

Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as award number NIHR129113. The contractual start date was in April 2020. The draft manuscript began editorial review in October 2022 and was accepted for publication in March 2024. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ manuscript and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this article.
Permissions
Copyright statement
Copyright © 2024 Evans et al. This work was produced by Evans et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This is an Open Access publication distributed under the terms of the Creative Commons Attribution CC BY 4.0 licence, which permits unrestricted use, distribution, reproduction and adaptation in any medium and for any purpose provided that it is properly attributed. See: https://creativecommons.org/licenses/by/4.0/. For attribution the title, original author(s), the publication source – NIHR Journals Library, and the DOI of the publication must be cited.
2024 Evans et al.
Chapter 1 Background
About this chapter
In this chapter, we present the context of the CHIMES review, outlining the problem being addressed, the rationale for the review and how it responds to gaps in the extent evidence base, and the review’s aim and research questions (RQs).
Care-experienced, looked-after and in care: key concepts and definitions
Care-experienced children and young people represent a diverse population. There is extensive variation in nomenclature internationally. 1 Historically, in the UK, individuals who have been in care have been defined as ‘looked after’. However, recently there has been a move away from this term, as it has the potential to perpetuate some of the reported stigma associated with being in care. 2 For example, the practice of looked after child reviews, or the common acronym of LAC, might have negative connotations of ‘lack’ or ‘lacking’. As such, it is increasingly common to use terms such as ‘children looked after’, with some third-sector organisations indicating that young people prefer the term ‘in care’. 3 In light of these considerations, in the CHIMES review, we use the term ‘care-experienced’.
Care-experienced children or young people can include those who have resided in kinship care, foster care, or residential care. 4 In some cases, they might also remain at home with a supervision requirement order. Centrally, there is formalised statutory involvement, usually resulting in the transferral of parental rights. Care experience can include those who are currently in care but can extend to include care leavers. Again, this group is largely defined by their continued rights to statutory provision. For example, in Germany, individuals from a range of care placements are entitled to legal assistance until 21 years of age, whereas in England they are entitled to relevant services up to 25 years. 4 In the CHIMES review, we classify care-experienced young people as those aged up to 25 years.
Most recent data for 2021 report that 88,115 children and young people are registered as being in statutory, local authority care in England and Wales. 5,6 This reflects a continued trend in the growth of the ‘looked-after’ population, despite fewer placement commencements as a consequence of COVID-19 lockdown measures. 5,6
Mental health and well-being among care-experienced children and young people
The mental health and well-being of care-experienced populations remains a significant public health and social care concern. 7 Almost 50% of individuals involved in the child welfare system have a diagnosable mental health condition,8 and they are nearly five times as likely to have at least one psychiatric diagnosis compared with the general population. 9 Care-experienced individuals are at an elevated risk of poor subjective well-being,10 and are more than four times as likely as their peers to attempt suicide. 11
Poor mental health potentiates the risk of a range of adverse outcomes across the life course. This includes limited physical health, increased criminality, lower levels of educational engagement and attainment, and lower rates of employment. 12–14 A 2020 UK longitudinal study reported that individuals with a history of foster and/or residential care had excess mortality in adulthood due to increased risk of self-harm, accidents and other mental health and behavioural disorders. 15
Mental health problems can also incur significant health and social care costs, often due to the associated risk of placement instability and breakdown. 16–18 This is a notable challenge given the context of increasing financial pressure on the social care system in the UK, with reports of increased demand, reduced budgets and rising unit costs. 19
Prioritising the mental health and well-being of care-experienced children and young people: current policies, interventions and research
There is a clear need to prioritise mental health and well-being provision for care-experienced children and young people. The UK policy context has demonstrated a strong commitment in this area, with the Department for Education and Department of Health and Social Care’s joint statutory guidance on the promotion of health and well-being for care-experienced children mandating that local authorities ensure the provision of timely and adequate care. 20 National Institute for Health and Care Excellence (NICE) recommendations have indicated the need to enhance intervention across a range of domains, particularly in regard to relationship-based support, training for carers, introduction of a therapeutic approach to working practices and the immediate availability of specialist support for individuals awaiting access to Child and Adolescent Mental Health Services (CAMHS). 21
There are, however, potential barriers to improving the availability and quality of interventions. For example, with regard to access to mental health services, there are often reported incidents of failure to identify need, overly stringent eligibility thresholds and withholding of care where there is not a stable placement. 22 There are also concerns about the lack of support for carers’ own well-being, arising from the stress associated with parenting children with complex mental health and behavioural needs. 23
Intervention research to support policy and guidance recommendations has generally been limited, with NICE guidance previously stating that the UK evidence base does not adequately serve this population. 21 However, while there continues to be a lack of intervention research conducted in the UK, there is a wealth of interventions evaluated internationally. These can be preventative or treatment based. They operate across a range of socioecological domains, often targeting the skills of children and young people;24–26 interpersonal relationships with peers, carers and other adults;27–31 the ethos and culture of social care teams (e.g. adoption of trauma-informed practices);32–34 and the availability of wraparound community and mental health services provided by child welfare systems. 35
Given the emergent evidence base for intervention in the UK context, which contrasts to a relatively large (if equivocal) evidence base internationally, there is a clear need to explore the potential transportability of international approaches to this context. To this end, there is scope for systematic reviews that synthesise evidence on the effectiveness of interventions, while also exploring the contexts in which they are evaluated. Such work would help researchers and policymakers to understand the extent to which the evidence base for interventions is transferrable beyond their immediate implementation and evaluation context.
Limitations of the evidence base: the need for a complex system informed systematic review
To date, there have been a number of systematic reviews offering syntheses of the international evidence base for mental health and well-being interventions targeting the care-experienced population. 36–50 This includes a 2021 NICE review of interventions to promote physical, mental and emotional health and well-being of care-experienced children, young people and care leavers. 51 The review informed specific NICE guideline recommendations to consider the implementation of interventions within the UK context. 21
There are limitations with existing reviews, both in terms of methodology and focus, which together provide a rationale for the current CHIMES study. Reviews have often been restricted to specific intervention packages (e.g. treatment foster care, TFC),37,52 intervention outcomes (e.g. externalising behaviours)43,44 or population subgroups and care placement types (e.g. foster care). 24,37,39,43,48,53 Reviews within the UK context have predominantly been non-systematic literature reviews that do not use a robust methodology. 36
Of central importance is that reviews tend to focus on the synthesis of outcomes, with only rudimentary treatment of intervention theory, context or process data. Equally, where comprehensive syntheses of evidence reporting barriers and facilitators to intervention implementation have been conducted, they have not been fully integrated with outcome data to understand and explain variations in effectiveness. 51,54 As a result, they offer limited insight as to whether the international evidence base might be applied to the UK context.
In response to these limitations, we sought to conduct an integrative review, drawing together theory, context, process, outcome and economic data, to understand which interventions are effective in which contexts and why. This is supported by recent advances in complex-systems thinking in systematic reviews,55,56 which operate on the assumption that interventions are system disruptions and so their effectiveness is contingent on the system in which they are implemented. 57–59
This approach is further justified by recommendations from methodological guidance related to intervention development and evaluation,60,61 notably recent updated Medical Research Council guidance. 62 These frameworks and models emphasise the need to prioritise intervention theory and understand the mechanisms through which interventions operate and interact with contextual conditions, as the activation of relevant causal pathways is inherent to an intervention’s success. There is also a focus on process evaluation to explore how context factors inform facilitators and inhibitors of implementation and structure how diverse stakeholders interact with interventions. 63
More recent developments in methodological guidance have considered intervention adaptation and the potential transferability of interventions across contexts. Frameworks and recommendations, including the ADAPT guidance,64 indicate the need to understand similarities and differences between contexts before evidence-based interventions are transported, to ensure that necessary adaptations are made in relation to local needs.
The importance of attending to contextual specificities, such as international variations in social and healthcare systems, is apparent from the example of Multidimensional Treatment Foster Care (MTFC) and Multi-System Therapy (MST), which demonstrate the complexities in replicating the positive effects of US-originated interventions in Sweden. 65 MST was not effective when replicated in the new context, as it was essentially equal to usual care, whereas MTFC demonstrated impact, as it combined components that are common in usual care in Sweden but are rarely delivered as an integrated suite of provision.
Review aims and research questions
The CHIMES review is a complex-systems informed, multimethod systematic review that aimed to synthesise extant international evidence on interventions addressing the mental health and well-being of care-experienced children and young people and consider the potential applicability of this evidence base in the UK context.
This research aim was addressed through the following RQs:
-
What are the types, theories and outcomes tested in mental health and well-being interventions for care-experienced children and young people?
-
What are the effects (including inequities and harms) and economic effects of interventions?
-
How do contextual characteristics shape implementation factors, and what are key enablers and inhibitors of implementation?
-
What is the acceptability of interventions to target populations?
-
Can and how might intervention types, theories, components and outcomes be related in an overarching system-based programme theory?
-
Drawing on the findings from RQ1 to RQ5, what do stakeholders think is the most feasible and acceptable intervention in the UK that could progress to further outcome or implementation evaluation?
Summary
In this chapter, we have considered the context for the CHIMES review and its aim to address limitations with the extant evidence base. The next chapter reports the methodology of the review.
Chapter 2 Methodology
About this chapter
In this chapter, we outline the methodology used in the CHIMES review. The methods were a priori defined in the protocol. 66 Amendments to the protocol are listed in Appendix 1. To date, there are no recommended reporting checklists for complex-systems-informed, multimethod systematic reviews. As such, we report the review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist. 67 Method-specific syntheses are reported in accordance with relevant checklists in associated publications: the evidence map68 is reported with reference to the PRISMA Extension for Scoping Reviews69 and the process evaluation synthesis is reported with reference to the ‘Enhancing transparency in reporting the synthesis of qualitative research’ statement. 70 Stakeholder engagement is reported in accordance with the short form Guidance for Reporting Involvement of Patients and the Public version 2 (GRIPP2). 71
Review design, research questions and work packages
The CHIMES review aimed to synthesise extant international evidence on interventions addressing the mental health and well-being of care-experienced children and young people. The RQs are presented in the previous chapter.
The review process was conducted in three phases. First, we constructed an evidence map charting key evidence gaps and clusters (RQ1). From here, with input from stakeholder consultation, we refined and confirmed the parameters of the review. Second, we conducted a systematic review with method-level syntheses (RQ2–4). Third, these method-level syntheses were integrated into a review-level synthesis (RQ5), which was the basis of further stakeholder consultation (RQ6). This work mapped on to five interrelated work packages (WPs):
-
WP0: study co-ordination and dissemination (RQ1–6)
-
WP1: searches, extraction and appraisal (RQ1–4)
-
WP2: intervention theories, context, implementation and acceptability (RQ1, RQ3, RQ4)
-
WP3: intervention effects (RQ2)
-
WP4: modelling of intervention theory (RQ5)
-
WP5: stakeholder consultation (RQ6)
The remainder of this chapter is structured to present the methodology linked to each of these WPs.
Work package 0: study co-ordination and dissemination (research questions 1–6)
The first WP co-ordinated the review, overseeing governance and protocol compliance, risk monitoring, stakeholder collaboration, output management and impact activities. It had a specific remit for ensuring the integration of subsequent WPs. While published after the commencement of the CHIMES review, the study co-ordination was supported by the TRANSFER Approach framework,72 which is a seven-stage model to encourage partnership between review teams and stakeholders to consider systematically and transparently the factors that impact the transferability of systematic review findings to a specified context.
CHIMES collaboration partnership: establishing review need and relevance
The review was a formal collaboration between Cardiff University, University of Bangor, University of Exeter and the Fostering Network in Wales. Our collaboration initially addressed stage one of the TRANSFER framework,72 which is to establish the need for a review. Meetings between the review team and the Fostering Network in Wales (2018–9) identified a paucity of evidence-based interventions supporting the mental health and well-being of care-experienced children and young people in Wales, despite an evident need. The application to the National Institute for Health and Care Research (NIHR) Public Health Research (PHR) funding panel for the CHIMES review was a product of these initial meetings.
Project advisory group
The review was overseen by a project advisory group, which comprised two academics, two policy and practice professionals and two foster carers. The advisory group convened at four key time points during the study:
-
On completion of the initial mapping of the research evidence to confirm the parameters of the review (month 6).
-
On completion of the process evaluation synthesis to reflect on the findings and undertake an initial exploration of how they might support the interpretation of the outcome evaluation synthesis (month 12).
-
To consider the content and structure of final stakeholder consultations (month 22).
-
To reflect on the review and explore opportunities for future intervention research (month 28).
Stakeholder consultations
We conducted stakeholder consultations in two phases. The first phase, undertaken within the first 12 months of the review, was to refine the review parameters after the evidence-mapping stage. The first phase included identifying key context factors in the UK social care system that should be prioritised in the conduct of the review, which is prescribed by stages 2 and 3 of the TRANSFER model. 72 The second phase, undertaken in the last 6 months of the review, was to interpret and reflect upon the review findings (WP5).
A summary of the three consultations undertaken during phase one is presented in Table 1. The first consultation was conducted with CASCADE Voices, a young people’s advisory research group comprising care-experienced individuals up to the age of 25 years. As the group was facilitated by a third-party organisation, we did not have specific details on the age or care history of participating members. Key discussion points confirmed that the synthesis needed to focus on the priority outcomes of well-being and suicide-related outcomes. It further identified key context factors in the UK that should be attended to and foregrounded as part of the process evaluation synthesis, notably around system identities and resources.
| Stakeholders | Structure of consultations | Summary of consultations | |
|---|---|---|---|
| Priority intervention types and outcomes | Key context factors | ||
| CASCADE Voices (28 May 2020) | Online consultation facilitated by the CASCADE Engagement Manager at Cardiff University; 8 young people aged up to 25 years | Need to prioritise positive constructs of well-being (e.g. self-care, resilience, self-worth) and suicide-related outcomes. Lack of structural-level interventions currently being implemented in UK | System identities: UK has a deficit model of care-experienced young people, with negative perception that poor mental health is simply attention seeking. As a result, there may be a lack of system support for implementing mental health and well-being promotion interventions |
| System resources: UK has long waiting lists and lack of resources for children and young people’s mental health. Funding mental health interventions may not be feasible | |||
| The Fostering Network in Wales Young Person Forum (17 February 2021) | Online consultation facilitated by the Fostering Network in Wales; 7 young people aged 16–26 years | Need to prioritise positive constructs of well-being and suicide-related outcomes | System culture: perception that US social care system more punitive than UK making it ‘frightening’ and ‘abusive’. May reduce young people’s receptiveness to engage with interventions developed in the US care system |
| System resources: perception that US has stronger emphasis on removing children from the family than the UK so have more resources to support out-of-home care. UK less likely to resource interventions to support foster carers | |||
| All-Wales Fostering Team Managers Forum (25 March 2021) | Online consultation facilitated by the Fostering Network in Wales; 17 foster carer managers | Need to prioritise well-being | System identities: concern about UK foster carers’ dual identity as parent and professional, and difficulty of balancing the role if having to deliver specialist trauma-informed approaches. May compromise perceived safety of care placement where young person is receiving a mental health intervention from a carer who is also a ‘parent’, potentially leading to increased breakdown in placements |
| System resources: concern about the availability and level of carer skill to deliver mental health and well-being intervention in the UK. International interventions that target foster carers may not be feasible in UK as suitable carers not funded and available. Lack of system support for carers, which may make it harmful if delivering mental health support ‘out of work’ hours | |||
A further two consultations were planned at this time but, as a consequence of the COVID-19 pandemic, these consultations were delayed until January–February 2021. One consultation was hosted with the Fostering Network in Wales Young Person Forum, which is a group of care-experienced young people who provide advice and guidance to the charity on their programmes of work. A second consultation was conducted with the All-Wales Fostering Team Managers Forum, which is also facilitated by the Fostering Network in Wales. The forum comprises a range of local authority and independent foster-care providers working in Wales. While these consultations were hosted as the review was in progress, they did help to confirm the scope and focus. They also extended and refined the key context factors to be explored.
It should be noted that, in our consultation with the Young Person Forum, young people queried why the review was considering the transportability of interventions across contexts, questioning why interventions were not being developed to meet the specific needs of care-experienced children and young people in the UK.
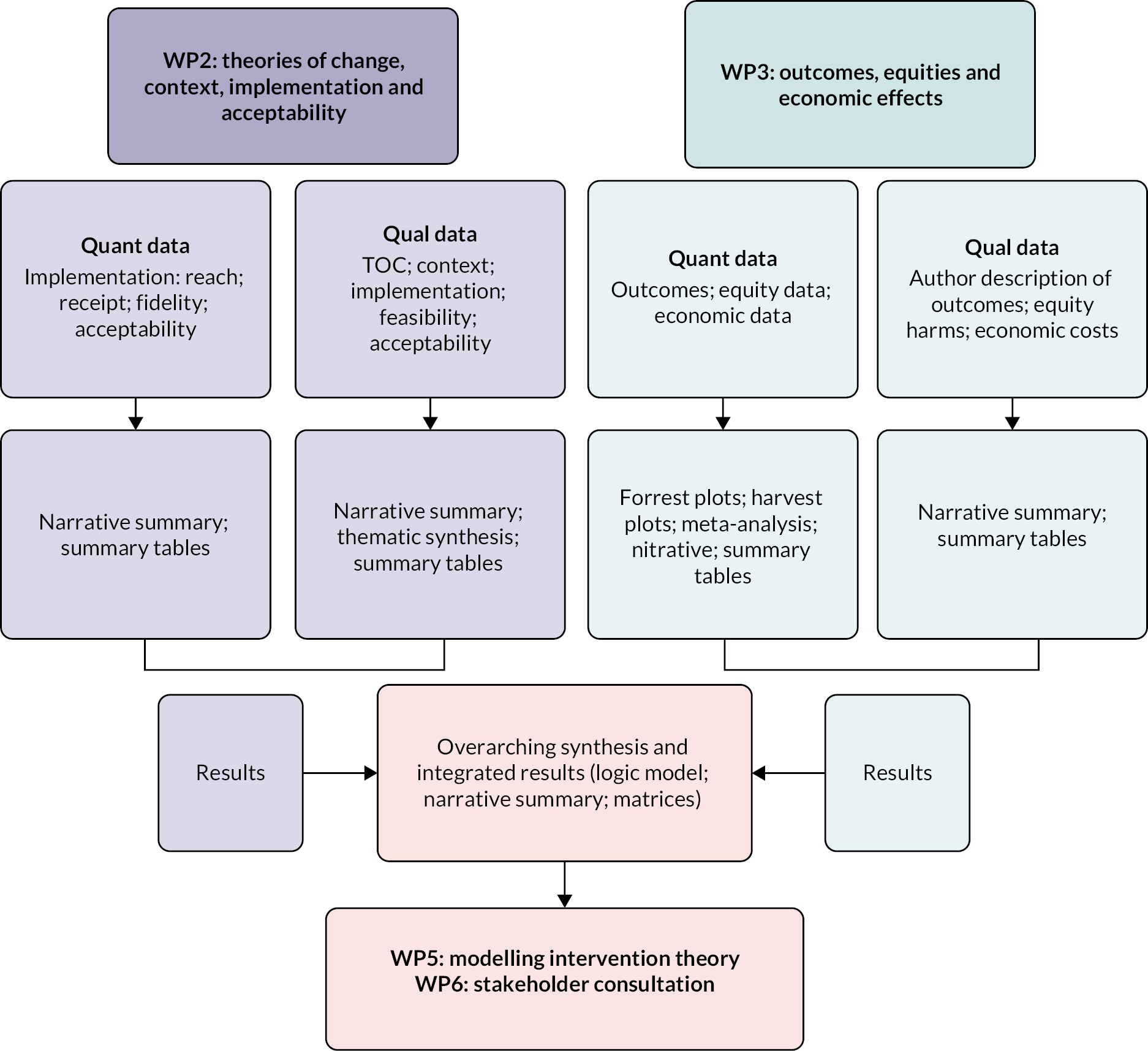
Convergent synthesis design
The review adopted a convergent synthesis design. 73,74 This approach entailed data from method-specific WPs being extracted, analysed and synthesised in a complementary manner, before being harmonised and integrated into an overarching review-level synthesis. RQs were designed to be complementary and contingent, where achieving a comprehensive answer to one question was dependent on the answers to other questions. Furthermore, when conducting the review, we (1) had the same members of the research team work on both the synthesis of qualitative and quantitative data; (2) screened all study types simultaneously and by the same members of the research team, storing data in EPPI-Reviewer version 4 (EPPI Centre, Social Science Research Unit, UCL Institute of Education, London, UK) to ensure ease of sharing of study data across syntheses and (3) used method specific appraisal tools that have been combined in previous reviews due to providing epistemological flexibility or consonance.
Work package 1: searches, extraction and appraisal (research questions 1–4)
Eligibility criteria
The inclusion parameters for the review are reported in accordance with the PICOS (population, intervention, comparison, outcomes and study) framework.
Types of participants
Intervention participants could be care-experienced children and young people or their proximal relationships, organisations and communities. For participating children and young people, they had to be aged ≤ 25 years. The upper limit of 25 years was selected as in the UK care leavers are eligible for statutory local authority support until this age. They could be currently placed in care, transitioning out of care or have previous care experience. The amount of time in care was not restricted. Care could include in-home and out-of-home care (foster care, residential care and formal kinship care). Care had to specify statutory involvement. For participating families, organisations and communities, they could be any individual or group. These could include but were not limited to carer, birth family, teacher or social worker. The following populations were excluded: general population, children in need, individuals at the edge of care, care without statutory involvement (e.g. informal kinship care), adoption, or unaccompanied asylum seekers and refugees.
Intervention
We defined interventions broadly, conceiving them as any attempt to disrupt existing system practices. They could be monocomponent or multicomponent and could operate across any of the following socioecological domains: intrapersonal, interpersonal, organisational, community and policy. Interventions could focus on prevention and/or management/reduction of symptomatology. Interventions did not necessarily have to be termed ‘mental health’ interventions; they could be interventions addressing education, social care, criminal justice or housing, provided that they included a relevant mental health outcome. There were no a priori criteria for implementation (i.e. delivery setting, delivery mode, delivery agent). Pharmacological interventions were excluded.
Comparator
For outcome evaluations, a comparator was required and could include treatment as usual, other active treatment or no specified treatment.
Outcomes
There were three domains of eligible outcomes, with interventions having to target one of these outcomes as a primary of secondary outcome:
-
Subjective well-being (eudaimonia and hedonia), life satisfaction and quality of life
-
Mental, behavioural or neurodevelopmental disorders as specified by the International Classification of Diseases, 11th Edition (ICD-11). The specific disorders were: neurodevelopmental; schizophrenia/primary psychotic; catatonia; mood; anxiety/fear-related; obsessive–compulsive disorder; stress; dissociation; feeding/eating; elimination; impulse control; disruptive/dissocial; personality; paraphilic; factitious; neurocognitive; mental/behavioural associated with pregnancy/childbirth
-
Self-harm; suicidal ideation; suicide
We made protocol amendments to outcomes at the stage of mapping study reports. First, quality of life was included as an explicit outcome. Second, the mental, behavioural or neurodevelopmental category was inductively classified into a set of subdomains that reflected the measurement domains and assessment tools reported in studies. These domains were: total social, emotional and behavioural problems; social–emotional functioning difficulties; internalising behaviour problems; externalising behaviour problems; depression; anxiety; stress and post-traumatic stress disorder (PTSD); attention and hyperactivity; attachment; psychosis. These domains are presented in more detail in the outcome synthesis reported in Chapter 4.
Outcome measures could be dichotomous, categorical or continuous. Domains of outcomes could be ascertained through clinical assessment, self-report or report by another informant (e.g. teacher). Outcomes had to be reported at the level of the child or young person. The following outcomes were excluded: substance misuse/substance use disorder; euthanasia or assisted suicide; accidental death (e.g. accidental overdose); biomedical markers of potential mental health problems (e.g. cortisol as an indicator of stress related disorder).
Study design
Different study designs were eligible according to the RQ being addressed:
-
Programme theory: described intended theory or mechanisms of effect. Could include mediation analysis or logic model.
-
Outcome evaluation: (individual/cluster) randomised controlled trials (RCTs) and quasi-experimental study designs (difference in difference; non-equivalent control groups). We excluded post measurement only or pre/post measurement in intervention group only.
-
Process evaluation: all qualitative and quantitative study designs. Included studies had to empirically report on implementation, relevant contextual influences and/or acceptability.
-
Economic evaluation: economic evaluations had to relate costs to benefits. They could report cost-minimisation, cost-effectiveness, cost–utility or cost–benefit analysis. They could be model or trial based. Decision-analytic models capturing intervention impacts on mental health and well-being were eligible.
Countries
Countries were limited to higher income countries as classified by the World Bank.
Information sources
We identified study reports from five information sources: (1) electronic bibliographic databases; (2) websites; (3) expert recommendations; (4) screening of relevant systematic reviews and (5) citation tracking of included study reports.
Databases
We searched 16 electronic bibliographic databases, covering a range of research disciplines, in May–June 2020 and again in April–May 2022. These databases were identified by the review team based on experiences of conducting related reviews.
The bibliographic databases were:
-
Applied Social Sciences Index and Abstracts
-
British Education Index
-
Child Development and Adolescent Studies
-
Cochrane Central Register of Controlled Trials
-
Cochrane Database of Systematic Reviews
-
Cumulative Index to Nursing and Allied Health Literature
-
Education Resources Information Center
-
EMBASE
-
Health Management Information Consortium
-
International Bibliography of the Social Sciences
-
MEDLINE (including MEDLINE in Process and MEDLINE ePub)
-
PsycInfo
-
Scopus
-
Social Policy and Practice
-
Sociological Abstracts (including Social Services Abstracts)
-
Web of Science (Social Sciences Citation Index, Conference Proceedings Citation Index Social Science and Humanities, Emerging Sources Citation Index).
Websites
We searched 22 websites of relevant social and healthcare organisations in May–June 2020 and again in April–May 2022. Again, these were identified by the review team based on their substantive and methodological expertise, combined with their experience of related systematic reviews:
-
Action for Children
-
Barnardo’s
-
Care Leavers’ Association
-
Catch-22
-
Child Poverty Action Group
-
Children’s Commissioner for four UK nations
-
Children’s Society
-
Department for Education
-
Early Intervention Foundation
-
Joseph Rowntree Foundation
-
Mental Health Foundation
-
Mind
-
National Children’s Bureau
-
Nurtureuk
-
Rees Centre
-
Samaritans
-
Spring Consortium
-
Thomas Coram Foundation
-
Young Minds.
Expert recommendation
We identified a total of 32 subject experts and 17 third-sector organisations. They were contacted via e-mail, inviting them to indicate any grey literature, unpublished research or ongoing studies of relevance.
Screening of relevant systematic reviews
We identified relevant systematic reviews to unpick and retrieve potential study reports for inclusion. Reviews were identified at the protocol development stage and through the searches of electronic bibliographic databases.
Citation tracking
We conducted forward and backward citation tracking of included study reports. To maximise resource efficiency, citation tracking prioritised identifying clusters of theory, context and process evaluations linked to included interventions to strengthen understanding of effects. We also placed an emphasis on citation tracking of evaluations conducted in the UK, as one of the central aims of the review was to consider the evidence base in relation to this context and initial searches revealed the predominance of study reports from the USA.
Search strategy
For bibliographic databases, we developed and tested a search strategy in OVID MEDLINE (see Appendix 2). It was adapted to the functionality of each bibliographic database. Search terms were clustered around the areas of: children; social care; mental health; well-being; study design. Where appropriate, subject headings were included in the search strategy. Searches were limited in date from 1990 to coincide with the ratification of the United Nations Convention on the Rights of the Child,75 which prescribes comprehensive social and healthcare provision for children internationally and started the proliferation of intervention in this area. No further limits were used within the search.
For websites, the search strategy depended on the functionality of the platform. Search terms focused on children and young people in care, mental health and well-being. These terms were searched through the website search function or Google advanced search, and in the absence of this functionality website pages and publication lists were screened for relevant study reports.
Selection process
We uploaded retrieved study reports to the EPPI-Centre’s specialist online review software EPPI-Reviewer version 4.0 for storage and management. The software stores the bibliographic details of each study report, including the abstract. For citations that progress to full text screening, the software enables the upload of related electronic documents.
We conducted screening of retrieved study reports in three stages. First, retrievals from electronic bibliographic databases and websites were screened to identify clearly irrelevant retrievals by checking the record title (e.g. animal testing of pharmacological treatment). To note, while the search strategy was designed for specificity and sensitivity, it did retrieve a large evidence base on older people’s social care. This stage was conducted by one member of the review team. Retrievals identified as clearly irrelevant were checked by a second reviewer. Where there was a conflict in decisions, the study report was marked as clearly relevant and progressed to the next stage of screening. Study reports identified through the other additional information sources were not assessed for relevance.
Second, we screened the title and abstracts of retrievals from almost all information sources independently and in duplicate. Where there was a conflict on exclusion, the study report progressed to the next stage of screening. At this stage, there was a 5% rate of conflict in decision-making. Expert recommendations were not screened at this stage as responses provided study reports specific to the review remit and generally needed consideration at full text in the first instance.
Third, we screened the full text of study reports from all information sources independently and in duplicate. Where there was a conflict, a decision was made through recourse to a third member of the research team. At this stage, there was a 13% rate of conflict, reflecting some of the complexities in deciding if the population (e.g. care-experienced or children in need) or outcome (e.g. self-esteem) was eligible for the review.
An inclusion criteria proforma guided the selection process (see Report Supplementary Material 1). The review protocol specified that the proforma would be tested and calibrated by two reviewers screening the title and abstracts of the same 50 references. Owing to the size and brevity of the available literature, we increased this to 117 references, which was more than 1% of the retrievals from the electronic bibliographic database and website searches. Three members of the review team test screened the sample, with each retrieval being screened by two reviewers. There was a 10% conflict rate. Discussion among the review team indicated that the inclusion criteria were clear, but that we needed to ensure familiarity with the agreed criteria. For example, this included the countries (e.g. higher income countries) that were eligible for the review. The inclusion criteria proforma was regularly reviewed, with any clarifications reported in an update to the review protocol.
Economic evaluation searches and study identification
While we conducted the aforementioned searches and selection, we progressed with searches for economic evaluations by unpicking a recent relevant review of economic evaluations of children and young people’s social care interventions conducted by authors of the CHIMES review. 76
The 20 study reports included in the economic evaluation review were assessed against the CHIMES review’s inclusion criteria. We screened titles and abstracts independently and in duplicate. Eighteen progressed to screening at full text. None were assessed to be eligible for the present review. Reasons for exclusion were: wrong population (n = 14); wrong outcome (n = 3); evaluation report could no longer be accessed (n = 1).
The original review had run searches until 2018. Using the review’s search strategy, we reran searches from 2018 to May 2020. This retrieved 3411 additional citations. Following de-duplication, we screened 1636 retrievals at title and abstract, with 42 progressing to full text screening. No study reports were identified as eligible. Reasons for exclusion were: wrong publication type (n = 4); wrong outcome (n = 3); wrong population (n = 33). Two study reports could not be accessed. Economic evaluations were also searched for in the main CHIMES review searches.
Evidence map, relationship between study designs and method-level syntheses
Following the identification of eligible study reports, we constructed an evidence map. From here, we assessed which study reports would be included in method specific syntheses.
To be included in the description of programme theories, interventions had to have an associated outcome evaluation.
For process evaluations, we constructed a classification which identified evaluations as either ‘conceptually and/or empirically thin’ or ‘conceptually and/or empirically rich’. Thin process evaluations had to have an associated outcome evaluation to be included. They often formed part of a mixed-method study report anddid not have a dedicated description of method. They also lacked transferrable data or interpretations that could help to understand the context of intervention implementation and acceptability more broadly. Rich process evaluations were included as stand-alone study reports in the process synthesis, regardless of whether there was a linked included outcome evaluation, as they provided potentially generalisable contextual insight into how interventions might interact with complex system characteristics.
To support classification of thin and rich process evaluations, we drew upon an existing review’s classification system for the sampling of qualitative research to develop an assessment tool77,78 (Table 2).
| CHIMES classification of process evaluations | Score | Definition |
|---|---|---|
| Conceptually and/or empirically rich | 4 | Empirical: a large amount and depth of qualitative data AND conceptual: substantial interpretation by the authors and consideration of the transferability of data |
| 3 | Empirical: a large amount and depth of qualitative data OR conceptual: substantial interpretation by the authors and consideration of the transferability of data | |
| Conceptually and/or empirically thin | 2 | Empirical: a small amount of qualitative data, often from a limited number of participants OR conceptual: lack of interpretation by authors, with data presented fairly descriptively, potentially using an analytical approach (e.g. simple thematic analysis) that does not facilitate theoretical insights |
| 1 | Empirical: a small amount of qualitative data, often from a limited number of participants AND conceptual: lack of interpretation by authors, with data presented fairly descriptively, potentially using an analytical approach (e.g. simple thematic analysis) that does not facilitate theoretical insights |
Owing to the scale of the review, we made an a priori decision that we would only include interventions targeting the intrapersonal and interpersonal level in the outcome synthesis if they were evaluated with a RCT study design. For interventions operating at the organisational, community and policy level (which were identified as priority areas but are typically less amenable to RCT study designs), we included all eligible evaluation study designs (e.g. RCT and non-RCT) in the outcome synthesis.
Economic evaluations did not have to have an associated outcome evaluation.
Data extraction and data items
Data extraction process
We developed and calibrated a standardised data extraction form in EPPI-Reviewer 4, with extraction items being converted into a coding tree that included selectable a priori defined items and free-text coding. The coding tree had different sets of codes for each RQ and study design. For each study design, two to three study reports were used to develop and calibrate the extraction form. Once confirmed, we coded a minimum of 10% of study reports independently and in duplicate. The remainder of the study reports were coded by one reviewer and checked for accuracy by a second reviewer. Discrepancies were resolved through discussion.
Review mapping, intervention characteristics and programme theory
In the first instance, we coded all eligible study reports as part of the evidence map. We extracted the following data items: country; publication date; intervention type according to socioecological domain; target population; intervention name; evidence type; study design; intervention outcome domains. As part of the convergent synthesis design, this mapping also served to structure the analysis undertaken as part of the subsequent process evaluation and outcome synthesis (e.g. grouping of outcomes for meta-analysis).
Intervention characteristics were coded in accordance with the Template for Intervention Description and Replication (TIDieR) checklist for intervention development. 79 We extracted intervention rationale, material provided to participants, procedures and activities, delivery agent, mode of delivery, location of delivery, period of delivery and dose, plan for personalisation or adaptation and modifications undertaken. These items were parent codes, with child codes being inductively coded from the study reports. In practice, descriptions of interventions provided limited detail.
For study reports presenting a programme theory, data extraction was guided by tools used in other reviews80 (see Report Supplementary Material 2). We extracted method or process for developing the theory, name of theory, discipline of theory, socioecological domain of theory, description of theory and how the theory is articulated (e.g. a logic model). These items were parent codes, with child codes being inductively developed from the study reports.
Process evaluation extraction tool
We used different extraction tools with thin and rich process evaluations. For thin-process evaluations, which included quantitative and mixed method data, we used generic codes for context, implementation and acceptability (see Report Supplementary Material 3). For rich-process evaluations, data extraction was informed by the context and implementation of complex interventions (CICI) framework to emphasise the prominence of context in the review81 (see Report Supplementary Material 3). We extracted: study characteristics; context, which was classified according to the CICI domains of epidemiological, sociocultural, political, legal, ethical, geographical and socioeconomic; implementation, which was classified according to the CICI domains of implementation theory/strategy, implementation agents and implementation outcomes (including reach, receipt and fidelity); and acceptability, which was coded according to participants, implementers, funders and other stakeholders. These items were parent codes, with child codes inductively developed from study reports. We extracted data from the results sections of studies, but also authors’ narratives and interpretations.
Outcome evaluation extraction tool
For outcome evaluations, both randomised and non-randomised study designs had the same parent codes for data extraction. These were: study design; population; study arms and duration; analysis; effectiveness outcomes; mediators; moderators. For each type of study design, the child codes were tailored. Under the study design parent code for RCTs, we extracted method of recruitment, method of randomisation, unit of randomisation, cluster randomisation, blinding, allocation sequence, allocation concealment, total sample size and power calculation (see Report Supplementary Material 4). For non-RCTs, owing to the diversity of study designs, generic child codes were included: study design, method of recruitment and total sample size (see Report Supplementary Material 5).
Equity harms extraction tool
We extracted equity harms from study reports that included moderator analysis or interaction effects. Harms were initially categorised according to the PROGRESS-Plus for equity harms:82 place; race/ethnicity; occupation; gender/sex; religion; education; socioeconomic status; social capital; discriminated characteristics; relationship features; time-dependent relationships. Subdomains were inductively coded from study reports. We extracted PROGRESS-Plus domain, equity subdomain, absolute effects and relative effects.
Economic evaluation extraction tool
For economic evaluations, data were intended to be extracted according to the Drummond checklist,83 with key data items being direct and indirect costs, perspective, structural and empirical inputs, time horizon and cost-effectiveness.
Missing data
Where data were incomplete or information (e.g. outcome measurements or primary data to calculate effect size) was missing and the data could not be located, we recorded it as missing and considered it in the risk of bias (RoB) assessment.
Quality assessment
Quality assessment process
We appraised the quality of each study report independently by two reviewers. Quality appraisal was undertaken in EPPI-Reviewer 4.
Programme theory quality appraisal tool
We appraised programme theory study reports using a tailored appraisal tool developed for a previous systematic review with a theory synthesis81 (see Report Supplementary Material 2). While the review focused on mapping intervention theories, quality appraisal was useful in considering the strength of intervention’s associated theories and the extent to which they could help inform future intervention development and adaptation. The quality domains assessed were: clarity: clarity of construct definition; clarity: clear pathway from inputs to outcomes; plausibility and feasibility: theorised pathways are plausible; plausibility and feasibility: empirical evidence in support of theory; testability: evidence of empirical testing of theory; ownership: theory developed with children and young people; ownership: theory developed with parents, carers, social care professionals and other stakeholders; generalisability: theory presented as general; generalisability: theory describes its application to different contexts; and generalisability.
We adapted the appraisal tool to meet the needs of the CHIMES review by including two ownership domains, whereas the original version included one. This was due to our awareness of extant research and practice, where the voices of care-experienced children and young people are rarely privileged. As such we wanted to have a clear assessment of the extent to which they were engaged in intervention development. Domains were rated according to a binary assessment of yes or no.
