already answered the questions.
-
With respect to the PS questionnaire, judicious use of open-ended questions would allow us to collect further insight into varied perspectives across the PS cadre, augmenting the qualitative data collection.
Methodological strengths and limitations
This study has a number of strengths. Intervention development followed a rigorous and theory-driven approach, involving significant co-production with young people, professional stakeholders and the trainers who subsequently delivered the intervention. Consistent with the existing literature,135–137 we found this process indispensable in establishing what was appealing to young people and feasible to implement. A strong feature of the evaluation was the wide range of data sources and use of synthesis and triangulation to develop a rich picture of intervention experience. In addition to establishing the potential of the intervention approach, the study has made key contributions to understanding the social network position of individuals rated as influential by their peers, and the potential of using social media within the context of peer-led and school-based sexual health interventions.
Some of the study limitations relate to those of feasibility studies in general. The small sample means that the study cannot give an indication of future effectiveness. It also placed limits on the extent to which we were able to investigate the reliability and validity of candidate measures. Owing to the lack of precision, we avoided reporting p-values.
A limitation of the qualitative methods employed in the process evaluation was that embarrassment and stigma associated with the topic appeared to constrain the depth and candidness of student accounts. Conversations were sometimes stilted or dominated by banter that served to mask embarrassment and avoid loss of face. This was particularly the case in a group (albeit friendship) setting and school context. It was therefore difficult to interpret whether or not lack of recall of detailed information about the STASH study related to minimal engagement or reluctance to talk about the topic in front of other group members. This was much less an issue for PSs, who were more comfortable with the topic following their training. In terms of sampling, we were limited in the extent to which we could follow-up PSs who had dropped out or interview students beyond those in PS friendship groups. We also did not interview parents, relying on PSs and teachers to report their reactions. An absence of complaints by parents does not necessarily imply that all parents were happy with the intervention or with their child being a PS. A practical limitation was that group interviews had to take place within a school period. Once participants had gathered, and informed consent had been taken, there were sometimes only 30 minutes remaining for discussion.
Finally, in common with much feasibility work, the STASH study took place within a small geographical area and transferability to regions with different educational contexts will require careful attention to differences in context, particularly those relating to preconditions of the intervention.
Conclusion and first steps towards future evaluation
This study has demonstrated that the STASH study is a feasible approach to undertaking STI prevention within the context of Scottish secondary schools. It can be implemented with good fidelity and is acceptable to those involved. We have established the potential of carefully managed social media use when supported by face-to-face conversation. All bar one of our progression criteria were met, with the weight of evidence supportive of continuation to a full-scale evaluation. Prior to this, we believe that small-scale work may be prudent to ‘future proof’ the website to interact with a range of social media platforms. We should also pilot more flexibility and less monitoring of social media, enhanced ways to increase the salience of the intervention in schools, enhanced methods of peer recruitment and implementation in an older year group. As the feasibility and acceptability of the intervention has been established, it seems reasonable to test any proposed changes to intervention delivery (including the switch to an older age group) as an internal pilot. We envisage the next step as a multicentre evaluation across the UK. This will involve adjustments to other UK education systems, for example in relation to the timing of the STASH study within the academic year, timetabling of activities, school pastoral support structures and existing provision of sex education in schools. In England, sex education has recently become a statutory requirement and the STASH study is likely to appeal to school leaders as a student-led initiative that delivers on this requirement. Other key policies, such as the use of mobile phones in school, are subject to change in future and may impinge both on intervention and evaluation designs. The STASH study will also need to keep apace with technological and legal changes in relation to social media apps. The project will need to build in flexibility to adjust to these differences and potential changes, most of which will be outside the research team’s control.
The starting point for the scaled-up evaluation is further refinement to our programme theory. We will discuss the refinements proposed by this study with key stakeholders, and undertake a literature review and stakeholder consultation to confirm the optimal study design, primary outcome measure and sample size.
Acknowledgements
The study was funded by the National Institute for Health Research Public Health Research programme (14/182/14). The intervention costs were funded by the Edinburgh & Lothians Health Foundation (861) and the Scottish Government (14/182/14). We are grateful to all three funders for giving us the opportunity to develop and evaluate the STASH study. We would like to thank the Population Health Research Facility at the MRC/CSO Social and Public Health Sciences Unit, University of Glasgow, for their professional and dedicated approach to questionnaire data collection. We would also like to thank our TSC (Professor James Hargreaves, Professor Simon Forrest, Dr David Gillespie and Ms Alice Hoyle) for their constructive feedback and support throughout. We are grateful to our collaborators, Sally Good (Evidence to Impact Ltd), and Lesley Walker and Yvonne Kerr (NHS Lothian) for their support of the project. We would like to thank our colleagues Laura Sharp, Elaine MacLennan and Chris Read at Fast Forward, and Lesley Brogan and Brian Pringle at the West Lothian Drug and Alcohol Service, for helping us design content and bringing the STASH project to life. Thanks also to Richard Tibbitts and Boaz Yehezkel from Antbits for developing the STASH study website.
Thanks to our colleagues Susan Patterson, Rachel Wilson-Lowe, Julie Riddell and Kaye Ross at the MRC Social and Public Health Sciences Unit for their input to the project, and Maija Hirvonen for her analysis of the social media component.
We are indebted to all the young people and professionals who gave their time and expertise at our stakeholder consultations and events. We thank all the students in the study schools who gave their time to participate in the evaluation. Finally, we thank the PSs, their contact teachers and senior management teams, for their enthusiasm and commitment throughout.
KRM, LM, LMcD, CP, CB, MMcC, RF and SAS are supported by the UK’s MRC and the Scottish Government CSO at the MRC/CSO Social and Public Health Sciences Unit, University of Glasgow (MC_UU_12017/11, SPHSU11, MC_UU_12017/14 and SPHSU14). SAS and MMcC are also supported by a MRC Strategic Award (MC-PC-13027).
Contributions of authors
Kirstin R Mitchell (https://orcid.org/0000-0002-4409-6601) (Professor of Social Science and Public Health) was a co-principal investigator and designed the intervention and study, directed the research project, led the drafting and editing of the report, contributed to the writing of the report and undertook some of the qualitative data collection.
Carrie Purcell (https://orcid.org/0000-0002-2651-9201) (Research Fellow) led on the qualitative data collection and analysis, contributed to the design of the intervention and study, and contributed substantially to the writing of the report.
Ross Forsyth (https://orcid.org/0000-0002-0414-5640) (Project Manager) managed the study, led the quantitative data collection, contributed to the design of the intervention and study, and contributed to the writing of the report.
Sarah Barry (https://orcid.org/0000-0003-3039-8729) (Chancellor’s Fellow) planned and led the statistical analysis and interpretation, contributed to the study design, and contributed to the writing and editing of the report.
Rachael Hunter (https://orcid.org/0000-0002-7447-8934) (Associate Professor, Health Economics) led on the design analysis and interpretation of the health economics component, and contributed to the writing and editing of the report.
Sharon A Simpson (https://orcid.org/0000-0002-6219-1768) (Professor of Behavioural Sciences and Health) contributed to the development of the study, provided expertise in behaviour change, and contributed to the writing and editing of the report.
Lisa McDaid (https://orcid.org/0000-0002-7711-8723) (Professor of Social Sciences and Health) contributed to the development of the study, provided expertise in sexual health, provided expertise in co-production, and contributed to the writing and editing of the report.
Lawrie Elliot (https://orcid.org/0000-0001-7727-231X) (Professor of Social Sciences and Health) contributed to the development of the study, provided expertise in sexual health, and contributed to the writing and editing of the report.
Mark McCann (https://orcid.org/0000-0002-6100-1416) (Research Fellow) designed, analysed and interpreted the social network component, and contributed to the writing and editing of the report.
Kirsty Wetherall (https://orcid.org/0000-0003-0547-3184) (Trainee Biostatistician) undertook data analysis, and contributed to the writing and editing of the report.
Chiara Broccatelli (https://orcid.org/0000-0002-1289-174X) (Research Assistant) analysed and interpreted the social network component, and contributed to the writing and editing of the report.
Julia V Bailey (https://orcid.org/0000-0002-5001-0122) (Associate Professor in Primary Care) contributed to the development of the study, provided expertise in sexual health, provided expertise in social media, and contributed to the writing and editing of the report.
Laurence Moore (https://orcid.org/0000-0003-2182-823X) (Director of the MRC/CSO Social and Public Health Sciences Unit) was a co-principal investigator and designed the intervention and study, provided mentorship and support for research project, supported the drafting and editing of the report, and contributed to the writing of the report.
Publications
Forsyth R, Purcell C, Barry S, Simpson S, Hunter R, McDaid L, et al. Peer-led intervention to prevent and reduce STI transmission and improve sexual health in secondary schools (STASH): protocol for a feasibility study. Pilot Feasibility Stud 2018;4.
Hirvonen MK, Purcell P, Elliott L, Bailey JV, Simpson SA, McDaid L, et al. Peer-to-peer sharing of sexual health social media messages in a school-based intervention: opportunities and challenges identified in the STASH feasibility trial. J Med Int Res 2020; in press.
Data-sharing statement
We will make anonymised qualitative extracts plus raw quantitative data available to other researchers on request and will deposit the questionnaire data in an appropriate database, such as the University of Glasgow’s Enlighten database. Please send any requests to the corresponding author.
Data were collected and stored in accordance with the Data Protection Act 1998138 and (from May 2018) the European Union General Data Protection Regulation. At the point of data entry, participants were provided with a unique identifier, which protects their anonymity throughout the analysis process. A unique identifier was also assigned to participants in the process evaluation transcripts. Personal details were removed and stored separately from the participant data. A de-code key to the ID has been kept securely.