Process evaluation appraisal tool
We appraised qualitative data within rich process evaluations using a tool developed in a previous systematic review84 (see Report Supplementary Material 3). We made a global assessment of overall reliability/trustworthiness and overall trustworthiness. Rigour domains included: steps taken to increase rigour in sampling; steps taken to increase rigour in data collection; steps taken to increase rigour in the analysis of data; findings grounded in/supported by the data. Usefulness domains included: breadth and depth of study; study privileges the perspectives and experiences of children and young people; study privileges the perspectives and experiences of parents, carers, social care professionals and other stakeholders. Domains were rated as high, medium, low or unclear.
Randomised controlled trials appraisal tool
We appraised outcome evaluations that were conducted using a RCT study design using the Cochrane risk of bias tool for randomised trials (RoB 2)85 (see Report Supplementary Material 4). The quality domains assessed were: bias arising from the randomisation process; bias due to deviations from intended interventions; bias due to missing outcome data; bias in measurement of the outcome; and bias in selection of the reported result. Each domain has a number of signalling questions to inform assessment, which can be assessed as yes, probably yes, probably no, no, and no information. We judged the domains according to low RoB, some concerns and high RoB.
Non-randomised intervention studies appraisal tool
We appraised outcome evaluations using a non-randomised study design, or quasi-experimental design (QED), with the Cochrane Risk Of Bias In Non-randomized Studies – of Interventions (ROBINS-I)85 (see Report Supplementary Material 5). The quality domains assessed were: bias due to confounding; bias in selection of participants into the study; bias in the classification of interventions; bias due to deviations from the intended intervention; bias due to missing data; bias in measurement of outcomes; bias in the selection of the reported result. We judged the domains according to low risk, moderate risk, serious risk, critical risk and no information.
Economic evaluation appraisal tool
We did not formally assess economic evaluations with a quality appraisal tool, but the one retrieved partial evaluation was considered in relation to the items of the Drummond checklist,83 which covers the reporting of study design, data collection and analysis and interpretation of results.
Data synthesis
Mapping of evidence, intervention characteristics and theories
We used scoping review methods and systematic mapping guidance to support the mapping of the evidence base86–88 (Figure 1). Following the coding of study reports, we constructed numerical and narrative summaries of evidence clusters and gaps, accompanied by descriptive tables and infographics. For details on intervention characteristics, a narrative summary described the interventions in detail, with an accompanying table presenting a summary of extractable data according to the TIDieR framework. For the subset of interventions reporting on intervention theory, these were narratively summarised according to the socioecological domains in which the theories operated and accompanied by a summary table.
FIGURE 1.
Results-based convergent synthesis design.
Process evaluation synthesis
For thin-process evaluations, we constructed a narrative summary for the main domains of context, implementation and acceptability. This was accompanied by a summary table. For rich-process evaluations, we drew upon the principles of framework analysis and thematic analysis. 89–91 Analysis commenced with familiarisation of evaluations to become sensitised to within study and between study differences. We then developed a conceptual framework that integrated elements of process evaluations that might support explanation of intervention functioning: context, implementation and acceptability. Context and implementation were defined in reference to the CICI framework. 81 Study reports were then identified and coded according to this conceptual framework. Ten per cent were done independently and in duplicate, with the remainder coded and checked by one reviewer and verified by a second. The next stage was the charting of the coded, with study reports grouped according to context and how it related to implementation and acceptability. These categories formed the basis of initial themes or ‘context factors’ that went beyond the CICI framework and were more closely aligned with the data. The final stage was mapping and interpretation, which entailed transforming the initial themes into analytical themes, and generating new interpretive insights. For example, we transformed an initial theme related to the lack of time into a richer theme of ‘intervention burden’. This extended to include the cognitive, time and emotional burden linked to intervention delivery and engagement. The initial phase of stakeholder consultation supported this transformation. We presented the synthesis narratively, with a summary table reporting study report characteristics and the key context factors presented at the individual-study level.
Outcome evaluation synthesis
We constructed a narrative summary and descriptive tables to present the results of outcome evaluations. We conducted meta-analyses for outcome categories evaluated by RCT study designs, relating to mental, behavioural or neurodevelopmental disorders as specified by ICD-11. There was not an adequate number of studies to conduct meta-analyses for the outcome domains of subjective well-being or suicide-related outcomes. Owing to the small number of eligible non-randomised evaluations, these were also not synthesised through meta-analysis.
For the meta-analysis, we extracted effect estimates for the subdomains of mental, behavioural or neurodevelopmental disorders from study reports. Where appropriate, outcomes were converted to odds ratios using logistic transformation for pooling. Estimates from cluster randomised trials were checked for unit of analysis issues and, where necessary, an inflation factor was applied to the standard error of effect estimates. Where intracluster correlation coefficients (ICC) were not available and effect estimates had not been adjusted for clustering, we imputed an ICC using the average of estimates for specific outcomes from ‘most similar’ intervention evaluations.
We undertook robust variance estimation meta-analyses according to intervention outcome and time point, considering up to 6 months from baseline as short-term outcomes, and outcomes measured between 7 months and 2 years as long term. Robust variance estimation meta-analysis is a method that permits the inclusion of more than one effect estimate per study in a meta-analysis; this is in contrast to standard meta-analysis models that assume independence between individual effect estimates. It is common in meta-analysis of psychosocial interventions for outcome evaluations to present multiple relevant effect estimates per outcome (e.g. multiple estimates of child behavioural problems). This method permitted use of all relevant information from included studies. Within each meta-analysis, we examined heterogeneity using a combination of Cochran’s Q, τ2 and I2. Where heterogeneity was substantial (I2 > 50%), we scrutinised included studies to hypothesise and explore the reasons for this.
Equity harms synthesis
We produced a narrative overview and summary table of equity harms. We intended to construct harvest plots for the three key outcome domains of the review: (1) subjective well-being; (2) mental, behavioural or neurodevelopmental disorders and (3) suicide-related outcomes. Owing to the number of study reports presenting moderator analysis or interaction effects, harvest plots could only be generated for mental, behavioural or neurodevelopmental disorders.
Economic evaluation synthesis
Only one partial economic evaluation was identified, and we summarised this in narrative form.
Method-level syntheses integration and review-level synthesis
As reported, we used a results-based convergent synthesis design,73,74 which supported the integration of method-level syntheses to construct a review-level synthesis (see Figure 1). There were two key mechanisms through which we integrated the method-level syntheses. First, the synthesis of thin and rich process evaluations was integrated with outcome data to explain intervention effectiveness and variations in effects. 92 In alignment with stages 4 and 5 of the TRANSFER model,72 which focuses on assessing the relevance of international review evidence to the local context, integration paid attention to the context in which outcome and process syntheses were conducted and the implication for intervention in the UK moving forward.
Second, we constructed two integrative matrices, which were adapted from an approach used in a 2017 Cochrane review. 93 This was conducted as part of WP6. The first of these 2 × 2 matrices mapped interventions and their evidence base by stakeholder (both in process evaluations and consultations) preferences in regard to intervention theories and types. This was intended to establish whether current interventions are relevant and responsive to needs within the UK context. The second of these 2 × 2 matrices mapped intervention outcomes by stakeholders’ priority outcomes to assess if interventions are targeting desired effects.
Assessment of certainty
For the assessment of the certainty of the evidence base, we used the Grading of Recommendations Assessment, Development and Evaluation (GRADE)94,95 and GRADE Confidence in the Evidence from Reviews of Qualitative research (GRADE-CERQual)96 tools. This supported the convergent synthesis design and maps to stage 6 of the TRANSFER framework. 72
We applied the GRADE tool to evidence of effectiveness from randomised and non-RCTs. 95,97 Certainty was assessed for short- and long-term outcome subdomains relating to subjective well-being, mental, behavioural and neurodevelopmental disorders and suicide-related outcomes. This was done for the RCTs that assessed intrapersonal, interpersonal, organisational, community and policy-level interventions. It was conducted for non-randomised evaluations of organisational, community and policy-level interventions.
For both randomised and non-randomised studies, we conducted an assessment to decide if an individual study was biased or unbiased for each outcome, which was largely derived from the quality appraisals. RCTs had a baseline rate of high certainty and non-randomised studies a low certainty rating. As per GRADE guidance, the certainty assessment per outcome was then determined by prespecified criteria. Certainty was rated down according to RoB, imprecision, inconsistency, indirectness and publication bias. Certainty was rated up for large magnitude of effect, dose–response gradient and residual confounded would decrease the magnitude of effect (where this is an effect). The certainty of the evidence was assessed according to very low, low, moderate and high. Where there were serious concerns about the evidence, it was downgraded by + 1 points, and where there were very serious concerns, it was downgraded by + 2 points. Where there were reasons to upgrade the evidence, it was upgraded by + 1 point if there was sufficient reasoning and by + 2 points if there was strong reasoning.
We used the GRADE-CERQual96 tool to assess the certainty of evidence from rich process evaluation studies, with six statements being generated. Each statement was assessed across four components: methodological limitations; coherence; adequacy; and relevance. Each evidence statement was rated as high in the first instance and was rated down if there were concerns about each component. From here, an overall CERQual assessment of confidence in the evidence was made, with an accompanying explanation. Confidence in the evidence was rated as high, moderate, low or very low.
Work package 4: modelling of intervention theory (research question 5)
Drawing upon the integrated data from WP2 and WP3, we identified evidence-based interventions and, where reported, associated theories that could potentially address the CHIMES review outcomes. As per the protocol, the aim was to generate an overarching candidate intervention and theory to share as part of stakeholder consultations for WP5. This was to be accompanied with a narrative description and logic model. However, as the review indicated a range of interventions with a largely mixed evidence base and a lack of reported programme theories, we felt that they could not be integrated into a single approach and modelled without further consultation from stakeholders. As such, we decided to share descriptions of individual evidence-based interventions from across the socioecological domains for stakeholders to discuss.
Work package 5: stakeholder consultation and intervention prioritisation (research question 6)
The final stage of the review involved seven stakeholder consultations to consider the applicability of the review evidence base to the UK context, and identify a potential intervention for further development, adaptation and evaluation. This WP responds to the last stage, stage 7 of the TRANSFER model, which recommends discussing the transferability of review findings with stakeholders. 72 The membership of the stakeholder consultations, the structure of events, and the key discussion points are reported in Chapter 6. As part of the consultations, we conducted three phases of assessment, as outlined in Figure 2.
FIGURE 2.
Intervention prioritisation for development, adaptation and evaluation in UK context.
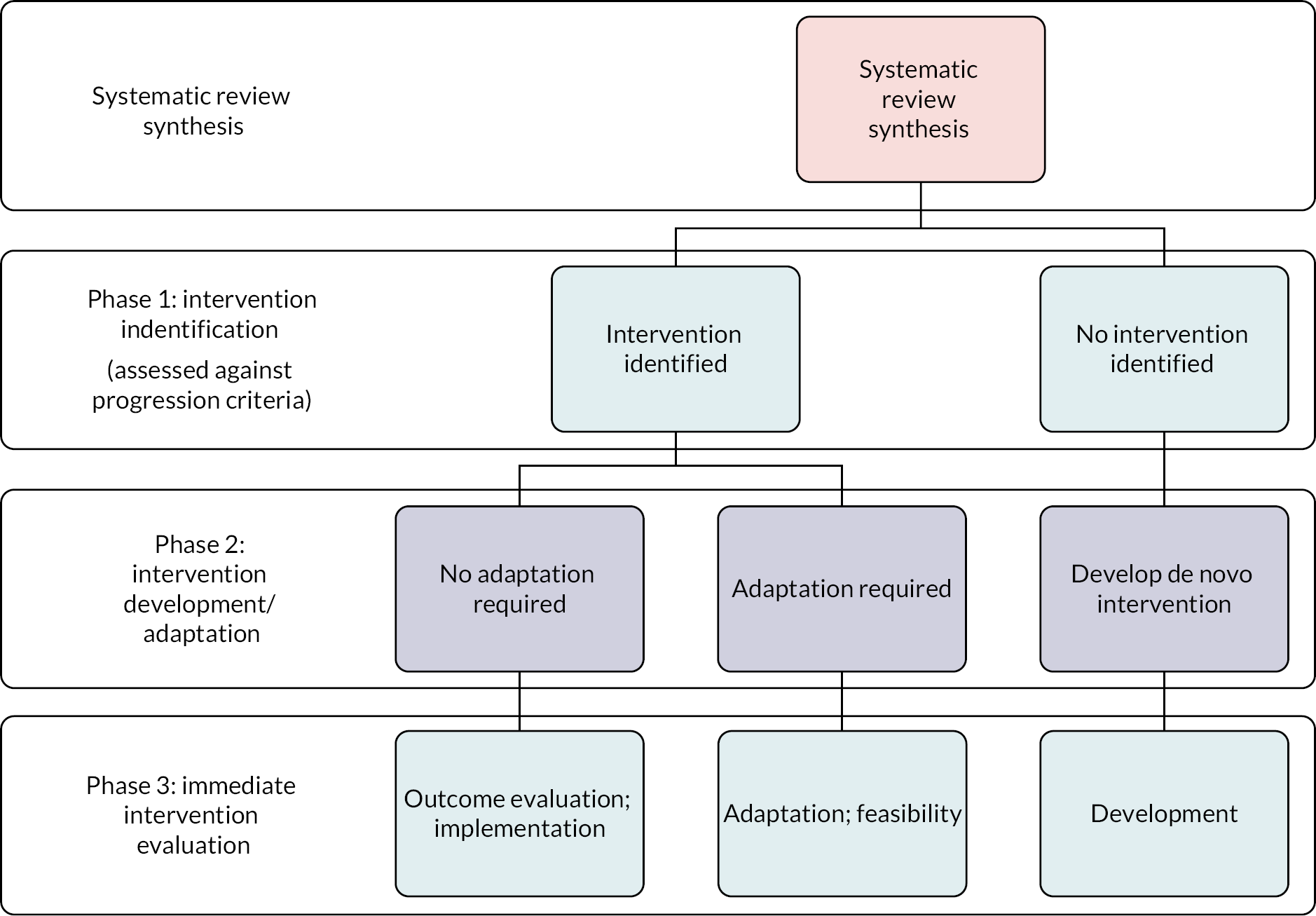
Phase 1: intervention identification
We asked stakeholders to assess the potential candidate evidence-based intervention theories and types identified from the review against the following progression criteria: (1) acceptability; (2) potential effectiveness and (3) feasibility (particularly feasibility of implementing an intervention in the UK context). To support this process, consultations considered the key context factors identified from earlier consultations and the process evaluation synthesis.
Phase 2: intervention development and adaptation
The next stage was to identify an intervention to take forward for future development, adaptation and evaluation. Stakeholders in this phase of consultation, combined with the discussion from earlier consultations, generally felt that the interventions identified in the evidence base were not exactly relevant to the UK context. As such, much of the emphasis of discussion was on the potential for de novo intervention development. To support this, we considered any additional context factors that would need to be taken account of, preferable intervention theories and associated components, and priority outcomes. Following the consultations, we cross-referenced this discussion with the review evidence base to check if there were interventions that may not necessarily have established evidence of effectiveness, but enacted the preferred theories, used suggested components and targeted priority outcomes. This was considered as part of the 2 × 2 integrative matrices on priority intervention types, theories and outcomes.
Phase 3: intervention evaluation
The final phase was considered by the research team and focused on recommendations for future research, considering potential intervention development and evaluation in accordance with Medical Research Council’s guidance. 98
Ethical considerations
Cardiff University School of Social Sciences Research Ethics Committee (REC) considered the CHIMES review to assess whether ethical approval was required from the REC. The REC requested to consider the review in two discrete parts: (1) desk-based review (WP1–4) and (2) consultations to support the identification of an intervention for the UK context (WP5). The REC agreed that neither of the two stages of work required ethical approval. This was largely due to consultations not involving the generation of individual-level participant data, meaning that individual names were not recorded and only summary notes of discussion were taken. We did undertake steps to ensure the safety and well-being of participants engaged in stakeholder consultations. One of the primary reasons for using pre-existing groups for young people and carers (e.g. CASCADE) was that there was a clear infrastructure available to participants after consultation in the event that they required follow-on support.
Summary
In this chapter, we have reported the methodology for the CHIMES review. The next chapter presents the results of the searches, the associated PRIMSA flow diagram and the results of the mapping phase of the study.
Chapter 3 Mapping interventions
About this chapter
In this chapter, we report the mapping of interventions and associated study reports included in the CHIMES review. It addresses the following RQ:
-
What are the types, theories and outcomes tested in mental health and well-being interventions for care-experienced children and young people?
As indicated in the methodology, construction of the evidence map served two functions. First, it supported mapping of key evidence clusters and gaps, with the identification of paucities in certain types of intervention research offering direction to strengthen the evidence base moving forward. Second, given the potential size of the review, it facilitated refinement and confirmation of the scope of the subsequent method-level syntheses.
In this chapter, we first present the results of the searches. We then detail the characteristics of included interventions and study reports, mapping the types of evidence retrieved for each RQ, the rates of report, geographical location, types of interventions, intervention characteristics, programme theories and intervention outcomes. We further summarise key intervention clusters and gaps and the confirmed scope of the systematic review.
Search results and study report inclusion
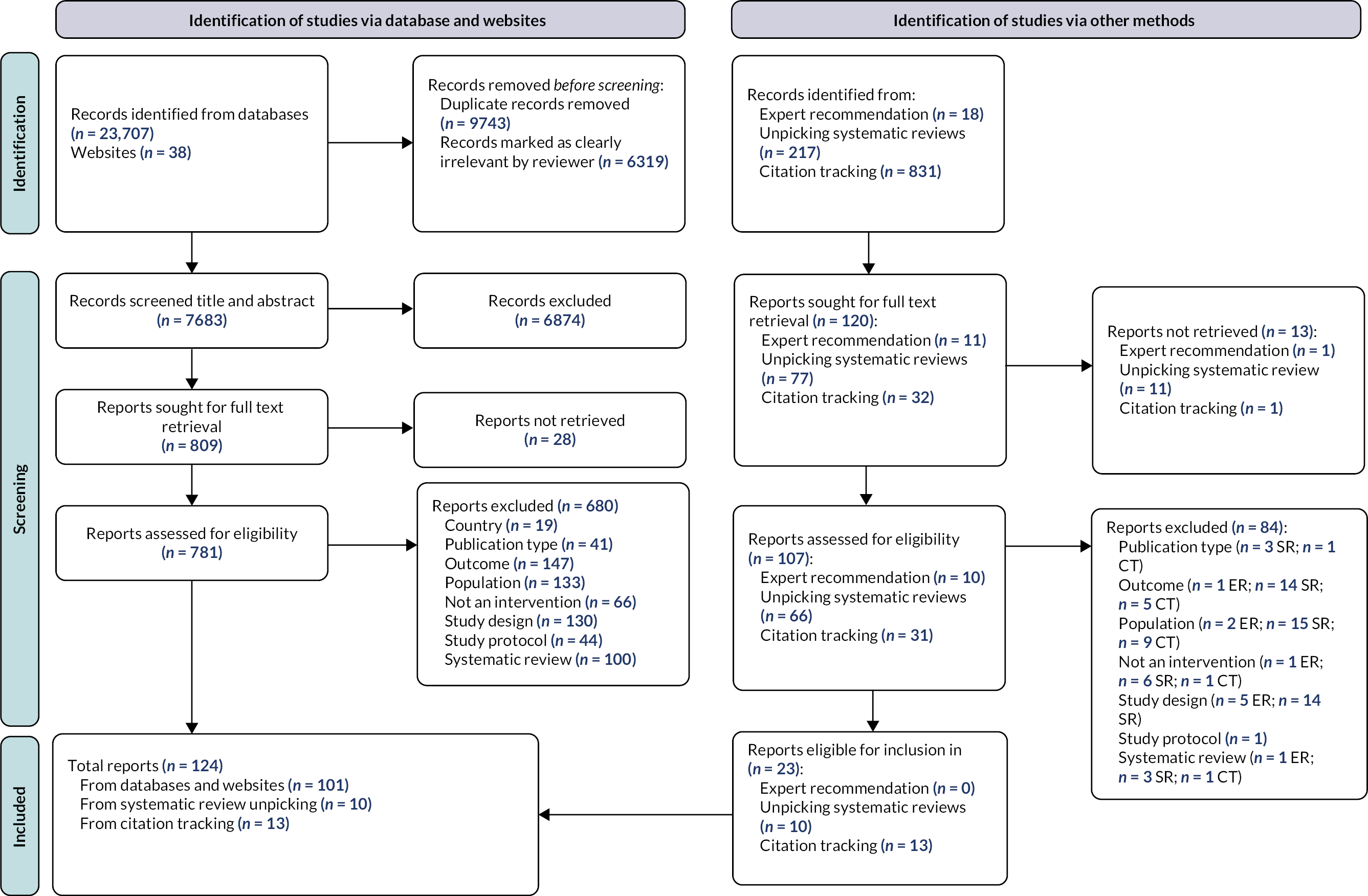
The process of study report retrieval and the number of reports identified through each data source is reported in the PRISMA flow diagram (Figure 3). In total, 124 unique study reports were included in the review, linked to 64 interventions. Of these, 101 were from databases and websites, 10 were from the unpicking of systematic reviews and 13 were from citation tracking.
FIGURE 3.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram. CT, citation tracking; ER, expert recommendation; SR, systematic review.
Study characteristics
Types of evidence
All 124 reports, linked to 64 interventions, were eligible as part of the evidence map. We have included these in the present chapter (RQ1). Study reports presented theory, process, outcome and economic evaluations. We classified study types by evaluation design to support understanding of whether current evaluation practice in this area is conducted in accordance with methodological guidance on intervention development and evaluation, which recommends the integration of these four evaluation types;98,99 24 reports provided an explanation of interventions’ programme theory (RQ1);25,27,28,30,100–119 50 process evaluations, both conceptually rich and thin, provided data on context, implementation and acceptability (RQ3; RQ4). 27,34,108,114,118,120–164 There were 86 outcome evaluations, using a RCT or non-randomised study design (RQ2). 26,27,29,31,33–35,100,103,108,109,111,113–118,122,128,130,131,134,135,140,142,143,147,148,151,157–160,162,163,165–212 There was one partial economic evaluation (RQ2). 213 The study reports according to each evidence type are presented in Report Supplementary Material 6.
Rates of report
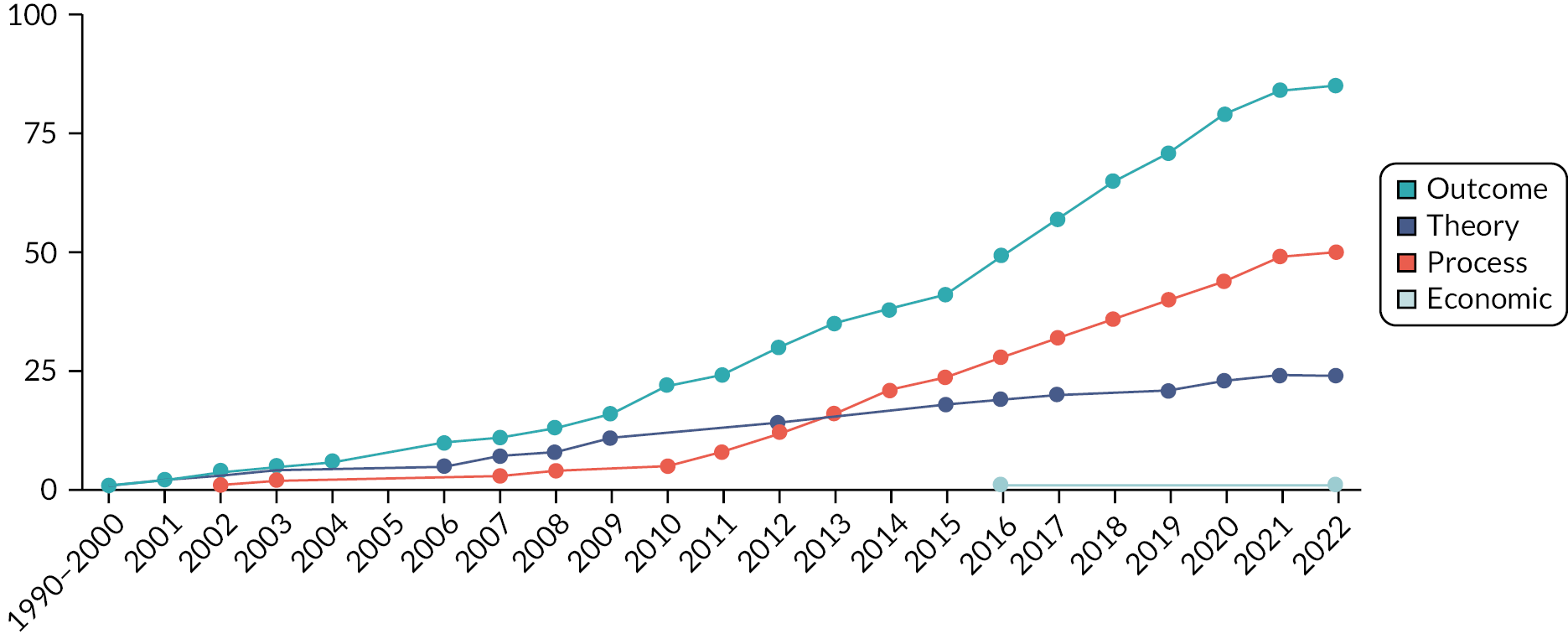
The 124 study reports were published between 1990 and 2022. Only two reports were published between 1990 and 2000. 105,170 Reports were published by subsequent years as follows: 1 in 2001;178 3 in 2002;106,109,148 3 in 2003;30,126,202 1 in 2004;188 5 in 2006;101,171,174,203,205 2 in 2007;108,112 3 in 2008;117,127,192 6 in 2009;28,107,110,169,184,206 6 in 2010;26,131,168,172,197,211 4 in 2011;136,146,160,183 7 in 2012;100,102,114,122,134,159,201 8 in 2013;35,103,111,125,133,142,153,187 7 in 2014;31,120,124,129,141,158,176 5 in 2015;25,27,135,164,182 12 in 2016;104,144,150,151,163,177,180,181,189,191,194,213 11 in 2017;34,113,121,149,152,173,175,186,190,198,204 10 in 2018;33,128,132,143,145,166,185,193,199,200 8 in 2019;29,116,123,140,147,161,167,207 11 in 2020;157 and 8 in 2021115,130,137,139,155,162,165,210 and 1 in 2022. 157 Figure 4 reports the number of study reports published by year according to the review RQ and evidence type. Study reports are double counted where they report evidence according to more than one RQ. There were no significant increases in reporting on programme theory. In contrast, there was a growing number of intervention evaluations using RCT and non-randomised evaluation designs and an expansion in the use of process evaluation.
FIGURE 4.
Cumulative rate of report and evidence type.
Geographical location
We specified that study reports had to be located in higher income countries as the review was primarily concerned with intervention transportability to the UK context. In total, the study reports were from 12 countries, with one report being conducted across both the USA and UK. 102 A significant majority of reports were from the USA (n = 77). 25,26,28–30,33–35,101–108,110–112,115–117,119,123–125,127–129,131,132,135,137,141,142,145–147,152,156,158–161,164–167,169–172,174,177,180–184,186–192,194,197,199–202,205–207,210–212 The remainder were from UK (n = 22);27,31,102,109,118,120–122,126,130,133,134,136,139,140,149–151,154,155,178,179,213 the Netherlands (n = 6);143,163,173,175,193,203 Belgium (n = 3);113,114,185 Australia (n = 3);153,162,209 Portugal (n = 3);144,204,208 Canada (n = 2);148,176 Ireland (n = 2);138,196 Israel (n = 2);100,168 Germany (n = 1);157 Spain (n = 1)198 and Sweden (n = 1). 195
Types of interventions
We classified types of interventions according to the socioecological domain or domains in which they operated (see Report Supplementary Material 6). The range of interventions are described in Figure 5. As indicated in Chapter 2, this was undertaken to respond to the review’s focus on the contextual contingency of intervention effects; we operated on the assumption that interventions working at different socioecological levels may interact differentially with the system depending on the area in which they are implemented. Classification of socioecological domain was informed by the theoretical basis of interventions, where this information was available. However, as the majority of interventions did not present a clear theory, we also considered information on the population and setting that was targeted by intervention activities (e.g. a skills curriculum directly engaging children and young people).
FIGURE 5.
Overview of intervention type by socioecological domain.
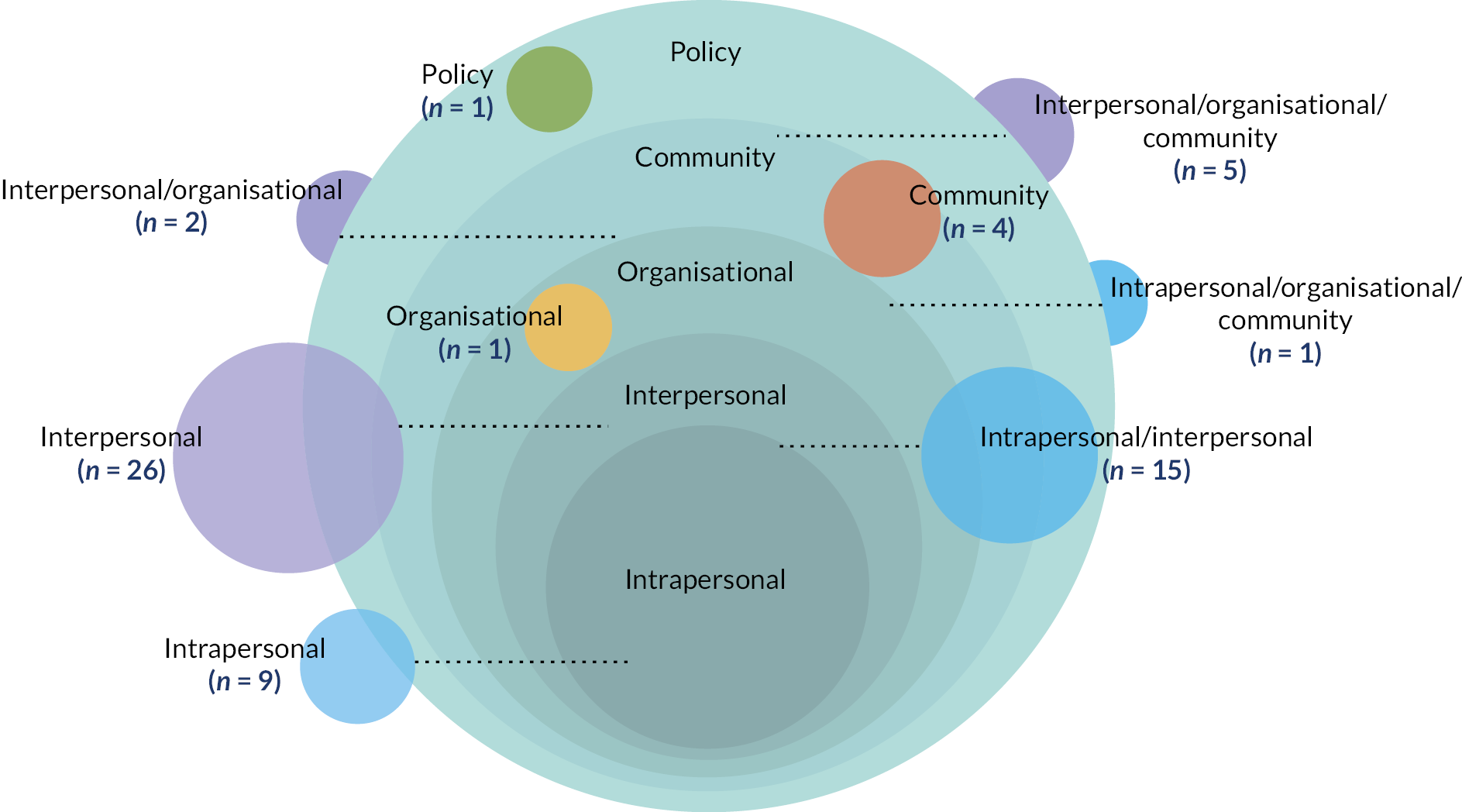
Nine interventions, with nine study reports, operated at the intrapersonal level, primarily targeting children and young people;120,135,142,143,151,168,200,202,204 15 interventions, with 24 study reports, targeted both the intrapersonal and interpersonal domain. 25,26,100,105,111,112,115,116,118,129,131,147,154,155,158,159,169,176,188,195,198,203,206,208 These interventions largely combined skill and knowledge development for children and young people, with curricula and coaching to support the carer–child relationship. 105 One intervention targeted the intrapersonal, organisational and community domains. 170
A total of 26 interventions, with 47 study reports, targeted the interpersonal domain, primarily focused on the relationship between care-experienced young people and their peers, carers and parents or other significant adults. 27,33,103,108,109,113,114,123,128,130,133,134,138,140,145,146,148,156,157,160,162,163,165–167,174,175,178–181,183,185,186,192,194,196,204,205,207,209,210,212 Two interventions, with 2 study reports, operated at the interpersonal and organisation level;132,139 5 interventions, with 32 study reports, targeted the interpersonal, organisational and community domains. 28–31,101,102,105–107,110,117,121,122,124,125,127,136,137,141,149,150,152,153,161,164,172,173,182,189,201,213
One intervention, with two study reports, targeted the organisational domain, focusing on organisational culture. 119,191 Four interventions, with four study reports, targeted community mental health and well-being provision. 34,35,126,187 One intervention, with four study reports, operated at the policy level, and focused on the comparison of different placement types that might be prioritised and funded. 190,193,197,199
Intervention characteristics
We mapped interventions against the TIDieR framework to describe their characteristics. 214 Owing to limits in the ways that interventions were reported in the literature, not all domains of the framework could be comprehensively addressed, particularly in relation to plans for adaptation and subsequent modifications. As such, domains with extractable data are discussed presently. Interventions are presented according to the primary socioecological domains in which they operated. Further description of included interventions is presented in Report Supplementary Material 6.
Intrapersonal intervention characteristics
The nine interventions classified as operating primarily at the intrapersonal level tended to focus on developing the skills, knowledge and resilience of children and young people. Cognitive and affective bibliotherapy comprises eight sessions with young people in residential care, exploring written texts as a departure point for discussing emotions. 168 Cognitively based compassion training is a 6-week, foster care-based cognitive training programme that delivers twice weekly sessions to teach competency in loving kindness, empathy and compassion. 142 One intervention provides additional therapeutic support, namely individual and rehabilitative strategies, to children and young people in intensive TFC. 200 The Sanctuary Model (Sanctuary Institute, New York, NY, USA) delivers 12 weekly psychoeducational group curricula to children and young people in residential care, with these groups also supporting trauma recovery. 202 Staff provide ongoing technical assistance and consultation, in addition to twice daily community meetings in the placement to teach young people awareness about the importance of proximal relationships.
Two cognitive–behavioural therapy (CBT) informed interventions were delivered through online and virtual modalities. One computer game intervention for young people in residential care entails playing the computer game The Sims: Life Stories (or ‘electronic dolls house’), to identify and model emotions, with parallel emotion regulation skill coaching by a social worker. 120 Meanwhile, Dojo Biofeedback is a game that teaches young people in residential care CBT-based relaxation techniques through a series of tutorials and mini-games. 143
Two interventions emphasised mindfulness practice. One is a 20-week Kundalini yoga programme delivered in residential settings, which addresses posture, breathing and mindfulness techniques. 151 The second is a mindfulness curriculum for children and young people in foster and kinship care, which includes guest speakers, arts and crafts activities, yoga instruction, playing music and open time to socialise. 135 Finally, Opportunities Box is a 6-week programme focusing on promoting career ability, adaptability and decision-making for institutionalised youth with a history of care. 204
Fifteen interventions operated at both the intrapersonal and interpersonal level, often combining individual development with group-based curricula and relationship-based components. Acceptance and commitment therapy for children in residential care comprises group-based psychoeducational curricula including experiential exercises, role plays and illustrations to develop psychological flexibility. 195 One intervention for children and young people in care tests a range of treatments that includes behavioural management by online care workers, psychodynamic treatment, structured boundaries and relationships, and adventurous learning that models self-supportive, adaptive behaviours. 203 Derived from MTFC, early-intervention foster care intends to provide parenting coaching and group support to foster carers to encourage placement permanency. 105 This is combined with behavioural specialist services and weekly therapy playgroup sessions for children.
Two interventions explicitly drew on a range of creative and leisure activities to support children and young people’s skills development and relationships. HealthRHYTHMS Drumming Protocol is a weekly group session for young people to non-verbally express themselves through music, before progressing to verbal and written forms of communication. 169 Wave by Wave is a 3-hour weekly psychoeducational programme for young people in foster care, which includes the physical activity of surfing to reduce the potential stigma of receiving mental health support. 208
Two interventions had a focus on animal-based therapy. Equine-facilitated psychotherapy (EEP) provides 7 months of weekly sessions with a horse for young people in residential care, with the aim of building a therapeutic alliance, developing adaptability and providing a healing experience. 100 Animal-assisted psychotherapy for children in foster care includes individual and small-group sessions with animals during an overnight visit to a farm. 198
Two interventions in this domain also included parents and carers alongside young people. One Medicaid-funded intensive outpatient service provides in home support for 1–2 years, offering individualised family-focused and child-centred treatment face to face, in addition to specialist support to relevant adults. 206 Trauma-focused CBT (TF-CBT) provides cognitive development support through child, carer and conjoint child-caregiver sessions. The intervention also includes an engagement component, with contact between the family and delivery agent to target perceptual barriers to participation. 129,158
Two interventions focused on mentoring. Fostering Healthy Futures (FHF) provides group-based curricula and mentoring for children and young people in out of home care. 25,26,111,112,115,116,147 The weekly sessions, over 30 weeks, follow a manualised curriculum addressing cognitive and behavioural skills, while individualised mentoring is provided by graduate social work students to model prosocial relationships. Take Charge provides mentor coaching to young people with additional needs in self-determination, combined with mentoring group meetings with intervention peers and foster care alumni. 159 With a focus on the relationship with the clinician, Life Story work targets children in foster care with a family history of methamphetamine-use and centralises building a trusting relationship before the child and clinician work together over 7 months to construct a culturally sensitive narrative of personal experience that challenges information and perceptions of high-risk behaviours. 131
Two interventions operating across the intrapersonal and interpersonal domains had a primary focus on educational outcomes. Kids in Transition to School (Oregon Social Learning Center, Eugene, OR, USA) is a school-based therapeutic playgroup, aimed at practising social skills and self-regulation to support school readiness. 188 Teach Your Children Well includes individualised tutoring for children, focused on reading and mathematical competency. 176
One intervention had a focus on drug and alcohol use. Supporting Looked-After Children in Decreasing Drugs and Alcohol (SOLID) provides six sessions of two interventions: first motivational enhancement therapy delivering client-centred counselling with a problem feedback component to reflect on the impact of drug and alcohol use and behavioural and cognitive strategies to build social networks to support positive behaviour change. 118,154,155
One intervention targeted the intrapersonal, interpersonal and organisational domain. Fostering Individualized Assistance Program (FIAP) provides a family specialist to children in foster care, acting as a family-centred clinical care manager and home-based counsellor. 170 They offer strength-based assessment, life domain planning, clinical case management and follow-along supports and services, providing a tailored set of services to meet the child’s needs.