Digital interview recordings were stored on an encrypted, password-protected network drive, separately from identifying information. Transcription was undertaken by a specialist transcription service with whom the Social and Public Health Sciences Unit had an ongoing contractual arrangement, confidentiality agreement and relationship of trust. Following transcription, identifying information was removed. Anonymised transcripts printed for the purpose of analysis were stored in a locked cabinet and destroyed following the completion of analysis.
All data will be kept for at least 10 years, in line with University of Glasgow Research Governance Framework Regulations for clinical research. Data will be stored confidentially on password-protected servers maintained on the University of Glasgow network. Data integrity will be checked every 2 or 3 years. Further details on data management are described in a separate data management plan (see Report Supplementary Material 8).
We will make anonymised qualitative extracts plus raw quantitative data available to other researchers on request and will deposit the data in an appropriate database, such as the UK Data Archive.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health and Social Care.
References
- Lewis R, Tanton C, Mercer CH, Mitchell KR, Palmer M, Macdowall W, et al. Heterosexual practices among young people in Britain: evidence from three national surveys of sexual attitudes and lifestyles. J Adolesc Health 2017;61:694-702. https://doi.org/10.1016/j.jadohealth.2017.07.004.
- Sonnenberg P, Clifton S, Beddows S, Field N, Soldan K, Tanton C, et al. Prevalence, risk factors, and uptake of interventions for sexually transmitted infections in Britain: findings from the National Surveys of Sexual Attitudes and Lifestyles (Natsal). Lancet 2013;382:1795-806. https://doi.org/10.1016/S0140-6736(13)61947-9.
- Kirby DB, Laris BA, Rolleri LA. Sex and HIV education programs: their impact on sexual behaviors of young people throughout the world. J Adolesc Health 2007;40:206-17. https://doi.org/10.1016/j.jadohealth.2006.11.143.
- Macdowall W, Jones KG, Tanton C, Clifton S, Copas AJ, Mercer CH, et al. Associations between source of information about sex and sexual health outcomes in Britain: findings from the third National Survey of Sexual Attitudes and Lifestyles (Natsal-3). BMJ Open 2015;5. https://doi.org/10.1136/bmjopen-2015-007837.
- Tanton C, Jones KG, Macdowall W, Clifton S, Mitchell KR, Datta J, et al. Patterns and trends in sources of information about sex among young people in Britain: evidence from three National Surveys of Sexual Attitudes and Lifestyles. BMJ Open 2015;5. https://doi.org/10.1136/bmjopen-2015-007834.
- Ofsted . Not Yet Good Enough: Personal, Social, Health and Economic Education in Schools 2013.
- Frith E. Social Media and Children’s Mental Health: A Review of the Evidence. London: Education Policy Institute; 2017.
- Mercer CH, Tanton C, Prah P, Erens B, Sonnenberg P, Clifton S, et al. Changes in sexual attitudes and lifestyles in Britain through the life course and over time: findings from the National Surveys of Sexual Attitudes and Lifestyles (Natsal). Lancet 2013;382:1781-94. https://doi.org/10.1016/S0140-6736(13)62035-8.
- Family Planning Association . Sexually Transmitted Infections Factsheet 2016.
- Marston C, King E. Factors that shape young people’s sexual behaviour: a systematic review. Lancet 2006;368:1581-6. https://doi.org/10.1016/S0140-6736(06)69662-1.
- Wellings K, Johnson AM. Framing sexual health research: adopting a broader perspective. Lancet 2013;382:1759-62. https://doi.org/10.1016/S0140-6736(13)62378-8.
- Hensel DJ, Fortenberry JD. Understanding the association of sexual health to health equity and well-being in adolescent women. J Adolesc Health 2013;52. https://doi.org/10.1016/j.jadohealth.2012.05.017.
- Philpott A, Knerr W, Maher D. Promoting protection and pleasure: amplifying the effectiveness of barriers against sexually transmitted infections and pregnancy. Lancet 2006;368:2028-31. https://doi.org/10.1016/S0140-6736(06)69810-3.
- Halpern CT. Reframing research on adolescent sexuality: healthy sexual development as part of the life course. Perspect Sex Reprod Health 2010;42:6-7. https://doi.org/10.1363/4200610.
- Scottish Government . Respect and Responsibility, Sexual Health Strategy Second Annual Report 2008.
- Department of Health and Social Care (DHSC) . A Framework for Sexual Health Improvement in England 2013.
- Welsh Assembly Government . Sexual Health and Wellbeing Action Plan for Wales, 2010–2015 2010.
- Department of Health, Social Services and Public Safety . Sexual Health Promotion Strategy &Amp; Action Plan 2008–2013 2008.
- Scottish Government . The Curriculum for Excellence 2010.
- Scottish Government . Getting It Right for Every Child 2006.
- Scottish Government . Relationships, Sexual Health and Parenthood n.d. https://rshp.scot/ (accessed 11 April 2019).
- Bonell C, Jamal F, Harden A, Wells H, Parry W, Fletcher A, et al. Systematic review of the effects of schools and school environment interventions on health: evidence mapping and synthesis. Public Health Res 2013;1. https://doi.org/10.3310/phr01010.
- Jamal F, Bonell C, Wooder K, Blake S. Let’s talk about sex: gender norms and sexual health in English schools. Sex Health 2015;12:1-3. https://doi.org/10.1071/SH15010.
- Valente TW, Fosados R. Diffusion of innovations and network segmentation: the part played by people in promoting health. Sex Transm Dis 2006;33:23-31. https://doi.org/10.1097/01.olq.0000221018.32533.6d.
- Shepherd J, Kavanagh J, Picot J, Cooper K, Harden A, Barnett-Page E, et al. The effectiveness and cost-effectiveness of behavioural interventions for the prevention of sexually transmitted infections in young people aged 13–19: a systematic review and economic evaluation. Health Technol Assess 2010;14. https://doi.org/10.3310/hta14070.
- Owen J, Carroll C, Cooke J, Formby E, Hayter M, Hirst J, et al. School-linked sexual health services for young people (SSHYP): a survey and systematic review concerning current models, effectiveness, cost-effectiveness and research opportunities. Health Technol Assess 2010;14. https://doi.org/10.3310/hta14300.
- Oringanje C, Meremikwu MM, Eko H, Esu E, Meremikwu A, Ehiri JE. Interventions for preventing unintended pregnancies among adolescents. Cochrane Database Syst Rev 2016;2. https://doi.org/10.1002/14651858.CD005215.pub3.
- Lopez LM, Bernholc A, Chen M, Tolley EE. School-based interventions for improving contraceptive use in adolescents. Cochrane Database Syst Rev 2016;6. https://doi.org/10.1002/14651858.CD012249.
- Mason-Jones AJ, Sinclair D, Mathews C, Kagee A, Hillman A, Lombard C. School-based interventions for preventing HIV, sexually transmitted infections, and pregnancy in adolescents. Cochrane Database Syst Rev 2016;11. https://doi.org/10.1002/14651858.CD006417.pub3.
- Shepherd J, Harden A, Barnett-Page E, Kavanagh J, Picot J, Frampton GK, et al. Using process data to understand outcomes in sexual health promotion: an example from a review of school-based programmes to prevent sexually transmitted infections. Health Educ Res 2014;29:566-82. https://doi.org/10.1093/her/cyt155.
- Goesling B, Colman S, Trenholm C, Terzian M, Moore K. Programs to reduce teen pregnancy, sexually transmitted infections, and associated sexual risk behaviors: a systematic review. J Adolesc Health 2014;54:499-507. https://doi.org/10.1016/j.jadohealth.2013.12.004.
- Tolli MV. Effectiveness of peer education interventions for HIV prevention, adolescent pregnancy prevention and sexual health promotion for young people: a systematic review of European studies. Health Educ Res 2012;27:904-13. https://doi.org/10.1093/her/cys055.
- Stephenson J, Strange V, Allen E, Copas A, Johnson A, Bonell C, et al. The long-term effects of a peer-led sex education programme (RIPPLE): a cluster randomised trial in schools in England. PLOS Med 2008;5. https://doi.org/10.1371/journal.pmed.0050224.
- Mellanby AR, Newcombe RG, Rees J, Tripp JH. A comparative study of peer-led and adult-led school sex education. Health Educ Res 2001;16:481-92. https://doi.org/10.1093/her/16.4.481.
- Kim CR, Free C. Recent evaluations of the peer-led approach in adolescent sexual health education: a systematic review. Perspect Sex Reprod Health 2008;40:144-51. https://doi.org/10.1363/4014408.
- Sun WH, Miu HYH, Wong CKH, Tucker JD, Wong WCW. Assessing participation and effectiveness of the peer-led approach in youth sexual health education: systematic review and meta-analysis in more developed countries. J Sex Res 2018;55:31-44. https://doi.org/10.1080/00224499.2016.1247779.
- Harden A, Oakley A, Weston R. A Review of the Effectiveness and Appropriateness of Peer-delivered Health Promotion for Young People. London: Institute of Education, University of London; 1999.
- Green J. Peer education. Promot Educ 2001;8:65-8. https://doi.org/10.1177/102538230100800203.
- Orme J, Starkey F. Peer drug education: the way forward?. Health Education 1999;99:8-16. https://doi.org/10.1108/09654289910248472.
- Starkey F, Audrey S, Holliday J, Moore L, Campbell R. Identifying influential young people to undertake effective peer-led health promotion: the example of A Stop Smoking In Schools Trial (ASSIST). Health Educ Res 2009;24:977-88. https://doi.org/10.1093/her/cyp045.
- Smith MU, Dane FC, Archer ME, Devereaux RS, Katner HP. Students together against negative decisions (STAND): evaluation of a school-based sexual risk reduction intervention in the rural south. AIDS Educ Prev 2000;12:49-70.
- Bailey J, Mann S, Wayal S, Hunter R, Free C, Abraham C, et al. Sexual health promotion for young people delivered via digital media: a scoping review. Public Health Res 2015;3. https://doi.org/10.3310/phr03130.
- Levine D. Using technology, new media, and mobile for sexual and reproductive health. Sex Res Soc Policy 2011;8:18-26. https://doi.org/10.1007/s13178-011-0040-7.
- Swendeman D, Rotheram-Borus MJ. Innovation in sexually transmitted disease and HIV prevention: internet and mobile phone delivery vehicles for global diffusion. Curr Opin Psychiatry 2010;23:139-44. https://doi.org/10.1097/YCO.0b013e328336656a.
- Gabarron E, Wynn R. Use of social media for sexual health promotion: a scoping review. Glob Health Action 2016;9. https://doi.org/10.3402/gha.v9.32193.
- Kanuga M, Rosenfeld WD. Adolescent sexuality and the internet: the good, the bad, and the URL. J Pediatr Adolesc Gynecol 2004;17:117-24. https://doi.org/10.1016/j.jpag.2004.01.015.
- Guse K, Levine D, Martins S, Lira A, Gaarde J, Westmorland W, et al. Interventions using new digital media to improve adolescent sexual health: a systematic review. J Adolesc Health 2012;51:535-43. https://doi.org/10.1016/j.jadohealth.2012.03.014.
- Jones K, Eathington P, Baldwin K, Sipsma H. The impact of health education transmitted via social media or text messaging on adolescent and young adult risky sexual behavior: a systematic review of the literature. Sex Transm Dis 2014;41:413-19. https://doi.org/10.1097/OLQ.0000000000000146.
- Swanton R, Allom V, Mullan B. A meta-analysis of the effect of new-media interventions on sexual-health behaviours. Sex Transm Infect 2015;91:14-20. https://doi.org/10.1136/sextrans-2014-051743.
- Bailey JV, Murray E, Rait G, Mercer CH, Morris RW, Peacock R, et al. Interactive computer-based interventions for sexual health promotion. Cochrane Database Syst Rev 2010;9. https://doi.org/10.1002/14651858.CD006483.pub2.
- Yonker LM, Zan S, Scirica CV, Jethwani K, Kinane TB. ‘Friending’ teens: systematic review of social media in adolescent and young adult health care. J Med Internet Res 2015;17. https://doi.org/10.2196/jmir.3692.
- Gold J, Pedrana AE, Sacks-Davis R, Hellard ME, Chang S, Howard S, et al. A systematic examination of the use of online social networking sites for sexual health promotion. BMC Public Health 2011;11. https://doi.org/10.1186/1471-2458-11-583.
- Bull SS, Levine DK, Black SR, Schmiege SJ, Santelli J. Social media-delivered sexual health intervention: a cluster randomized controlled trial. Am J Prev Med 2012;43:467-74. https://doi.org/10.1016/j.amepre.2012.07.022.
- Jones K, Baldwin KA, Lewis PR. The potential influence of a social media intervention on risky sexual behavior and chlamydia incidence. J Community Health Nurs 2012;29:106-20. https://doi.org/10.1080/07370016.2012.670579.
- Gold J, Pedrana AE, Stoove MA, Chang S, Howard S, Asselin J, et al. Developing health promotion interventions on social networking sites: recommendations from The FaceSpace Project. J Med Internet Res 2012;14. https://doi.org/10.2196/jmir.1875.
- Nguyen P, Gold J, Pedrana A, Chang S, Howard S, Ilic O, et al. Sexual health promotion on social networking sites: a process evaluation of The FaceSpace Project. J Adolesc Health 2013;53:98-104. https://doi.org/10.1016/j.jadohealth.2013.02.007.
- Campbell R, Starkey F, Holliday J, Audrey S, Bloor M, Parry-Langdon N, et al. An informal school-based peer-led intervention for smoking prevention in adolescence (ASSIST): a cluster randomised trial. Lancet 2008;371:1595-602. https://doi.org/10.1016/S0140-6736(08)60692-3.
- National Institute for Health and Care Excellence (NICE) . Smoking Prevention in Schools: Public Health Guideline [PH23] 2010.
- Rogers EM. Diffusion of preventive innovations. Addict Behav 2002;27:989-93. https://doi.org/10.1016/S0306-4603(02)00300-3.
- May C. Towards a general theory of implementation. Implement Sci 2013;8. https://doi.org/10.1186/1748-5908-8-18.
- Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ 2008;337. https://doi.org/10.1136/bmj.a1655.
- Forsyth R, Purcell C, Barry S, Simpson S, Hunter R, McDaid L, et al. Peer-led intervention to prevent and reduce STI transmission and improve sexual health in secondary schools (STASH): protocol for a feasibility study. Pilot Feasibility Stud 2018;4. https://doi.org/10.1186/s40814-018-0354-9.
- Harden KP. A sex-positive framework for research on adolescent sexuality. Perspect Psychol Sci 2014;9:455-69. https://doi.org/10.1177/1745691614535934.
- Kirby D, Short L, Collins J, Rugg D, Kolbe L, Howard M, et al. School-based programs to reduce sexual risk behaviors: a review of effectiveness. Public Health Rep 1994;109:339-60.
- Protogerou C, Johnson BT. Factors underlying the success of behavioral HIV-prevention interventions for adolescents: a meta-review. AIDS Behav 2014;18:1847-63. https://doi.org/10.1007/s10461-014-0807-y.
- Kelly JA. Popular opinion leaders and HIV prevention peer education: resolving discrepant findings, and implications for the development of effective community programmes. AIDS Care 2004;16:139-50. https://doi.org/10.1080/09540120410001640986.
- Audrey S, Cordall K, Moore L, Cohen D, Campbell R. The development and implementation of a peer-led intervention to prevent smoking among secondary school students using their established social networks. Health Educ J 2004;63:266-84. https://doi.org/10.1177/001789690406300307.
- Wight D, Wimbush E, Jepson R, Doi L. Six steps in quality intervention development (6SQuID). J Epidemiol Community Health 2016;70:520-5. https://doi.org/10.1136/jech-2015-205952.
- Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci 2011;6. https://doi.org/10.1186/1748-5908-6-42.
- Cane J, O’Connor D, Michie S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement Sci 2012;7. https://doi.org/10.1186/1748-5908-7-37.
- Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implement Sci 2010;5. https://doi.org/10.1186/1748-5908-5-69.
- Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol 2013;13. https://doi.org/10.1186/1471-2288-13-117.
- Ritchie J, Lewis J. Qualitative Research Practice: a Guide for Social Science Students and Researchers. London: SAGE Publications Ltd; 2003.
- Nilsen P. Making sense of implementation theories, models and frameworks. Implement Sci 2015;10. https://doi.org/10.1186/s13012-015-0242-0.
- Dobbie F, Purves R, McKell J, Bauld L, Dougall N, White J, et al. A Process Evaluation of the Implementation of ASSIST in Scotland: Final Report 2017. https://doi.org/10.1136/jech-2017-SSMAbstracts.188.
- Scottish Government . National Health and Wellbeing Outcomes 2017.
- Blake S, Emmerson L, Hayman J. Sex and Relationships Education (SRE) for the 21st Century. London: Brook/Sex Education Forum/PSHE Association; 2014.
- Gordon R, Gere D. Sex Squad: engaging humour to reinvigorate sexual health education. Sex Education 2016;16:324-36. https://doi.org/10.1080/14681811.2015.1120193.
- Barker G, Ricardo C, Nascimento M, Olukoya A, Santos C. Questioning gender norms with men to improve health outcomes: evidence of impact. Glob Public Health 2010;5:539-53. https://doi.org/10.1080/17441690902942464.
- Aggleton P, Campbell C. Working with young people – towards an agenda for sexual health. Sex Relatsh Ther 2000;15:283-96. https://doi.org/10.1080/14681990050109863.
- Fisher JD, Fisher WA. Changing AIDS-risk behavior. Psychol Bull 1992;111:455-74. https://doi.org/10.1037/0033-2909.111.3.455.
- Audrey S, Holliday J, Campbell R. It’s good to talk: an adolescent perspective of talking to their friends about being smoke-free. Soc Sci Med 2006;63:320-34. https://doi.org/10.1016/j.socscimed.2005.12.010.
- Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol 2000;55:68-7. https://doi.org/10.1037//0003-066x.55.1.68.
- Scottish Government . Saltire Awards n.d. https://saltireawards.scot/ (accessed 4 August 2020).
- Henderson M, Wight D, Raab G, Parkes A, Scott S, Hart G. Impact of a theoretically based sex education programme (SHARE) delivered by teachers on NHS registered conceptions and terminations: final results of cluster randomised trial. BMJ 2007;334. https://doi.org/10.1136/bmj.39014.503692.55.
- Turner RM, Thompson SG, Spiegelhalter DJ. Prior distributions for the intracluster correlation coefficient, based on multiple previous estimates, and their application in cluster randomized trials. Clin Trials 2005;2:108-18. https://doi.org/10.1191/1740774505cn072oa.
- Moore GF, Audrey S, Barker M, Bond L, Bonell C, Hardeman W, et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015;350. https://doi.org/10.1136/bmj.h1258.
- Ritchie J, Spencer L, Huberman AM, Miles MB. The Qualitative Researcher’s Companion. London: SAGE Publications Ltd; 2002.
- Girvan M, Newman ME. Community structure in social and biological networks. Proc Natl Acad Sci USA 2002;99:7821-6. https://doi.org/10.1073/pnas.122653799.