Interpersonal intervention characteristics
Twenty-six interventions operated at the interpersonal level, with the vast majority focusing on training in parental management skills for foster and kinship carers. One social worker delivered intervention, derived from Save the Children’s content, provides 3 days of training to improve foster carers’ communication and attachment to the child. 178 Another intervention similarly offers 3 days of in-person group training to foster carers, although delivered by a clinical psychologist, with the aim to improve behavioural management. 109
Attachment and biobehavioural catch-up (ABC) is a home-based parenting programme for foster carers, with child–carer interactions videotaped to tailor content to their specific attachment and parenting needs. 184 Child Adult Relationship is a 6-hour, trauma-informed parenting programme to support the relationship with children and their foster carers. 33 Family Minds is a group-based online curriculum to increase carers reflective functioning and mentalisation skills. 165 One foster carer training provided at home visits by specialist foster carers to deliver a curriculum to improve parenting practices, behavioural management and carer stress, with monthly group sessions providing peer support. 113,114 Fostering Changes is a 12-week group-based training programme for foster carers that combines with a support group to improve parenting practices and communication styles. 179 Fostering Connections is a 6-week trauma-informed psychoeducational programme for carers to help understand and apply trauma-informed parenting strategies, with training including experiential exercises, videos, role play, discussion and home exercises. 138,196
The Herts and Mind study evaluated mentalisation-based therapy, a 12-week programme for foster carers, combing psychoeducation on attachment and mentalising among children with histories of maltreatment, consultation with professionals and direct relational work with families. 140 Non-violent resistance training is a 10-week foster carer training programme focused on parental submission and power struggles in the caring relationship, with telephone support sessions and accompanying learning materials. 185 Solution-focused parenting groups comprises a six-session group programme for foster carers of children with behavioural problems to improve parenting competence, with assignment activities to enact parenting goals. 148 A version of Triple P, adapted to foster carers, provides five weekly group parenting sessions to parents to teach parental management, combined with two telephone consultations. 157
Parent–child interaction therapy (PCIT) is a two-stage parent management training (PMT) programme for foster carers in outpatient settings: child-directed interaction to cultivate parent–child bonding; and parent-directed interaction to enhance parents’ behaviour management skills. 123,177,205,212 This is combined with a one-to-one home visit programme to reinforce and model key skills taught during sessions and is accompanied with a monthly support group for intervention families.
Several interventions had an explicit focus on kinship care or a range of placement types that went beyond foster care. Child-directed interaction training provides eight group-based coaching sessions to kinship carers to enhance the attachment relationship by improving parenting skills. 180 Connect-KP provides a nine-session group-based trauma and attachment-based parenting support for carers, while exploring the particular challenges of kinship care. 162 Incredible Years provides a trauma-informed group parenting programme to biological, foster, kinship and residential carers to support positive parenting and engaging in child serving systems. 108,128,130,133,144,174 PMT Treatment Oregon Model (PMTO) is a variation of MTFC. They tend to encompass a 1- to 2-weekly group parenting programme, home practice assignments and home visit supervision in behavioural management by trained PMTO facilitators. 146,160,163,166,167,175,210
Three interventions focused on relationships with biological families and reunification. One intervention, kContact, provides caseworker support to biological parents during contacts with their child, with telephone sessions encouraging parents to plan for, reflect upon and review the goals of contact. 209 Pathways Home aims to prevent reunification failure, providing a parenting curriculum and booster sessions to biological parents to ensure a safe and nurturing environment. 103 Similarly, Promoting First Relationships is a home visiting programme for biological parents to support reunification, through 10 brief manual-based sessions to increase parenting confidence and competence. 181
One intervention focused on improving carer–child relationships, in addition to peer relationships, to prevent internalising and externalising problem behaviours among girls. The intervention comprises six sessions of professionally led groups, one each for girls and foster carers during the school summer holidays, and weekly training and support over the subsequent academic year. 183 One intervention provides therapeutic mentoring by a clinician to young people in foster care, where they engage in a range of preplanned, mutually agreed activities. 211 Two interventions emphasised relationships with other adults and peers. Youth-initiated mentoring (YIM) matches young people in foster care with trained mentors to establish a one-to-one community-based relationship. 145 One intervention delivers a peer mentoring programme for girls at risk of pregnancy, where trained mentors support one mentee for a year to engage in a range of activities and contacts, through a range of means (e.g. face-to-face meetings, e-mail, telephone conversations and texts). 27
Interventions further worked to extend children and young people’s support networks. Family Finding entails professional, independent workers searching for, discovering and engaging actual and fictive kin for children and young people in foster care, with these individuals providing resources and various supports. 156,186,194
One interpersonal intervention increased resources available to foster carers through a private foster care agency, with carers having more financial resources to support the child, access to case manager support and educational support. 192
Two interventions targeted the interpersonal and organisational domains. Head, Heart, Hands aims to introduce social pedagogy to foster carers and service staff, through a series of taster sessions, courses and support groups, to create relationships with children that foreground social connections, co-creation and meaning making. 139 Intensive Permanence Services (IPS) is a 24-month programme that engages young people’s family members and other supportive family members to support them on the path to permanency. 132
Five interventions targeted the interpersonal, organisational and community level. Three of these interventions, MTFC, keeping foster parents trained and supported (KEEP), and TFC are derived from the same approach and principles. MTFC centralises placing young people in specialist, supervised foster homes with expertise in positive behavioural management. 30,31,101,102,107,122,124,136,173 Regular support is provided by programme supervisors with small caseloads, and the care placement is integrated into a range of system services. System-wide delivery models, such as train the trainer, have been developed to improve implementation.
Keeping foster carers and kinship carers supported draws upon components of MTFC for delivery with ‘regular’ foster and kinship carers. 28,29,102,125,127,152,182,189 Training can include participation in weekly training and support meetings, and twice weekly calls with a MTFC paraprofessional. As with MTFC, additional components have been added to optimise implementation and integrate the intervention into the wider social care system.
Treatment Foster Care (TFC) is a parenting programme that is integrated into a suite of wraparound services. 104,106,110,137,141,161 Together Facing the Challenge (TFTC), a close variant of TFC, is a weekly parenting programme for foster carers in effective behaviour management, which is embedded in a wider context of social care system activities. TFC for older youth is another adaptation that includes a clear psychiatric component, life skills development, future planning for education and employment and involvement of youth voice. In addition to foster carer training, it includes a range of wraparound services: psychiatric nurse support, family consultation, life coaching and skills coaching. 164
Evolve Behaviour Support Services provides therapeutic mental health, disability, behaviour support and educational services to disabled children and young people in out of home care. 153 Through co-ordinated stakeholders’ service delivery, it offers positive behaviour support through child-focused therapy, carer education and training and environmental strategies.
Glasgow Infant and Family Team (GIFT) and London Infant and Family Team (LIFT) are versions of the New Orleans Model. Children who have been abused and placed into foster care are referred to the service and, through a series of interviews, observations and questionnaires, working with families for approximately 3 months, the multidisciplinary team is able to make an informed decision about the best placement outcome for the child. 149,150,215
Organisational, community and policy intervention characteristics
One intervention operated at the organisational level, shifting organisational culture to have a more therapeutic, trauma-informed approach. Children and Residential Experiences (CARE) provides consultation, training and technical assistance to residential placement settings to create a more therapeutic environment through improvement to their policies and practices. 119,191
Four interventions targeted the community level, emphasising choice, availability and access to community mental health services. Head Start is a large publicly financed childhood education and care-programme, providing comprehensive wraparound community services to support disadvantaged children and families, including young people in care. 35 One study focused on optimising CAMHS for children and young people in care. It includes a model to support the interface between healthcare and social care professionals, and a single referral to services to improve access and effective engagement with young people through joint forums, partnership working and professional training. 126 One intervention improves choice and availability of different community outpatient mental health services, that includes drug and alcohol clinics, community health centres, crisis centres and private professional treatment. 187 Trauma systems therapy (TST) is a system wide-trauma informed model of practice to improve decision-making for the treatment pathway of children and young people in care, and enhance service co-ordination. 34
There was one intervention at the policy level, which was care placement type (e.g. foster, residential and kinship care). 190,193,197,199 In this instance, local and regional government legislation and policy increases the availability of different types of care and evaluation compares mental health related outcomes across placement type.
Programme theories for the interventions
A subset of 13 interventions, with 24 associated study reports, included an explicit programme theory. 25,27,28,29,100–103,105–119,172 Programme theories could include theories of change, which explicate the mechanisms through which interventions are intended to bring about change; theories of implementation, which explain how the intended is intended to be delivered; theories of context, which consider how wider contextual influences may interact with, and impact upon, intervention mechanisms. Details of the theoretical basis for interventions are presented in Report Supplementary Material 7.
Quality appraisal
The quality appraisal assessment of theory study reports is presented in Report Supplementary Material 8. This was primarily to assess the strength of the theoretical basis of interventions, which could support decision-making on the development, adaptation and evaluation of theoretically informed interventions moving forward. To note, we assessed each report on a case-by-case basis, so study reports linked to the same intervention evaluation could be assessed differently across different quality domains.
We identified two key limitations with study reports. First was a lack of involvement of children, young people, carers and professionals in the development of the theoretical basis for interventions. Only two interventions reported explicit involvement of care-experienced individuals in theory development. 112,118 One stated the process for development but stakeholder involvement was not clearly specified. 27
Second, there was a lack of clarity regarding the theoretical constructs drawn upon. Some reports provided an extensive description of a range of principles and literatures, including ‘formal’ established theories but did not always integrate them into a coherent programme theory. Commonly, there was a lack clear linkage between the theory and the intervention components and outcomes. Reports tended to describe theories in the background section, while the description of the intervention focused more on activities and delivery strategies. There was also limited use of logic models, being included in seven study reports. 25,26,106,107,113,118,119
Description of intervention theories
We present intervention theories according to the socioecological domains used to classify intervention types.
Intrapersonal: skills, knowledge and resilience of children and young people
Three interventions included intrapersonal theories of change. The FHF intervention presents theories related to improving skills, knowledge and resilience of care-experienced young people. 112,115,147 The intervention’s skill building curriculum is informed by positive youth development, a strengths-based developmental approach emphasising prosocial relationships and harnessing young people’s own resources. Resilience is referenced, with emphasis on developing adaptive functioning. Curriculum objectives align with these theories by addressing emotional regulation, modulation of behaviour and adaptation to school environment, positive relationships with peers and maintenance of a positive sense of self.
The SOLID intervention, which primarily aims to decrease alcohol and substance use among young people in care, draws upon motivational interviewing as the primary mechanism for behaviour change. 118 This entails engaging young people in cognitive and behavioural strategies to remove ambivalence about substance misuse behaviours and orientating them to positive action. EEP, while less explicit in its intrapersonal theoretical basis, is informed by the hypothesis that young people’s exposure to a horse’s movement and riding can encourage a human’s own mental and physical development. 100
Interpersonal: positive relationships with parents, carers and key figures
Twelve interventions included interpersonal theories of change. Three of the interventions theorise that the therapeutic context of relationships would support positive change. In one intervention exploring EEP, there is an emphasis on how the relationship with a horse provides a ‘healing experience’ that establishes interpersonal skills, where the emergence of a trusting relationship with the ‘other’ can set a template for other positive relationships. 100 Early-intervention and TFC models operate according to a similar set of assumptions, although in these cases the therapeutic relationship is forged with the foster carer. 105,110 TFC theorises that this relationship can provide the developmental progress required to overcome delayed maturation. 110
Seven interventions focus on enhancing parent and carer knowledge, skills and functioning to modify their relationship with the care-experienced young person. 28,30,101,102,104–109,113,114 Training curricula are often guided by Bowlby’s attachment, social learning theory, positive youth development and resilience, which together foreground the significance of positive relationships. Attachment cites the importance of providing consistent caregiving, emotional availability and security in developing children’s functioning, especially among care-experienced individuals who may have unavailable biological caregivers. 27,113,114 Positive attachments provide a context conducive to social learning, whereby individuals learn prosocial behavioural repertoires observationally through modelling and imitation. 28,29,101,108,113,114 Interventions further integrate learning about the causes and impacts of trauma, often by teaching TF-CBT. 30,101,104
Theories also link to parenting skill sets, notably around coercion and operant conditioning. 30,101,109 These work to reduce coercive interactions between the carer and child while enhancing effective management of negative behaviour through positive reinforcement and non-harsh disciplinary methods. They also encourage monitoring of young people’s relationships. Mediation analysis conducted with the KEEP intervention evidenced that reduction in children and young people’s problem behaviours is partly attributable to an increase in positive reinforcement practices. 117 Meanwhile, the Pathways Home intervention, which supports reunification, operates through encouragement-based parenting strategies. 103 The evaluation tested this theoretical model, reporting that while the intervention increased this approach to parenting, it did not translate into a reduction in total problem behaviours.
Interventions related to TFC theorise the relevance of carer characteristics to activating intervention mechanisms. One cites the importance of role satisfaction, motivation and identity perception. 106 TFTC explores the significance of role enactment when using behavioural management skills. 104 In the study analysis, participating foster carers were asked if they identify as parent or professional. Those more closely aligned with being a parent were more likely to achieve the interventions’ causal processes associated with TF-CBT.
Two mentoring interventions drew upon similar theoretical approaches, using attachment theory, social learning theory and positive youth development. 25,27,111,112,115,147 Here, the emphasis is on providing positive, prosocial relationships across multiple contexts to help young people’s development. 25 FHF centres the importance of prior relationship attachments when theorising how young people might respond to the mentoring relationship, specifically how relationship quality with birth parents and foster carers moderate impacts on mental health problems, PTSD and dissociation. 115 Meanwhile, the SOLID study emphasises the importance of positive social networks in helping young people to deal with their problems effectively and attain their goals. 118
Fostering Healthy Futures is the only included intervention to theorise iatrogenic causal pathways as a result of interpersonal theories. Group-based curricula are argued to potentially reinforce problematic skills sets, encourage the negative labelling of young people and facilitate the learning of disruptive behaviours (i.e. deviancy training). Groups are designed to mitigate these risks by comprising heterogeneous participants, including ‘prosocial’ young people. Prosocial skills are also practised within the relationship with the mentor.
Organisational level and community level: system change
Four interventions presented system-level theories across organisational and community domains. 28,102,106,107,119 These theories link to mechanisms of change, implementation theory and context theory. First, mechanisms of change focus on transforming organisational ethos within social care systems and creating alignment with an attachment or trauma-informed practice model. For example, the CARE intervention provides consultation, training and technical assistance to social care agencies, while reconfiguring organisational policies and practices to create a trauma-informed therapeutic ethos. 119
Second, implementation theories focus on restructuring local and regional contexts. 28,102,107 This is often to optimise the implementation of group-based parenting curricula. For the large part, there was no formally named theory associated with these approaches and we termed this ‘generic system change’. Study reports on MTFC and KEEP described two implementation theories. 28,102,107 Cascading dissemination aims to reduce the role of intervention developers via community development teams, which build local system capacity through facilitated peer-to-peer exchanges. The rolling cohort model is a training sequence that starts with a small number of implementation sites, before taking learning from these sites to support wider roll out.
Third, context theories identify wider system factors impacting on an intervention’s intrapersonal or interpersonal theories that can potentially inhibit effectiveness. For example, young people may be prevented opportunities for positive social relationships due to a paucity of resources, educational disruption and being placed away from their social networks. 106
Intervention outcomes
We mapped the outcomes targeted by each intervention (Figure 6). Depending on the type of study report and the RQ addressed, outcomes were theorised (e.g. study reports with theoretical descriptions) or empirically assessed (e.g. study reports of outcome evaluations). For theory and process evaluation studies, it was not always possible to identify target intervention outcomes. Study reports generally did not differentiate between primary and secondary outcomes. As such, primary and secondary outcomes were all mapped. Of note, study reports linked to the same intervention could theorise or evaluate different outcomes. Only the subset of study reports that specified a particular outcome for an intervention are cited for that outcome domain and subdomain.
FIGURE 6.
Map of primary and additional outcome domains.
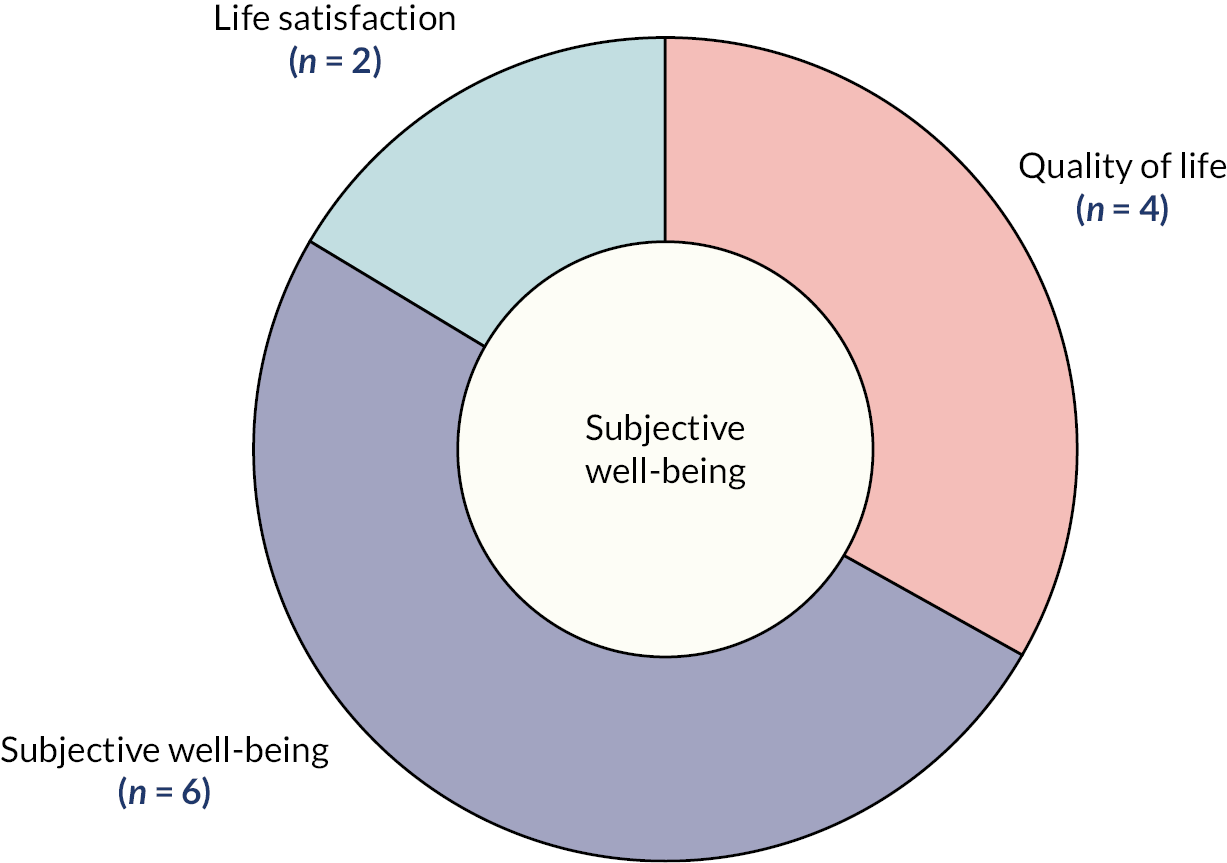
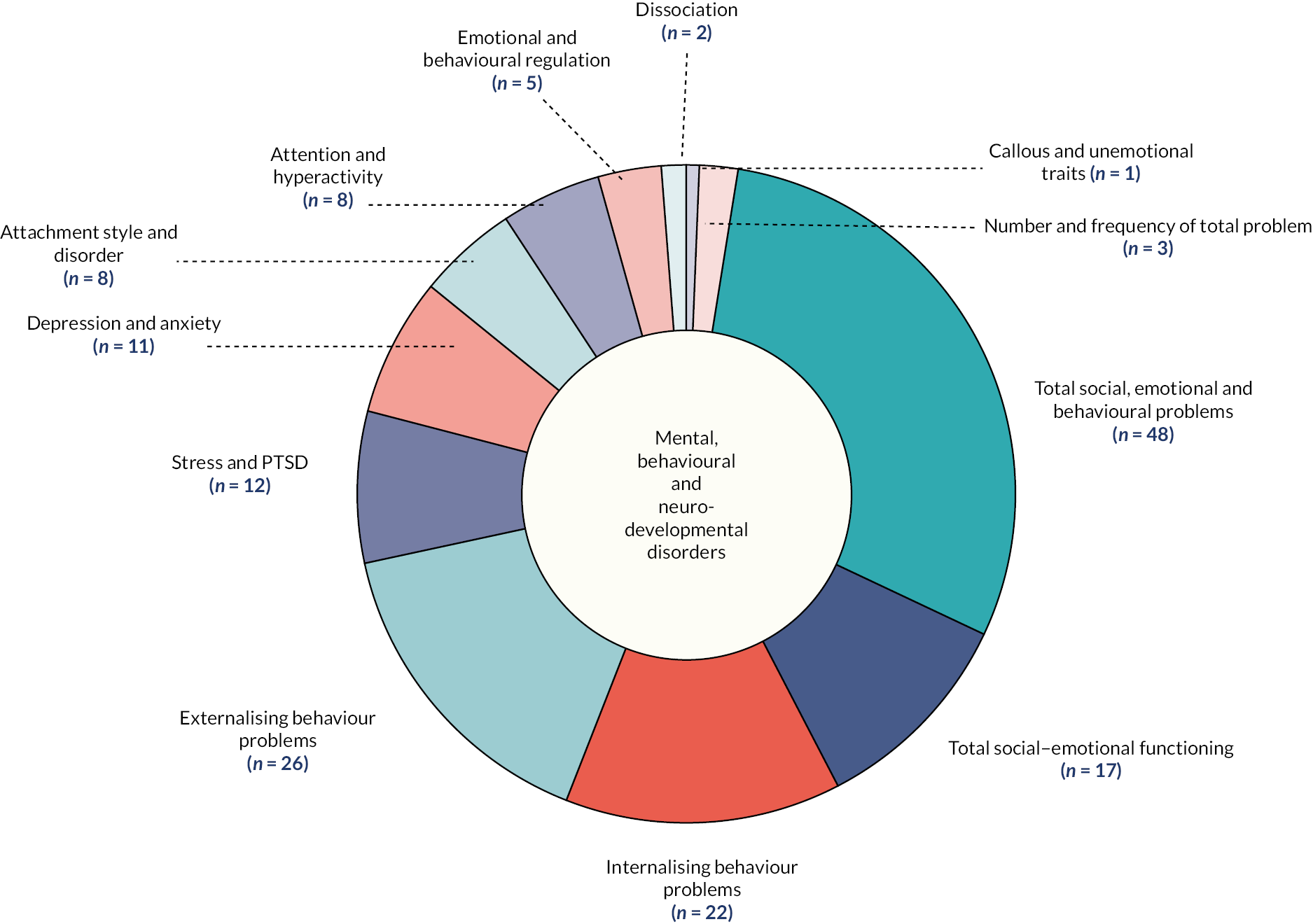
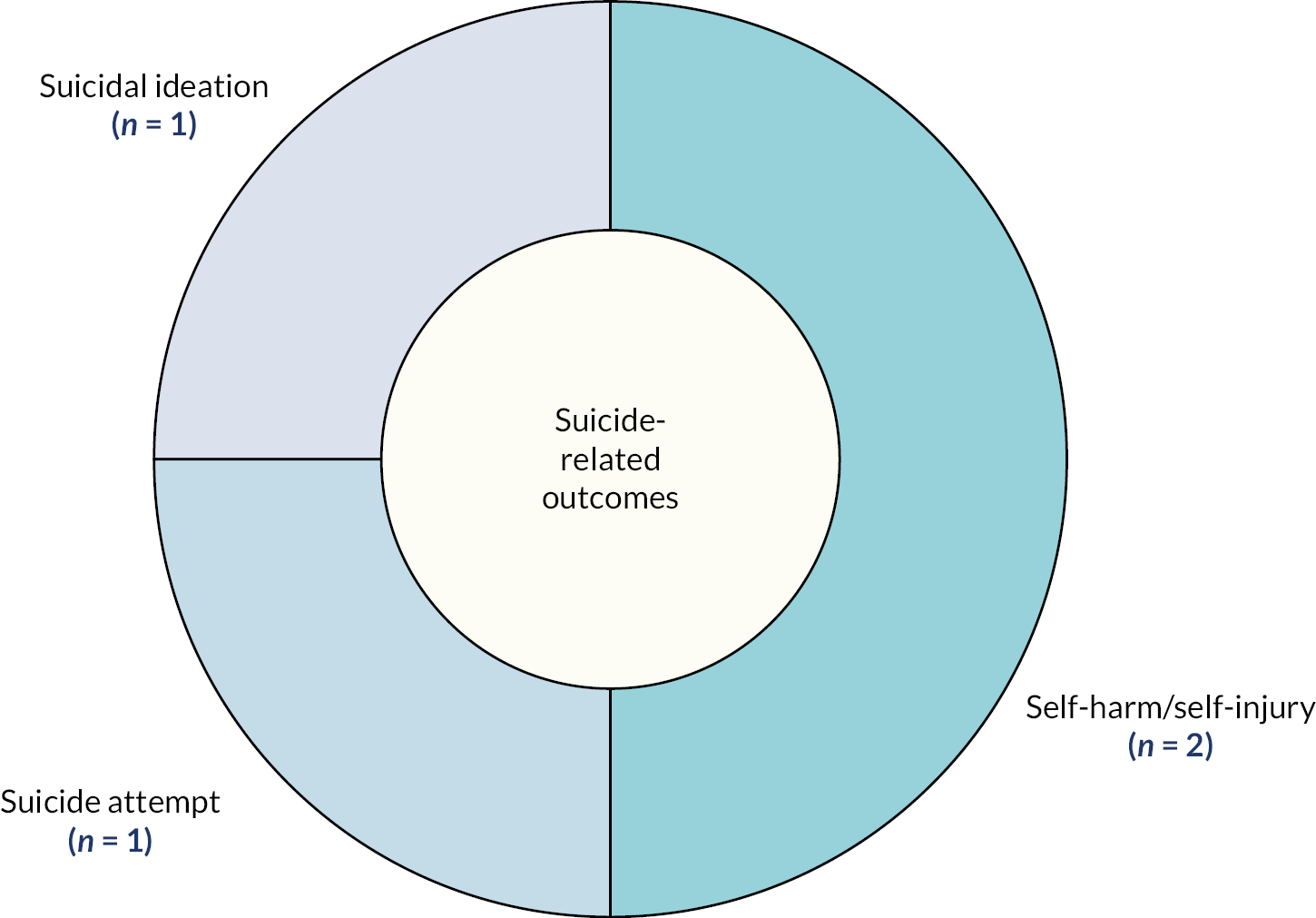
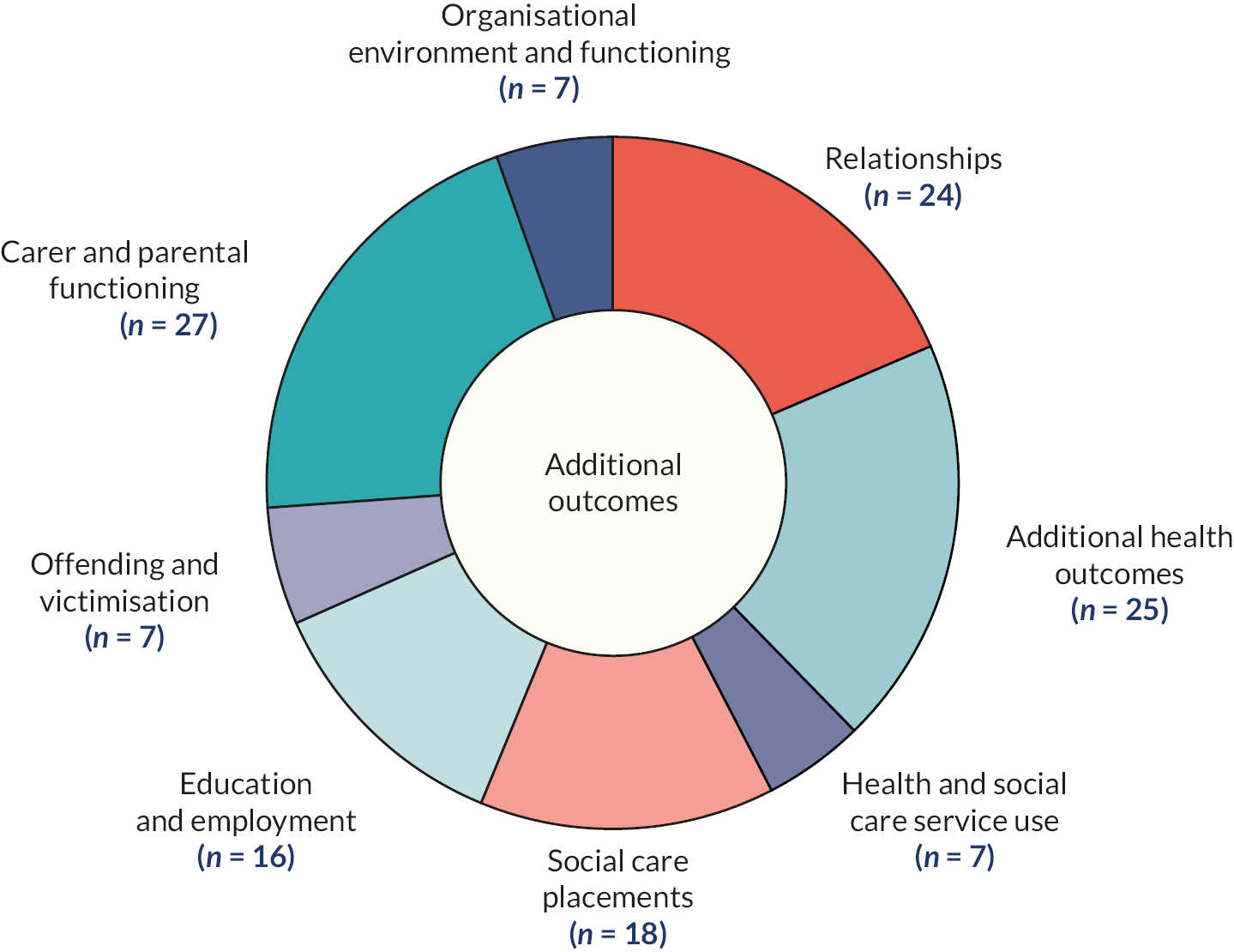
Primary outcome domains
Targeted intervention outcomes are presented in Report Supplementary Material 9. There were three primary outcome domains of the review: (1) subjective well-being; (2) mental, behavioural and neurodevelopmental disorders and (3) suicide-related outcomes. These domains and their subdomains were specified a priori.
The majority of outcome measurements were linked to child mental, behavioural and neurodevelopmental disorders, which had 13 associated subdomains. The most frequently measured of these subdomains were: total social, emotional and behavioural problems, which was targeted by 48 interventions with 74 associated study reports;25–29,31,35,103,105,106,109,112–114,117–119,122,127,129–131,133,134,140,142,144,146–150,153–156,158,159,162–167,170–173,175,177,178–186,189,193,195–197,199–203,205,207–210,212,213 social–emotional functioning difficulties, which was targeted by 17 interventions with 33 study reports;25,31,34,100,106–108,110,111,115,120,122,128,134,152,157,166–170,174,188,190,198,199,202,205,206,211–213 internalising problem behaviours, which was targeted by 22 interventions with 32 study reports;103,108,111–113,115,123,128,131,133,135,140,160,163,170,173,175,177,180,181,183–187,193,194,197–199,203,207 and externalising problem behaviours, which was targeted by 26 interventions with 38 study reports. 103,108,112–114,123,128,129,131,133,135,140,143,158,160,163,169,170,173–175,177,180,181,183–188,193,194,197–199,203,207,212
Subjective well-being and suicide-related outcomes were less frequently assessed. Only 11 interventions targeted domains of well-being related to quality of life;25,26,111,115,118,147,152,154,155,208 subjective well-being;118,132,145,151,154,155,176,197 and life satisfaction. 100,204 Suicide-related outcomes were targeted by four interventions, including suicidal ideation,123 self-harm95,150 and suicide attempt. 59
Additional outcome domains
In total, there were eight domains (see Report Supplementary Material 10). Six of these related to child-level outcomes, one was related to parent-level outcomes and one was related to organisational- and community-level outcomes. These domains, and their associated subdomains, were inductively classified from the study reports. In this instance, reports were coded using the concepts cited by the author(s) and then combined into categories of domains and subdomains (e.g. child offending and delinquency were combined into a category of antisocial behaviour, delinquency and offending).
For child-level outcomes, the most frequently assessed outcome domains was additional health outcomes, with the majority within this domain linked to coping, self-esteem and related constructs. 26,27,100,111,116,119,135,137,142,152,156,158,159,169,172,178,186,195,198,202,204,208 Meanwhile, social care outcomes were commonly assessed, with 14 intervention and 19 study reports, targeting placement stability, changes and breakdown. 28,34,105,113,118,154–156,159,162,164,170,179,185,186,189,190,194,207 A range of subdomains linked to carer- and parent-level outcomes were assessed, with the more frequently targeted one being carer/parent mental health and well-being. 107–109,113,123,128,130,133,151,162,163,165,173,175,179–182,184,185,189,205,209,213 A total of 7 interventions, with 10 study reports, targeted organisational environment and functioning. 102,119,124,125,130,132,136,191,202,213
Evidence clusters and refinement of the CHIMES review
Our mapping of the evidence identified the spread of available literature in relation to interventions targeting the mental health and well-being of care-experienced children and young people. Most evidently, the main cluster of evaluated interventions related to intrapersonal or interpersonal interventions, often targeting the skills and competencies of young people, improving the parenting practices of carers or facilitating prosocial relationships with significant others. However, current interventions are largely under-described and poorly theorised, with only 13 of the 64 included interventions having a clear theoretical basis. In contrast, there are clear evidence gaps in relation to structural-level interventions that target organisations, community and policy, which the initial stage of stakeholder consultation identified as a priority.
For the large part, interventions included in the CHIMES review originated from, and were evaluated in, the USA. Initial stakeholder consultations queried the lack of contextual congruence between the USA and other countries, notably the UK. The predominance of interventions from this single country highlights potential gaps in knowledge about the implementation of approaches in diverse contexts, cultures and countries. Equally, it raises important considerations about the transportability of evidence-based interventions.
There are clear evidence clusters related to the three primary outcomes of the review. The vast majority of the evidence base includes interventions focused on mental health, behavioural and neurodevelopmental disorders. In contrast, there is a substantial gap in relation to positive constructs of well-being, quality of life and life satisfaction, which were targeted by only 11 interventions. Similarly, suicide-related behaviours are also under-addressed, being targeted by only four interventions. Initial stakeholder consultations maintained that they wanted evidence-base interventions with a clear focus on well-being, while young people cited the importance of suicide-related outcomes due to their severely detrimental impact.
The evidence mapping also considered the types of evidence being generated in this research area. Recommendations from methodological guidance on intervention development and evaluation98 cite the importance of an integrated programme theory, process evaluation, outcome evaluation and economic evaluation. Accordingly, we considered the prevalence of these evaluation approaches in the literature. As indicated, there is a paucity of programme theory reports and a significant lack of economic evaluations. The latter is of particular concern given extant issues around escalating costs in the UK social care systems. 19 More positively, there has been an expansion in the conduct of process evaluations in recent years, reflecting an increased interest in context, implementation and acceptability. 63
We also used the evidence map to refine and confirm the subsequent systematic review, specifically the method-level syntheses. The mapping work showed that a systematic review was feasible in terms of size and specificity of available literature. Further, there was sufficient evidence to progress synthesis for the three primary outcome domains, but only conduct meta-analyses for mental health, behavioural and neurodevelopmental disorders. A priori, we indicated that only evaluations of interventions operating at the intrapersonal and interpersonal level would be included in the outcome synthesis if they were evaluated via RCT, and that interventions operating at the organisation, community and policy level would progress to further synthesis if evaluated by a RCT or non-randomised study design. This decision was supported by the available literature, with sufficient RCTs of intrapersonal and interpersonal interventions (which were occasionally combined with components across other socioecological domains). Of the six interventions operating exclusively at the organisational, community and policy level, only one of these had been evaluated via a RCT. 35
Summary
In this chapter, we have reported the retrieval process of eligible study reports and mapped the characteristics of included interventions and associated study reports (RQ1). In the next chapter, we present the results of the outcome and economic evaluation synthesis.
Chapter 4 Outcome evaluation
About this chapter
In this chapter, we report on intervention outcome evaluations. The chapter addresses the following RQs:
-
2. What are the effects (including inequities and harms) and economic effects of interventions?
In this chapter, we first report outcome study reports identified as being eligible for inclusion in the evidence map. We then describe the RCT evaluations, non-randomised evaluations (which we term QED) and economic evaluations that included in the outcome evaluation synthesis and their quality assessment. We then report a summary of effectiveness for each of the primary outcome domains and relevant subdomains, with associated meta-analyses where there was sufficiency in study reports. Finally, we present intervention equity harms.
Outcome evaluations eligible for evidence map
In total, 86 outcome evaluations were eligible for inclusion for the evidence mapping. These included:
-
RCT evaluations (52)
-
QED evaluations (34)
In addition, we identified one partial economic evaluation. 213
As reported in the previous chapter, we a priori decided to include only RCT study reports linked to intrapersonal or interpersonal interventions in the outcome synthesis. This was in addition to all RCT and QED evaluations of organisational, community and policy evaluations.
Characteristics of study reports included in outcome synthesis
In total, 52 RCT studies, 3 non-randomised studies and 1 partial economic evaluation were included in the outcome evaluation synthesis (Table 3).
| Intervention | Socioecological domain | Evaluation design | Country | Target population | Intervention duration (weeks) | Children and young people age (years) | Outcome domains | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Interpersonal | Intrapersonal | Policy | Community | Organisational | Well-being | Mental health | Self-harm/suicide | ||||||
| ABC, Dozier et al. (2006)171 | √ | RCT | USA | Multiple | 8–16 | Infants/preschool (0–5) | √ | ||||||
| ABC, Sprang (2009)184 | √ | RCT | USA | Multiple | 8–16 | Infants/preschool (0–5) | √ | ||||||
| CARE, Messer et al. (2018)33 | √ | RCT | USA | Foster carers | 2–7 | Younger children (6–11) | √ | ||||||
| Child-directed interaction training, N’Zi et al. (2016)180 | √ | RCT | USA | Multiple | 2–7 | Younger children (6–11) | √ | ||||||
| Cognitive and affective bibliotherapy, Betzalel and Shechtman (2010)168 | √ | RCT | Israel | Children and young people | 8–16 | Young adolescents (12–16) | √ | ||||||
| Cognitively based compassion training, Reddy et al. (2013)142 | √ | RCT | USA | Children and young people | 2–7 | Young adolescents (12–16) | √ | ||||||
| Communication and attachment training for foster carers, Minnis et al. (2001)178 | √ | RCT | UK | Foster carers | 2–7 | Younger children (6–11) | √ | ||||||
| Connect-KP, Pasalich et al. (2021)162 | √ | RCT | Australia | Foster carers | 8–16 | Younger children (6–11) | √ | ||||||
| Dojo: Biofeedback videogame, Schuurmans et al. (2018)143 | √ | RCT | Netherlands | Children and young people | 8–16 | Young adolescents (12–16) | √ | ||||||
| Family Finding, Vandivere et al. (2017)186 | √ | RCT | USA | Children and young people | 20 + | Young adolescents (12–16) | √ | ||||||
| Family Minds, Adkins et al. (2021)165 | √ | RCT | USA | Foster carers | 2–7 | Younger children (6–11) | √ | ||||||
| Foster carer and foster children group-based intervention, Smith et al. (2011)183 | √ | RCT | USA | Multiple | 2–7 | Younger children (6–11) | √ | ||||||
| Foster Parent Intervention, Van Holen et al. (2017)113 | √ | RCT | Belgium | Foster carers | 8–16 | Younger children (6–11) | √ | ||||||
| Fostering Change, Briskman et al. (2012)134 | √ | RCT | UK | Foster carers | 8–16 | Younger children (6–11) | √ | ||||||
| Fostering Change, Moody et al. (2020)179 | √ | RCT | UK | Multiple | 8–16 | Younger children (6–11) | √ | ||||||
| FHF, Taussig and Culhane (2010)24,26 | √ | √ | RCT | USA | Children and young people | 20 + | Younger children (6–11) | √ | √ | ||||
| FHF, Taussig et al. (2019)147 | √ | √ | RCT | USA | Children and young people | 20 + | Younger children (6–11) | √ | √ | ||||
| FHF, Weiler and Taussig (2019)116 | √ | √ | RCT | USA | Children and young people | 20 + | Younger children (6–11) | √ | √ | ||||
| FHF, Weiler et al. (2021)115 | √ | √ | RCT | USA | Children and young people | 20 + | Younger children (6–11) | √ | √ | ||||
| FIAP, Clark et al. (1994)170 | √ | √ | √ | RCT | USA | Multiple | 20 + | Younger children (6–11) | √ | ||||
| Head Start, Lipscomb et al. (2013)35 | √ | RCT | USA | Multiple | 20 + | Infants/preschool (0–5) | √ | ||||||
| HealthRHYTHMS Bittman et al. (2009)169 | √ | √ | RCT | USA | Children and young people | 2–7 | Young adolescents (12–16) | √ | √ | ||||
| Incredible Years, Conn et al. (2018)128 | √ | RCT | USA | Foster carers | 8–16 | Infants/preschool (0–5) | √ | ||||||
| Incredible Years, Linares et al. (2006)174 | √ | RCT | USA | Foster carers | 8–16 | Younger children (6–11) | √ | ||||||
| kConnect, Suomi et al. (2020)209 | √ | RCT | Australia | Multiple | 20 + | Younger children (6–11) | √ | ||||||
| KEEP, Chamberlain et al. (2008)127 | √ | √ | √ | RCT | USA | Multiple | 8–16 | Younger children (6–11) | √ | ||||
| KEEP, Price et al. (2015)182 | √ | √ | √ | RCT | USA | Multiple | 8–16 | Younger children (6–11) | √ | ||||
| KEEP, Price et al. (2019)29 | √ | √ | √ | RCT | USA | Multiple | 8–16 | Younger children (6–11) | √ | ||||
| Life Story, Haight et al. (2010)131 | √ | √ | RCT | USA | Children and young people | 20 + | Younger children (6–11) | √ | |||||
| MBT, Midgley et al. (2019)140 | √ | RCT | UK | Multiple | 8–16 | Younger children (6–11) | √ | ||||||
| Mentoring intervention for teenage pregnancy, Mezey et al. (2015)27 | √ | RCT | UK | Children and young people | 20 + | Older adolescents (16+) | √ | √ | |||||
| Mindfulness, Jee et al. (2015)135 | √ | RCT | USA | Children and young people | 8–16 | Older adolescents (16+) | √ | ||||||
| MTFC, Biehal et al. (2012)122,214 | √ | √ | √ | RCT | UK | Multiple | 20 + | Young adolescents (12–16) | √ | ||||
| MTFC, Green et al. (2014)31 | √ | √ | √ | RCT | UK | Children and young people | 20 + | Young adolescents (12–16) | √ | ||||
| MTFC, Jonkman et al. (2017)173 | √ | √ | √ | RCT | Netherlands | Multiple | 20 + | Younger children (6–11) | √ | ||||
| Non-violent resistance training, Van Holen et al. (2018)185 | √ | RCT | Belgium | Foster carers | 8–16 | Young adolescents (12–16) | √ | ||||||
| PMTO, Akin et al. (2018)166 | √ | RCT | USA | Biological parents | 20 + | Younger children (6–11) | √ | ||||||
| PMTO, Akin et al. (2019)167 | √ | RCT | USA | Multiple | 20 + | Younger children (6–11) | √ | ||||||
| PMTO, Maaskant et al. (2016)163 | √ | RCT | Netherlands | Multiple | 20 + | Younger children (6–11) | √ | ||||||
| PMTO, Maaskant et al. (2017)175 | √ | RCT | Netherlands | Multiple | 20 + | Younger children (6–11) | √ | ||||||
| PMTO, Yan and De Luca (2021)210 | √ | RCT | USA | Biological parents | 20 + | Younger children (6–11) | √ | ||||||
| PCIT, Mersky et al. (2016)177 | √ | RCT | USA | Multiple | 8–16 | Infants/preschool (0–5) | √ | ||||||
| PCIT – Brief + Extended, Mersky et al. (2020)212 | √ | RCT | USA | Multiple | 8–16 | Infants/preschool (0–5) | √ | ||||||
| Pathways Home, DeGarmo et al. (2013)103 | √ | RCT | USA | Multiple | 20 + | Younger children (6–11) | √ | ||||||
| Promoting First Relationships, Oxford et al. (2016)181 | √ | RCT | USA | Multiple | 8–16 | Infants/preschool (0–5) | √ | ||||||
| SOLID, Alderson et al. (2020)118 | √ | RCT | UK | Children and young people | 8–16 | Older adolescents (16+) | √ | ||||||
| Take Charge, Geenen et al. (2012)159 | √ | √ | RCT | USA | Children and young people | 20 + | Young adolescents (12–16) | √ | |||||
| Teach Your Children Well, Marquis (2014)176 | √ | √ | RCT | Canada | Children and young people | 20 + | Younger children (6–11) | √ | |||||
| TFTC, Farmer et al. (2010)172 | √ | √ | √ | RCT | USA | Foster carers | 2–7 | Young adolescents (12–16) | √ | ||||
| CBT plus Evidence-Based Engagement Strategies, Dorsey et al. (2014)129 | √ | √ | RCT | USA | Multiple | 8–16 | Younger children (6–11) | √ | |||||
| Triple P for Foster Parents, Job et al. (2022)157 | √ | RCT | Germany | Multiple | 2–7 | Infants/preschool (0–5) | √ | ||||||
| Wave by Wave Surf Therapy, Pereira et al. (2020)208 | √ | √ | RCT | Portugal | Children and young people | 20 + | Young adolescents (12–16) | √ | √ | ||||
| TST, Murphy et al. (2017)34 | √ | QED | USA | Care staff | 20 + | Young adolescents (12–16) | √ | ||||||
| Access to outpatient mental health services, Bellamy et al. (2013)187 | √ | QED | USA | Children and young people | 20 + | Younger children (6–11) | √ | ||||||
| CARE, Izzo et al. (2016)191 | √ | QED | USA | Multiple | 20 + | Unclear | √ | √ | |||||
| New Orleans-Glasgow model, Boyd et al. (2016)213 | √ | √ | √ | Economic | UK | N/A | N/A | N/A | |||||
Synthesis of randomised controlled trial outcome evaluations
A total of 38 interventions, with 52 associated RCTs, were included in the synthesis (see Report Supplementary Material 11): 23 interventions, with 32 evaluations, were from the USA; 6 interventions, with 8 study reports, were from the UK; 3 interventions, with 4 study reports, were from the Netherlands; 2 interventions, with 2 study reports, were from Australia; 2 interventions, with 2 study reports, were from Belgium; 1 intervention, with 1 study report, was from Canada; 1 intervention, with 1 study report, was from Germany; 1 intervention, with 1 study report, was from Israel; 1 intervention, with 1 study report, was from Portugal.
Interventions primarily operated across the intrapersonal and interpersonal domains. Six interventions, with six associated study reports, targeted the intrapersonal domain; 22 interventions, with 32 associated evaluations, targeted the interpersonal domain, and 9 interventions, with 13 associated study reports, targeted both domains. There was one RCT evaluation of an intervention targeting the interpersonal, organisational and community domains. FIAP delivers intensive, personalised support services across agencies. 170 Only one RCT evaluation assessed a policy-level intervention, Head Start. 35
The comparator group for all evaluations was usual practice or standard care. There were three exceptions. Evaluation of TFTC, an extension of TFC, compared the extended intervention with the original TFC approach. 172 Evaluation of TF-CBT compared an optimised version of the intervention, including additional engagement activities, with TF-CBT alone. 158 Meanwhile, evaluation of Promoting First Relationships compared the intervention group with those receiving an active control of early educational support. 181
Three RCT evaluations reported more than one experimental group. Evaluation of bibliotherapy compared both cognitive bibliotherapy and affective bibliotherapy with usual care. 168 Evaluation of the HealthyRHYTHYMS protocol compared a standard or extended version of the protocol with usual care. 169 Evaluation of PCIT compared both a standard and extended version with usual care. 177
The duration of interventions ranged from 3 weeks178 to 18 months. 170 Nine interventions, with nine study reports, were delivered for 3–6 weeks. 33,142,157,165,169,172,178,180,183 Most interventions lasted a minimum of 2 months, with 13 interventions, and 22 associated study reports, lasting for 5 months or more. 26,27,31,35,103,116,122,131,147,159,163,166,167,170,173,175,176,186,209,210,218
We classified follow-up times for outcome assessment from baseline according to 0–6 months (shorter term) and more than 6 months (longer term) categories. Longer-term follow-up outcome data were available for 13 interventions, with 17 study reports. 26,27,31,113,122,131,147,159,163,166,170,172,176,178,179,186
Synthesis of quasi-experimental design outcome evaluations
Three interventions, with three associated study reports, were included in the synthesis34,187,191 (see Report Supplementary Material 12). All interventions were evaluated in the USA. One intervention targeted the organisational domain. CARE aims to improve ethos and practice across residential care agencies, and was evaluated using an interrupted time series design. 191 Two interventions targeted the community domain. One focuses on increasing the availability of community health services to young people, and was evaluated through routine administrative data;187 TST is system-wide effort to implement trauma-informed care and was evaluated across a large, private welfare system in the USA. 34 Intervention duration and time to follow-up times were typically longer than the RCT evaluations.
Synthesis of economic evaluations
Only partial economic evaluation was eligible for the review. 213 This was included on the advice of the project advisory group, who observed the paucity of economic evaluations in children’s social care. The evaluation examined the potential costs and consequences of implementing the New Orleans intervention in Glasgow (GIFT), comparing estimated costs of the new with the costs of the current foster care system (service as usual). Usual care was reported to cost approximately £30,586 per child for the first year and £24,924 per year thereafter. In comparison, they estimated that GIFT would cost approximately £55,345 per child for the first year, falling to £44,896 thereafter. However, based on reviews of the intervention delivered elsewhere and the consultation with expert stakeholders, evaluation estimated that implementation of GIFT would reduce the probability of children re-entering care from a 44% rate of return in the existing system to 3%. It would also reduce the average length of stay from 30 months to 20.5 months. As a result, the economic modelling estimated that the average cost per child would be lower with GIFT (£88,653) compared with the existing system (£95,473).
Risk of bias and quality assessment of outcome evaluations
We conducted RoB assessments for all RCT evaluations and QED evaluations included in the outcome evaluation synthesis.
Randomised controlled trial evaluations: quality appraisal
We appraised the 52 RCT evaluation with the RoB2 tool (see Report Supplementary Material 13). 219 The tool assesses potential bias across five domains: (1) bias arising from randomisation processes; (2) bias due to deviations from the intended intervention; (3) bias due to missing outcome data; (4) bias in the measurement of outcomes and (5) bias in the selection of reported results.
Overall bias
In total, seven RCT evaluations had a high overall RoB. 27,35,118,122,157,158,209 We assigned overall high RoB score where at least one of the five individual domains scored as high risk or where three or more domains were considered to have ‘some concern’ of bias. We assessed the remaining 45 evaluations to have ‘some concern’ of overall bias. Evaluations were largely driven by potential bias due to the RoB from measurement of outcomes.
Bias arising from randomisation process
In total, we considered 44 RCT evaluations (84.6%) to be at low RoB from randomisation procedures. Seven evaluations had some concerns of bias from randomisation29,33,35,128,157,158,168 and one had a high risk. 122 Generally, this bias arose from the reported need to balance methodological rigour with study design decisions that were minimally disruptive to existing practice. For example, in an evaluation of MTFC, the study team took a pragmatic, ‘suboptimal’ approach to randomising participants to the intervention arm, focusing on minimising the number of unfilled MTFC placements, to make the design of the study more acceptable to participating local authorities. 122
Bias due to deviations from intended interventions
In total, we considered 44 of the RCT evaluations (84.6%) to be at low risk with regard to potential bias from deviating from the intended intervention. Six evaluations had ‘some concerns’ of bias due to deviations from intended interventions,118,157,163,172,176,209 whereas two were high risk. 27,122
Bias due to missing outcome data
In total, we assessed 40 of the RCT evaluations (76.9%) to be at low RoB due to missing outcome data. Eleven evaluations had some concerns27,31,35,122,131,142,157,158,186,209,218 and one had a high RoB. 118 Typically, missing data related to high levels of drop out. There were issues about potential bias in the interpretation of group differences. For example, evaluation of MTFC-A indicated higher drop out rates in the control group relative to the intervention group, introducing the potential bias in group comparisons in post-intervention data,122 while a pilot RCT of the SOLID trial reported very high attrition rates in the intervention group relative to control groups. 118
Bias in the measurement of outcome
In total, we assessed that all 52 RCT evaluations (100%) had some concerns about outcome measurement. Most evaluations relied on either self-report or carer-reported assessments to measure child-level outcomes, with neither group being blinded to group allocation. Of the evaluations that used external assessment (clinician- or teacher-rated assessments), none reported that assessment staff were blinded to group allocation. As the outcomes being assessed invariably involved subjective assessment rather than diagnostic classification, we considered outcome assessments from each of the studies to have been at least ‘potentially influenced’ by knowledge of the intervention received. 219
Bias in selection of reported results
In total, we considered 51 (98%) of the RCT evaluations to be low risk. One evaluation had some concern due to only reporting significant post-intervention findings for a number of intervention effect estimates. 159
Quasi-experimental design evaluation: quality appraisal
We appraised the three QED evaluation with the ROBINS-I tool. 220 The tool assesses bias according to seven domains: confounding; selection of participants in the study; classification of interventions; deviations from intended interventions; missing data; measurement of outcomes; and selection of the reported results. Agreed assessments are reported in Table 4.
| Intervention | Bias from confounding | Bias from participant selection | Bias from classification | Bias from deviations | Bias from missing data | Bias from measurement | Bias from selection of results |
|---|---|---|---|---|---|---|---|
| CARE187 | Low | Low | Low | Low | No info | Moderate | Low |
| TST34 | Low | Low | Moderate | Moderate | No info | Moderate | Low |
| Outpatient mental health service access191 | Low | Low | Low | Low | No info | Moderate | Low |
We assessed the CARE intervention as low risk for each domain for the RoB from measurement, as the single informants (carers) were not blinded to allocation. 187 Insufficient data were provided to assess risk from missing data. We assessed TST34 as having risks due to the use of a non-standardised tool to assess outcomes, difficulties in defining dosage or exposure to the intervention, changes made to the evaluation programme and a reliance on proxy fidelity measures. We assessed the impact of access to outpatient mental health services as having low RoB across most domains, with the exception of bias from outcome measurement due to a reliance on agency staff to define ‘behavioural incidents’. 191
Outcome evaluation synthesis
In this section, we report the outcome synthesis the evidence of effectiveness for each of the primary outcome domains and subdomains. The primary outcome domains were:
-
child subjective well-being
-
child mental, behavioural and neurodevelopmental disorders
-
child self-harm and suicide.
As indicated, in the synthesis we differentiated between shorter-term outcomes (measured between 0 and 6 months post baseline) and longer-term outcomes (measured more than 6 months post baseline). For outcome domains where sufficient RCT evaluation effect sizes were available, we conducted a meta-analysis to evaluate the pooled effect of interventions. We did not include QED studies in the meta-analysis due to the insufficiency of study reports.
Subjective well-being
In accordance with the evidence map, we classified subjective well-being according to three subdomains: quality of life, subjective well-being and life satisfaction. Two interventions, with three RCT evaluations, assessed quality of life with child-reported measures at short and long-term follow-up (Table 5). 26,147,218
| Intervention | Study design | Intervention length (weeks) | Outcome assessed | Tool | Informant | Data type | Follow-up | Follow-up (category) (months) | Effect size | 95% CI (low) | 95% CI (high) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Wave by Wave Surf Therapy218 | RCT | 21 | Health-related quality of life | Kidscreen-10 | Child/young person | Scale | Post test | 4–6 | 0.25 | −0.26 | 0.76 |
| FHF26 | RCT | 30 | Quality of life | LSS | Child/young person | Scale | Post intervention | 7–12 | 0.42 | 0.12 | 0.71 |
| FHF26 | RCT | 30 | Quality of life | LSS | Child/young person | Scale | 6-month post intervention | 13–18 | 0.14 | −0.17 | 0.45 |
| FHF26 | RCT | 30 | Quality of life | LSS | Child/young person | Scale | 6-month post intervention | 13–18 | 0.16 | −0.04 | 0.36 |
Fostering Healthy Futures reported significantly better quality of life at post intervention (5 months post baseline) compared with the control group (d = 0.42, 95% CI 0.12 to 0.71). 26 No group differences existed at 6-month follow-up in the same cohort, and there were no significant differences observed in long-term quality of life measures in a later extension of the same study. 147 No group differences in quality of life were observed in the Wave-by-Wave intervention. 218 One pilot RCT measured quality of life using the EuroQol-5 Dimensions tool but the study did not present any data on group differences.
No RCT evaluations assessed subjective well-being or life satisfaction. There were insufficient data available to conduct meta-analysis for this outcome domain.
Mental, behavioural and neurodevelopmental disorders
In accordance with the evidence map, we classified mental, behavioural and neurodevelopmental disorders according to eight subdomains: total social, emotional and behavioural problems; social–emotional functioning; internalising behaviour problems; externalising behaviour problems; anxiety and depression; stress, PTSD and trauma; attachment style and disorder; attention and hyperactivity disorder.
Total social, emotional and behavioural problems
Some 16 interventions, with 22 RCT evaluations, reported outcomes relating to total social, emotional and behavioural problems (see Report Supplementary Material 14).
Shorter-term outcomes
Of the interventions, 6, with 10 RCT evaluations, did not demonstrate overall effectiveness for reduced short-term problem behaviours,103,128,163,166,167,175,181,185,210,221 while 1 evaluation did not present enough evidence to assess group differences. 171
Two evaluations of the KEEP intervention showed mixed results. In one US-based study, children aged between 6 and 11 years had significantly fewer carer-reported problem behaviours than control peers at 6-month follow-up (d = −0.26, 95% CI −0.43 to 0.09). 117 However, in a larger 2015 US study of the same intervention, there were no significant differences between intervention and control group children for carer-reported problem behaviours at 4-month follow-up (d = −0.01, 95% CI −0.22 to 0.21). 182
Evaluation of mentalisation-based therapy found that children and young people self-reported significant reductions in their problem behaviours at 12-week (d = −0.67, 95% CI −1.12 to −0.22) and 24-week (d = −0.76, 95% CI −1.21 to −0.31) follow-up. However, carer-reported problem behaviours demonstrated the opposite trend, with carers reporting that children in the intervention group showed more problem behaviours than the control group at 12 weeks (d = 0.31, 95% CI −0.09 to 0.71) and significantly more at 24 weeks (d = 0.34, 95% CI 0.04 to 0.84). 140
Evaluation of the brief and extended version of PCIT on children’s problem behaviour at 8- and 14-week follow-up, compared with a control group. 177 Carer-reported problem behaviours were significantly lower in the brief intervention group than control at 8-week follow-up (d = −0.64, 95% CI −1.16 to −0.12), but the difference was not significant at 14 weeks (d = −0.23, 95% CI −0.77 to 0.23). Children receiving the extended version of the intervention also had lower carer-reported problem behaviours at both follow-up times, but differences were not significant.
Young adolescents who received the ‘affective’ arm of the cognitive and affective bibliotherapy intervention showed lower total problem behaviours (as rated by counsellors) at 3-month follow-up than a control group (d = −1.02, 95% CI −1.60 to −0.44). No short-term improvements to problem behaviours were observed for participants in a parallel ‘cognitive’ arm of the trial.
Finally, evaluation of TFTC reported significantly improved short-term outcomes for problem behaviours among adolescents as compared with an active control group receiving the standard TFC. The intervention group had lower scores on the Parent Daily Report [β = 0.30, standard error (SE) = 0.11, p < 0.01] at 6-month follow-up.
Longer-term outcomes
Four interventions, with five RCT evaluations, did not demonstrate effectiveness for reduced problem behaviours at longer-term follow-up. 31,131,172,173,186 Two evaluations measured the effect of PMTO on longer-term child problem behaviours, with mixed results. In one US-based study, carer-reported problem behaviours were significantly lower in the intervention group compared to control at 12-month follow-up (d = −0.31, 95% CI −0.55 to −0.06). 166 However, implementation of the same intervention in the Netherlands showed no beneficial effect on carer-reported problem behaviours at 12 months (d = 0.00, 95% CI −0.35 to 0.35). 163 Teacher reported problem behaviours were higher in the intervention group at the same follow-up, though this did not reach significance (d = 0.37, 95% CI −0.12 to 0.86).
Young children whose carers who received Communication and Attachment training self-reported fewer total problem behaviours at 9-month follow-up compared to controls (d = −0.28, 95% CI −0.61 to 0.04), though the effect did not quite reach significance. However, teachers independently evaluating the same cohort reported the reverse pattern, with more problem behaviours in the intervention than the control group (d = 0.27, 95% CI −0.06 to 0.60). Again, this did not reach statistical significance. 178
Finally, young adolescents receiving the TFTC intervention showed significantly fewer problem behaviours on the parent daily report at 12-month follow-up than an active control group receiving the TFC intervention (β = −0.38, SE = 0.14, p < 0.05).
Meta-analysis of shorter- and longer-term follow-up
A total of 13 interventions, with 15 RCT evaluations, were eligible for inclusion in the meta-analysis of total problem behaviours. Seven RCT evaluations were ineligible: three were moderation analyses or reused analysis from other included evaluations,175,210 two evaluations used an active control group,172 and two did not provide sufficient information to extract effect sizes. 173 We undertook separate meta-analyses to investigate the effect of interventions on total problem behaviours measured at shorter-term (0–6 months of follow-up) and longer-term (> 6 months of follow-up) follow-up. Collectively, interventions significantly reduced problem behaviours in the short term (d = −0.15, 95% CI −0.28 to −0.02; Figure 7). The short-term meta-analysis included 20 effect sizes from 11 evaluations, with substantial between-studies heterogeneity (I2 = 62%). However, there was no evidence that interventions reduced total problem behaviours at longer-term follow-up (d = −0.07, 95% CI −0.38 to 0.25; Figure 8). For the longer-term follow-up meta-analysis, we included 12 effect sizes from 6 evaluations and observed moderate heterogeneity (I2 = 56%).
FIGURE 7.
Forest plot for meta-analysis of total problems (short term).
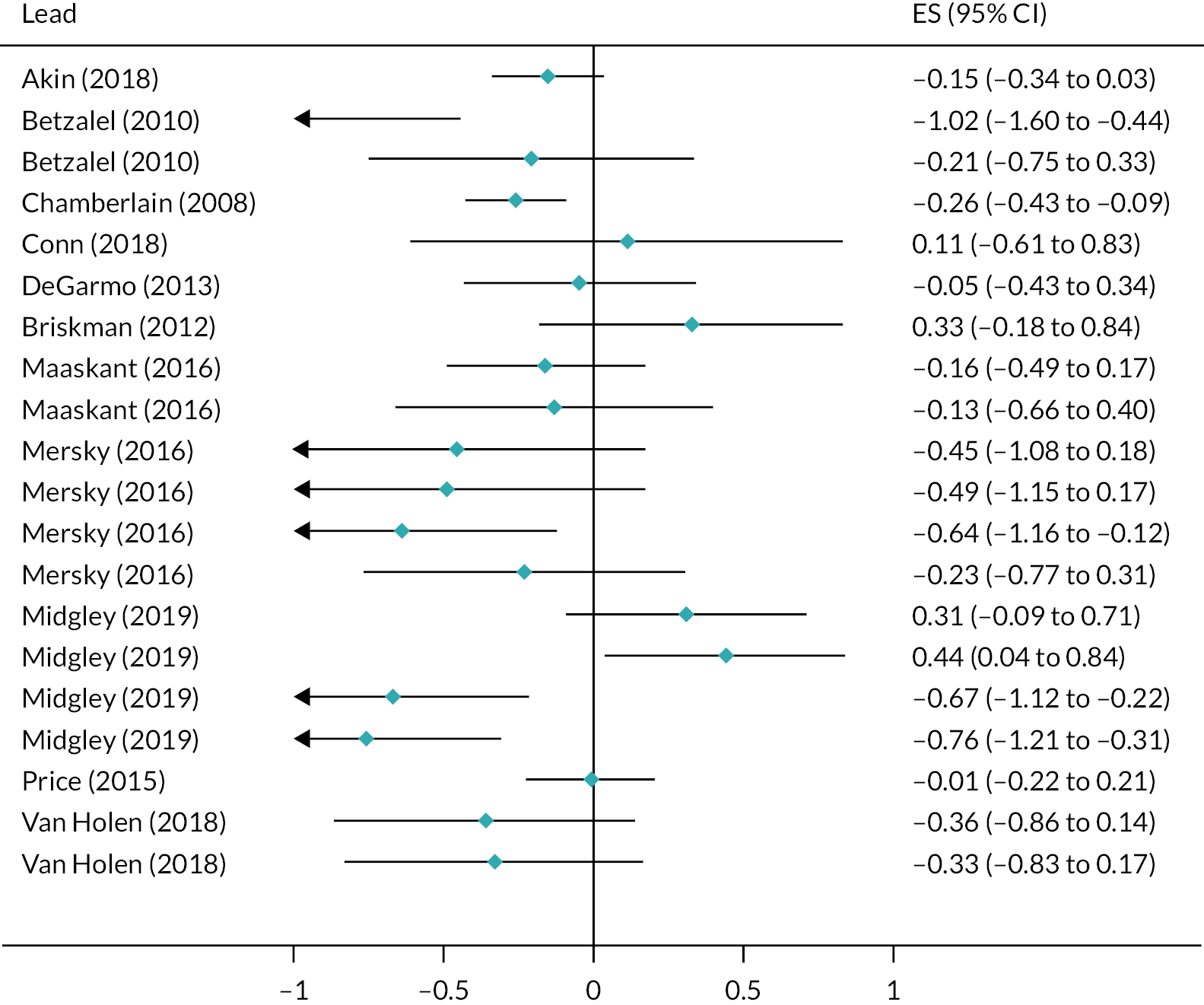
FIGURE 8.
Forest plot for meta-analysis of total problems (long term).
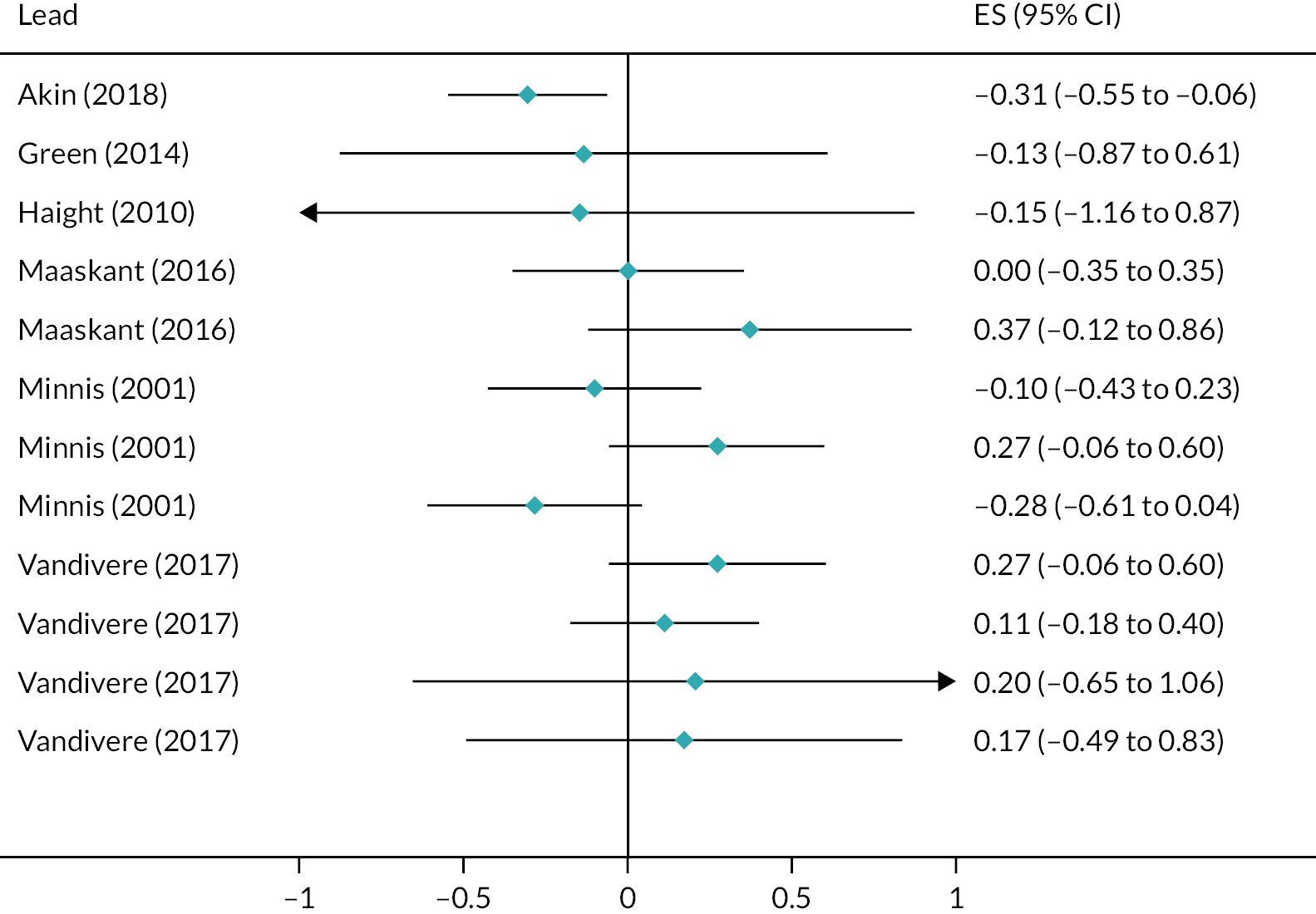
Total social–emotional functioning and/or impaired functioning
Of the interventions, 18, with 24 RCT evaluations and 1 QED evaluation, reported outcomes relating to social, emotional and behavioural functioning and/or impaired functioning (see Report Supplementary Material 14).
Shorter-term outcomes
Eight interventions, with eight RCT evaluations, demonstrated no effectiveness for reducing short-term social–emotional functioning difficulties. 142,158,162,165,172,183,218,221
Five interventions, with five study reports, demonstrated effectiveness in improving some aspect short-term functioning in children and young people. The Fostering Changes intervention reported significantly lower carer-rated scores than children in the control group for emotional difficulties (d = −0.33, 95% CI −0.60 to −0.06), total difficulties (d = −0.32, 95% CI −0.59 to −0.05) and peer problems (d = −0.28, 95% CI −0.56 to −0.01) at 3-month follow-up. 179 No significant group differences were found in an earlier UK evaluation of the same intervention. 221 Children in the ‘extended’ arm of the HealthRHYTHMS musical therapy intervention rated themselves as having significantly fewer interpersonal problems at 6-week follow-up (d = −0.90, 95% CI −1.60 to −0.20), while children in the standard intervention arm showed no difference from control group participants. There were no significant differences from control group participants for either group (standard or extended) on child-rated social adaptation scores or clinician-rated total functioning scores at 6 weeks. 169
In the PMTO intervention, children had significantly lower carer-rated social–emotional functioning scores than the usual care group at 6-month follow-up (d = −0.19, 95% CI −0.35 to −0.04). 166 Young children who had received PCIT were rated by foster carers as having significantly lower scores on the ‘lability/negativity’ scale of the Emotional Regulation Checklist measure than control group participants (d = −0.67, 95% CI −1.15 to −0.19). 212 Finally, adolescents in the intervention arm of the TFTC had lower 6-month follow-up scores than an active control group (TFC) for Behavioural and Emotional Ratings Scale (β = 0.41, SE = 0.12, p < 0.01) and higher scores for the strengths component of the Strengths and Difficulties Questionnaire (SDQ; β = −0.24, SE = 0.11, p < 0.05). 172
Longer-term outcomes
Six interventions, with seven associated RCT evaluations, showed no effectiveness at reducing long-term social and emotional functioning difficulties. 27,31,122,154,162,179,209
Three interventions showed some effectiveness at improving longer-term functioning outcomes. Evaluation of PMTO-reported children had significantly lower social–emotional functioning scores (as rated by carers) than the control group at 12-month follow-up (d = −0.38, 95% CI −0.57 to −0.19), with the between group difference increasing between 6- and 12-month follow-up. 166 Young foster children who took part in the FHF intervention had significantly lower scores on a multi-informant, composite ‘mental health functioning’ outcome, compared with control group participants, at 18 months (d = −0.25, 95% CI −0.47 to −0.04). Linked FHF study reports showed some moderating effects of risk exposure and relationship history on these outcomes. 115,116
Finally, a QED evaluation of the TST assessed the effect of increased child-level exposure to care agencies trained in trauma-informed practices, looking at trajectories in measures of child functioning, emotional regulation and behavioural regulation. 34 Change in functioning was not predicted by overall dosage, but increases in dosage were associated with decreased challenges with functioning (r = −0.37). For emotional regulation, overall dosage was associated with improvements in functioning over time (β = −0.18) but there was no significant correlation between increases in dosage and improvements in emotional regulation. Finally, change in behavioural regulation was not predicted by overall dosage, but increases in dosage over time were associated with temporal improvements in behavioural regulation (r = −0.17).
Meta-analysis of shorter-term and longer-term follow-up
A total of 9 interventions, with 16 RCT evaluations, were eligible for inclusion in the meta-analysis of total functioning. Eight RCT evaluations were ineligible: four were moderation analyses or reused analysis from other included evaluations;115,116,167,210 three evaluations used an active control group;158,172,181 and one did not provide sufficient information to extract effect sizes. 118 We undertook separate meta-analyses to investigate the effect of interventions on social–emotional functioning difficulties at short-term (0–6 months follow-up) and long-term (7 + months) follow-up. Collectively, interventions significantly reduced social–emotional functioning difficulties in the short term (d = −0.18, 95% CI −0.31 to −0.05; Figure 9). The analysis included 28 effect sizes from 10 evaluations, with moderate between-studies heterogeneity (I2 = 53%).
FIGURE 9.
Forest plot for meta-analysis of total functioning (short term).
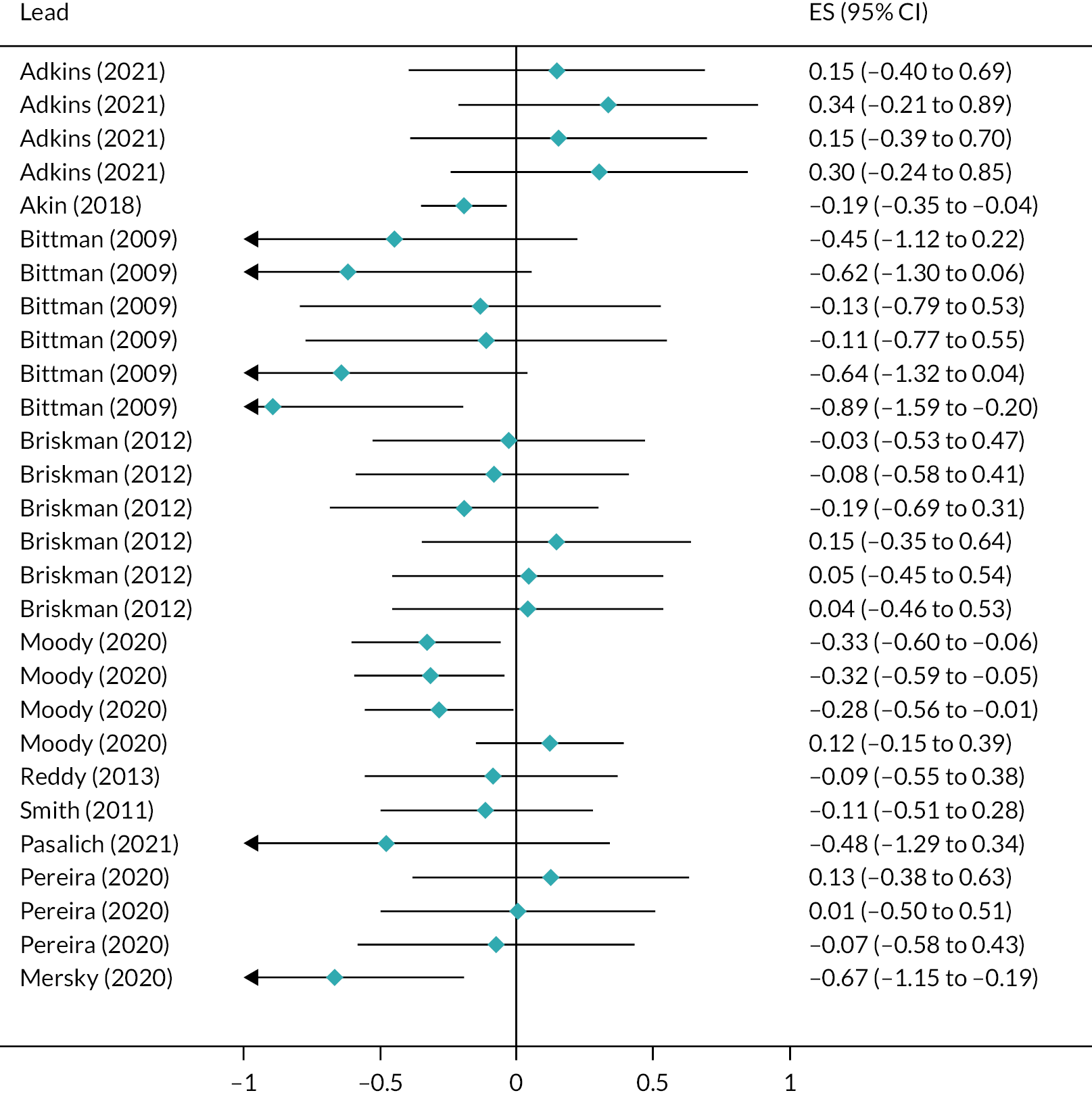
When evaluated at longer-term follow-up, interventions showed some effect at reducing social–emotional functioning difficulties, with the effect approaching but not reaching statistical significance (d = −0.15, 95% CI −0.40 to 0.09; Figure 10). For longer-term follow-ups, we included 14 effect sizes from 8 evaluations and observed substantial heterogeneity (I2 = 63%).