- Borgatti SP, Everett MG, Johnson JC, Zachary N. Analyzing social networks. J Math Sociol 2013;39:221-2. https://doi.org/10.1080/0022250X.2015.1053371.
- Snijders TAB, Van de Bunt GG, Steglich CEG. Introduction to stochastic actor-based models for network dynamics. Soc Networks 2010;32:44-60. https://doi.org/10.1016/j.socnet.2009.02.004.
- Steglich C, Snijders TAB, West P. Applying SIENA: an illustrative analysis of the coevolution of adolescents’ friendship networks, taste in music, and alcohol consumption. Methodol 2006;2:48-56. https://doi.org/10.1027/1614-2241.2.1.48.
- Snijders TAB. Stochastic actor-oriented models for network change. J Math Sociol 1996;21:149-72. https://doi.org/10.1080/0022250X.1996.9990178.
- Ripley RM, Snijders TAB, Boda Z, Vörös A, Preciado P. Manual for RSiena. Oxford: University of Oxford; 2011.
- Cook JA, Julious SA, Sones W, Hampson LV, Hewitt C, Berlin JA, et al. DELTA2 guidance on choosing the target difference and undertaking and reporting the sample size calculation for a randomised controlled trial. Trials 2018;19. https://doi.org/10.1186/s13063-018-2884-0.
- Bailey JV, Pavlou M, Copas A, McCarthy O, Carswell K, Rait G, et al. The Sexunzipped Trial: optimizing the design of online randomized controlled trials. J Med Internet Res 2013;15. https://doi.org/10.2196/jmir.2668.
- Tucker JS, Fitzmaurice AE, Imamura M, Penfold S, Penney GC, Teijlingen EV, et al. The effect of the national demonstration project Healthy Respect on teenage sexual health behaviour. Eur J Public Health 2007;17:33-41. https://doi.org/10.1093/eurpub/ckl044.
- Erens B, Phelps A, Clifton S, Mercer CH, Tanton C, Hussey D, et al. Methodology of the third British National Survey of Sexual Attitudes and Lifestyles (Natsal-3). Sex Transm Infect 2014;90:84-9. https://doi.org/10.1136/sextrans-2013-051359.
- Palmer MJ, Clarke L, Ploubidis GB, Wellings K. Prevalence and correlates of ‘sexual competence’ at first heterosexual intercourse among young people in Britain [published online ahead of print January 14 2019]. BMJ Sex Reprod Health 2019;45:127-37. https://doi.org/10.1136/bmjsrh-2018-200160.
- Mitchell KR, Mercer CH, Ploubidis GB, Jones KG, Datta J, Field N, et al. Sexual function in Britain: findings from the third National Survey of Sexual Attitudes and Lifestyles (Natsal-3). Lancet 2013;382:1817-29. https://doi.org/10.1016/S0140-6736(13)62366-1.
- Tennant R, Hiller L, Fishwick R, Platt S, Joseph S, Weich S, et al. The Warwick–Edinburgh Mental Well-being Scale (WEMWBS): development and UK validation. Health Qual Life Outcomes 2007;5. https://doi.org/10.1186/1477-7525-5-63.
- Robins RW, Hendin HM, Trzesniewski KH. Measuring global self-esteem: construct validation of a single-item measure and the Rosenberg Self-Esteem Scale. J Pers Soc Psychol Bull 2001;27:151-61. https://doi.org/10.1177/0146167201272002.
- Sawyer MG, Pfeiffer S, Spence SH, Bond L, Graetz B, Kay D, et al. School-based prevention of depression: a randomised controlled study of the beyondblue schools research initiative. J Child Psychol Psychiatry 2010;51:199-20. https://doi.org/10.1111/j.1469-7610.2009.02136.x.
- Moilanen KL. The adolescent self-regulatory inventory: the development and validation of a questionnaire of short-term and long-term self-regulation. J Youth Adolesc 2007;36:835-48. https://doi.org/10.1007/s10964-006-9107-9.
- Wu S, Crespi CM, Wong WK. Comparison of methods for estimating the intraclass correlation coefficient for binary responses in cancer prevention cluster randomized trials. Contemp Clin Trials 2012;33:869-80. https://doi.org/10.1016/j.cct.2012.05.004.
- National Institute for Health and Care Excellence (NICE) . Developing NICE Guidelines: The Manual 2014.
- Stevens K. Assessing the performance of a new generic measure of health-related quality of life for children and refining it for use in health state valuation. Appl Health Econ Health Policy 2011;9:157-69. https://doi.org/10.2165/11587350-000000000-00000.
- Edwards RT, Charles JM, Lloyd-Williams H. Public health economics: a systematic review of guidance for the economic evaluation of public health interventions and discussion of key methodological issues. BMC Public Health 2013;13. https://doi.org/10.1186/1471-2458-13-1001.
- Office for National Statistics (ONS) . Earnings and Hours Worked, Occupation by Four-Digit SOC: ASHE Table 14 2018.
- Curtis L, Burns A. Unit Costs of Health and Social Care 2017. Canterbury: PSSRU, University of Kent; 2017.
- NHS Improvement . NHS Improvement Reference Costs 2017–2018 2018. https://improvement.nhs.uk/resources/reference-costs/ (accessed 11 April 2019).
- Curtis L. Unit Costs of Health and Social Care 2013. Canterbury: PSSRU, University of Kent; 2013.
- Boots Company plc . Condoms &Amp; Sexual Health n.d. www.boots.com/health-pharmacy/condoms-sexual-health%20%20 (accessed 10 October 2018).
- Joint Formulary Committee . British National Formulary n.d. www.medicinescomplete.com (accessed 4 August 2020).
- Boots Company plc . Pregnancy Test n.d. www.boots.com (accessed 10 October 2018).
- Scottish Government . Curriculum for Excellence: Health and Wellbeing Experiences and Outcomes n.d. https://education.gov.scot/Documents/health-and-wellbeing-eo.pdf (accessed 11 April 2019).
- Johnson AM, Copas AJ, Erens B, Mandalia S, Fenton K, Korovessis C, et al. Effect of computer-assisted self-interviews on reporting of sexual HIV risk behaviours in a general population sample: a methodological experiment. AIDS 2001;15:111-15. https://doi.org/10.1097/00002030-200101050-00016.
- Delk J, Harrell MB, Fakhouri THI, Muir KA, Perry CL. Implementation of a Computerized tablet-survey in an adolescent large-scale, school-based study. J Sch Health 2017;87:506-12. https://doi.org/10.1111/josh.12521.
- Sekhon M, Cartwright M, Francis JJ. Acceptability of healthcare interventions: an overview of reviews and development of a theoretical framework. BMC Health Serv Res 2017;17. https://doi.org/10.1186/s12913-017-2031-8.
- Varghese B, Maher JE, Peterman TA, Branson BM, Steketee RW. Reducing the risk of sexual HIV transmission: quantifying the per-act risk for HIV on the basis of choice of partner, sex act, and condom use. Sex Transm Dis 2002;29:38-43. https://doi.org/10.1097/00007435-200201000-00007.
- Marston C, Lewis R. Anal heterosex among young people and implications for health promotion: a qualitative study in the UK. BMJ Open 2014;4. https://doi.org/10.1136/bmjopen-2014-004996.
- Stone N, Hatherall B, Ingham R, McEachran J. Oral sex and condom use among young people in the United Kingdom. Perspect Sex Reprod Health 2006;38:6-12. https://doi.org/10.1363/3800606.
- Information Services Division ISD of Scotland . Teenage Pregnancy: Year of Conception, Ending 31 December 2016 2018.
- Cullen BL, Wallace LA, Glancy ME, Shepherd J, Templeton K, Goldberg DJ. Genital Chlamydia and Gonorrhoea Infection in Scotland: Laboratory Diagnoses 2008–2017. Glasgow: Health Protection Scotland; 2018.
- Public Health England (PHE) . Contraception: Economic Analysis – Estimation of the Return on Investment (ROI) for Publicly Funded Contraception in England 2018.
- Scottish Government . Sexual Health and Blood Borne Virus Framework 2015–2020 Update 2015.
- Department for Education . Relationships Education, Relationships and Sex Education (RSE) and Health Education: Draft Statutory Guidance for Governing Bodies, Proprietors, Head Teachers, Principals, Senior Leadership Teams, Teachers 2019.
- White J, Hawkins J, Madden K, Grant A, Er V, Angel L, et al. Adapting the ASSIST model of informal peer-led intervention delivery to the Talk to FRANK drug prevention programme in UK secondary schools (ASSIST + FRANK): intervention development, refinement and a pilot cluster randomised controlled trial. Public Health Res 2017;5.
- Rogers EM. Diffusions of Innovations. New York, NY: Free Press; 2003.
- Byron P. Troubling expertise: social media and young people’s sexual health. Commun Res Pract 2015;1:322-34. https://doi.org/10.1080/22041451.2015.1110085.
- Byron P, Albury K, Evers C. ‘It would be weird to have that on Facebook’: young people’s use of social media and the risk of sharing sexual health information. Reprod Health Matters 2013;21:35-44. https://doi.org/10.1016/S0968-8080(13)41686-5.
- Bonell C, Fletcher A, Fitzgerald-Yau N, Hale D, Allen E, Elbourne D, et al. Initiating change locally in bullying and aggression through the school environment (INCLUSIVE): a pilot randomised controlled trial. Health Technol Assess 2015;19. https://doi.org/10.3310/hta19530.
- Coyle K, Basen-Engquist K, Kirby D, Parcel G, Banspach S, Collins J, et al. Safer choices: reducing teen pregnancy, HIV, and STDs. Public Health Rep 2001;116:82-93. https://doi.org/10.1093/phr/116.S1.82.