FIGURE 10.
Forest plot for meta-analysis of total functioning (long term).
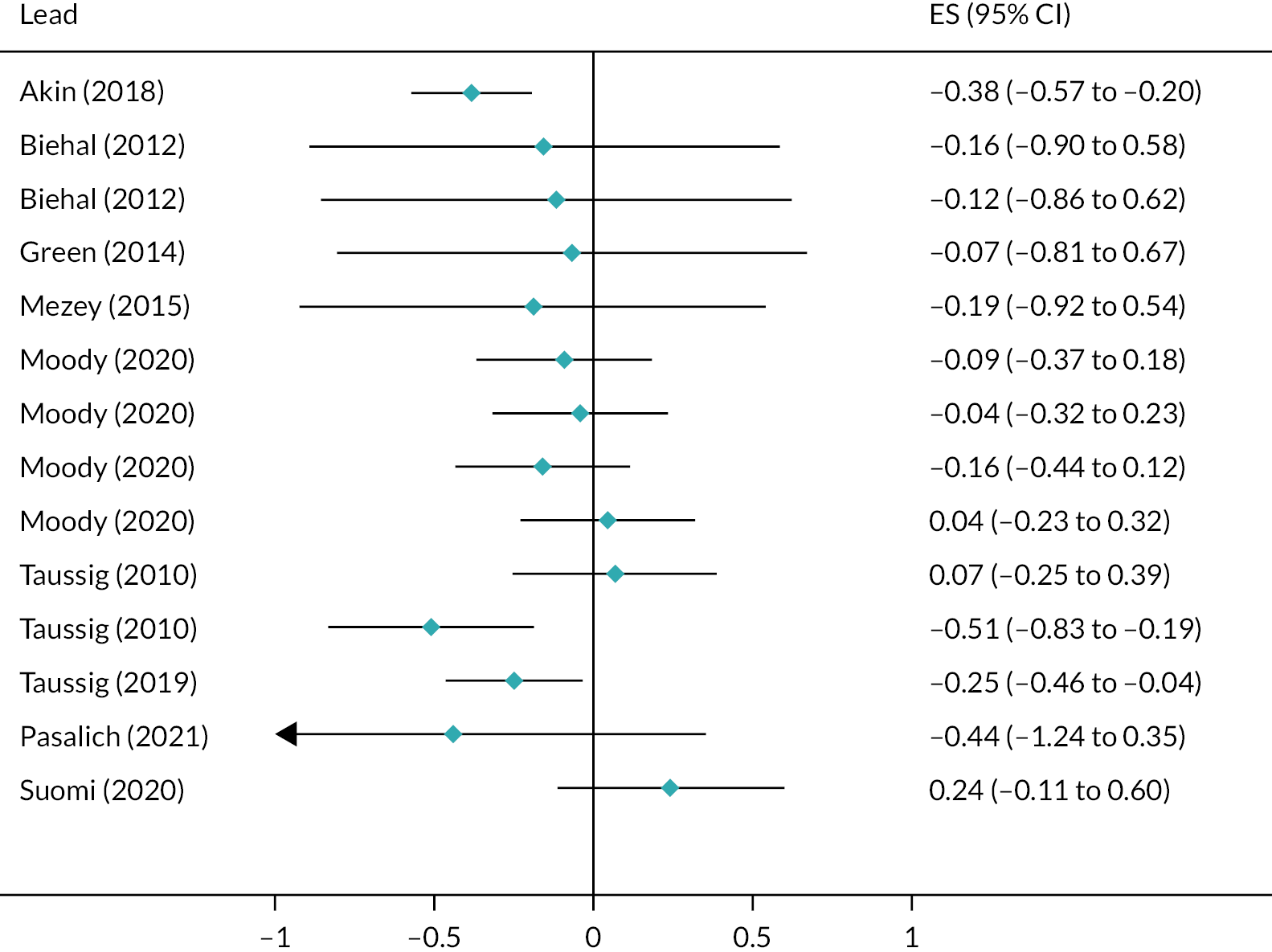
Internalising behaviour problems
A total of 22 interventions, with 22 RCT evaluations and 1 QED evaluation, reported outcomes relating to internalising behaviour problems. Total internalising behaviour problems were most commonly assessed by the internalising sub-scale of the Child Behaviour Checklist (CBCL) tool, with assessments primarily made by parents or carers (see Report Supplementary Material 14).
Shorter-term outcomes
Nine interventions, with nine evaluations, showed no effectiveness in reducing short-term internalising problem behaviours. 113,128,158,163,169,180,181,185,212
Young adolescents in the ‘cognitive’ arm of the cognitive and affective bibliography intervention showed significantly better outcomes at 3-month follow-up compared with the control group for clinician-rated internalising problems (d = −0.77, 95% CI −1.33 to −0.21) and withdrawal (d = −0.75, 95% CI −1.31 to −0.18), but not psychosomatic problems (d = 0.00, 95% CI −0.54 to 0.54). However, participants in the ‘affective’ arm of the same intervention did not differ from control group participants on any of the outcomes at 3 months post intervention. 168
Infants whose carers had received the ABC intervention showed significantly lower rates of carer-rated internalising behaviour problems compared with control participants at 6-month follow-up (d = −1.60, 95% CI −2.22 to −0.98). 184 KEEP reported that children were significantly less likely than the control group to show clinical (d = −0.23, 95% CI −0.45 to −0.01) or borderline-level scores (d = −0.23, 95% CI −0.45 to −0.01) on the internalising behaviour problems scale of the CBCL scale, as assessed by carers at 6 months. There were no group differences in somatic complaints, and the absolute difference in continuous scores on the internalising scale did not reach significance. 29
Finally, young children who had taken part in mentalisation‐based therapy self-reported significantly lower levels of internalising behaviour problems than control group children, at both 12-week (d = −1.04, 95% CI −1.54 to −0.54) and 24-week (d = −1.30, 95% CI −1.80 to −0.80) follow-up. However, assessment of internalising problems made by carers showed the opposite trend, with intervention group children scoring significantly higher than those in the control group at 12-week (d = 0.35, 95% CI 0.00 to 0.70) and 24-week (d = 0.48, 95% CI 0.13 to 0.80) follow-up.
Longer-term outcomes
Seven interventions, with six RCT evaluations and one QED evaluation, showed no effectiveness for reducing internalising behaviour problems at long-term follow-up. 131,163,170,173,174,186,209
The Take Charge intervention showed lower scores for young people than control group peers for carer-rated somatic complaints at 12-month follow-up (d = −0.30, 95% CI −0.65 to 0.06), although the difference did not reach statistical significance. At the 18-month follow-up, the difference between groups persisted and was significant (d = −0.54, 95% CI −0.90 to −0.18).
Meta-analysis for shorter- and longer-term outcomes
A total of 18 interventions, with 18 RCT evaluations, were eligible for inclusion in the meta-analysis of total functioning. Four RCT evaluations were ineligible. One reused analysis from another included evaluation,175 and one did not provide sufficient data to calculate effect sizes,173 while two evaluations used an active control group. 158,181 We undertook separate meta-analyses to investigate the effect of interventions on internalising problem behaviours measured at short-term (0–6 months) and long-term (> 6 months) follow-up. Collectively, interventions significantly reduced internalising problem behaviours in the short term (d = −0.35, 95% CI −0.61 to −0.08; Figure 11). The analysis included 32 effect sizes from 12 evaluations, with substantial between-studies heterogeneity (I2 = 74%).
FIGURE 11.
Forest plot for meta-analysis of total internalising problems (short term).
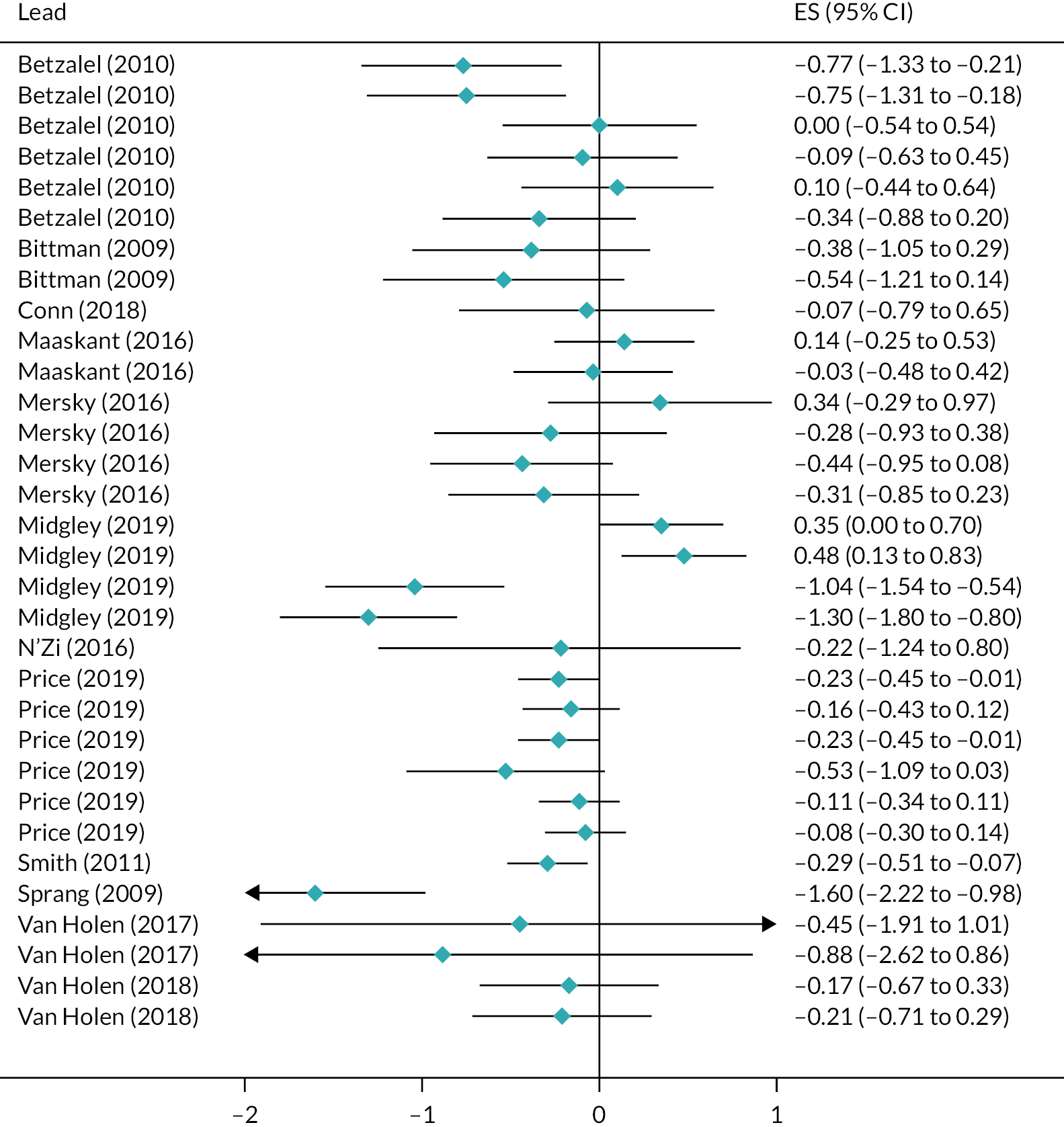
However, there was no evidence that interventions reduced internalising problem behaviours when evaluated at longer-term follow-up (d = −0.03, 95% CI −0.31 to 0.25) (Figure 12). For longer-term follow-up, we included 16 effect sizes from 7 evaluations and observed moderate heterogeneity (I2 = 53%).
FIGURE 12.
Forest plot for meta-analysis of total internalising problems (long term).
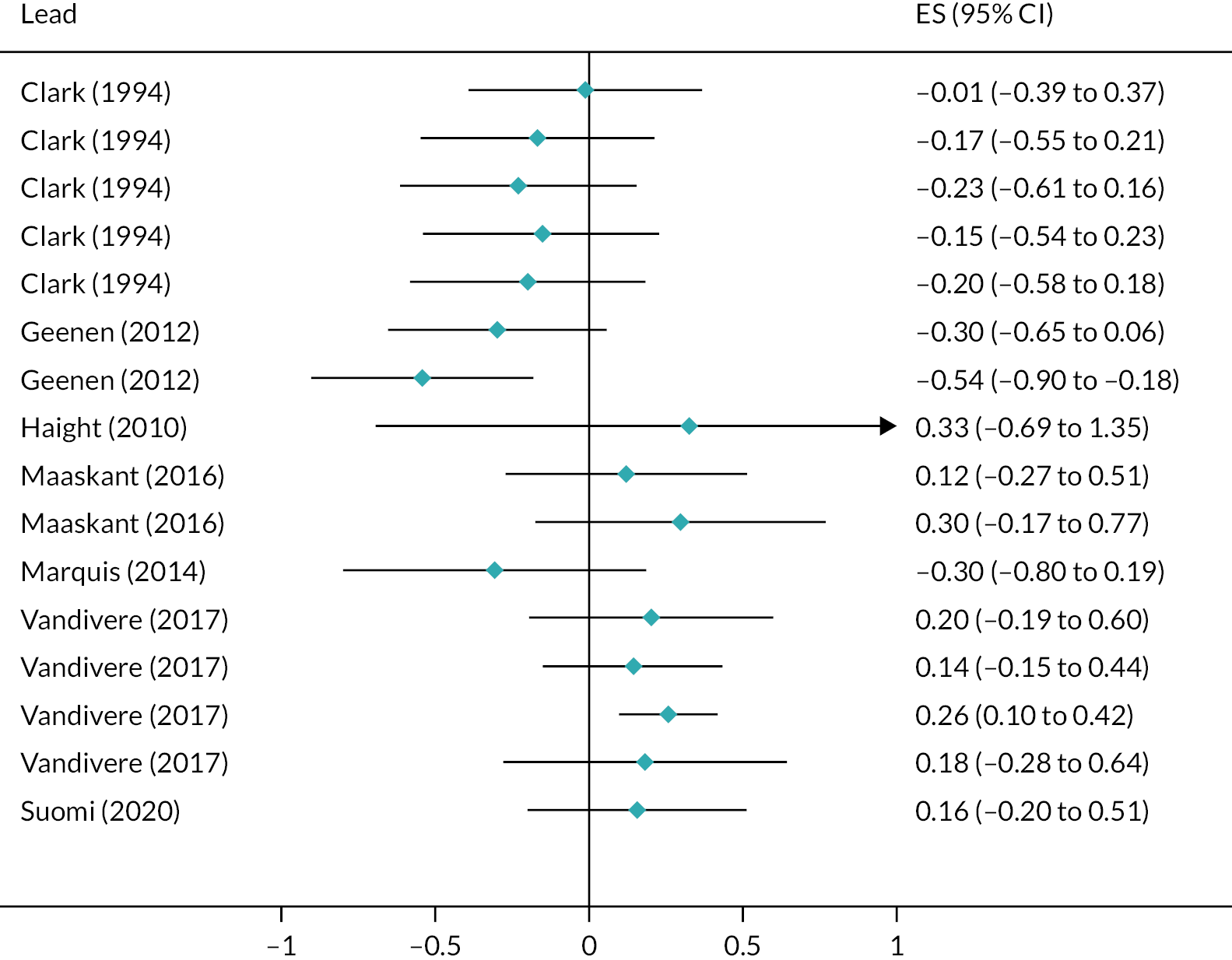
Externalising behaviour problems
A total of 32 interventions, with 30 associated RCT evaluations and 2 QED evaluations, reported outcomes relating to externalising behaviour problems. Total externalising behaviour problems were most commonly assessed by the externalising subscale of the CBCL tool, with assessments primarily made by parents or carers (see Report Supplementary Material 14).
Shorter-term outcomes
Some 13 interventions, with 13 outcome evaluations, demonstrated no effectiveness at reducing children and young people’s externalising problems in the short term. 29,33,113,128,140,158,165,174,177,179–181,185
Eight interventions demonstrated effectiveness for short-term reductions in externalising problem behaviours. Young adolescents in the ‘extended’ arm of a musical therapy intervention, HealthRHYTHMS, self-reported significantly lower levels of anger at 6-week follow-up compared with control group peers (d = −0.94, 95% CI −1.64 to −0.24). Adolescents receiving the standard intervention did not differ from controls for self-reported anger at follow-up, and neither intervention group differed from controls at 6-week follow-up for self-reported aggression. 169
Carers who had taken part in the ABC intervention rated children as having significantly fewer externalising problem behaviours than controls at 6-week follow-up (d = −1.80, 95% CI −2.44 to −1.16). 184 Adolescents who received the ‘affective’ arm of the cognitive and affective bibliography intervention (including discussions about their emotional reactions) were rated by clinicians as significantly lower than control group participants for total externalising behaviour problems (d = −1.07, 95% CI −1.65 to −0.49), delinquency (d = −0.99, 95% CI −1.57 to −0.41) and aggression (d = −0.96, 95% CI −1.54 to −0.39), 3 months after the intervention. Participants in a parallel ‘cognitive’ arm of the intervention (with more focus on coping techniques) were rated lower than control groups on the same measures, but unlike those in the ‘affective’ arm, the differences did not reach statistical significance. 168
Young adolescents who took part in the Dojo: Biofeedback videogame intervention self-reported significantly lower levels of externalising problem behaviours compared with control group peers, both post intervention and at 6-month follow-up. 143 However, independent ratings from carers showed no difference from control group participants on the same measure at either time point.
Foster carers who took part in a brief skills-based intervention rated their young foster children’s externalising behaviour problems as significantly lower than those in a control group, at 6-month follow-up (d = −0.09, 95% CI −0.16 to −0.02). 183
Young children of foster carers who took part in the kConnect intervention had significantly lower scores for carer-rated ‘affect dyscontrol’ than control group participants at post-intervention follow-up (d = −0.97, 95% CI −1.81 to −0.12),209 while children taking part in the PMTO intervention also had lower carer-rated scores than a control group for externalising problems at 6-month follow-up (d = −0.33, 95% CI −0.66 to 0.00). 163
Finally, evaluation of KEEP reported that a lower proportion of children were rated by their carers at 6-month follow-up as having ‘rule breaking’ scores on the CBCL measure that exceeded the ‘borderline’ threshold (d = −0.293, 95% CI −0.57 to −0.01). 29 However, no differences were found between groups for children who reached the ‘clinical’ cut-off threshold or when continuous scores were compared. Similarly, no differences were found in carer ratings of total externalising behaviour problems or aggression.
Long-term outcomes
A total of 12 interventions, with 11 RCT evaluations and 1 QED evaluation, showed no effectiveness for reduced externalising behaviour problems at long-term follow-up. 35,118,131,157,162,163,173,176,179,186,187,209
Two interventions were effective at reducing externalising behaviour problems. Young children who received FIAP self-rated their externalising behavioural problems (d = −0.43, 95% CI −0.82 to −0.05) and aggression (d = −0.42, 95% CI −0.80 to −0.03) as being significantly lower than control group children at 18-month follow-up. There were no differences between groups for self-rated delinquency and no group differences for any of the measures when assessed independently by carers at 18 months. 170 The CARE intervention reported a significant longitudinal improvement in the slope of incidents relating to aggression towards residential care staff among foster children who attended residential homes whose staff had been trained in trauma-informed care (programme effect: β = 0.87, 95% CI 0.81 to 0.94).
Meta-analysis for shorter- and longer-term outcomes
A total of 23 interventions, with 24 associated RCT evaluations, were eligible for inclusion in the meta-analysis of externalising problems. Six RCT evaluations were ineligible: one reused analysis from another included evaluation,210 two evaluations used an active control group158,181 and three evaluations presented insufficient information to calculate effect sizes. 35,118,173 We undertook separate meta-analyses to investigate the effect of interventions on externalising problem behaviours measured at short-term (0–6 months) and long-term (> 6 months) follow-up. Collectively, interventions significantly reduced externalising problem behaviours in the short term (d = −0.30, 95% CI −0.53 to −0.08; Figure 13). The analysis included 44 effect sizes from 18 evaluations, with substantial between-studies heterogeneity (I2 = 73%).
FIGURE 13.
Forest plot for meta-analysis of total externalising problems (short term).
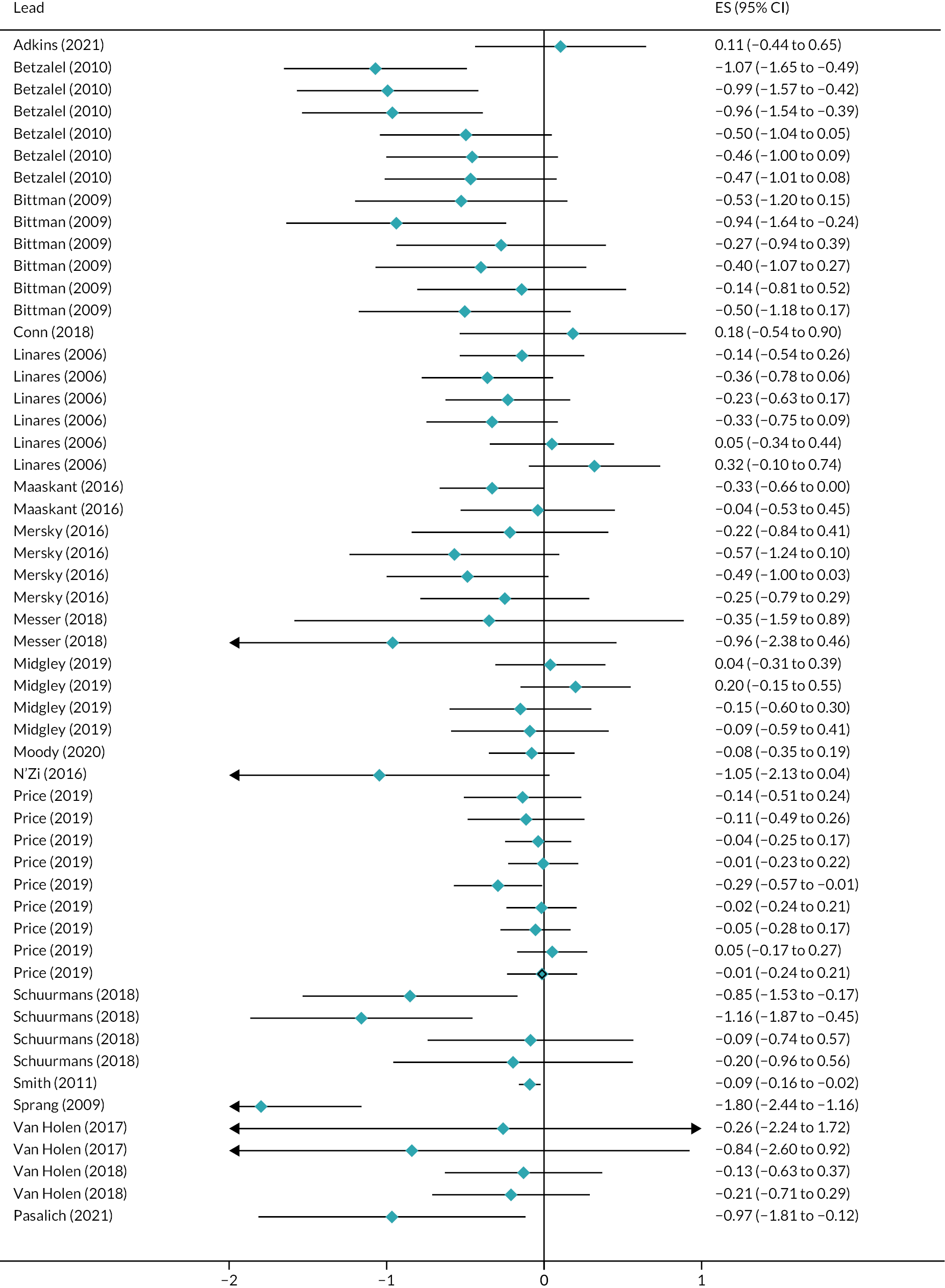
There was, however, no evidence that interventions reduced externalising problem behaviours when evaluated at longer-term follow-up (d = 0.02, 95% CI −0.17 to 0.20; Figure 14). For longer-term follow-up periods, we included 19 effect sizes from 9 evaluations and observed moderate heterogeneity (I2 = 45%).
FIGURE 14.
Forest plot for meta-analysis of total externalising problems (long term).
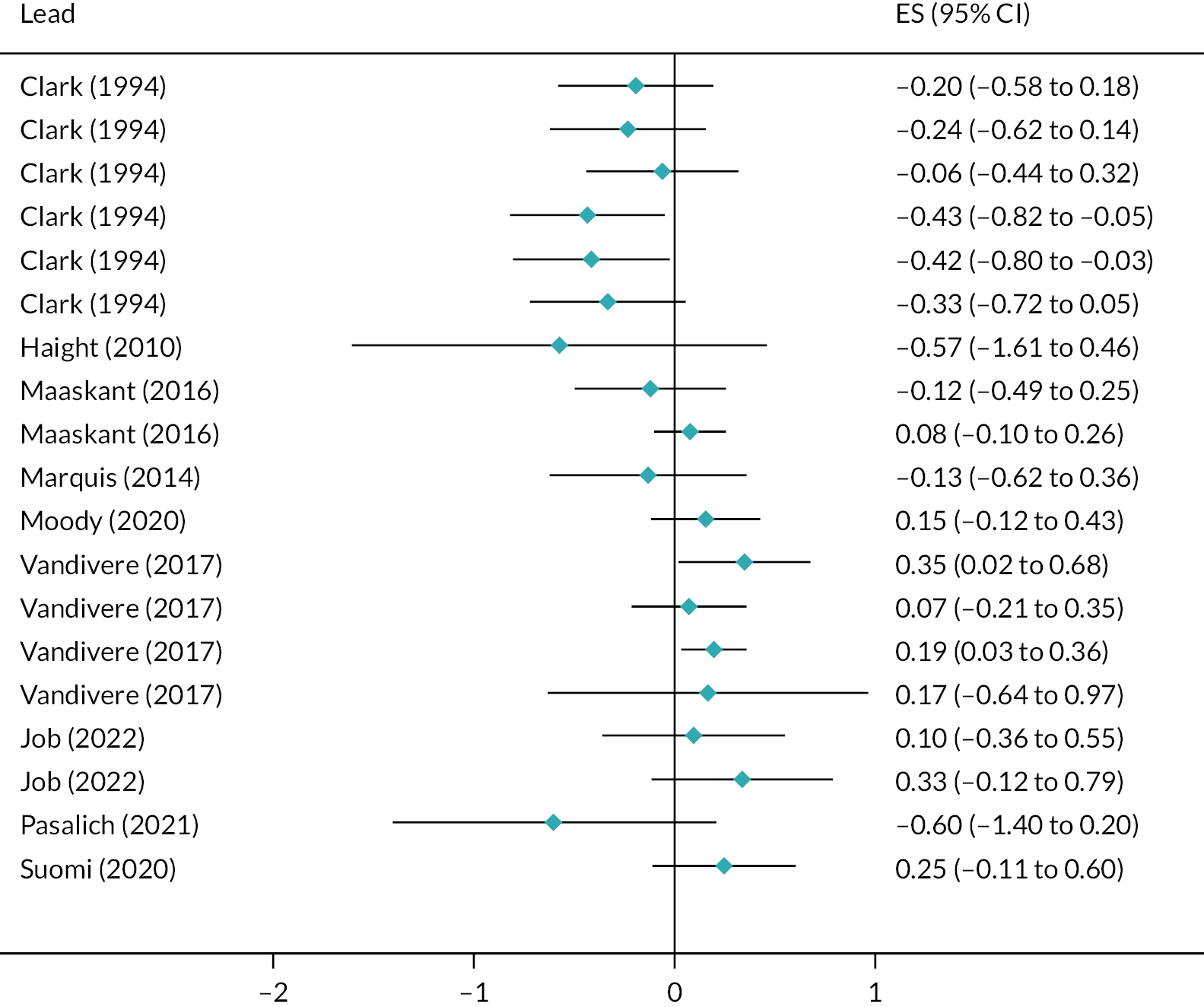
Anxiety and depression
Some 12 interventions, with 12 associated RCT evaluations, reported outcomes relating to anxiety and depression. They were most commonly assessed via the Revised Children’s Manifest Anxiety Scale or CBCL by self-report from children and young people (see Report Supplementary Material 14).
Shorter-term outcomes
Five interventions, with five RCT evaluations, demonstrated no effectiveness for reducing anxiety and/or depression in children and young people. 135,142,143,169,218
Three interventions showed some short-term effectiveness. Children in the PMTO intervention were significantly less likely than control peers to reach the ‘borderline’ threshold on the withdrawn and depressed subscale of the CBCL, as assessed by carers (d = −0.35, 95% CI −0.61 to −0.10). However, no group differences were observed for the ‘clinical’ threshold or differences in continuous scores and there were no group differences for scores on the anxiety and depression subscale. 29 Adolescents in residential foster care receiving the ‘affective’ arm of the cognitive and affective bibliotherapy intervention had significantly lower levels of clinician-assessed scores on the anxiety and depression subscale of the teacher report form compared with controls at 6-month follow-up (d = −0.73, 95% CI −1.30 to −0.17). However, there were no differences compared with control on several other anxiety measures for either the ‘affective’ or ‘cognitive’ intervention groups, at either 3- or 6-month follow-up points. 168 Finally, young children in foster care whose carers had taken part in the CARE intervention were reported by carers to have significantly lower anxiety scores at 3-month follow-up (d = −1.59, 95% CI −3.03 to −0.14). No differences were found for the same outcome at 1-month follow-up, or for depression scores at either follow-up point. 33
Longer-term outcomes
Three RCT evaluations of three interventions showed no effectiveness for reducing depression and/or anxiety in children and young people. 27,157,170
Young adolescent children in foster care who took part in the Take Charge mentoring intervention showed significantly lower scores at long-term follow-up in a series of measures: carer-rated anxiety and depression scores at 12-month (d = −0.65, 95% CI −1.02 to −0.29) and 18-month (d = −0.36, 95% CI −0.71 to −0.00) follow-up; carer-rated withdrawal and depression scores at 12-month (d = −0.41, 95% CI −0.77 to −0.05) and 18-month (d = −0.37, 95% CI −0.73 to −0.01) follow-up; and self-rated anxiety and depression at 12-month (d = −0.44, 95% CI −0.79 to −0.08) follow-up. 159
Meta-analysis of shorter-term outcomes
Eight interventions, with eight RCT evaluations, were eligible for inclusion in the short-term meta-analysis of anxiety and depression. There were insufficient available effect sizes to conduct a meta-analysis of long-term (> 6 months of follow-up) intervention effects. Collectively, interventions significantly reduced scores on measures of anxiety and depression in the short term (d = −0.26, 95% CI −0.40 to −0.13), relative to control groups (Figure 15). The analysis included 40 effect sizes from 8 evaluations, with minimal between-studies heterogeneity (I2 = 8%).
FIGURE 15.
Forest plot for meta-analysis of anxiety and depression (short term).
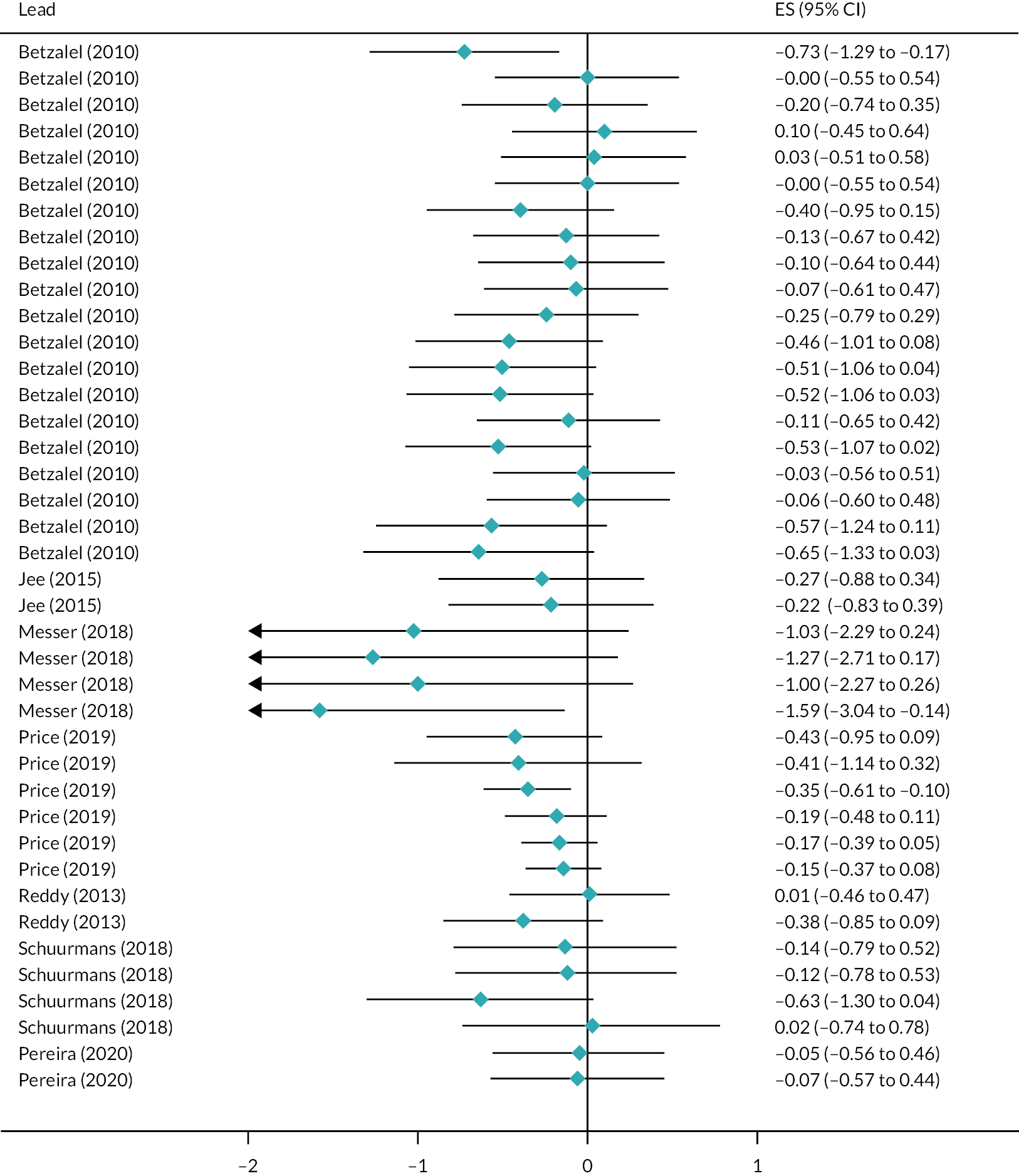
Stress, post-traumatic stress disorder and trauma
Four interventions, with seven RCT evaluations, reported outcomes relating to stress, PTSD or trauma (Table 6). Outcomes were most commonly assessed via the Trauma Symptom Checklist for Young Children by child self-report. Three interventions showed no evidence of effectiveness. 33,131,158 There was evidence of longer-term effectiveness from two separate evaluations of the FHF intervention. Foster children self-reported significantly fewer dissociation symptoms at 6 months post intervention in a 2010 evaluation (d = −0.39, 95% CI −0.70 to −0.08) and subsequent 2019 evaluation (d = −0.29, 95% CI −0.50 to −0.09). No significant group differences were found for post-traumatic symptoms in either evaluation. 26,147 There were insufficient data available to conduct meta-analysis for this outcome domain.
| Intervention | Study design | Intervention length (weeks) | Outcome assessed | Tool | Informant | Data type | Follow-up | Follow-up (category) (months) | Effect size | 95% CI (low) | 95% CI (high) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Stress and post-traumatic stress outcomes | |||||||||||
| CARE33 | RCT | 4 | PTS arousal | TSCYC | Parent/carer | Scale | 1-month follow-up | 0–3 | −0.72 | −1.97 | 0.53 |
| 3-month follow-up | 4–6 | −1.01 | −2.44 | 0.41 | |||||||
| FHF26 | RCT | 30 | Post-traumatic symptoms | TSCYC | Child/young person | Scale | Post intervention | 7–12 | −0.10 | −0.42 | 0.22 |
| Dissociation symptoms | −0.13 | −0.45 | 0.19 | ||||||||
| Post-traumatic symptoms | 6-month post intervention | 13–18 | −0.30 | −0.63 | 0.02 | ||||||
| Dissociation symptoms | −0.39 | −0.70 | −0.08 | ||||||||
| FHF147 | RCT | 30 | Post-traumatic symptoms | TSCYC | Child/young person | Scale | 6-month post intervention | 13–18 | −0.20 | −0.40 | 0.00 |
| Dissociation symptoms | −0.29 | −0.49 | −0.09 | ||||||||
| FHF116 | RCT | 30 | Post-traumatic symptoms | TSCYC | Child/young person | Scale | 6-month post intervention | 13–18 | Moderation analysis | ||
| Dissociation symptoms | |||||||||||
| FHF115 | RCT | 30 | Post-traumatic symptoms | TSCYC | Child/young person | Scale | 6-month post intervention | 13–18 | Moderation analysis | ||
| Dissociation symptoms | |||||||||||
| Life Story131 | RCT | 28 | PTSD/disassociation | CBCL | Parent/carer | Scale | 12-month follow-up | 7–12 | 0.00 | −1.01 | 1.01 |
| TF-CBT plus evidence-based engagement strategies158 | RCT | 13 | PTSD severity | PTSD-RI | Parent/carer | Scale | Post test | 0–3 | Insufficient data to estimate effect size | ||
| 3-month follow-up | 4–6 | ||||||||||
| Attachment style and disorder outcomes | |||||||||||
| Communication and Attachment Training for Foster Carers178 | RCT | 3 | RADS score | RADS | Parent/carer | Scale | 9-month follow-up | 7–12 | −0.13 | −0.46 | 0.19 |
| Attention and hyperactivity disorder outcomes | |||||||||||
| Family Minds165 | RCT | 5 | Hyperactivity–inattention | SDQ | Parent/carer | Scale | 6-week follow-up | 0–3 | 0.34 | −0.21 | 0.89 |
| Fostering Changes179 | RCT | 12 | Hyperactivity–inattention | SDQ | Parent/carer | Scale | 3-month follow-up | 0–3 | 0.87 | 0.59 | 1.15 |
| 12-month follow-up | 7–12 | −0.07 | −0.35 | 0.20 | |||||||
Attachment style and disorder
One intervention, with one study report assessed child attachment disorder according to the carer Reactive Attachment Disorder Scale178 (see Table 6). There was no evidence of effective at 9-month follow-up. There were insufficient data available to conduct a meta-analysis for this outcome domain.