- Fonner VA, Kennedy CE, O’Reilly KR, Sweat MD. Systematic assessment of condom use measurement in evaluation of HIV prevention interventions: need for standardization of measures. AIDS Behav 2014;18:2374-86. https://doi.org/10.1007/s10461-013-0655-1.
- McCarthy O, Carswell K, Murray E, Free C, Stevenson F, Bailey JV. What young people want from a sexual health website: design and development of Sexunzipped. J Med Internet Res 2012;14. https://doi.org/10.2196/jmir.2116.
- Milward J, Khadjesari Z, Fincham-Campbell S, Deluca P, Watson R, Drummond C. User preferences for content, features, and style for an app to reduce harmful drinking in young adults: analysis of user feedback in app stores and focus group interviews. JMIR Mhealth Uhealth 2016;4. https://doi.org/10.2196/mhealth.5242.
- Aventin Á, Lohan M, O’Halloran P, Henderson M. Design and development of a film-based intervention about teenage men and unintended pregnancy: applying the Medical Research Council framework in practice. Eval Program Plann 2015;49:19-30. https://doi.org/10.1016/j.evalprogplan.2014.11.003.
- Great Britain . Data Protection Act 1998 1998.
- Blenkinsop S, Wade P, Benton T, Gnaldi M, Schagen S. Evaluation of the APAUSE Sex and Relationships Education Programme. Slough: National Foundation for Educational Research; 2004.
- Camp S, Askelson NM, Spies EL, Losch M. Caution, the use of humour may lead to confusion: evaluation of a video podcast of the Midwest Teen sex show. Am J Sex Educ 2010;5:201-16. https://doi.org/10.1080/15546128.2010.503857.
- Berkowitz AD. The Social Norms Approach: Theory, Research and Annotated Bibliography 2004. www.alanberkowitz.com/articles/social_norms.pdf (accessed 1 September 2020).
- Bandura A. Social cognitive theory: an agentic perspective. Annu Rev Psychol 2001;52:1-26. https://doi.org/10.1146/annurev.psych.52.1.1.
- Fisher WA, Fisher JD, Harman J, Suls J, Wallston KA. Social Psychological Foundations of Health and Illness. Oxford: Blackwell Publishing Ltd; 2003.
- Public Health Scotland . SHARE Education Resource 2016. www.healthscotland.com/documents/4946.aspx (accessed 4 August 2020).
- Brook . Pornography and Relationships n.d. www.brook.org.uk/your-life/pornography-and-relationships/ (accessed 13 May 2020).
Appendix 1 Intervention development tables
| Stage 1: evidence collation and synthesis | Key findings | Recommendations for intervention design |
|---|---|---|
| Scoping review |
Searched for existing digital media interventions for sexual health implemented in relatively closed social systems, such as schools; identified only one existing peer-led, school-based sexual health intervention41 (proposal 21). As with ASSIST, this used diffusion of innovation theory, but did not use social media. Other young people’s sexual health interventions have used social media, but not in schools using a school-based model48–52 Learning from three rigorously evaluated UK school-based interventions – SHARE (Scotland, teacher led), RIPPLE (England, peer led), Added Power and Understanding in Sex Education (APAUSE) (England, both) – indicated:Review contributed to mapping out key concepts to be operationalised (e.g. ‘competence’ at first sex, i.e. autonomous decision, both equally willing, right timing, contraceptive protection99) and preliminary topics into which intervention might be organised (e.g. ‘readiness’, ‘relationships’, ‘safety’, ‘consent’, ‘communication’, ‘diversity’, ‘online’, ‘pleasure’) Effective components of online interventions include: use of humour,78 although in moderation to limit potential confusion;140 social and emotional learning; interactive components; designs that consider participatory nature of social media and do not just approach it as a means of one-way dissemination of information130 |
Opportunities to capitalise on potential of social media are yet to be fully explored and harnessed. Development should explore most effective means of doing so, to diffuse change, from perspective of young people Explore potential to use same-age peers and how factual information might be packaged to enable young people to effectively deliver, with minimal ask of them. Explore how best to capitalise on informal interaction and how diffusion of positive messages might be embedded into these Limit self-selection of PSs by following nomination process used in ASSIST To organise and highlight relevance, intervention might be mapped into key topics or themes (e.g. ‘readiness’, ‘safety’). These should address reported gaps in young people’s sexual health knowledge (which tends to cluster around a limited range of STIs). Relevance of topics should be informed by collaborative development with young people Intention should be to address healthy relationships, as well as safer sexual behaviour; to create safe space for young people to develop their thinking about sex and relationships, and to practise communicating with one another about sex in a positive way; and to minimise ‘cringe factor’ associated with school SRE. Key values should include positive gender norms and sex positivity Use humour to deliver key messages in relatable way and maximise potential of social media by using in dynamic, interactive way, based on young people’s everyday usage (e.g. in a way that facilitates social support among PSs) |
| Theory review | Relevant theories identified: DoI,59 IT,60 SNT,141 SCT,142 SDT83 and IMB model.143 Based on these, intervention should address the following:
|
Intervention to include the following behaviour change techniques, derived from the theories identified:
|
| Review of grey literature, existing resources and social media platforms | Grey literature: identified broad parameters for intervention at national and local authority level, including high-level policy. Relevance for the STASH study as follows:
|
Overarching aims of intervention should include building confidence, responsibility and ownership, and inclusivity Intervention should address key concepts and concerns outlined in relevant education policies, so that it speaks to schools’ needs and thus becomes more amenable to embedding in school practice Intervention should align with outcomes of the Sexual Health and Blood Borne Virus Framework 2015–2020 Update strategy,126 not only around reduction of STIs but also positive attitudes, and addressing coercion and negative gender norms |
Resources: identified broad range of existing resources, with varied current relevance
|
Content should speak to current concerns of/for young people’s sexual well-being, including consent, ‘sexting’, pornography and the internet The STASH study website could be a curated collection of resources, rather than creating lots of new content Tone of content needs to balance authoritative with relatable and credible. In addition, the content should aim to be context appropriate (i.e. UK rather than USA) Consider whose voices included and in what format (e.g. links to Instagram/YouTube influencers could bring credibility, as could familiar formats, such as BuzzFeed-style lists) Could be scope to create some new content that addresses information gaps, as well as using or adapting what’s currently available |
|
Social media platforms: key functionality refined to ability to post web links and visual content, potential for closed (invite-only) groups and option for private messaging (to ask anonymous questions)
|
Facebook closed group may be best option for functionality (and requirements of research). Facebook may be the only feasible option, although acceptability to young people may have some limitations (to be explored in subsequent development activities) | |
| Young people (pre-study patient and public involvement and pre-pilot discussion groups) |
General: Topics:Proposed intervention: |
Intervention should pursue use of social media as an acceptable platform for peer leader role/diffusion Explore best use of a private group format to provide PSs with security about taking part in the role Consideration needs to be built in of how to engage and motivate boys as active PSs. Ensure relevance and encourage ownership of sexual health issues by different genders Explore means by which to circumvent local variations in language and embarrassment (e.g. visual representations of information) Consent should be included as key topic Intervention should aim to create space for young people to work on communication skills and confidence Explore ways in which the social media component might help with lack of discussion of SRE learning (creating space). Consider that discussion of some of these issues is not the norm, so intervention may be disrupting usual interaction Information should include prevalence of sexual activity, LGBTQ+ and gendering of attitudes around sexual behaviour Intervention should provide accurate information/evidence on young people’s sexual behaviour Content/ethos should aim to challenge negative norms, including those presented in some popular reality television shows Development should be cognisant of varying levels of maturity in target group (and difference by gender) In general, intervention needs to create a safe, supportive space for PSs to explore and discuss these ideas Clear processes and procedures should be in place for dealing with negative behaviour and sensitive disclosures (while also recognising the autonomy of the young people involved and that managing these, within reason, builds their confidence/capability, etc.) Need clear pathway for any students involved to speak to a teacher if needed (preferably one that they have an existing relationship with). Include clear parameters in terms of expectations on PSs about disclosures and what information they need to pass on to an adult Allow choice of medium for PSs – face-to-face or online communication – facilitating choice to encourage ownership To engage and motivate, need for format and content to be correctly pitched, but also engaging and snappy |
| Stakeholders |
|
Emphasise role of trainers as experts and as non-teachers Delivery needs to fit with S4 curriculum demands and must speak to schools’ needs and demands on them Include information that is not currently addressed in school-based SRE Encourage participation and engagement with inclusion of dynamic, interactive activities Ensure website includes list of sources of support and local services, as well as reliable information Focus on creating safe space for conversations, bearing in mind safeguarding concerns of schools and local authorities Procedures for monitoring and reporting child protection concerns should be developed in a written protocol Contact teacher should be designated in each school and should attend PS training. In addition, the contact teacher should contribute understanding on individual students’ potential vulnerabilities Extent to which schools can influence choice of supporters should be clarified and emphasised from beginning Alternative arrangements to lunchtime follow-up sessions should be explored to facilitate PS engagement |
| Professional workshop 1 |
|
Format needs a structure that includes the trainer in the group Schools/PSs should be encouraged to promote the intervention (e.g. at assembly) Intervention plans should consider variable resources available to PSs and not assume that all will have access to a smartphone Training should emphasise that PSs are only expected to signpost, not to know all the answers themselves Refine ambition of the intervention and clarify an overall ethos: embracing inclusivity, equality, diversity, being yourself, bodily autonomy and agency, gender neutrality of messages (as far as possible) Create safe space and encourage critical thinking in relation to sex and relationships; portrayals of ‘perfection’ on social media Include clear information on consent and communication |
| Stages of framework that explain change we intended to bring about | |||
|---|---|---|---|
| Theory | Purpose of approach | Key features (what the theory describes) | How we expected/intended this to be useful in STASH intervention development |
| Social systems (high-level) theory | |||
| Diffusion of innovation theory59 |
Broad scale explanation of how change occurs in social systems Provides overall theoretical grounding for intervention |
Over time, novel ideas and behaviours spread through social networks Effective when there is perceived advantage of new idea; compatibility with existing values, experiences and needs of early adopters; ease of understanding of new idea; and visibility of new behaviours in others Applicable in closed systems (e.g. school setting) Maintains focus on achievable change made relevant, accessible and visible to target population |
Would inform a key intervention mechanism, namely nomination of influential peers to act as ‘PSs’ Would highlight need for intervention objectives to be achievable for young people aged 14–16 years, and for intervention components and content to be relevant to needs and interests of target group, accessible to them (e.g. language, format) and visible in schools/among peer social networks, to explain how change would spread |
| Implementation theory60 |