Attention and hyperactivity disorder
Two interventions, with two associated evaluations, reported outcomes for children and young people’s attention and hyperactivity, both measured by the SDQ via care report (see Table 6). Neither intervention demonstrated effectiveness. 165,179 There were insufficient data available to conduct a meta-analysis for this outcome domain.
Suicide-related outcomes
Three interventions, with two RCT evaluations and one QED evaluation, assessed suicide-related outcomes. One RCT evaluation of a peer mentoring intervention to reduce teenage pregnancy-assessed attempted suicide,27 and a second musical therapy intervention measured self-reported suicidal ideation. 169 Both evaluations also measured self-harm episodes. No significant group differences were noted. One other QED study of the CARE intervention measured self-harm incidents and found no significant intervention effect. There were insufficient data available to conduct meta-analysis for this outcome domain. 191
Grading of Recommendations Assessment, Development and Evaluation of outcome evaluations
We constructed GRADE evidence assessments for each of the three primary outcome domains and subdomains, for both short- and long-term outcomes. 220 Assessments were completed in GRADEpro software (McMaster University and Evidence Prime, www.gradepro.org), and PET-PEESE (precision-effect test and precision-effect estimate with standard error) analysis was conducted to evaluate selection bias. 221 We assessed evidence from RCTs according to five factors: RoB, inconsistency, indirectness, imprecision and publication bias.
For short-term outcomes, we assessed there to be low certainty of effectiveness for interventions targeting total problem behaviours, social–emotional functioning and externalising problems (see Report Supplementary Material 15). For each of these domains, we assessed a serious RoB and serious imprecision. All other outcome domains were assessed as being very low certainty of evidence, based on serious RoB and very serious imprecision. All long-term outcome domains were assessed as having very low certainty of effectiveness due to the same RoB and serious imprecision concerns (see Report Supplementary Material 16).
Equity harms synthesis
We considered the equity harms associated with interventions. In total, 14 studies linked to 8 interventions reported moderator analysis or interaction effects. Using the PROGRESS-Plus schema for intervention harms as an initial organising framework, we inductively coded review-specific equity domains from included study reports. 222 These domains were: children and young people’s age; children and young people’s gender; children and young people’s ethnicity; children and young people’s baseline mental health problems; children and young people’s history of maltreatment; placement type and placement changes; birth parent and carer characteristics; other additional equity harms. We mapped these equity domains according to the three primary outcomes domains: subjective well-being, mental, behavioural and neurodevelopmental disorders, and suicide-related behaviours. For outcomes where three of more different evaluations reported on a specific equity harm, we constructed harvest plots.
Subjective well-being
Three studies reported five equity harms related to subjective well-being, which were all related to Fostering Healthy Futures (FHF) . Evaluations reported that there were no differential effects for a number of sociodemographic and care placement characteristics: children and young people’s gender; ethnicity; intelligence quotient (IQ); baseline mental health problems; quality of relationship with foster carers; placement type (foster care vs. kinship care). 115,147
Three study reports linked to the same evaluation examined the interaction of history of maltreatment and quality life. One study report found that FHF had a stronger effect for children exposed to fewer adverse childhood experiences (ACEs). 147 This was a composite measure of physical abuse, sexual abuse, removal from a single parent household, exposure to community violence, caregiver transitions and school transitions. This finding was not replicated in other analyses. 111,147 There was indication that the intervention was more effective for children with poorer relationship quality with their birth parents and for those who have had fewer caregivers. 115
Mental, behavioural and neurodevelopmental disorders
A total of 8 interventions, with 14 associated study reports, considered equity harms for mental, behavioural and neurodevelopmental disorders.
Children and young people’s age
Four studies reported on the moderating effect of children and young people’s age on mental, behavioural and neurodevelopmental disorders (Figure 16).
FIGURE 16.
Equity harms for mental health, behavioural and neurodevelopmental disorders by children and young people’s age. Notes: Price et al. (2015)182 (¼ bar); DeGarmo et al. (2013)103 (¼ bar); Smith et al. (2011)183 (¼ bar); Dozier et al. (2006)171 (4/4 bar). Height of bars represent the nature of the evidence presented by the trial: full height – significant moderation for a given outcome; three-quarter height – pattern of moderation estimates including some significant moderation; half height – non-significant moderation trending in one direction; one-quarter height – only non-significance reported. Shading of bars represent time to outcome at follow-up: blue – short-term outcomes of < 6 months post baseline; red – long-term outcomes of 6 months or more post baseline.
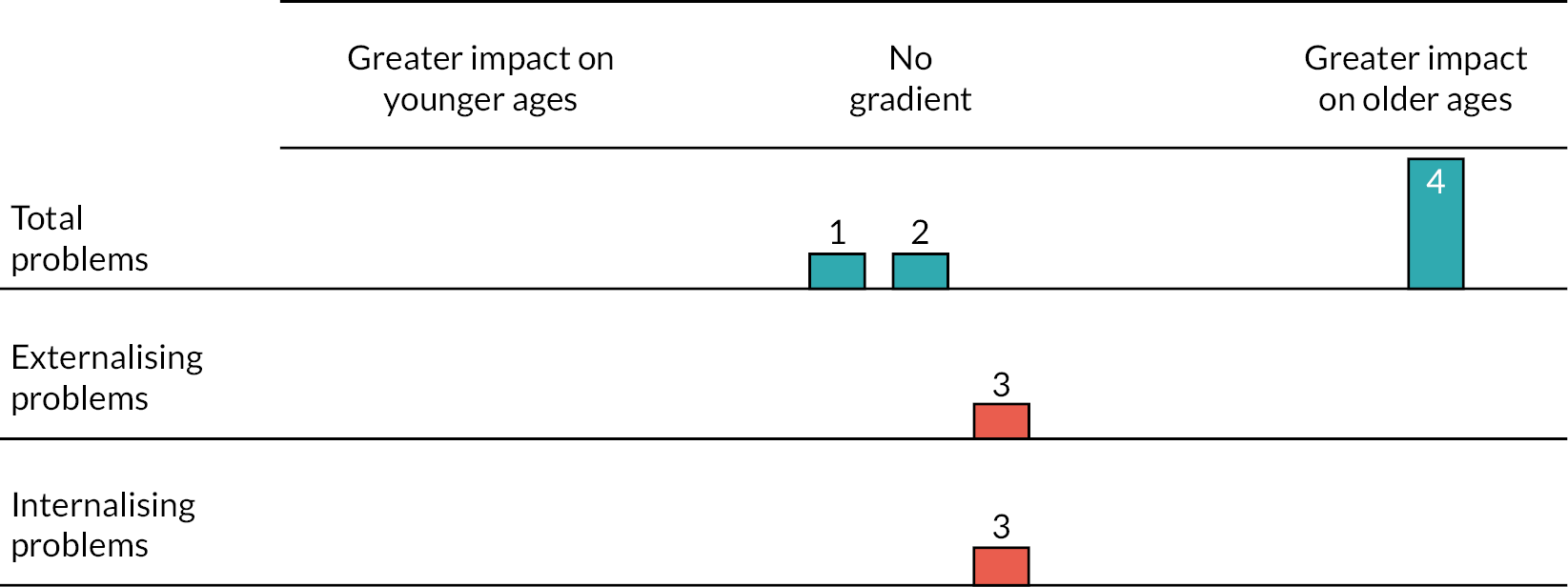
One study reporting an evaluation of ABC found an interaction effect. 171 The intervention was more effective for toddlers (18–36 months) compared with infants (0–17 months) in reducing total social, emotional and behavioural problems. Three studies reported no interaction effect for total social, emotional and behavioural problems, internalising and externalising problems. 171,182,183
Children and young people’s gender
Three study reports examined equity harms related to children and young people’s gender, which evaluations classified according to the binary of male and female (Figure 17). None of the studies reported differential effects for total social, emotional and behavioural problems, attention deficit hyperactivity disorder (ADHD), externalising problems, internalising problems, PTSD or dissociation. 103,147,176
FIGURE 17.
Equity harms for mental health behavioural and neurodevelopmental disorders by children and young people’s gender. Notes: DeGarmo et al. (2013)103 (¼ bar); Taussig et al. (2019)147 (¼ bar); Marquis (2013)176 (¼ bar). Height of bars represent the nature of the evidence presented by the trial: full height – significant moderation for a given outcome; three-quarter height – pattern of moderation estimates including some significant moderation; half height – non-significant moderation trending in one direction; one-quarter height – only non-significance reported. Shading of bars represent time to outcome at follow-up: blue – short-term outcomes of < 6 months post baseline; red – long-term outcomes of 6 months or more post baseline.
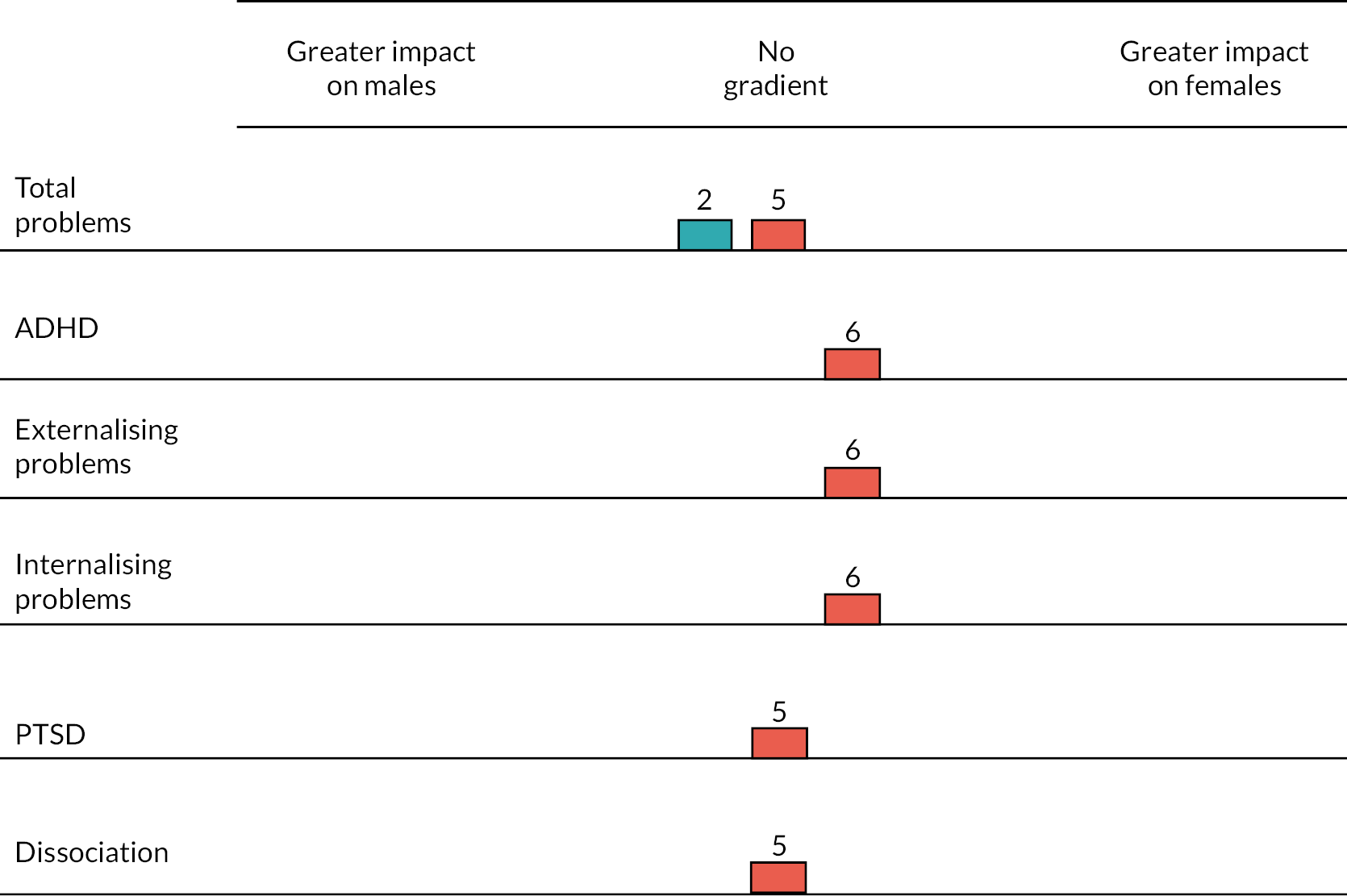
Children and young people’s ethnicity
Three studies explored the moderating effect of children and young people’s ethnicity on mental, behavioural and neurodevelopmental problems (Figure 18). Study reports tended to classify populations according to white and non-white participants. None of the studies found an interaction effect in relation to total social, emotional and behavioural problems, social-emotional functioning, PTSD or dissociation.
FIGURE 18.
Equity harms for mental health behavioural and neurodevelopmental disorders by children and young people’s ethnicity. Notes: Taussig et al. (2019)147 (¼ bar); Price et al. (2015)182 (¼ bar); Akin et al. (2019)167 (4/4 bar). Height of bars represent the nature of the evidence presented by the trial: full height – significant moderation for a given outcome; three-quarter height – pattern of moderation estimates including some significant moderation; half height – non-significant moderation trending in one direction; one-quarter height – only non-significance reported. Shading of bars represent time to outcome at follow-up: blue – short-term outcomes of < 6 months post baseline; red – long-term outcomes of 6 months or more post baseline.
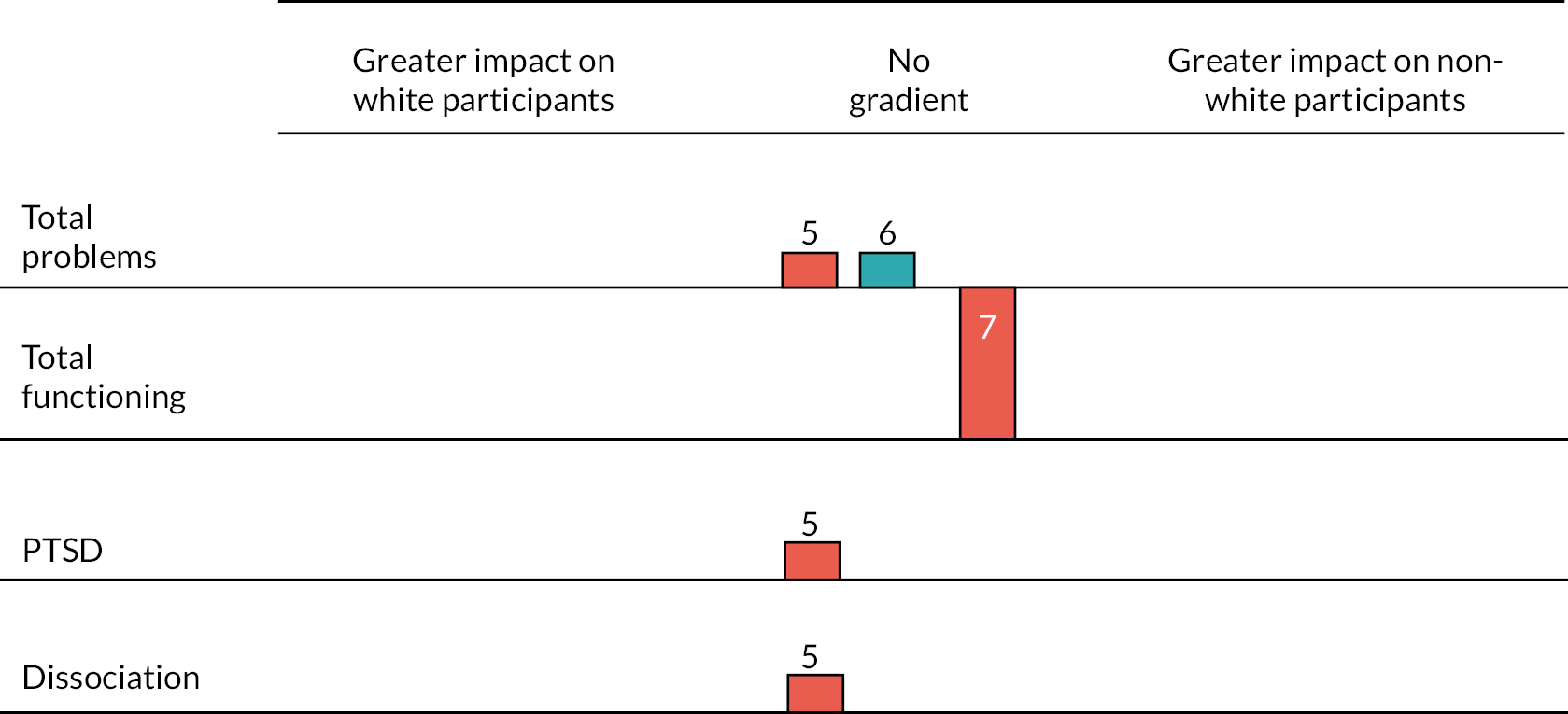
Children and young people’s history of maltreatment
Five study reports examined the moderating effect of history of maltreatment and adverse events on mental, behavioural and neurodevelopmental problems. One analysis of FHF reported that children with lower exposure to ACEs (composite of physical abuse; sexual abuse; removal from a single parent household; exposure to community violence; caregiver transitions; school transitions) had fewer symptoms of PTSD and dissociation. 116 A second analysis of the data set from the same intervention found that the intervention had a stronger treatment effect for PTSD for those who had a lower number of ACEs. 147 There was no differential effect for total social, emotional and behavioural problems or dissociation. 111,116,147
Evaluation of a version of MTFC that targets girls in foster care reported that precare exposure to sexual abuse and physical abuse did not predict any reduction in internalising or externalising problems. 183 Meanwhile, analysis of the reunification intervention, Pathways Home, indicated that prebaseline exposure to risk (e.g. mother or father has been arrested, has a history of drug abuse, mental illness, poverty) did not moderate total social, emotional and behavioural problems. 183
Children and young people’s baseline mental health problems
Six study reports, linked to five interventions considered the moderating effect of baseline mental health problems on mental, behavioural and neurodevelopmental disorders (Figure 19). Two evaluations of MTFC indicated that the intervention was more effective in impacting total social, emotional and behavioural problems among high-risk children, who were classified as those whose carers reported six or more problem behaviours each day. 117,122 To note, in one of these evaluations, there was variance in the differential impact on social and emotional functioning depending on the outcome measurement tool used. 122
FIGURE 19.
Equity harms for mental health behavioural and neurodevelopmental disorders by baseline mental health problems. Notes: Smith et al. (2011)183 (¼ bar); Taussig et al. (2019)147 (¼ bar); Akin et al. (2019)167 (4/4 bar); Biehal et al. (2012)135 (¼ bar); Chamberlain et al. (2008)117 (4/4 bar); Linares et al. (2006)175 (¼ bar). Height of bars represent the nature of the evidence presented by the trial: full height – significant moderation for a given outcome; three-quarter height – pattern of moderation estimates including some significant moderation; half height – non-significant moderation trending in one direction; one-quarter height – only non-significance reported.
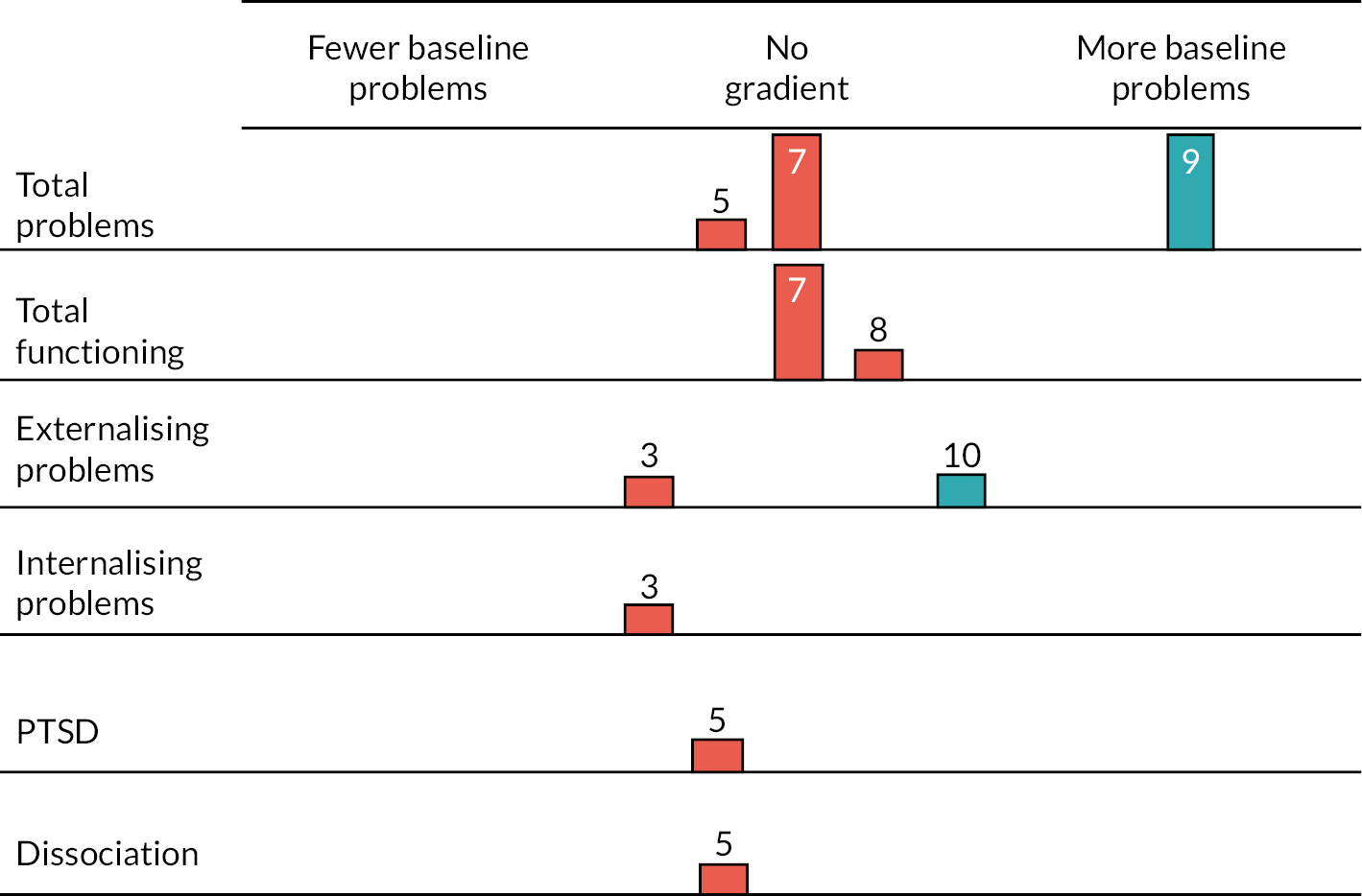
Four studies reported no interaction effect: total social, emotional and behavioural problems or functioning,147,167 externalising problems,174,183 internalising problems,183 symptoms of PTSD147 or dissociation. 147
Children and young people’s placement type and placement change
Five studies linked to four interventions reported on equity harms related to placement type and placement change. FHF indicated that the number of caregivers was associated with effectiveness for PTSD and dissociation, with individuals being more responsive when they had fewer caregiver transitions from birth to study baseline. 115 However, this relationship was not observed for total problem behaviours. A second intervention found that an individual with prior foster care placement removal was less likely to have a reduction in problem behaviours. 167 Meanwhile, studies reported no differential effects according to placement transition rate,103 number of parent and residential transitions,103 placement type (foster care vs. kinship care),147 children’s relationship to the caregiver (kin vs. non-kin)182 and quality of relationship with birth parents and foster carers. 115
Parent and carer characteristics
Four studies, associated with three interventions, reported on equity harms related to parent and carer characteristics. One evaluation of PMTO examined the interaction effect of carer age on children’s total social, emotional and behavioural problems and total social–emotional functioning. 167 There was no difference for outcomes if the carer was older or younger. One study report considered the interaction of carer ethnicity and children’s total social–emotional and behavioural problems, finding no effect. 182 This study also examined an interaction effect for the number of months a carer had been a foster carer and children’s total social, emotional and behavioural problems. There was no interaction effect.
One study reported on birth parent characteristics, as part of an evaluation of an intervention to prevent reunification breakdown failure for children returning home from foster care. 103 The intervention was more effective in addressing child total social, emotional and behavioural problems where birth mothers had a higher level of drug and alcohol cravings. A second study, reporting on PMTO, examined differential effects for different population groups, finding clearer effects for participants with high parental functioning compared to low parental functioning. 210 It found that for participants where biological parents had poor parental functioning combined with high levels of child problem behaviours, the intervention was more likely than the control group to remain in this group classification (i.e. poor parental functioning and child problem behaviours). In contrast, participants with high parental functioning and high child social–emotional issues were more likely than the control group to move to a higher parental functioning class after intervention participation.
Additional equity harms
Moderator analyses and interaction effects were considered in studies for additional equity harms related to children and young people’s mental, behavioural and neurodevelopmental disorders. An evaluation of the KEEP intervention examined the interaction effect of children’s language group and total social, emotional and behavioural problems. 182 There was no interaction effect. One study assessed the interaction of stages of girls’ pubertal development and internalising and externalising problem behaviours. 183 Pubertal development comprised body hair changes, skin changes, breast growth and mensuration. No interaction effect was found. A third study examined the moderating effect of child IQ on total emotional, social and behavioural problems, PTSD and dissociation. 147 IQ was not found to moderate intervention outcomes.
Suicide-related behaviours
No studies reported moderation analysis or interactions effects for outcomes related to suicide-related behaviours.
Conclusion
In this chapter, we have reported outcome evaluations of interventions targeting care-experienced children and young people’s subjective well-being, mental, behavioural and neurodevelopmental disorders, and suicide-related outcomes. Meta-analysis indicated some shorter-term effectiveness for mental health outcomes, but the certain of evidence was low. There was no evidence that interventions improved mental health outcomes in the longer term. There was limited evidence for subjective well-being and suicide-related outcomes. Interventions may have differential effects, working more effectively for those with more baseline mental health problems or lower exposure to maltreatment. The following chapter presents the process evaluation synthesis, reporting key context factors that may structure intervention implementation and acceptability.
Chapter 5 Process evaluation
About this chapter
In this chapter, we report on intervention process evaluations. The chapter addresses the following RQs:
-
3. How do contextual characteristics shape implementation factors and what are key enablers and inhibitors of implementation?
-
4. What is the acceptability of interventions to target populations?
As outlined in the methodology, we classified two types of process evaluation:
-
Conceptually and/or empirically thin evaluations that provided limited generalisable knowledge.
-
Conceptually and empirically rich process evaluations that provided rich insight in the contextual conditions of intervention implementation and acceptability, and generalisable knowledge that could support understanding of other interventions and other contexts.
In this chapter, we first present a summary of findings from thin process evaluations. We then report the synthesis of rich process evaluations, which generated key context domains that serve as enablers and inhibitors of implementation and stakeholders’ acceptability. The chapter continues with the integration of the process evaluation synthesis with the outcome evaluation synthesis, to explore how context, implementation and acceptability may explain variation in intervention effectiveness. We conclude with the GRADE CERQual assessment of confidence in the synthesised rich process evaluation findings.
Thin-process evaluations
A total of 27 study reports were included as relevant thin-process evaluations, which were linked to 20 interventions. 34,108,114,123–125,127,128,130,131,133,135,137,140,142–144,147,148,152,157–160,162,163,219 A summary of the study reports and findings are reported in the Report Supplementary Material 17; 14 interventions, with 17 study reports were conducted in the USA. 34,108,123–125,127,128,131,135,137,142,143,147,152,158–160 Three interventions, with three study reports, were conducted in the UK. 133,140,221 One intervention, with one study report, was evaluated respectively in Australia,162 Belgium,114 Canada,148 Ireland,130 Germany,157 the Netherlands163 and Portugal. 144
For thin-process evaluations, we summarised findings across three domains: contextual characteristics, implementation and acceptability.
Contextual characteristics
Only six interventions, with six associated study reports, referenced relevant contextual factors. 124,127,130,131,148,163 This lack of detail was one of the key reasons why they were classified as thin-process evaluations.
Geography was considered in one study report, with issues around the rurality of communities providing a barrier to accessing services. 131
The wider economic context was reported as a relevant factor in one study report, where a major economic recession in the USA led to budgetary constraints and a reduced willingness and capacity among social welfare agencies to implement MTFC. 124 The organisation and resourcing of social welfare systems was considered important in another evaluation of a solution-focused parenting groups intervention, where the structurally restricted and isolated role of the foster carer profession gave a sense of limited autonomy, which could compromise implementation. 148 An evaluation of PMTO addressed the importance of ‘usual care’ when the intervention was transported to the Netherlands from the USA, with the authors reflecting that standard practice is comparatively high in Northern Europe relative to the USA and could therefore potentially mask intervention effectiveness. 163
There were also reported sociocultural factors in relation to the transportation of interventions to new populations and countries. 127,130 Evaluation of Incredible Years in Ireland, an intervention transferred from the USA, ascribed challenges with implementation and acceptability to uniquely local issues, including interprofessional working and the historic non-engagement of biological families in social work. Local teams also reported concerns about the suitability of American-style language and activities for an Irish audience. 130
Implementation
A total of 19 interventions, with 25 associated study reports, reported data on implementation. 34,108,114,123–125,127,128,130,131,133,135,137,140,143,147,148,152,157–160,162,163,221 These data mapped to two categories: recruitment and retention, and fidelity to the intervention. 13 interventions, with 15 study reports, provided data on intervention recruitment and retention, primarily in relation to parents and carers. 108,114,123,127,128,130,131,135,140,143,147,158–160,221
A key issue in recruitment was capacity among targeted carers. Carers often had too much work, too many children, family illness or no interest in the intervention. 127 Foster carers found training in parenting skills as being inconsistent with their role as a professional caregiver, which contributed to drop out. 130 There was also reference to challenges of interprofessional working,130,140,158 including a reliance on CAMHS or social workers for referrals in the UK. 140,158
Retaining participants in interventions was another issue, with notable barriers to retention being children and young people moving care placements or areas,131,143 carer illness221 or inability to secure childcare arrangements. 221 Some interventions worked to retain children and young people by offering transportation, dinner, respite care or payment. 135,147 One intervention promoting mindfulness did not explicitly advertise the programme as an intervention, rather an opportunity to meet peers socially, which the intervention team thought would improve take-up and retention. 135 Retention rates among subgroups of intervention participants were not routinely reported, but the evaluation of the PCIT found that African American carers were more likely to drop out of the intervention. 123
A total of 17 interventions, with 22 linked study reports, considered intervention fidelity. 34,108,114,123–125,128,130,133,137,140,143,147,148,152,157–160,162,163,221 Generally, interventions reported a high level of fidelity,128,140,143,147,148,158,162,221 although one study report indicated issues with therapists not delivering all intervention components, which correlated with carers not completing follow-up assessments. 140
Two study reports, related to the KEEP and MTFC, explored implementation models to support the intervention. One assessed whether or not a ‘train the trainers’ model could achieve equal fidelity compared with a model where the intervention developers provided training, but reported no difference in fidelity. 125 A second study assessed differences in fidelity when delivering standard MTFC implementation training, compared with standard training plus support from two consultants, finding that the involvement of consultants was linked to higher levels of fidelity. 124
Barriers to fidelity were explored in several studies. In one intervention aimed at supporting children and young people’s relationships with birth parents, parents reported not having enough time during visits with their child to implement newly acquired parenting skills. 130 For carers, the solution-focused parenting groups approach reported continued issues with foster carers feeling too restricted in their role to change young people’s disruptive behaviours. 148 Meanwhile, a qualitative exploration of researchers’ and practitioners’ experiences of TFC suggested that carers struggled to balance their caregiver role with what they saw as their ‘professional’ role, and the need to develop a productive relationship with their social worker. 137 Carers also identified issues relating to finding childcare for other children and balancing the needs of the care-experienced child and biological children. 133,134 At the organisational level, perceived barriers included mental health needs being only one of numerous priorities being addressed by child welfare social workers, which could act as a barrier to timely and appropriate referrals. 158
There were perceived facilitators to implementation fidelity, which included flexibility in the frequency and timing of sessions to accommodate participants’ needs. 140,221 Suggestions to improve fidelity to parenting programmes were explored. For TFC, one suggestion was to develop carers’ understanding and knowledge of how to navigate the broader child welfare system and the adoption of a strengths-based approach to support them. 137 The evaluation suggested this could be improved through experiential training, peer support and ongoing skill building.
Acceptability
A total of 13 interventions, with 16 linked study reports, considered intervention acceptability. 108,127,128,130,131,133,135,140,142–144,148,157,158,162,221 Of these, 5 interventions with 5 study reports presented data on acceptability to children and young people,131,135,142,143,158 7 interventions, with 11 study reports, presented acceptability to parents and carers,108,128,130,131,132,140,144,148,157,158,162,221 and 5 interventions, with 6 study reports, considered acceptability to delivery agents and related stakeholders. 127,130,131,133,140,162 Evaluations tended to have limited descriptions of acceptability, with many confined to quantitative assessments of satisfaction.
Overall, levels of acceptability were high across stakeholders. 127,130,131,134,140,142,143,162,204 Qualitative data reported that children and young people valued the relationship-building element of interventions that included working with local people they were familiar with, working with others from similar backgrounds and working with clinicians for mental health support. 131,135
The value attached to relationships was echoed among parents and carers who welcomed the way interventions facilitated new relationships for young people. Carers also appreciated intervention components that provided opportunities for their own relationship development. This included opportunities for peer support, reflection and discussion. 128,130,131 They also valued developing and expanding their parenting skills. 148 Delivery agents recognised that interventions provided additional value to existing services in a way that helped reduce placement breakdowns. 130,140
For parents and carers, challenges to acceptability often related to their identity and relationships. In one intervention, kinship carers found it hard to fit into group sessions alongside other types of carers due to different relationships with biological families. 133 In another intervention, acceptability was impacted by some carers in the sessions feeling criticised for their parenting approaches. 140 When training sessions ended, carers reported struggling to implement newly acquired skills and knowledge as they juggled different parenting strategies for foster children and biological children. 133 Both children and young people, and parents and carers, felt that their intervention experiences could have been enhanced with longer intervention timescales to further develop skills and build relationships. Suggestions included follow-up support, refresher sessions or more permanent, ongoing provision. 131,148
For those delivering interventions, acceptability issues mapped to challenges in delivering interventions in the home setting and, in some instances, the difficulties associated with the emotional burden of managing interventions without adequate training and supervisory support. 131
Rich-process evaluations
In this section, we report the framework synthesis of rich process evaluations from 16 interventions, with 23 associated study reports27,118,120,122,126,129,132,136,138,139,141,145,146,149–151,153–156,161,164,215 (see Report Supplementary Material 18).
Study characteristics
Study reports were published between 2003 and 2021; 9 interventions, with 14 associated study reports, were evaluated in the context of the UK and Ireland. 27,118,120,122,126,136,138,139,149–151,154,155,215 Six interventions, with eight study reports, were from the USA. 129,132,141,145,146,156,164,223 One study report, with one intervention, was from Australia. 153
Quality assessment
We quality appraised rich study reports with an adapted qualitative appraisal tool84 (see Report Supplementary Material 19). We made 21 assessments, as 3 study reports were related to the same evaluation of a single intervention. Overall scores were assessed for reliability and usefulness.
For overall reliability, 2 study reports were assessed as having high reliability, 14 as medium, 4 as low and 1 as unclear. For overall usefulness, 5 study reports were assessed as having high usefulness, 14 as medium and 2 as low. Only one of the studies was rated highly in both categories150 and two were rated low. 141,215
There were a number of methodological limitations across the evaluations. In terms of reliability, assessment of sampling indicated widespread challenges in engaging care-experienced children and young people, in addition to their parents and carers. Studies tended to rely on a pragmatic, convenience approach to sampling and, on occasion, reported approaching populations based on ease of access. 120 There were efforts to sample diverse care-experienced populations, but this was sometimes compromised by participant drop out.
The grounding of findings in the data was variable. Higher-rated study reports demonstrated a clear link between qualitative data, interpretation and conclusions. They presented a range of quotes from participants, and the provenance of each quotation was clearly labelled. In lower-rated study reports, there was limited linking of data and the findings. It was often unclear how representative quotations were, usually as a result of non-specific labelling.
In reference to usefulness, there was a general issue with the under-representation of children and young people’s voices. A number of evaluations made a concerted effort to engage with this group,27,120,132,145 but they were clearly missing from other study reports. In some instances, this was due to the evaluation focusing on maximising implementation and intervention functioning, and hence a focus on delivery agents as study participants. 129,141,153 In this case, we assessed usefulness as not applicable. In other study reports, evaluations explored the experiences of intervention participants, which tended to involve a focus on carers. While children and young people were not the direct target population of these interventions, interventions did assess outcomes related to children and young people’s mental health and well-being, and so it may have been appropriate to include their voice. Accordingly, these studies were rated low for usefulness in relation to children and young people’s voices. Furthermore, while some interventions were focused on younger-aged children (e.g. children aged under 5 years) who may have been more difficult to engage, these studies were also assessed as low where there was limited or no consideration of potential opportunities to secure their participation.
Context factors as enablers and inhibitors of implementation and acceptability
The synthesis of qualitative data from the rich-process evaluations generated three overarching themes, or context factors, with five associated domains. These themes explore how key dimensions of context shape intervention implementation and acceptability.
System resources
System resources refer to the financial, technical and capacity resources to deliver interventions, while also considering the burden of intervention implementation and participation within systems that are already overstretched.
Limited resource and competing demands
Seven interventions, with nine study reports, indicated a lack of capacity for intervention delivery, which reflected wider structural issues around inadequate resources in the social care system and the challenge of managing a high volume of competing demands. 27,118,122,138,146,151,154,155,215
Evaluations centralised the issue of social care professionals’ existing and often overwhelming workloads. Across intervention types, social workers were reported to have full and complex caseloads, which were often being managed in negative and unsupportive working cultures: ‘overwhelming amounts of paperwork, low pay, negative agency climates due to a culture of fear, and unstable leadership’. 146
Similar issues were reported for other delivery agents, such as peer mentors in interpersonal interventions, who described the challenge of managing their commitment to the intervention with busy home lives, which included their own childcare responsibilities. 27
High workloads and competing demands had potentially adverse consequences for implementation. A lack of system resource meant that there was limited capacity to relieve professionals of their workload to ensure that they received the training required to support implementation. 138 One intervention, delivered in a residential care setting, stated that social care staff were often distracted by their other responsibilities, which impacted on their capacity to engage with intervention sessions. 151 Such issues were compounded by system barriers to addressing capacity shortfalls, with studies reporting challenges with filling staff vacancies to support delivery. 118,122
In a UK peer mentoring intervention to prevent teenage pregnancy for girls in foster care, there was a reported lack of communication between local authority staff overseeing the intervention and mentors. Communication issues were perceived as being a consequence of high caseloads among local authority staff, extensive organisational inspections, organisational restructuring and staff cutbacks. 27 This led to tensions and frustration among mentors, who felt frustrated with the time gap between their training and being matched with a mentee, and the effect this had on their ability to put into practice what they had learnt. 27
A lack of resources among delivery agents was felt to be a particular barrier where interventions were targeting outcomes that were not considered to be a ‘system priority’. For example, in the peer-support intervention aimed at preventing pregnancy,27 a perceived lack of local authority commitment was partly attributed to the non-prioritisation of preventative work. Equally, in the SOLID study, which had a primary emphasis on alcohol and substance use, implementation was frequently deprioritised in favour of ‘core business’ by drug and alcohol treatment providers from voluntary sector organisations. 118
Intervention burden
Eight interventions, with nine study reports, considered how the delivery of interventions in an overstretched system created the experience of burden for delivery agents and participants. 138,139,141,145,146,150,151,156,161
There were three key domains of burden that we conceptualised as part of the synthesis: time, cognitive and emotional. In terms of the burden of time, carers participating in parenting programmes noted the significant demands of the intervention as being unrealistic given their other commitments. Evaluation of the interpersonal PMT intervention reported concerns among carers about the frequency and timing of training sessions and the burden of regularly completing parenting tasks as part of the homework activities:
Because for example, I used to work 10–12 hours and if I worked 10–12 hours, I don’t feel like doing anybody’s homework or helping them with homework. Actually, doing behavior charts … I’m a working parent. Working parents don’t always have a lot of time. 146
In some instances, this sense of carer burden was intensified by the lack of background information about foster children provided to carers, as this was seen to place a weight on carers and their families in terms of adjusting to the new young person and their specific needs. 161 There was also an important consideration in regard to the various opportunity costs involved with the intervention. In the Head, Heart Hands intervention, carers stated that in the context of limited time, they were ‘uncomfortable’ with the amount of space taken up with social introductions at the expense of exploring approaches to meeting children’s needs. 139
Cognitive burden, often intersecting with the issue of limited time, was linked to the complexity of interventions and the challenge of translating newly acquired skill and knowledge into real world practice. In one intervention where social workers supported young people to participate in yoga, professionals commented that study documentation was too onerous and tedious, while others commented on their lack of confidence to complete the required paperwork. 151 Moreover, parenting interventions reported that a lack of detailed description on parenting strategies could inadvertently exacerbate tensions, such as the removal of a child’s privileges resulting in the whole family being punished. 146
Similar issues were found with TFTC intervention, which had a significant parent training component. 141 While foster carers were committed to the approach, in practice they lacked implementation skills in their daily lives and therefore capacity to change was restricted, with a carer suggesting that ‘it is one thing to understand an intervention; it is another to possess the skill to implement the intervention in vivo’. 141 Importantly, evaluation of Finding Family reported that comprehensive training and support was important in ensuring effective implementation. 156
Emotional burden and the lack of support for the emotional impact of interventions were considered across a number of study reports. For social care professionals, studies recognised that the stress of working in the care sector and the addition of interventions to their existing workload could exacerbate existing feelings of being overwhelmed. 151
Such issues were experienced by other intervention delivery agents; for example, in the Fostering Connections study, which was the primary study to report emotional burden. 138 In this trauma-informed intervention, facilitators who delivered training to carers reported on the unexpected emotional strain:
When you are talking about attachment and you are telling the carers about healthy attachment and then we start talking about un-healthy attachment and these are the children they are caring for and I think it is very sad and you can’t but feel that.
Facilitator 3138 (p. 4)
Delivering parenting interventions for foster carers also came with challenges in terms of managing personal disclosures within group settings. Facilitators were often not prepared for this and had to develop strategies for ensuring an element of group safety was integrated into the intervention. As a consequence, the process evaluation stated the need for adequate supervision and support for delivery agents to help them manage the emotional load. 138
Minimising or finding strategies to effectively address burden for delivery agents may be important to improving fidelity. Evaluation of Finding Family indicated that implementation was improved when delivery agents, in this case permanency specialists, had persistence and resilience to manage systematic barriers, such as youth not being able to connect with certain adults due to caseworkers making decisions about visitations with family. 156
Emotional burden was also explored in relation to carers. For example, in the GIFT intervention, carers reported the anxiety of being video-recorded as part of the process. 150 One process evaluation reflected on key pressure points where foster carers would experience significant emotional strain. It noted how issues of social care staff transience could create feelings of abandonment among carers, while they were also forced to adjust to new workers. 161
Within these interventions, however, there was also evidence of carers feeling supported. In the process evaluation of the GIFT intervention, carers commented favourably on the way in which the intervention took account of their own mental health needs, in addition to those of the child. 150 Elsewhere, interventions provided carers with the first opportunity to reflect on their caring. This gave them an opportunity to make sense of their experiences, and provided confidence for understanding children and their behaviours. 138 Acknowledging the emotional burden of the role, carers placed an emphasis on the need for ‘self-care’ in delivering the learning from interventions, and this was reinforced by facilitators. 138
Children and young people occasionally picked up on this sense of burden experienced by adult groups who were delivering interventions, which could make them disinclined to engage with the intervention. In a US-based YIM intervention, young people expressed concerns about further overburdening their mentors and mentioned not wanting to contact them due to concern about ‘stacking’ up problems for them. 145
System culture and interprofessional working
A total of 7 interventions, with 12 study reports, explored how system culture, particularly the culture of interprofessional working across health and social care, was imperative to the effective implementation of interventions. 118,126,136,138,141,149,150,154–156,161,215
In one approach to TFC, partnership working was considered central to its perceived effectiveness, with carers citing the importance of support from across the system. 161 Intervention stakeholders also explored the usefulness of expanding knowledge and expertise across professional boundaries. In the GIFT intervention, social workers indicated the importance of introducing a mental health focus, with it adding ‘a string to the bow’ when conducting their assessments. 149,150 More specifically, they felt that a mental-health lens allowed them to conduct a more detailed, intricate assessment of children and young people’s needs, enabling them to identify issues that might have otherwise been overlooked. This was also reflected in a trauma-informed foster care intervention, with the adoption of a trauma-informed approach providing foster carers with a deeper understanding about children’s behaviour in a trauma context. 138
Despite apparent benefits of interprofessional working, there were historic structural issues with collaboration across social care and health systems and several evaluations documented tumultuous relationships. A UK-based evaluation that explored efforts to develop new mental health services within CAMHS for children in care observed previous difficulties between social services, residential social workers and mental health professionals. Difficulties were attributed to limited understanding about how other partner organisations worked, poor cross-sector communication, feelings of alienation due to organisation-specific jargon, competing targets and pressures, and ill-defined and overlapping boundaries. 126 As a result, the evaluated reported the need for more groundwork to strengthen relationships, for future cross-sector interventions to be successful. Meanwhile, in an evaluation of Family Finding, an intervention focused on promoting relationships between foster children and biological family members, there were perceived structural issues with the wider social care system not being trained in the ethos and importance of the intervention. There was a need to extend training more widely to ensure investment and belief in the approach. 156
Interventions reported implementation strategies for improving inter-professional working and/or ensuring the system culture was supportive of the intervention. TFTC facilitated extensive organisational change to improve system infrastructures to support staff and foster families. 141 The intervention to develop new mental health services within CAMHS adopted two strategies to improve the structure of the care system and interorganisational relationships. First, increasing understanding of other organisations’ working practices amid recognition that jargon can be alienating and prevent partnership building. Second, improving support for foster carers and their children to prevent them from feeling isolated and unsupported in the midst of organisational tensions. 126 Furthermore, MTFC was built upon a comprehensive approach to multiagency working, aiming to bring together a range of partners to collaborate by providing a common language so as to diffuse potential conflict and clarify goals for young people. 136
In some instances, efforts to enhance interprofessional partnerships actually created further tensions in the system. In the GIFT intervention, there were concerns that newly facilitated partnerships undermined stakeholders’ decision-making. 150 The absence of a historical perspective by other partners meant social workers feared a clash with their own judgements when they came into the legal system. This resonated with feedback from social workers in the MTFC intervention, who reported feeling ‘out of the loop’ in terms of decision-making. They were concerned about not being told about specific incidents and also missing out on ongoing issues, which had implications for who was accountable for keeping children safe. 136
System identities
System identities refers to the sociocultural positioning of both children and young people, and their carers, within the care system. It further considers the values and needs of these different groups based on their structured identities.
Care-experienced children and young people’s identities, values and needs
Eight interventions, with ten study reports, centralised the issue of the positioning of care-experienced children and young people within the care system, often being marginalised, disenfranchised and devalued. 27,118,120,126,132,145,146,154,155,164
In the peer-mentoring programme to prevent pregnancy in teenage girls in foster care, the process evaluation recognised that this population often feel disempowered. 27 Evaluation explained that this feeling left young people without a voice to express their needs, so they might decline to take part in an intervention. In the intervention, this disengagement resulted in some foster children irregularly attending meetings, frequently altering the time or venue of the meeting with short notice, not turning up due to school work, seeing friends instead or lacking motivation.
The structural devaluation of children and young people in care occasionally permeated the accounts of carers. In the US-based PMT intervention,146 foster carers mentioned that the rights-based approaches adopted by statutory authorities meant children were fully aware of their rights and foster carers felt that this undermined their attempts to change behaviour:
They say, you can’t hit me, you can’t whoop me. You ain’t my mama. You don’t tell me what to do. So, if they putting this already in the child’s head … then of course they’re going to do what they want to do and say what they want to say.
Spielfogel et al. (2011, p. 3673)146
Furthermore, there were occasions of young people blaming themselves when the intervention was not delivered as expected. Again, in the peer-led mentoring programme to prevent pregnancy in teenage girls, the premature ending of mentoring relationships and infrequent meetings led to mentees feeling they had done something wrong and scrutinising how they had interacted with the mentor: ‘Cos I’ve had two [mentors] and they haven’t really worked out so well. But then, it kind of questions me, like maybe it’s something I’m doing wrong’ (LA1 mentee 1001; Mezey et al., 2015, p. 92. 27
Intersecting with issues around the identity of being in care, study reports also described the additional perceived stigma of interventions targeting mental health and well-being. Where care-experienced young people were already seen as different from others, there was a reported concern about being further marginalised if they were seen to have mental health problems. Evaluation of new mental health services in CAMHS referenced a ‘language of abnormality’, which served as a barrier to young people engaging with the intervention:126
The child, who’s only nine, has actually said ‘I’m not going in there because that’s a place for nutters’. I mean I was quite shocked that a child of, you know, a relatively quite young age, has got this association.
Childcare operations worker126 (p. 54)
In this context, children and young people often emphasised the need for choice and control. As reported in the SOLID study, this included them engaging with interventions at a point they felt ready to change and not rigidly relying on talking therapies if this did not meet the need of the young person. 118
Children and young people also expressed a desire to build meaningful relationships where they were not marginalised or treated differently. Where mentoring worked well, young people described strong connections with their mentors, likening them to role models, parents and friends. 145 In the SOLID study, there was an emphasis on taking advantage of professionals already involved with young people to reduce the number of adults rotating in their lives, although there was less enthusiasm for this among the professionals themselves. 118
Notably, in the peer-support programme to prevent pregnancy, children and young people stated that they valued building relationships with mentors who had a shared experience of care and appreciated opportunities to establish a connection with someone they could relate to. 27 In a second mentoring intervention, participants indicated that a commonality in background, which included similar cultural experiences and social interests, could encourage engagement. 145 Further qualities of the relationship considered important were a non-judgemental attitude, sharing personal experiences, providing companionship, offering information and instrumental support, and persistence in the relationship. 27,145,164
There were a number of reported benefits from building strong and meaningful relationships. Within peer mentoring programmes, young people indicated that their relationship with their mentor had led to wider improvements in relationships with family members and friends. 145 They also allowed young people to become more open and confident about their sexuality, improved their self-esteem, and empowered them to make better life choices. 27 In a computer game-based intervention, young people suggested that one of the main appeals of the intervention was that it allowed them to spend more time with social workers. 120
There were reported limitations to the mentoring relationships, however, and some individuals declined to participate. In the peer mentoring intervention to prevent teenage pregnancy, some young people wanted to maintain their independence; they did not feel that they could identify an appropriate mentor, or the nominated mentor was not contactable or declined to offer support. 27 Meanwhile, in the computer game intervention supported by social workers, some young people found that their involvement could be a distraction. 120
Carer identity, values and needs
A total of 10 interventions, with 12 study reports, explored the position of carers (e.g. foster, kinship and residential) within the social care system. 118,120,129,132,136,138,139,146,151,153–155
As with children and young people, many carers felt structurally disadvantaged as a consequence of wider sociocultural conditions, believing that their expertise and experiences were often discounted. Across studies, there were reports of discord between intervention aims and the needs and values of carers, with carers often left feeling devalued. One evaluation of a foster carer training programme reported that the intervention lacked relevance because it replicated the principles that already underpinned carers’ existing practices. 139 A second evaluation of MTFC in the UK explored how carers felt challenged to balance the principles of the intervention with their own value judgements and more individualised practices. 136
Relatedly, in an evaluation of TFC,139 carers expressed concern about the wider system’s propensity to respond to and support changes in the way that carers work. They noted that without structural change that led to a realignment in system values, carers’ voices would continue to be discounted:
It’s like trying to fit social pedagogy into a system it doesn’t fit with; when [foster carers are] skilled up we should be able to make decisions but I don’t think the system or social workers are necessarily up for that.
McDermid et al. (2021, p. 8)139
Intersecting with complexities related to the identity of being a carer were important sociocultural dimensions of race and ethnicity. One PMT intervention in the USA experienced issues with engaging African American foster parents due to some incongruence in parenting values and strategies, and differences in language and phrasings. 146 Past carer experiences around the use of mental health services and therapy could also shape carers intervention engagement. 129
Evaluations also highlighted issues around identity conflict, where carers were required to adopt multiple roles. Studies reported challenges in negotiating the role as parent and disciplinarian, and how this could be further complicated with living with other adults also imposing sanctions and discipline. Alongside these considerations were doubts about whether carers should be taking on the role of intervention ‘delivery agent’. Residential carers in the SOLID study, which addressed alcohol and substance use, felt that their role the intervention could damage relationships with young people, who feared sanctions if they disclosed their behaviours. 118
Responsiveness to the identity, values and needs of carers raised important questions about the adaptability of interventions to accommodate different contexts and needs. 153 For example, carers engaged in a UK implementation of MTFC maintained that the US-developed intervention was overly prescriptive and rigid and had not been sufficiently adapted to meet their needs in the UK. They felt that judgement of whether child behaviours could be identified as ‘stressful’ was subjective and varied according to carers’ tolerance and time of day. There was also debate about finding the right rewards and tasks for children in a range of family setups. More fundamentally, carers felt that certain elements of the intervention were unacceptable and questioned the inclusion of certain tools and language in the UK context. This included reference to ‘mean talk’, classifying self-harm as ‘destructiveness’ and the absence of eating disorders other than ‘skipping meals’. 136 Carers were also particularly concerned about interventions that had the potential to increase the pain experienced by children and young people as a result of addressing past traumas. In the IPS intervention, carers were also concerned about children and young people reconnecting with relatives who contributed to past traumas. 132
Some interventions anticipated the need for adaptability, with developers ‘striking a balance’ between tailoring to parents’ needs alongside managing intervention fidelity to support carer engagement. 146 This was illustrated in the Fostering Connections intervention, where adaptations to local needs was seen as crucial in terms of reach and engagement. However, the researchers discussed achieving a balance between this adaptability and a recognition that ongoing fidelity research was essential to ensure accuracy and consistency in any future iteration of the intervention. 138 Equally, there was consideration of the need to co-produce interventions in response to the sociocultural context of implementation: ‘Implementation strategies should be co-produced with stakeholders to ensure that these are sensitive to cultural differences and relevant to a specific point in time’ Vallejos et al. (2016, p. 273). 151
Grading of Recommendations Assessment, Development and Evaluation confidence in the evidence from reviews of qualitative research assessment of rich-process evaluations
Based on the three overarching themes and five domains, we constructed six evidence statements that describe key context factors that may structure implementation and acceptability.
Three of these statements were rated as having high certainty of evidence:
-
High social care workloads can limit professionals’ capacity for intervention delivery.
-
Care-experienced children and young people can feel disempowered within the social system, meaning that their needs are not always acknowledged.
-
Children and young people value building positive relationships, particularly where those relationships are with individuals who understand or have experienced care.
Three statements were rated as having moderate certainty of evidence:
-
Implementation involves a time, cognitive and emotional burden, of which young people may be aware, and so may discourage their engagement.
-
A supportive system culture that promotes interprofessional relationships is needed for intervention implementation.
-
Carers feel that interventions do not value their knowledge and expertise and want adaptive approaches that are responsive to their specific needs.
The full evidence assessments are presented in the Report Supplementary Material 20.
Integration of outcome and process synthesis
The outcome synthesis in the previous chapter identified a mixed evidence base for interventions across the three primary outcome domains. The meta-analyses for interventions targeting mental health, behavioural and neurodevelopmental disorders indicated that interventions improved several outcomes in the shorter-term (up to 6 months post baseline), but there was no evidence that these effects persisted when outcomes were measured in the longer-term (> 6 months after baseline). Owing to the low number of studies measuring relevant outcomes, we did not conduct a meta-analysis for domains related to subjective well-being or suicide-related outcomes.
As part of the convergent synthesis design,73,74 we constructed a matrix of data from outcome evaluations mapped against data from the thin and rich process evaluations. This involved adding detail on the overarching outcome findings, where available, to the tables summarising the process evaluation findings (see Report Supplementary Material 21). From here, we mapped which interventions demonstrated effectiveness, non-effectiveness or harms, and how the related process evaluation data might explain these outcomes. 92 Comparing outcome and process data across individual interventions allowed us to establish potential trends in the link between intervention outcomes, context, implementation and acceptability. Outcome evidence was classified as direct, meaning that outcome and process data were generated from the same evaluation, or as indirect, meaning that outcome and process data were from different evaluations of the same intervention.
For the thin-process evaluations, four interventions with outcome data from the same overarching evaluation (i.e. direct), had some evidence of effectiveness. 26,34,147,159,166,167 The interventions, two of which had an emphasis on mentoring and one of which focused on creating a trauma-informed system, generally reported high fidelity and acceptability. Six interventions reported mixed evidence of effectiveness from direct or indirect evidence. 29,127,140,143,162,163,175,177,212 Again, underpinning process evaluations largely indicated that these interventions achieved high levels of fidelity and acceptability, although there were some issues with usual care overlapping with elements of the intervention. 140 The majority of interventions (n = 11) showed no evidence of effectiveness from direct or indirect outcome evaluations. 31,113,122,124,128,131,134,135,142,157,158,173,174,179 These interventions also indicated broadly high fidelity and acceptability across stakeholders, particularly with regard to the quality of training for parenting programmes. However, there were some issues around recruitment and retention for these parenting interventions, and there were key challenges with carers implementing parenting skills and integrating interventions into their existing practices. 130,137
For the rich-process evaluation synthesis, six interventions had associated outcome evaluations. For three interventions there was direct evidence27,122,129,156 and for four interventions there was indirect evidence. 31,163,166,167,172,173,175,186 Outcome evaluations of one intervention, PMT, reported either some evidence of effectiveness166,167 or no effect,175 but associated process evaluations still indicated issues around intervention resources, burden and stakeholder identity. Two interventions showed mixed evidence of effectiveness from indirect outcome evaluations,27,31,124,129 with process data showing particular issues related to burden on delivery agents and challenges in interprofessional working. Three of the interventions did not report effectiveness,122,129 although the evaluation of the mentoring programme to prevent teenage pregnancy was intended as a pilot study. 27,122 Two of these interventions had a focus on parenting components and had issues with carer identity. 122,129 MTFC and the mentoring intervention, while primarily focused on interpersonal relationships, had significant limitations with system resources, burden and interprofessional working. 27,122
Beyond the individual report-level integration of process evaluation and outcome data, we considered of how the process evaluation synthesis may explain the findings from the outcome synthesis and meta-analysis. Of particular interest was the fact that interventions measuring outcomes related to mental, behavioural and neurodevelopmental disorders showed some effectiveness in the shorter but not the long term. From the thin-process evaluations, which had associated outcome evaluations that were typically included in the meta-analysis, there was no clear explanation of the link between implementation, acceptability and outcomes. Generally, apart from some issues with recruitment and retention, most interventions reported high levels of fidelity and acceptability regardless of effectiveness.
While the rich-process data did not necessarily have linked outcome evaluations included in the meta-analysis, findings potentially offer insight into structural challenges that might impact interventions targeted at care-experienced children in the longer term. For example, the large number of parenting interventions included in the meta-analysis were generally shown to be implementable and acceptable within the context of shorter-term delivery, with much of the process evaluation data focused on the (often relatively intense) initial intervention training period. However, integrating and sustaining the intervention within the wider culture of parenting practices, discordance with existing expertise, lack of wider systemic support and conflicting commitments, could be challenging to longer-term delivery. These issues were hinted at within the thin process evaluations. 130,137
Summary
In this chapter, we have provided a description and synthesis of process evaluation findings of eligible study reports. Thin-process evaluations provided mixed evidence related to intervention implementation and stakeholder acceptability, but overall both were high. Rich-process evaluations reported key system-level contextual factors, which may help to explain the challenges of implementation and issues with acceptability, with these relating to system resources, interprofessional culture and system personal identities. In the next chapter, we present the review-level synthesis, stakeholder consultations and review recommendations.
Chapter 6 Integration and discussion
About this chapter
In this chapter, we bring together the findings from the three previous chapters, reporting the mapping of interventions and study reports, outcome synthesis and process evaluation synthesis. The chapter addresses the following review questions:
-
5. Can and how might intervention types, theories, components and outcomes be related in an overarching system-based programme theory?
-
6. What do stakeholders think is the most feasible and acceptable intervention in the UK that could progress to further outcome or implementation evaluation?
In this chapter, we first provide an overview of method-level syntheses and initial review-level synthesis, with explanation of how the process evaluation synthesis supports interpretation of the outcome evaluation synthesis. We then present findings from stakeholder consultations, including consideration of the potential for candidate interventions identified by the review to be implemented in the UK context or if de novo intervention development is required. We conclude the chapter with recommendations for future research in relation to intervention development, adaptation and evaluation, and for policy-makers and practitioners.
Overview of review aims and research questions
The CHIMES review was a complex-systems-informed, multimethod systematic review that aimed to synthesise international evidence on interventions addressing the mental health and well-being of care-experienced children and young people.
This research aim was addressed through the following RQs:
-
What are the types, theories and outcomes tested in mental health and well-being interventions for care-experienced children and young people?
-
What are the effects (including inequities and harms) and economic effects of interventions?
-
How do contextual characteristics shape implementation factors and what are key enablers and inhibitors of implementation?
-
What is the acceptability of interventions to target populations?
-
Can and how might intervention types, theories, components and outcomes be related in an overarching system-based programme theory?
-
What do stakeholders think is the most feasible and acceptable intervention in the UK that could progress to further outcome or implementation evaluation?
Overview of review findings (research questions 1, 2, 3 and 4)
Overview of intervention types and evidence types
We identified 64 separate interventions, with 124 associated study reports. Of these reports, 24 described the intervention’s programme theories, 50 were process evaluations, 85 were outcome evaluations and 1 was a partial economic evaluation. The majority of the 124 studies described interventions that were delivered and evaluated in the USA (n = 77). Of the 64 interventions, there was a clear focus on approaches that target the skills and knowledge of young people (n = 9 interventions), emphasise improvement of carer parenting practices and young people’s relationships (n = 26 interventions), or a combination of the two (n = 15 interventions). Of these interventions, 13 included an explicit programme theory, with 12 prioritising theories that operate within the interpersonal domain (e.g. relational) of the socioecological model. Interventions primarily targeted mental health, behavioural and neurodevelopmental disorders, with 48 interventions assessing children and young people’s total social, emotional and behavioural problems and 26 targeting children and young people’s externalising problem behaviours. Only 11 interventions targeted subjective well-being, with 4 targeting suicide-related outcomes.
Overview of outcome synthesis
We synthesised evidence from 44 RCTs of 35 interventions that evaluated the effectiveness of interventions for improving children and young people’s subjective well-being, mental, behavioural and neurodevelopmental disorders and suicide-related issues. Synthesised evaluations predominantly related to interventions that operated across the intrapersonal and/or interpersonal domain, and were largely conducted in the USA or UK.
Meta-analyses of RCT evaluations showed that interventions collectively improved short-term outcomes (those measured at 0–6 months post baseline) across several mental, behavioural and neurodevelopmental disorder domains. Using GRADE evidence assessments, we judged there to be low or very low certainty for short-term effectiveness in these outcome domains, as a result of concerns relating to RoB and/or imprecision. For longer-term outcomes (> 6 months post baseline), meta-analyses showed no significant effectiveness across any of the assessed mental, behavioural and neurodevelopmental outcome domains. Combined with concerns regarding RoB and imprecision, our GRADE evidence assessment indicated very low certainty that interventions are effective in the longer-term for these child-level outcomes.
Quasi-experimental design evaluations of community-level (n = 2) and organisational-level (n = 1) interventions showed mixed results, with some limited evidence of longer-term improvements in child-level functioning and emotional/behavioural regulation where care agencies receive specialist trauma-informed training.
There were few evaluations that looked at the effectiveness of interventions on children and young people’s subjective well-being outcomes or outcomes relating to suicide and self-harm.
Fourteen evaluations provided moderator analyses or interaction effects that allowed us to assess whether interventions might deliver adverse or inequitable effects. Evidence was mixed, with the majority of evaluations showing no moderating effects. There was some limited evidence that interventions may work more effectively for those with more baseline mental health problems or lower exposure to maltreatment.
Explaining outcomes findings: context factors and process evaluation synthesis
We classified process evaluations as either conceptually and/or empirically thin (n = 27) or conceptually and/or empirically rich (n = 23). Thin evaluations, which were linked to outcome evaluations, tended to have limited data availability that was generalisable beyond the immediate evaluation context. Rich evaluations presented generalisable findings that had explanatory power beyond the proximate evaluation context. Thin-process evaluations generally demonstrated that interventions reported high levels of fidelity, in terms of the quantity and quality of intervention delivery. Equally, acceptability was reported as largely positive across a range of stakeholder groups, although the perspectives of children and young people were largely under-represented. However, there were potential implementation challenges reported in terms of recruitment and retention to interventions and the evaluation study. This was a particular issue for parent and carers who struggled to manage the intervention with a range of other commitments.
The synthesis of rich-process evaluations progressed understanding of wider context factors that might help to explain potential issues around implementation and acceptability. We identified five key context factors: (1) lack of system resources for intervention training and implementation, partly because health promotion is not ‘core business’; (2) intervention burden, which encompasses the time, cognitive and emotional burden associated with implementation and participation. Importantly, young people engaged in mentoring interventions cited concerns about burdening their mentor and hence feeling disinclined to seek support;145 (3) interprofessional relationships, where historical and ongoing tensions between health and social care professionals can inhibit interventions that are reliant on effective multiagency communication and collaboration; (4) care-experienced young people’s identity, where their systematic disenfranchisement can mean they feel unable to express dissatisfaction with an intervention, which might encourage disengagement and (5) carer identity, where interventions may not engage carers as they feel their expertise and history of parenting practices are not valued, creating misalignment between interventions and the wider contexts of their lives.
Through integration of the outcome and process evaluation data, we sought to explain the outcome synthesis. At the level of the individual intervention, there was no clear trend between implementation, acceptability and effectiveness. From the thin-process evaluations, interventions were largely implemented with high levels of fidelity and acceptability whether they were effective or not. However, these thin-process evaluations tended to focus on the immediate period of intervention training. For example, they assessed carers attendance and learning at parenting training courses, rather than carers’ longer-term delivery of their newly acquired skills sets within the real-world contexts of their lives. In contrast, the rich-process evaluations offer insight into the structural challenges to intervention, which may compromise longer-term implementation. This can include the potential incongruence of learning from parenting training with carers’ own values, practices and commitments within their wider family and community,136 which can impede delivery and reduce acceptability. These context factors may help explain the key findings from the outcome meta-analysis, namely that interventions targeting domains of mental, behavioural and neurodevelopmental disorders are effective in the shorter term (0–6 months) but not the longer term (> 6 months).
Overview of economic evaluation
We included one partial economic analysis. Evaluation in Scotland examined the potential costs and consequences of implementing a New Orleans intervention model in Glasgow, comparing estimated costs with estimated costs of the current foster care system (usual care). The study reported that although the New Orleans model would incur greater costs due to being more resource intensive (i.e. involving more healthcare professionals, such as psychologists and psychiatrists), it would significantly reduce the length of stay and probability of return to care. As such implementation could lead to overall savings per child, with a reduction to £88,653 from the current £95,473.
Identification of interventions for development, adaptation and evaluation in the United Kingdom context: work package integration and stakeholder consultation (research questions 5 and 6)
On completion of the method-level syntheses, and the integration of these, we identified candidate evidence-based interventions (RQ5) and conducted stakeholder consultations to consider which approaches would be potentially feasible and acceptable within the UK context, and could progress to further evaluation (RQ6).
Overview of stakeholder consultations
We conducted seven stakeholder consultations between April and September 2022. The details of the stakeholder groups and structure of consultations is presented in Table 7. Consultations with care-experienced young people were conducted through CASCADE Voices and the Fostering Network in Wales Young Person Forum. Recruitment of participants to these consultations was challenging, reflecting widely reported barriers to engagement with this population during the COVID-19 pandemic. 224 Consultations with experienced foster carers were conducted through the Wales Foster Carer Advisory Forum.
| Stakeholder group | Structure of consultations | Participants |
|---|---|---|
| CASCADE Voices (21 May 2022) | Online consultation facilitated by CASCADE engagement manager, Cardiff University | 5 young people aged up to 25 years |
| Public Health Wales LAC Steering Group (7 September 2022) | Online consultation facilitated by clinical lead, LAC Steering Group | 11 professionals |
| Public Health Wales NHS Wales National Safeguarding Network (26 July 2022) | Online consultation facilitated by clinical lead, National Safeguarding Network | 22 professionals |
| The Fostering Network in Wales Young Person Forum (28 April 2022) | Online consultation facilitated by project manager, Fostering Network in Wales | 3 young people aged 16–26 years |
| Wales Foster Carer Advisory Forum (6 April 2022) | Online consultation facilitated by project manager, Fostering Network in Wales | 7 foster carer advisory members |
| Welsh Government Social Services and Integration Directorate (27 April 2022) | Online consultation facilitated by CHIMES principal investigator (RE), Cardiff University | 2 Welsh Government staff |
| Welsh Medical Group (Association for Fostering and Adoption Special Interest Group) (24 June 2022) | Online consultation facilitated by clinical lead, Welsh Medical Group | 12 medical advisors (primarily clinical paediatricians) |
Four stakeholder groups were conducted with policy-makers, professionals and practitioners. First was the Public Health Wales National Health Service (NHS) Wales National Safeguarding Network, which is an independent team of doctors, nurses and a National general practitioner (GP) lead, it provides strategic focus and professional direction to NHS Wales in promoting the welfare and safeguarding of children, particularly those looked after by their local authority. Second was the Welsh Government Social Services and Integration Directorate, which included policy staff with remit for care-experienced children and young people. Third was the Welsh Medical Group, which is an Association for Fostering and Adoption Special Interest Group funded by the Welsh Government. It comprises medical advisors operating in Wales with a role in assessing the well-being of care-experienced children and providing medical advice to local authorities and other adoption and fostering agencies. Fourth was the Public Health Wales Looked-after Children Steering Group, which has clinical representatives from all local health boards in Wales and aims to support health boards and trusts to deliver best practice in improving outcomes for care-experienced children and young people.
Consultations lasted between 30 and 90 minutes as, in some instances, they were part of a wider programme of activity. A member of the CHIMES research team provided a 15- to 30-minute PowerPoint® (Microsoft Corporation, Redmond, WA, USA) presentation outlining key findings from the review (see Report Supplementary Material 21). The structure, language and length of each presentation was adapted to each stakeholder group. Stakeholders were asked to: (1) Consider key context factors identified by the review as influencing implementation and acceptability and reflect upon the relevance of these factors to the UK context. We asked stakeholders if there were additional context factors that should be attended to in future intervention development and research. (2) Appraise the evidence-based interventions identified by the review for potential acceptability, feasibility and effectiveness in the UK context. This discussion point was underpinned by the aims of stage 7 of the TRANSFER model, which recommends discussing the transferability of review findings with stakeholders. 72 Where stakeholders positively appraised an intervention, we asked them to consider potential adaptations that would be required to ensure intervention-context fit in the UK. (3) Identify potential de novo intervention development, including priority intervention types, theories and outcomes.
Note that, while each consultation followed a similar structure, in practice not all discussion points were considered by each group to the same degree. There was variation in the extent of elaboration, explanation and endorsement of different ideas. For example, the young people’s group discussed context factors to a lesser extent. Differences between groups was partly a consequence of the length of the consultations, the fact that different facilitators guided discussions (e.g. the CASCADE engagement manager was led by young people’s interests and priorities) or that stakeholders focused on context factors and interventions more directly related to their own experiences and needs (e.g. foster carers emphasised structural barriers to supporting young people’s mental health and appraised the merits of parenting programmes).
In drawing together, the consultations, we compared and contrasted discussion both within and across groups. The final themes from the discussion were verified against the summary notes, checking for key negative cases. Overall, there was no significant discrepancies between the groups. Rather they had different emphasis on what they felt should be the priority moving forward.
Key context factors and transferability to the United Kingdom context
Consultation groups were presented with an overview of the five key context factors identified by the process evaluation synthesis and the context in which the intervention was delivered and evaluated (Table 8). These were: (1) system resources available for implementation and competing demands; (2) intervention burden; (3) system culture and interprofessional working; (4) the systemic disenfranchisement of children and young people’s identity, values and needs, meaning they feel unable to express dissatisfaction and (5) carer identity values and need, linked to the misalignment between intervention requirements and the wider context of their lives. Most interventions contributing to the context factors were delivered and evaluated in the UK (n = 8 interventions). Table 9 presents the context factors that were discussed as relevant by each group following presentation of all five factors.
| Key context factor | Country | |||
|---|---|---|---|---|
| Australia (n = 1 intervention) |
Ireland (n = 1 intervention) |
UK (n = 8 interventions) |
USA (n = 6 interventions) |
|
| System resources and competing demands | Fostering Connections138 | GIFT/LIFT149,150,215 Kundalini yoga151 MTFC122,136 Mentoring for teenage pregnancy27 SOLID118,154,155 |
PMT146 | |
| Intervention burden | Fostering Connections138 | GIFT/LIFT149,150,215 Head, Heart, Hands139 Kundalini yoga151 |
Family Finding156 PMT146 TFC141,161,164 YIM relationships145 |
|
| System culture and interprofessional working | Fostering Connections138 | CAMHS126 GIFT/LIFT149,150,215 MTFC122,136 SOLID118,154,155 |
Family Finding156 TFC141,161,164 |
|
| Children and young people identity, values and needs | CAMHS126 Computer game120 Mentoring for teenage pregnancy27 SOLID118,154,155 |
IPS132 PMT146 TFC141,161,164 YIM relationships145 |
||
| Carer identity, values and needs | Evolve Behavioural Support Services153 | Fostering Connections138 | Computer game120 Head Heart Hands139 Kundalini yoga151 MTFC122,136 SOLID118,154,155 |
IPS132 PMT146 TF-CBT129 |
| Stakeholder group | Context factors | Priority interventions and outcomes |
|---|---|---|
| CASCADE Voices (21 May 2022) | Care-experienced children and young people’s identities, values, and needs | Priority interventions: mentoring from care-experienced peers/significant adults; carer training (but focus on positive support rather than behavioural management) Priority outcomes: well-being |
| Public Health Wales Looked-after Children Steering Group (7 September 2022) | Limited resources and competing demands; intervention burden; system culture and interprofessional working | Priority interventions: mentoring from care-experienced peers/significant adults; system culture and interprofessional relationships Priority outcomes: not discussed |
| Public Health Wales NHS Wales National Safeguarding Network (26 July 2022) | Limited resources and competing demands | Priority interventions: mentoring from care-experienced peers/significant adults; system culture and interprofessional relationships Priority outcomes: not discussed |
| Fostering Network in Wales Young Person Forum (28 April 2022) | Limited resources and competing demands; intervention burden; care-experienced children and young people’s identities, values and needs | Priority interventions: mentoring from care-experienced peers/significant adults Priority outcomes: well-being |
| Wales Foster Carer Advisory Forum (6 April 2022) | Limited resources and competing demands; intervention burden; system culture and interprofessional working; parent and carers identities, values, and needs | Priority interventions: mentoring from care-experienced peers/significant adults; carer training; system culture and interprofessional relationships Priority outcomes: well-being |
| Welsh Government Social Services and Integration Directorate (27 April 2022) | Limited resources and competing demands | Priority interventions: mentoring from care-experienced peers/significant adults Priority outcomes: not discussed |
| Welsh Medical Group (Association for Fostering and Adoption Special Interest Group) (24 June 2022) | System culture and interprofessional working | Priority interventions: mentoring from care-experienced peers/significant adults; system culture and interprofessional relationships Priority outcomes: not discussed |
Overall, stakeholders identified the need to attend to country-level variations in context, indicating that there may be challenges in adapting international evidence-based approaches, particularly from the USA to the UK. Of note, the Foster Carer Advisory Group reflected on the potential difficulties in transporting parenting interventions from the USA,138,196 due to differences in language and style, variations in parenting practices, and different sets of relationships and resources within the respective social care systems.