Alerts to how embeddedness of an intervention in social system is achieved To foreground role of agency in implementation Complements diffusion of innovation theory, but shifts focus from characteristics of intervention and individuals onto relationships Moves beyond an individualist view, as presented in psychology theories of agency, to consider significance of collective action |
Comprises four key elements on which potential for embeddedness is contingent: Capability: alerts to significance of workability (as in the relationship between users and intervention components) and integration (i.e. ‘the capability of agents to operationalize a complex intervention depends on its workability and integration within a social system’) Capacity: ‘The incorporation of a complex intervention within a social system depends on agents’ capacity to co-operate and co-ordinate their actions’ Potential: ‘The translation of capacity into collective action depends on agents’ potential to enact the complex intervention’ Contribution: ‘The implementation of a complex intervention depends on agents’ continuous contributions that carry forward in space and time’ |
Would foreground the need to attend to dynamic elements of implementation context in the process of intervention development, for the intervention to be successful Would suggest that sustainability of the STASH study requires the following as either preconditions or elements that the intervention should build/address: |
| Individual behaviour change theory/theory informing specifics of intervention content | |||
| Social norms theory141 | To foreground significance of perceptions of behaviour of others in a social group or network in shaping behaviour |
(Mis)perceptions about behaviours within social groups shape member behaviour Addressing such misperceptions can facilitate behaviour change |
Would support potential of addressing key misconceptions about young people and sexual activity (i.e. that most 16-year-olds are sexually active) |
| Social cognitive142 | To highlight the impact on behaviour of observing behaviour of others | Reproduction of this behaviour is influenced by stages which are:
|
Would sensitise intervention development to the significance of sex and relationships factors, such as self-efficacy, provision of encouragement and reinforcement, social support, modelling behaviour, knowledge, skills and goal-setting |
| Self-determination theory83 | To explain intrinsic (self-) motivation to change, how that might be brought about | Three central concepts:
|
Would orient to the significance of young people’s perceptions of their own capabilities in the context of sex and relationships, and to the significance of engaging them in a way that makes them feel in control of intervention, connection and social cohesion with other PSs (complementing IT), and independence and ownership over intervention delivery |
| Information, motivation, behaviour theory81 | Explains key constructs required to engage in health behaviour and change | Three key components:
|
Would sensitise intervention development to the need to provide accurate information, motivation and to facilitate development of the relevant health behaviour skills Would facilitate and encourage social support through peer group and increased perception of self-efficacy (as with social cognitive theory) |
| Stage 2: co-production | Key findings and recommendations |
|---|---|
| Phase 1: website co-development |
Discussion of potential functionality and needs suggested that website should be created as follows: Level 1 (PSs) access, including options to set number of weekly topic areas containing shareable content; for users to mark topic areas as ‘completed’; for content to be shared via Facebook (or Facebook Messenger) custom URI scheme (via a Facebook connect app, although this may not be technically possible, no working example available); a ‘copy URL to clipboard’ function; ‘Ask a trainer’ function (via incorporation of a third-party open-source solution, such as Simple Forum); FAQ section Level 2 (trainers) as above, with the addition of a messaging feature that would allow communications to multiple PSs Level 3 (administration). Functionality to include a content management console [featuring ability to set access level (e.g. availability to non-logged-in users); create basic HTML page elements (images and text); use rich text editor, which allows quick creation of HTML content; place code snippets (e.g. embedded YouTube links, etc.); create a preview area, with both mobile and desktop preview environments]; a user management console (to include option to add, edit, remove and assign trainers); an analytics area (featuring ability to adjust report time period, graphs of user activity over time by school, as well as an overview and same data summarised in a tabular form); and an administer site content (e.g. FAQ area and other supplementary pages) |
| Content drafting |
Multiple iterations of the training manual and slides, follow-up sessions and website consent were drafted (led by KRM). Drafts explored various combinations of key themes (as identified in stage 1), revised and adapted relevant training activities from ASSIST, and explored potential inclusions of new material and activities identified in the review of existing resources (1.1.3) SRE expert review of a full draft suggested: |
| Young people development workshops |
|
| Stage 3: testing and optimising | Key findings and recommendations for intervention design |
|---|---|
| Pilot intervention |
|
| Pilot process evaluation |
Key findings: Feasibility: training delivered without any discipline issues and with high level of engagement from PSs Intervention acceptability (PSs, non-PS S4 students): training particularly successful regarding the more dynamic activities and helped by good rapport with trainers (especially by second day). Students tended to work better in smaller groups than all together. Barriers to engagement included unclear instructions and some embarrassment (e.g. when doing role-plays). Good overall group dynamic, no-one obviously excluded. Trainers worked flexibly and responded to issues arising in context. PSs expressed some ongoing reservations about interacting around the STASH study with students outside their immediate friend group Non-PS S4 students found that the topics and messages they were aware of to be broadly acceptable and relevant, and the intervention concept acceptable, but thought it might be more effective with a different group of PSs Intervention acceptability (trainers and teachers): trainers reported the training process and role to be acceptable to them. Each had engaged at some level on Facebook (primarily one trainer) and valued the opportunity to be involved in intervention development. Teachers felt that more advanced preparation of materials would allow more content to be worked through in the training sessions Teachers’ awareness of the intervention was extremely limited, with only the contact teacher (of the three interviewed) having much familiarity. Informal feedback on the training and follow-ups suggested that these were acceptable, although, again, awareness and involvement was minimal. None had seen the STASH study website Evaluation methods acceptability: trainers and teachers were happy to take part in interviews, although there was limited awareness and familiarity with the project among the latter. Some PSs more reluctant and only three non-PS S4 students volunteered and turned up on the day (could reflect relatively limited engagement and awareness of the STASH study beyond the PS group) Non-PS S4 students reported baseline questionnaire to be quite ‘intense’ and they were made uneasy by adults patrolling the room. Teachers expressed some surprise and discomfort at outcome questions they had seen on screen (reflected on how comfortable they would have felt responding to the questions) Context: this year group happened to have two large friend groups (one male, one female) that all PSs came from, so groups were already friends and known to each other (result of this is little reach beyond PSs) Reach: non-PS S4 participants felt that there was secrecy from PSs about what they were doing in the STASH study [i.e. did not tell them much; little awareness across year group (even for them as friends of PSs); Facebook group interaction mostly among other PSs and not the wider year]. Teachers, likewise, suggested reach was limited and they knew little about it, other than the contact teacher Fidelity: challenging to assess, other than that training was delivered largely as designed (although research team were still making modifications as it progressed) PSs did not post many messages and few had face-to-face conversations (suggests that if there was any change indicated between baseline and follow-up, it would probably be for PSs as a result of the training, not delivery of the intervention per se). What they did post was as intended, not adapted or reworded Recruitment and retention: overall, 17 of 19 PSs stayed involved throughout. According to the teachers, the two who left were ‘quieter’ and felt that it was not for them Regarding ongoing engagement, PSs tended to forget to post until prompted by trainers [i.e. trainers posted something from website to trainer page, they copied and pasted from that (or from each other)]. There were not that many visits to the site itself (in part explained by technical problems) Non-PS S4 students did not think PSs selected were necessarily best for the job and they would have chosen differently if they knew what nomination was for. Examples provided included taking it as a joke/’skive’, not seriously maybe not being confident enough to talk about what we were asking them to Perceived impact: non-PS S4 students did not perceive impact for themselves, but surmised possible impact for PSs. Some quite enjoyed getting to talk about and ‘learn about it all’ No issue with integration into everyday school life (in part because awareness so low) Unintended consequences: none raised Recommendations: |
| Professional workshop 2 |
Following overview of findings from 3.1, queries raised around: Reach: might result in most vulnerable students being excluded from the intervention due to recruitment process (including young people with lower literacy and additional support needs). Inadvertent recruitment of friendship groups could result in intervention being perceived as ‘cliquey’ and harder for non-PSs to become integrated. There is potential for a lack of viability of intervention among teachers and wider year group How best to measure the reach and impact of intervention: need to do as much as possible to ensure we are trying to reach and engage the most vulnerable young people in the year. Increase the percentage of nominated students in the year group who are invited to take part, to broaden potential uptake and participation Engagement: lack of sharing online and offline. Perceived (by S4 students) relevance of the intervention and content and how this may have an impact on engagement and sharing of messages. Emphasised the need to motivate PSs and for them to feel a sense of ownership over the intervention Encourage school engagement by emphasising with school staff the potential link to health and well-being indicators (i.e. the relevance and potential benefit for them, as well as students) PS training: expectations on PSs, particularly concerning face-to-face engagement. Intervention design needs to be cognisant of the range of barriers to transferring knowledge about sexual health. There is need for clear guidance and support for PSs, including those with low literacy or additional support for learning needs. As above, PSs emphasised the need for clear articulation of the PS role, with no expectation on them to be advisers (beyond what they would normally do with friends) Website: ensure relevance of content. if the whole year group given access, would this ‘dilute’ intervention, shift focus away from peer influence and locus of power out of the hands of PSs? Some thought this would improve reach and accessibility of information to those who may be excluded. There should be quality assurance of sources and content promoted. The design process should explore synergies with other message providers to develop coherence between messages provided in sex education lessons and the STASH study. Explore the potential to add search function and FAQs to website Explore potential synergies with other message providers. Congruence with messages provided in sex education lessons and the STASH study would be ideal, although potentially not currently feasible as development of new national SRE resources are still in development at the time STASH was implemented. They are now available at URL: https://rshp.scot/ (last accessed 7 August 2020) |
| Intervention delivery partner meetings |
|
| Website testing (young people) |
|
| Phase 2 web development | Drew on all the above findings and recommendations
|
| Ad hoc consultation meetings |
|
Appendix 2 STASH study website screenshots
The following screenshots illustrate the design and functions of the STASH study website. This includes links to websites, embedded videos, memes and quizzes.
The STASH study welcome screen (mobile phone)
Topic 7: are pictures and porn OK?
Topic 8: how to feel good about myself
Example of a peer supporter sharing a message on Facebook
Conversation with a trainer on Facebook
Example of resources developed and shared by a peer supporter
Appendix 3 Social network analysis tables
Parameter estimates and standard errors of the meta-analysis for the six friendship networks
| Parameter | Effect size | SE | Fisher’s combination test p-value | |
|---|---|---|---|---|
| Left, one sided | Right, one sided | |||
| Network effect | ||||
| Density | –4.87 | 0.53 | 1 | < 0.001 |
| Reciprocity | 3.30 | 0.15 | < 0.001 | 1 |
| Transitivity | 2.27 | 0.07 | < 0.001 | 1 |
| Reciprocity × transitivity | –1.65 | 0.15 | 1 | < 0.001 |
| Indegree – popularity (sqrt) | –0.37 | 0.07 | 1 | < 0.001 |
| Indegree – activity (sqrt) | –1.00 | 0.15 | 1 | < 0.001 |
| Outdegree – activity (sqrt) | 1.56 | 0.12 | < 0.001 | 1 |
| Ego effects: gender and PS status | ||||
| Gender ego | 0.17 | 0.08 | 0.02 | 0.95 |
| PS status ego | –0.34 | 0.19 | 1 | < 0.001 |
| Alter effects: gender and PS status | ||||
| Gender alter | –0.10 | 0.06 | 0.95 | 0.16 |
| PS status alter | –0.26 | 0.14 | 1 | < 0.001 |
| Similarity effects: gender and PS status | ||||
| Same gender | 0.31 | 0.06 | < 0.001 | 1 |
| Same PS status | –0.46 | 0.10 | 1 | < 0.001 |
| Selection: effect of sexual experience on friendship formation | ||||
| Sex.var alter | 0.01 | 0.06 | 0.29 | 0.73 |
| Sex.var squared alter | 0.04 | 0.10 | 0.39 | 0.59 |
| Sex.var ego | –0.01 | 0.11 | 0.42 | 0.51 |
| Sex.var diff. squared | 0.00 | 0.08 | 0.56 | 0.30 |
| Sex.var ego x sex.var alter | 0.00 | 0.16 | 0.51 | 0.37 |
| Influence: risk knowledge as outcome | ||||
| Rate of change, t1 to t2 | 1.48 | 0.22 | < 0.001 | 1 |
| Linear shape | 0.04 | 0.14 | 0.68 | 0.60 |
| Total risk knowledge similarity friends | 0.26 | 0.13 | 0.05 | 0.94 |
| Influence: confidence as outcome | ||||
| Rate of change, t1 to t2 | 0.92 | 0.19 | < 0.001 | 1 |
| Linear shape | 0.50 | 0.29 | < 0.001 | 1 |
| Total confidence similarity friends | 0.31 | 0.22 | 0.20 | 0.96 |
| Influence: PSs on knowledge risk and confidence as outcome | ||||
| Effect from RPS – risk knowledge | 0.02 | 0.42 | 0.58 | 0.55 |
| Effect from RPS – confidence | –0.17 | 0.58 | 0.71 | 0.50 |
| School | School size, n | NAPS, n (%) | RPS, n (%) |
|---|---|---|---|
| School 1 | 170 | 40 (24) | 24 (14) |
| School 2 | 100 | 28 (28) | 12 (12) |
| School 3 | 183 | 40 (22) | 19 (10) |
| School 4 | 45 | 12 (27) | 7 (16) |
| School 5 | 135 | 31 (23) | 22 (16) |
| School 6 | 123 | 26 (21) | 7 (6) |
| Whole sample | 756 | 177 (23) | 91 (12) |
| School | Direct reach, n (%)a | Direct reach, n (%)b | Indegree | Two-step reach centrality | Eigenvector centrality, mean (SD) | ||
|---|---|---|---|---|---|---|---|
| Mean (SD) | Range | Mean (SD) | Range | ||||
| NAPS | |||||||
| School 1 | 82 (63) | 10 (83) | 4.7 (2.4) | 0–11 | 0.17 (00.4) | 0.08–0.26 | 0.21 (0.28) |
| School 2 | 42 (58) | 5 (100) | 5.8 (2.7) | 2–13 | 0.25 (00.7) | 0.11–0.40 | 0.24 (0.32) |
| School 3 | 48 (34) | 9 (81) | 5.5 (2.2) | 1–13 | 0.16 (00.2) | 0.09–0.28 | 0.20 (0.22) |
| School 4 | 27 (82) | 3 (50) | 3.6 (1.8) | 1–6 | 0.42 (00.8) | 0.11–0.64 | 0.28 (0.26) |
| School 5 | 49 (47) | 6 (50) | 5.3 (2.8) | 1–12 | 0.19 (00.8) | 0.10–0.33 | 0.46 (0.34) |
| School 6 | 54 (56) | 6 (45) | 5.4 (2.4) | 1–11 | 0.20 (00.4) | 0.10–0.33 | 0.10 (0.24) |
| Whole sample | 302 (52) | 39 (68) | 5.2 (2.5) | 0–13 | 0.21 (00.5) | 0.08–0.64 | 0.23 (0.28) |
| RPS | |||||||
| School 1 | 52 (36) | 6 (50) | 5 (2.5) | 0–9 | 0.18 (0.05) | 0.09–0.26 | 0.25 (0.28) |
| School 2 | 28 (32) | 4 (80) | 5.7 (2.4) | 2–11 | 0.24 (0.04) | 0.19–0.36 | 0.27 (0.36) |
| School 3 | 52 (32) | 6 (55) | 5.8 (2.2) | 2–10 | 0.19 (0.05) | 0.10–0.28 | 0.19 (0.20) |
| School 4 | 23 (61) | 2 (33) | 3.8 (1.6) | 1–6 | 0.46 (0.09) | 0.36–0.60 | 0.30 (0.24) |
| School 5 | 49 (43) | 6 (50) | 5.8 (2.8) | 1–12 | 0.20 (0.05) | 0.13–0.33 | 0.47 (0.22) |
| School 6 | 7 (22) | 6 (45) | 4.6 (2.7) | 1–8 | 0.16 (0.04) | 0.10–0.23 | 0.05 (0.11) |
| Whole sample | 229 (34) | 30 (53) | 5.3 (2.5) | 0–12 | 0.22 (0.09) | 0.09–0.60 | 0.26 (0.27) |
| School, n (%) | Whole sample, n (%) | ||||||
|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | ||
| Total in respondent network | 181 | 104 | 189 | 53 | 143 | 128 | 618 |
| Gender | |||||||
| Male | 54 (30) | 41 (39) | 71 (39) | 17 (32) | 51 (36) | 31 (24) | 265 (43) |
| Female | 87 (48) | 54 (52) | 94 (48) | 2 (4) | 71 (47) | 28 (22) | 336 (54) |
| Other | 5 (3) | 0 | 5 (3) | 0 | 2 (1) | 0 | 12 (2) |
| Missing | 35 (19) | 9 (9) | 16 (8) | 34 (64) | 19 (13) | 69 (54) | |
| PSs | |||||||
| No | 126 (86) | 78 (82) | 152 (87) | 18 (95) | 111 (90) | 55 (93) | 540 (87) |
| Yes | 20 (14) | 17 (18) | 23 (13) | 1 (5) | 13 (10) | 4 (7) | 78 (13) |
| Statistic | School | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | |||||||
| Time 1 | Time 2 | Time 1 | Time 2 | Time 1 | Time 2 | Time 1 | Time 2 | Time 1 | Time 2 | Time 1 | Time 2 | |
| Network measure | ||||||||||||
| Density | 0.018 | 0.013 | 0.039 | 0.035 | 0.023 | 0.018 | 0.038 | 0.019 | 0.023 | 0.021 | 0.025 | 0.028 |
| Mean degree | 3.171 | 2.343 | 4.048 | 3.587 | 4.291 | 3.291 | 2 | 1 | 3.301 | 2.993 | 3.211 | 3.508 |
| Number of ties | 574 | 424 | 421 | 373 | 811 | 622 | 106 | 53 | 472 | 428 | 411 | 449 |
| Missing fraction | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Tie changes from t1 to t2 | ||||||||||||
| Absent unchanged 0 → 0 | 31,793 | 10,125 | 34,449 | 2611 | 19,618 | 15,589 | ||||||
| Ties created 0 → 1 | 213 | 166 | 272 | 39 | 216 | 256 | ||||||
| Ties deleted 1 → 0 | 363 | 214 | 461 | 92 | 260 | 218 | ||||||
| Present unchanged 1 → 1 | 211 | 207 | 350 | 14 | 212 | 193 | ||||||
| Hamming distance | 513 | 360 | 668 | 63 | 446 | 447 | ||||||
| Jaccard coefficient | 0.268 | 0.353 | 0.323 | 0.097 | 0.308 | 0.289 | ||||||
Appendix 4 Primary outcomes by exposure
| All | Trained PS | Exposed student | Unexposed student | ||
|---|---|---|---|---|---|
| Oral sex ever | Nobs (Nmiss) | 573 (38) | 87 (5) | 259 (9) | 227 (24) |
| Yes, n (%) | 167 (29.1) | 30 (34.5) | 71 (27.4) | 66 (29.1) | |
| No, n (%) | 406 (70.9) | 57 (65.5) | 188 (72.6) | 161 (70.9) | |
| Most recent oral sex | Nobs (Nmiss) | 164 (3) | 30 (0) | 70 (1) | 64 (2) |
| Last 6 months, n (%) | 122 (74.4) | 24 (80.0) | 51 (72.9) | 47 (73.4) | |
| More than 6 months, n (%) | 42 (25.6) | 6 (20.0) | 19 (27.1) | 17 (26.6) | |
| Oral sex for first time in last 6 months | Nobs (Nmiss) | 121 (1) | 24 (0) | 51 (0) | 46 (1) |
| Yes, n (%) | 37 (30.6) | 10 (41.7) | 15 (29.4) | 12 (26.1) | |
| No, n (%) | 84 (69.4) | 14 (58.3) | 36 (70.6) | 34 (73.9) | |
| Use of condom/dental dam at last oral sex | Nobs (Nmiss) | 118 (4) | 23 (1) | 51 (0) | 44 (3) |
| Yes, n (%) | 14 (11.9) | 0 (0.0) | 7 (13.7) | 7 (15.9) | |
| No, n (%) | 104 (88.1) | 23 (100.0) | 44 (86.3) | 37 (84.1) | |
| Main reason for no condom/dental dam at last oral sex | Nobs (Nmiss) | 102 (2) | 22 (1) | 44 (0) | 36 (1) |
| Got carried away and forgot, n (%) | 18 (17.6) | 4 (18.2) | 7 (15.9) | 7 (19.4) | |
| Did not have one to hand, n (%) | 28 (27.5) | 5 (22.7) | 12 (27.3) | 11 (30.6) | |
| I/my partner did not think it was necessary, n (%) | 40 (39.2) | 10 (45.5) | 18 (40.9) | 12 (33.3) | |
| I/my partner did not know how to use one, n (%) | 1 (1.0) | 0 (0.0) | 1 (2.3) | 0 (0.0) | |
| I/my partner did not want to use one, n (%) | 10 (9.8) | 2 (9.1) | 4 (9.1) | 4 (11.) | |
| We had one but it broke, n (%) | 1 (1.0) | 0 (0.0) | 0 (0.0) | 1 (2.8) | |
| Other, n (%) | 4 (3.9) | 1 (4.5) | 2 (4.5) | 1 (2.8) | |
| Vaginal sex ever | Nobs (Nmiss) | 569 (42) | 87 (5) | 260 (8) | 222 (29) |
| Yes, n (%) | 120 (21.1) | 18 (20.7) | 54 (20.8) | 48 (21.6) | |
| No, n (%) | 449 (78.9) | 69 (79.3) | 206 (79.2) | 174 (78.4) | |
| Most recent vaginal sex | Nobs (Nmiss | 119 (1) | 18 (0) | 54 (0) | 47 (1) |
| Last 6 months, n (%) | 94 (79.0) | 15 (83.3) | 43 (79.6) | 36 (76.6) | |
| More than 6 months, n (%) | 25 (21.0) | 3 (16.7) | 11 (20.4) | 11 (23.4) | |
| Vaginal sex for first time in last 6 months | Nobs (Nmiss) | 94 (0) | 15 (0) | 43 (0) | 36 (0) |
| Yes, n (%) | 29 (30.9) | 4 (26.7) | 17 (39.5) | 8 (22.2) | |
| No, n (%) | 65 (69.1) | 11 (73.3) | 26 (60.5) | 28 (77.8) | |
| Use of condom at last vaginal sex | Nobs (Nmiss) | 94 (0) | 15 (0) | 43 (0) | 36 (0) |
| Yes, n (%) | 38 (40.4) | 10 (66.7) | 15 (34.9) | 13 (36.1) | |
| No, n (%) | 56 (59.6) | 5 (33.3) | 28 (65.1) | 23 (63.9) | |
| Main reason for no condom at last sex | Nobs (Nmiss) | 55 (1) | 5 (0) | 27 (1) | 23 (0) |
| Got carried away and forgot, n (%) | 13 (23.6) | 1 (20.0) | 4 (14.8) | 8 (34.8) | |
| Did not have one to hand, n (%) | 15 (27.3) | 1 (20.0) | 8 (29.6) | 6 (26.1) | |
| I/my partner did not think it was necessary, n (%) | 7 (12.7) | 1 (20.0) | 3 (11.1) | 3 (13.0) | |
| I/my partner did not know how to use one, n (%) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| I/my partner did not want to use one, n (%) | 4 (7.3) | 0 (0.0) | 1 (3.7) | 3 (13.0) | |
| We had one but it broke, n (%) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Both got tested for STIs and had another form of contraception, n (%) | 13 (23.6) | 2 (40.0) | 8 (29.6) | 3 (13.0) | |
| Other, n (%) | 3 (5.5) | 0 (0.0) | 3 (11.1) | 0 (0.0) | |
| Frequency of condom use for vaginal sex (last 3 months) | Nobs (Nmiss) | 91 (3) | 15 (0) | 43 (0) | 33 (3) |
| Always, n (%) | 27 (29.7) | 8 (53.3) | 10 (23.3) | 9 (27.3) | |
| Often, n (%) | 9 (9.9) | 0 (0.0) | 6 (14.0) | 3 (9.1) | |
| Sometimes, n (%) | 18 (19.8) | 4 (26.7) | 9 (20.9) | 5 (15.2) | |
| Never, n (%) | 37 (40.7) | 3 (20.0) | 18 (41.9) | 16 (48.5) | |
| Ever anal sex | Nobs (Nmiss) | 563 (48) | 83 (9) | 261 (7) | 219 (32) |
| Yes, n (%) | 29 (5.2) | 3 (3.6) | 11 (4.2) | 15 (6.8) | |
| No, n (%) | 534 (94.8) | 80 (96.4) | 250 (95.8) | 204 (93.2) | |
| Most recent anal sex | Nobs (Nmiss) | 27 (2) | 3 (0) | 11 (0) | 13 (2) |
| Last 6 months | 16 (59.3) | 2 (66.7) | 4 (36.4) | 10 (76.9) | |
| More than 6 months | 11 (40.7) | 1 (33.3) | 7 (63.6) | 3 (23.1) | |
| Always practising safe sex | Nobs (Nmiss) | 566 (45) | 81 (5) | 262 (7) | 223 (33) |
| Yes, n (%) | 72 (12.7) | 9 (11.1) | 35 (13.4) | 28 (12.6) | |
| No, n (%) | 494 (87.3) | 72 (88.9) | 227 (86.6) | 195 (87.4) | |
List of abbreviations
- 6SQuID
- Six Steps in Quality Intervention Development
- APAUSE
- Added Power and Understanding in Sex Education
- API
- application programming interface
- app
- application
- ASSIST
- A Stop Smoking In Schools Trial
- BISH
- best in sexual health
- CHU-9D
- Child Health Utility 9D
- CI
- confidence interval
- CSO
- Chief Scientist Office
- CT
- contact teacher
- CV
- curriculum vitae
- DHT
- deputy head teacher
- FSM
- free school meals
- HT
- head teacher
- ICC
- intracluster correlation
- IT
- implementation theory
- MRC
- Medical Research Council
- NICE
- National Institute for Health and Care Excellence
- OECD
- Organisation for Economic Co-operation and Development
- OR
- odds ratio
- PCA
- principal component analysis
- PEG
- Project Executive Group
- PS
- peer supporter
- QALY
- quality-adjusted life-year
- RIPPLE
- Randomised Intervention trial of PuPil-Led sex Education
- S4
- secondary 4
- S5
- secondary 5
- S6
- secondary 6
- SD
- standard deviation
- SIMD
- Scottish Index of Multiple Deprivation
- SNA
- social network analysis
- SRE
- sex and relationships education
- STAND
- Students Together Against Negative Decisions
- STASH
- Sexually Transmitted infections And Sexual Health
- STI
- sexually transmitted infection
- SWEMWBS
- short Warwick–Edinburgh Mental Well-Being Scale
- TMG
- Trial Management Group
- TSC
- Trial Steering Committee
Notes
-
STASH peer supporter questionnaire: version 5.1, final version given to PSs
-
STASH follow-up questionnaire: version 13.4 (19 February 2018), final; given to participants
-
STASH procedure reporting of child protection concerns in schools: version 2 (11 April 2017)
-
STASH procedures reporting of harms to the NIHR TSC: version 3.2 (4 April 2017), final
Supplementary material can be found on the NIHR Journals Library report page (https://doi.org/10.3310/phr08150).
Supplementary material has been provided by the authors to support the report and any files provided at submission will have been seen by peer reviewers, but not extensively reviewed. Any supplementary material provided at a later stage in the process may not have been peer reviewed.