It should also be noted that in the first phase of consultations with care-experienced young people, stakeholders queried why the review was considering the transportability of interventions, maintaining that interventions should be co-produced with young people in the UK, as they are frequently devalued and neglected by current social care provision. This reflected a wider limitation with the interventions identified in the present review, namely the non-prioritisation of care-experienced young people’s mental health and well-being and their lack of involvement in the development of relevant interventions and their underpinning theory of change.
Stakeholder groups largely endorsed the five context factors, stating that they reflect many of the central issues influencing service implementation and acceptability in the UK. Across the majority of professional stakeholder groups, participants agreed that a lack of system resources would be the most significant barrier to any intervention delivery. Foster carers in particular maintained that the social care system in the UK is largely ‘broken’, with a lack of support for social workers who are managing complex caseloads and a lack of support for carers who are often managing challenging placements. They suggested that local councils were under increased pressure to return budget underspends to national governments. There were also reported issues around social workers having to constantly ‘firefight’ because social care and CAMHS operate below capacity due to recruitment challenges.
In one of the young person’s groups, participants suggested that there was a higher ratio of children to carers in the UK compared with the USA. With ever increasing numbers in care, this could limit capacity to take on additional interventions. While less specific in nature, Welsh Government stakeholders observed that there were extensive programmes and policies in place to support the mental health of care-experienced young people, but there was an ongoing implementation gap where they were not being taken up. Further work would be needed to consider if any additional resource would be needed to address this issue.
The two young people and one foster carer group emphasised issues around intervention burden. Young people reflected on mentoring-based interventions, observing both the cognitive and emotional burden this could place on the individual mentor when dealing with a child’s difficult experiences, so the mentor would also require supervision. There were questions whether this extra support could be provided. Foster carers mentioned the time and cognitive burden of constantly testing new interventions, which rarely translates into long-term change and improved outcomes for children in their care.
Interprofessional working was discussed in depth by three stakeholder groups (foster carers, Looked-after Children Steering Group, Welsh Medical Group). Foster carers characterised the social work system as ‘risk averse’ and ‘legalistic’, with different professionals conservatively working in their own discrete area without any creativity in collaboration. Carers felt that this translated into carers being mistrusted and receiving stringent deadlines and statutory targets to satisfy professionals in other parts of the system. They expressed a desire for an organisation or the government to take oversight and co-ordinate the system more effectively.
The final two context factors of identity were explored by four of the stakeholder groups (two young people’s groups, foster carers, Welsh Government policy stakeholders). In terms of young people, policy stakeholders noted that drop out from interventions was high and somehow there were challenges in engaging this population. In terms of carer identity, there were concerns among foster carers about the extension of their remit into a therapeutic role where they did not have sufficient skill or training. More significantly, they reported feeling undervalued and deskilled within the system, and that other professionals consistently failed to listen to them. They also reflected on the challenge of practically co-ordinating meetings where carers, social workers and other professionals could all attend. As such, while there was agreement that parenting courses could be helpful, there was a sense that there needed to be clear boundaries to the carer identity and for them to be supported by a culture change in the system.
Stakeholder perspectives on evidence-based interventions
As part of the consultations, we shared an overview of a range of intervention types, theories and specific packages with stakeholders that mapped across the socioecological model. Initially, as per RQ5, we intended to construct an overarching candidate programme theory to present to stakeholders. However, the findings of the review suggested that this was not feasible or appropriate as theories were underspecified, there was limited evidence of combining theories and components, and initial stakeholder feedback indicated that particular approaches (e.g. parenting classes) could be polarising in terms of acceptability and feasibility to different stakeholder groups. As such, we decided to present individual interventions.
The specific interventions presented to stakeholders indicated largely favourable evidence of effectiveness in the review, although for more complex organisational and community interventions, the evidence base was more mixed. The sampling of interventions was also partly informed by 2021 NICE guidance recommending further development and evaluation of mentoring, parenting and interprofessional collaboration interventions to address the mental health and well-being of care-experienced young people. 21 The presented interventions were:
-
Intra/interpersonal:
-
Interpersonal:
-
Organisation/community:
Intra/interpersonal
Stakeholders did not explicitly discuss the theories commonly underpinning interventions operating across these socioecological domains: attachment theory,227 positive youth development,226 resilience and social learning theory. 227 However, discussion did draw out the resonance between these theories and stakeholder preferences, with all participant groups indicating the need for positive, supportive attachments and the importance of consistent relationships with others.
Participants, particularly in the two young people’s groups discussed the FHF intervention at length. 25,26,111,112,115,116,147 The intervention combines a group-skills curriculum with mentoring. Young people reported a number of positive features of this type of approach. This included providing support to children aged 9–11 years, with participants feeling that individuals this young often didn’t get to access support. Equally, participants felt this was an appropriate time point in someone’s care journey as they suggested that 10 years old is when young people start to notice they are ‘in care’ or ‘different’ and begin to encounter the challenges of the system. However, this was not to suggest that older young people should be excluded.
The Fostering Network in Wales Young Person Forum indicated a number of issues with the skills curriculum, however, citing experiences of similar interventions causing emotional distress. Participants noted that young people in care may struggle to express emotions and it could be difficult if there was an expectation to share in a group context. They also discussed accounts of having to miss school following interventions or service meetings due to the stressful impact of having to share feelings.
All stakeholder groups were supportive of mentoring approaches that would provide positive relationships and meaningful and consistent attachments. They might also offer modelling of prosocial, healthy behaviours that could be replicated by young people. However, there were two central issues identified by both young people groups: the burdensome time commitment and the delivery agent. In regard to the issue of commitment, young people generally felt that 9 months was too long. There were further concerns that young people would have to miss out on socialising with their peer group or family members to attend, with participants citing experiences of missing out on events that were important to them so they could go to appointments. They suggested that a flexible intervention where they could drop in and out would be more acceptable.
In terms of delivery agent, there was consideration as to who constitutes an appropriate mentor. FHF uses graduate social workers. Young people queried whether this group of professionals had the requisite skills to support an intervention targeting mental health, and felt it may be within the remit of CAMHS. However, it should be noted that the intervention is not focused on individuals with diagnosed mental health conditions and participants may not necessarily meet the eligibility threshold for CAMHS.
There was also the issue, which reflected a key context factor in the process evaluation synthesis, with participants feeling themselves to be a burden in the system, stating that they already struggled to get any time with their social worker and did not anticipate that this intervention would change the situation. In contrast, some young people felt that having a mentor with social work experience could be helpful, as they understood how to navigate the care experience.
Participants felt more favourable about the skills curriculum and mentoring if they could definitely include other care-experienced young people and if individuals with experience of care were mentors. They felt that it could be positive being in a group with others who had similar experiences, and that they could build a stronger relationship with the mentor if they had experience of the care system rather than having studied it. Regardless of the mentor’s identity, participants felt that there was a risk associated with another relationship being terminated, which may create a sense of abandonment.
Interpersonal
The interpersonal type of intervention primarily addressed parenting knowledge and skills development. It was a particular focus of discussion in stakeholder consultations with young people and foster carers. In terms of the underpinning mechanisms of these approaches, young people felt that the emphasis on ‘behaviour management’109 was inappropriate, and they needed to be broader, focusing on well-being and positive relationships, which is reflected in some parenting approaches (e.g. ABC). 171
Consideration of types of intervention tended not to focus on a specific parenting intervention package, and discussion was more generic. Young people maintained that some training for carers in mental health and well-being support should be compulsory, given the complex histories and needs of many individuals who enter care. Both young people and carers felt that comprehensive training would potentially reduce the number of care placement breakdowns, maintaining that a lack of suitable carer training meant that young people were often rejected and moved to a new placement when they could not be ‘managed’. Young people felt that such training should have a particular focus on prevention, which would entail identifying early signs of mental health difficulties and improving how carers and other professionals talk to young people about their feelings.
Foster carers identified scope to optimise existing approaches. Some wanted more consistent, ongoing support rather than a discrete period of training, which they felt that interventions, such as KEEP delivered. 28,29,102,103,125,127,152,182,201 For example, this would include an ongoing contact they could telephone to ask for advice and support. They also felt that existing parenting courses were often quite generic in their approach and needed more individualisation to specific needs and contexts.
Discussion of interventions also intersected with issues around carer identity and the role and responsibilities of the profession. Foster carers maintained that the UK social care system has a focus on individualising structural issues and promoting interpersonal approaches that place responsibility on carers rather than on community and organisational practice. They felt that parent training programmes would contribute to the failure to address the structural determinants of poor mental health among children and young people in care, instead making carers unfairly accountable. Therefore, while parenting interventions were recognised as important, there was a preference for more organisational approaches that worked on interprofessional relationships.
Barriers to the implementation of parenting interventions were identified in the UK context. Young people highlighted the burden of time placed on carers, noting that their own carers already attended support groups to help with understanding the mental health of individuals in care, and this was too much for the carers given their other commitments. Interestingly, young people felt that if carers spent a significant amount of time training, there would not be enough time to undertake parenting and build a relationship with them. They did suggest that some flexibility in delivery mode, maintaining that the option for online provision could reduce the burden.
Organisation and community
Consultation discussions with policy-makers and medical and social care practitioners were particularly focused on organisational and community interventions. They were also considered to a lesser extent by young foster carers. Discussion of the theory, such as facilitating a trauma-informed approach, had support due to the potential for efficient interprofessional collaboration that could address current issues around lack of awareness across the system and poor multiagency communication. 34,119,170,191 However, both Welsh Government participants expressed some concern over the accessibility and understandability of this language around ‘trauma’ models, and the potential to alienate young people in care. This was part of a wider belief that young people want to be part of positively orientated clubs and social events rather than treatment services.
Discussion of preferable types of interventions moved beyond specific intervention packages and was more general. Young people and foster carers both felt that professionals should be trained in attachment and trauma-informed models of practice. More specifically, young people felt that social workers needed training to better support foster carers and those in care, due to a feeling that social workers are ‘quick to judge’ young people’s behaviour without understanding the root causes.
Foster carers were supportive of interventions that align the ethos of professional organisations, with the potential to address issues around interprofessional working where there is misalignment in approaches. Specifically, they felt interventions that created a trauma-informed approach in educational settings would be useful, suggesting that schools are aware of ACEs but not working in a trauma-informed way. This disjoint in approach between carers and schools had left carers feeling that they are on different tracks, and that carers are having to pick up supporting the mental health and well-being of children and young people, which had added further pressure to their work.
Stakeholder perspectives on de novo intervention development
Following exploration of evidence-based interventions identified by the review, stakeholders subsequently considered new intervention approaches that they would recommend for development, implementation and evaluation within the UK context.
As a starting point, stakeholders identified principles to underpin future intervention development. First, reflecting findings in the process evaluation synthesis theme on care-experienced young people’s identity is that individuals in care should not be treated as a homogeneous group. Rather there should be sensitivity and flexibility in responding to their needs at a time that suits them. Young people from CASCADE Voices stated that interventions need to be tailored to the stage of the individual care journey, maintaining that support should differ for a young person who is just entering care, someone who is struggling in their placement and a care leaver who is now living independently. This resonates with reports in the process evaluation synthesis, where intervention participants emphasised the need for intervention adaptability and scope for tailoring to meet local needs. 146,153 Second, and primarily considered by policy stakeholders, is the need to develop something scalable that can potentially be delivered on a regional or national scale. In this case, stakeholders from the NHS Safeguarding Network cited the importance of issues around workforce capability and capacity to deliver interventions at scale.
In terms of theory, young people stakeholder groups wanted a clear emphasis on early support and prevention to supplement existing provision around specialist mental health treatment. Building on reflections on theories that underpin existing approaches, stakeholders recommended approaches that promote positive relationships, which may link to attachment theory,225 positive youth development,226 resilience and social learning theory. 227 They also wanted attachment and trauma-awareness integrated into the system more widely. 34,119,170,191
Stakeholders recommended two types of interventions: mentoring, primarily by care-experienced young people and trusted adults, and promotion of interprofessional working and system change. In practice, these recommendations built upon discussion of existing intervention packages and so, while participants suggested de novo intervention work, it is possible that adaptation of the evidence-based approaches identified by the review may be feasible and more resource efficient.
The first type of intervention described models of mentoring. Participants suggested that mentoring should start from the age of 10 years, when children may become more aware of some of the structural disadvantages of being in care and may be developmentally ready to engage in social and emotional skills development. Young people’s stakeholder groups advocated for mentoring delivered by someone with extensive experience or knowledge of the care system (e.g. care leavers) so that they would understand potential issues and challenges. They felt that it was difficult to forge a positive and meaningful relationship with those who had not shared similar life events. Equally, as the mentoring models in the review were often unpinned by social learning theory,227 there was a sense that young people were less inclined to observe behavioural models from individuals to whom who they could not relate, or they may lack the belief that they can replicate certain modelled actions due to their structurally disadvantaged position of being in care. Participants further identified a range of skills and characteristics that they would like a mentor to have, including understanding, trustworthiness, honesty, compassionate nature and ability to speak to the young person as an equal.
Stakeholders explored how mentoring relationships could fit with the wider system of support. The two young people’s groups felt that mentoring could serve as early support while individuals were waiting for referrals to specialist mental health services, such as CAMHS. They also felt that other groups may be brought into the mentoring relationship where appropriate; for example, suggesting that foster carers may be involved in some later sessions to be aware of their child’s progress and needs.
The second type of intervention focused on addressing interprofessional relationships, which may be supported by upskilling professional groups involved in the care system. Stakeholders indicated that components could include training in trauma-informed or attachment-informed practice across local authority health, education and social care teams. It also extended to include recommendations for implementation models that facilitate multiagency wraparound provision for individuals in care, by having clearer and more co-ordinated communication channels, regular interprofessional meetings and potentially shared departmental budgets.
While stakeholder groups explored the potential for new intervention development, it should be noted that not all participants felt that the system needed a new approach. Indeed, the Welsh Government consultation discussion maintained there was a wealth of interventions already being funded and there was probably a gap between what young people perceive as being implemented and what is actually available to them. Stakeholders from the Welsh Medical Group reflected that there were already key policy efforts to integrate a systems approach into social care in Wales, as advocated by the Children’s Commissioner for Wales’ No Wrong Door report,228 which maintains a co-ordinated approach to supporting young people’s needs where all professional groups have a responsibility in working together to improve outcomes. As such the focus may need to be on addressing the implementation gap, and focusing on how awareness and access may be optimised moving forward.
Priority intervention types, theories and outcomes
Following consultations, we constructed two integrative matrices to map stakeholder preferences against the interventions included in the evidence base. 94 The first matrix mapped stakeholders’ priority intervention theories and types. The second mapped stakeholders’ priority outcomes. The aim of this approach was twofold. First, it demonstrated if interventions, and the associated evidence base, are addressing what stakeholders think is important and meaningful in terms of the mental health and well-being of care-experienced young people. Identifying incongruence in the evidence and priorities can help to refine the intervention and research agenda moving forward.
Second, it supplemented the process of identifying potential interventions to progress for future development, adaptation and evaluation. As part of the consultations, the emphasis was primarily on discussing a selection of approaches that demonstrated some evidence of effectiveness. However, we recognised that stakeholders could express a preference for theories or components that may not have been included in the consultation presentation but were eligible for inclusion in the CHIMES review. Constructing the matrix allowed us to iteratively return to the included interventions to identify if there were additional approaches that aligned with stakeholders’ priorities, but which may not have demonstrated effectiveness or even showed harm.
The process for constructing the matrices commenced with classifying priority intervention types, theories and outcomes from stakeholder data. This information was collated from study reports of interventions’ programme theories, thin- and rich-process evaluations; stakeholder consultations in the initial phase of study conduct, and stakeholder consultations during WP6 consultations. These were mapped to the interventions included in the review. Where interventions had been included in the outcome synthesis, we indicated the associated evidence base. They were categorised according to there being clear evidence of effectiveness, mixed evidence (i.e. effectiveness was not reported for all primary outcomes, was not consistent across reports (e.g. child and carers) or was not sustained over time) or no effectiveness. Similarly, we indicated where study reports included evidence that was not an outcome evaluation.
Priority intervention theories and types
Taken together, consultation, theory and process evaluation identified four key types of interventions that stakeholders would prioritise moving forward (see Table 10). Two of these operated within the interpersonal domain, focusing on relationships between care-experienced young people and peers, and their relationships with other significant adults (not carers). Mentoring was the primary mechanism to facilitate these relationships, particularly individuals who had personal knowledge or experience of care. Stakeholder discussions did not always have an explicit theoretical underpinning, but there was clear resonance with attachment theory,225 positive youth development226 and social learning theory,227 and general social support to construct strong social networks that promote positive health behaviours and outcomes.
| Type of evidence | Priority intervention types and theories | |||
|---|---|---|---|---|
| Interpersonal | Organisational/community/policy | |||
| Mentoring relationships with peers | Mentoring relationships with key others | Interprofessional/multiagency relationships and ethos | Funding for mental health and social care services | |
| Theories: attachment; positive youth development; social learning theory; social network support | Theories: attachment; positive youth development; social learning theory; social network support | Theories: attachment; trauma-informed practice; generic system change | None | |
| Evidence of effectiveness | TAKE CHARGE159 | FHFs25,111,112,115,147 | ||
| Mixed evidence of effectiveness | Family Finding156,186,194 | CARE,119,191 TST34 | ||
| No evidence of effectiveness | Mentoring for teenage pregnancy56 | Choice and availability of different community outpatient mental health services187 | ||
| Included in evidence map | ||||
| Theory and process evidence (feasibility, acceptability) | SOLID118,154,155 | Therapeutic mentoring,211 YIM143 | GIFT, 149,150,215 Optimising CAMHS126 | |
Table 10 presents the interventions included in the review that address the types and theories prioritised by stakeholders. Two mentoring interventions from the USA demonstrate some evidence of effectiveness, with FHF25,111,112,115,147 having a clear theoretical basis. 25,26,111,112,115,116,147,159 Four further interventions had a focus on mentoring, with a clearer focus on implementation and acceptability, reporting a range of system challenges to delivery. 118,145,154,155,211,229
Two of the prioritised intervention types targeted the organisational, community and policy domains. The first, which was mainly cited by carers and professionals, included interventions to address interprofessional relationships and the creation of multiagency teams to support decision-making. This was somewhat under-theorised, but referenced the potential to ensure everyone was responsible for young people’s mental health by upskilling professionals in attachment and trauma-informed practice, which would also lead to a common language that could facilitate collaboration. Carers also cited the need for mechanisms to improve the professional standing of carers to have a stronger voice in decision-making. The second type was increased resources for mental health and social care services. This was cited across data sources. There was no theoretical basis attached to this, but rather just a need to increase the availability of provision and reduce waiting lists for mental health service access for care-experienced young people. Relatedly, young people wanted more structural-level interventions that focused on improving service funding rather than focusing on their individual behaviours.
There were only six interventions that addressed these organisational, community and policy priorities. The available evidence did not indicate the effectiveness of these approaches, although CARE119,191 and TST34 demonstrated some mixed impacts. Two interventions from the UK were process evaluations that may support future optimisation of implementation. 126,149,150,215
Priority intervention outcomes
Together, the consultations and data from theory and process evaluations identified five key outcome domains stakeholders wanted to be targeted by interventions (Table 11). These domains were: positive constructs of well-being; quality of relationships with peers; quality of relationships with carers and other significant adults; suicide-related outcomes. As part of the matrix construction, we included priority outcomes where there was harmonisation across stakeholder groups in terms of support for them. For some cited outcome domains, notably diagnosable behavioural disorders, carer and professional stakeholders indicated that they were important. However, young people critiqued the focus on ‘deficit models’ when addressing their mental health and wanted more positively orientated approaches that looked more at their well-being. As such, given that care-experienced young people’s voices were often missing from the process of intervention development and evaluation, we focused on priorities with some endorsement from this group.
| Priority intervention outcomes | |||||
|---|---|---|---|---|---|
| Subjective well-being | Child–peer relationships | Child–carer/other adult relationships or carer–child relationships | Life skills | Suicide-related outcomes | |
| Evidence of effectiveness | FHFs25,26,111,115,147 | FHFs25 | |||
| Mixed evidence of effectiveness | KEEP152 | CARE119 | Connect-KP;162 CARE;119 Family Finding156,186 Fostering Changes134,179 |
CARE191 | |
| No evidence of effectiveness | Wave by Wave208 | MTFC107 | CDIT180 Incredible Years130 kContact209 MTFC107 TPFC157 |
HealthRHYTHMS88 Mentoring for teenage pregnancy56 | |
| Included in evidence map only | EFP100 Opportunities Box204 Registered Education Savings Plan176 Type of care placement197 |
Opportunities Box204 | Sanctuary Model202 EFP100 Head Start35 Prevention intervention183 |
CBCT142 | |
| Theory and recess evidence (feasibility, acceptability) only | Intensive Permanence Systems132 Kundalini Yoga151 SOLID118,154,155 YIM Relationships147 |
YIM Relationships145 | TFC110 YIM Relationships145 GIFT213 TFC106 Solution-Focused Parent Group148 TFTC141 |
TFC-OY164 | |
Of the included 64 interventions, 11 included measurements of subjective well-being or its associated domains of life satisfaction and quality of life. FHF25,26,111,112,115,116,147 was the single intervention demonstrating effectiveness in targeting these domains. 25,26,111,112,115,116,147 Four interventions targeted suicide-related outcomes. CARE had mixed evidence of effect. 119,191 Importantly, both FHF and CARE119,191 aligned with the intervention theories and types prioritised by stakeholder related to relationships. Although potentially serving as mediators rather than primary outcomes, we also mapped interventions that addressed relationship-based measures and the skills to engage in such relationships.
Recommendations for intervention development, adaptation and evaluation
Methods for intervention development and adaptation
While the CHIMES review largely focused on the evaluation of interventions, it generated important insights into the process of intervention development and adaptation. These insights were primarily ascertained through the quality appraisal of intervention theory and process evaluations. Generally, there was a lack of use of relevant frameworks and models to support intervention development,61,98,229 specifically in relation to identifying and articulating the programme theory. Importantly, there was a dearth of reported engagement with stakeholder groups in theory development, specifically children and young people. This should be remedied moving forward to ensure that interventions are contextually relevant and respond to local stakeholders understanding of the problem.
The review also indicated potential issues with the transportability of interventions across contexts. 138,196 In these instances, interventions failed to replicate feasibility, acceptability or effectiveness. Given the predominance of interventions developed and evaluated in the USA, there remains a significant lack of knowledge of how interventions can function in different contexts and the most effective mechanisms for supporting their successful transfer. More work is required in this field to integrate adaptation frameworks into the process of transporting approaches to maximise the likelihood of positive outcomes in new contexts. 64
Recommended interventions for development and/or adaptation
Drawing together the results of the review-level mixed-method synthesis, combined with stakeholder consultations, we can make recommendations in regard to intervention theories, types and outcomes to progress to further intervention development, adaptation and evaluation in the UK context.
In terms of programme theory, it is challenging to identify a central set of theoretical tenets as interventions were largely under-theorised and stakeholder consultation emphasised intervention types rather than mechanisms. However, there were two clear sets of theories that may be taken forward. The first set are orientated to positive relationship-based mechanisms, as expounded by attachment theory,225 social learning theory,227 positive youth development226 and, less specifically, social network approaches. These theories have been a key feature of mentoring from both peers and significant adults. 25–27,111,112,115,116,118,147,154,155 The second set is focused on creating a shared working practice and more efficient interprofessional relationships and decision-making to provide more comprehensive and tailored support to families and children. This may be facilitated by creating a shared theoretical alignment across agencies, such as attachment. 119,191
Interestingly, there was some evidence for interpersonal interventions targeting parents and carers to promote positive parenting. These included a combination of theoretical approaches, from social learning tyheory108 to behavioural management. 109 Stakeholders advocated for parenting interventions more aligned with ‘positive’ approaches of social learning theory, drawing parallels with mentoring by significant adults, with less endorsement of parenting interventions that rely on behavioural management techniques.
Specific recommendations for intervention types to progress to development and evaluation include a focus on mentoring and system approaches for ethos change, which are also recommended by a 2021 NICE review. 52,54 For mentoring approaches, this could include new intervention development. However, there are US-based interventions that could be considered for adaptation to the UK setting, such as TAKE CHARGE or FHF.
Recommendations for potential adaptations include changing the delivery agents to individuals with experience or knowledge of care. Equally, mentoring and social network interventions in the UK have demonstrated a lack of feasibility, largely due to the five context factors identified by the process evaluation synthesis. Adaptation could require contextual restructuring to account for system-level characteristics. 27,118,154,155
For interventions operating across organisations and communities to realign ethos, draw together professional groups and increase resources, evidence of effectiveness has not been fully established. 34,119,187 CARE is the only candidate intervention we identified with a mixed evidence base, showing limited evidence of reducing self-harm in residential settings. 119,191 Equally evaluation of such approaches in the UK have largely focused on feasibility and piloting testing, demonstrating potential acceptability but identifying issues around implementation. 149,150,215 Again, these issues link to the five context factors from the review, especially regarding interprofessional relationships. Hence, while there may be acceptability for this type of approach, developmental work is required to ensure an approach that is responsive to the specific health and social care system in the UK.
Interventions need to target a wider range of outcomes, particularly those that are prioritised by care-experienced children and young people and other stakeholders. They should include a focus on subjective well-being and suicide-related outcomes. Few interventions currently target well-being, although it is being addressed by some mentoring programmes or interventions promoting social networks. 25,26,111,112,115,116,118,145,147,154,155 Equally, suicide-behaviour outcomes are rarely assessed, although they have been theorised as appropriate in interventions that modify organisational and interagency culture and ethos. 119,191
One of the RQs of the CHIMES review (RQ5) was to assess if prioritised theories, types, and outcomes could be combined into an overarching programme theory. Based on the interventions identified in the review, there is no currently available evidence for interventions that combine mentoring approaches with system-level interventions that focus on aspects of culture, multiagency working and interprofessional relationships. However, given the fact that process evaluations of mentoring intervention or social network building relationships report issues around the health of care-experienced young people not being ‘core business’, lack of resources and the systemic devaluing of young people, there is potential for organisational and community-based approaches to facilitate a culture that mitigates some of these structural barriers. 27,118,154,155 The identification of theories at the organisational and community level may be of import. These either sought to reconfigure organisational policies and practices to create a trauma-informed therapeutic ethos119,191 or delivered enhanced implementation models to facilitate the delivery of parenting interventions. 28,102,107,119
Evaluation study designs
Types of evaluation eligible for inclusion in the review were theory, process, outcome and economic. The inclusion criteria for the outcome study designs were RCTs or non-randomised evaluations. No quality threshold was used as part of the inclusion criteria for study design.
There were a number of limitations with existing approaches to evaluation that could be addressed to further strengthen the evidence base. First, there is a need to improve description and reporting of the study designs used in evaluation in this area. In particular, study reports often conflated feasibility testing with outcome evaluations. Relatedly, claims about effectiveness were often made where evaluations did not include a power calculation or were underpowered. As such it would be helpful for intervention studies to engage more clearly with frameworks that recommend and detail different evaluation study designs that are appropriate to different aims and RQs. 62
Second, there are study designs that are currently under-used, which, given the mixed evidence base, could helpfully be employed moving forward. There is a lack of theoretical descriptions, and qualitative research, process evaluations, realist evaluation or mediation analysis within outcome evaluations can all support the articulation and testing of interventions’ causal mechanisms. Theory evaluations also need to include a clear focus on context, working to understand how interventions interact with the system and how this changes over time. 57
There is also a need for more economic evaluations, which reflects a wider issue in the field of social care. 76 A 2021 systematic review, conducted by members of the CHIMES review team, identified that, in the field of children and young people’s social care more widely, there has been a tendency to use cost–benefit analysis and, while this is useful, there is also scope to take more advantage of cost consequence analysis. The review further provide 10 recommendations to improve the conduct of economic evaluations, which include: pilot measures and data sources; engage with stakeholders; explore strategies to maintain recruitment; define and justify the approach; define and justify the time horizon; clearly identify all costs; identify routine data sources; carry out sensitivity analysis; carry out subgroup analysis; and consider using economic models alongside or as an alternative to a within-trial economic evaluation. 76
Intervention reporting and future systematic reviews
Reflecting on the CHIMES review and its associated challenges, we have a number of recommendations that can support the future conduct of systematic reviews at the interface of public health and social care. First, is the need to improve the reporting of interventions. Currently, there is a lack of use of reporting standards for social care interventions, such as the TIDieR framework, to describe theory, components and implementation strategies. 214 Equally, given the reviews’ emphasis on the importance of context and the contextual contingency of intervention effects, future syntheses would benefit from more comprehensive reporting of key context factors within evaluations, potentially drawing on models, such as the CICI framework. 82
Second, we recommend further standardisation and harmonisation of outcome measurements used to assess intervention effectiveness, which can support meta-analyses. While there were a select number of outcome measures routinely used in evaluations, such as the SDQ and Children’s Global Assessment Scales, further work might be undertaken to support the implementation of core outcome measurements across domains of subjective well-being, mental health, behavioural and neurodevelopmental disorders and suicide-related outcomes.
Third, the review has highlighted the utility of complex-systems informed approaches,57,58 that draw together theory, process and outcome evaluations to understand how system characteristics shape intervention implementation and structure outcomes. To date, the reliance on synthesising outcome studies in reviews of the mental health of care-experienced young people has ensured limited understanding of how interventions work in context and their potential transportability to other systems. As we have highlighted the strength of the evidence base in United States and issues about replicability in other countries, we need to foreground questions about the applicability of international evidence to local contexts as part of the review process. Although published after commencement of the present review, we found the TRANSFER framework to be supportive in exploring stakeholder priorities and perspectives to understand issues around transportability, and further integration of such frameworks into reviews would help to progress the evidence base. 72
Summary recommendations for research
We developed a set of six core questions for researchers to consider when developing, adapting, evaluating and reporting interventions, specifically in relation to mental health interventions for care-experienced children and young people. These were informed by our reflections on the evidence base and our experiences of conducting the CHIMES review.
-
Stakeholder involvement in intervention development: were care-experienced children and young people, parents and carers, and health and social care professionals involved in the development of the intervention? Stakeholders, especially young people, have largely been excluded from the process of intervention development.
-
Describing the intervention theory and components: have you described the programme theory and components so that it could be replicated? To date, interventions have been under-theorised and have not used reporting guidelines to describe the theory, components or implementation strategies.
-
Intervention transportability and adaptation: if an intervention has been delivered and evaluated in a different context, have you considered potential similarities and differences between the original and new context and the need for adaptation? Most of the evidence base is from a select number of countries (e.g. USA) and there may be need to adapt interventions to meet the needs of different social care and healthcare systems.
-
Appropriate intervention evaluation study designs: have you selected an appropriate research design that can address the evaluation RQ? Evaluations often make claims about intervention effectiveness based on feasibility or pilot studies, or from underpowered outcome evaluations.
-
Integrated intervention evaluation study designs: does your intervention evaluation integrate description of the programme theory, outcome evaluation, process evaluation and economic evaluation? There is currently a lack of theory and economic evaluations in social care.
-
Complex-systems informed systematic reviews: does your systematic review take account of the contexts in which interventions are developed, delivered and evaluated? Complex-systems informed systematic review can support decision-making about the potentially transportability of the international evidence base to local contexts.
Summary recommendations for policy and practice
We developed a set of 10 core questions for policy-makers and practitioners to consider when implementing interventions targeting the mental health and well-being of care-experienced children and young people (Figure 20). This is an approach developed in previous Cochrane reviews. 95 Questions were informed by the evidence synthesis, associated GRADE statements with high to moderate certainty, and key reflections from stakeholder consultations. The questions have a particular focus on optimising the implementation of interventions, especially by making sure that it functions in the UK context, and ensuring stakeholder acceptability.
FIGURE 20.
Questions for policy-makers and practitioners.
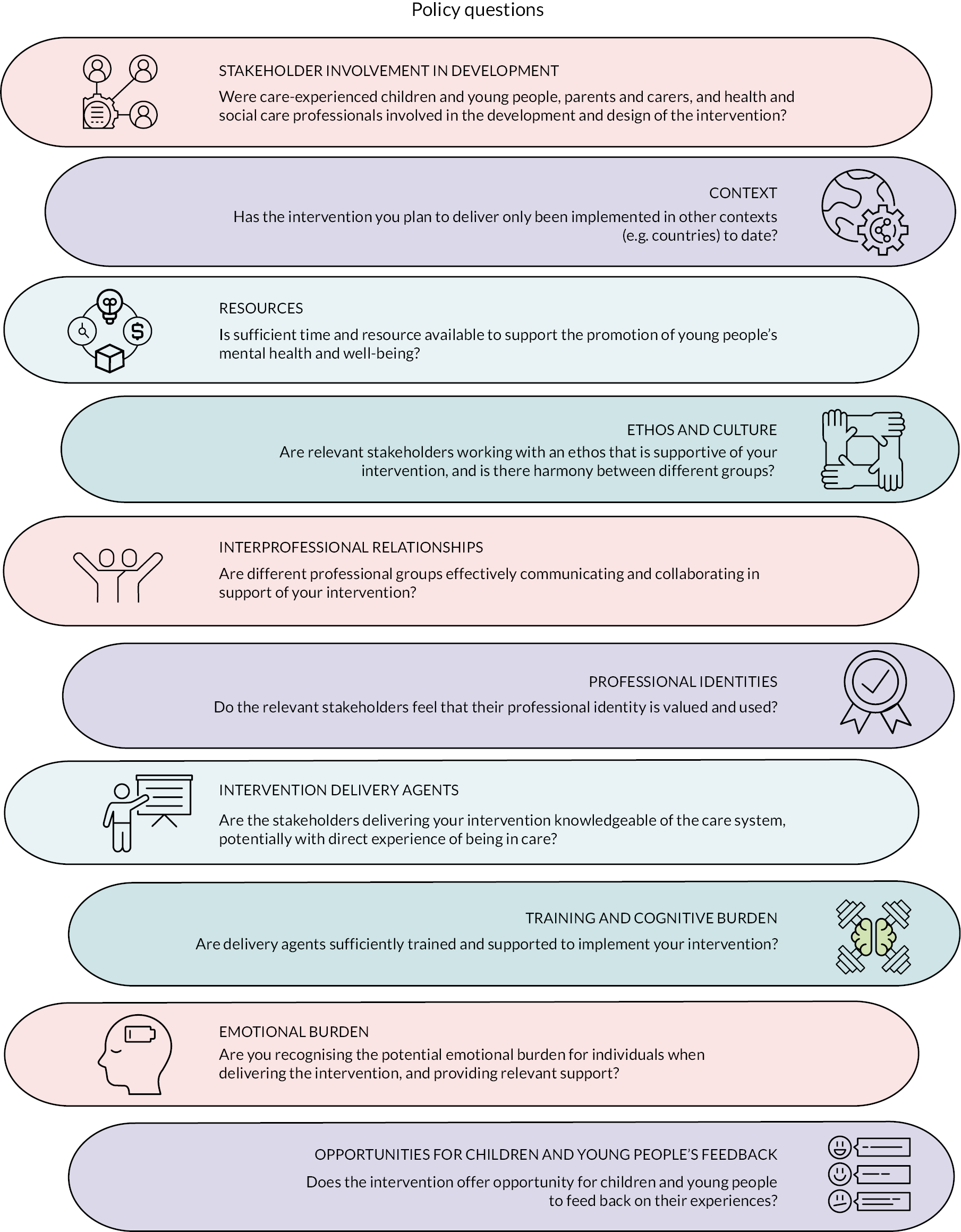
-
Stakeholder involvement in intervention development: were care-experienced children and young people, parents and carers, and health and social care professionals involved in the development and design of the intervention and identification of target outcomes? Young people have often been excluded from the development process; co-producing interventions with the target population may increase the likelihood of them being engaging and acceptable.
-
Context: has the intervention you plan to deliver only been implemented in other contexts (e.g. countries) to date? If so, you will need to consider potential differences and similarities in implementation contexts. The intervention, its implementation strategies and the implementation context may need to be modified, provided that this modification does not significantly comprise the functioning of the intervention.
-
Resources: are sufficient time and resources available to support the promotion of young people’s mental health and well-being? Sometimes, the health of care-experienced individuals is not prioritised in a system with numerous competing demands, which can prevent delivery agents having the time to attend necessary training or to implement the intervention.
-
Ethos and culture: are relevant stakeholders working with an ethos that is supportive of your intervention and is there harmony between different groups? Sometimes delivery agents find it easier to support and implement interventions when there is alignment in organisational culture, practices and values. This might include a trauma-informed or attachment-based approach to working.
-
Interprofessional relationships: are different professional groups effectively communicating and collaborating in support of your intervention? There can be historic tensions between different professional groups and it may be important to work to resolve such issues to facilitate multiagency working that is supportive of intervention implementation.
-
Professional identities: do the relevant stakeholders feel that their professional identity is valued and used? Parents and carers in particular can feel that their expertise is devalued and that they are excluded as an important group that can make a meaningful contribution to intervention implementation.
-
Intervention delivery agents: are the stakeholders delivering your intervention knowledgeable of the care system, potentially with direct experience of being in care? Care-experienced young people and other relevant stakeholders think that it is important that they are supported by peers and adults that understand their unique histories and needs.
-
Training and cognitive burden: are delivery agents sufficiently trained and supported to implement your intervention? Parents and carers in particular can feel that they do not have the required skill, knowledge and support to deliver interventions, specifically in relation to mental health and well-being.
-
Emotional burden: are you recognising the potential emotional burden for individuals when delivering the intervention and providing relevant support? Social and healthcare professionals, and parents and carers, can often find it an emotional experience to offer support around the mental health and well-being of care-experienced young people, in addition to the individuals close to the child.
-
Opportunities for children and young people’s feedback: does the intervention offer opportunity for children and young people to feedback on their experiences? Sometimes care-experienced young people feel that they do not have a voice to express their needs, so dropping out or disengaging may be the only mechanism available to express that an intervention does not suit their preferences. Designated feedback loops, with the intervention being enhanced to meet young people’s needs, may reduce disengagement.
Equality, diversity and inclusion
We have aimed to conduct an accessible and inclusive review, which has been facilitated by a diverse research team and the engagement of the Fostering Network in Wales as a collaborating partner. The involvement of this partner was supportive in ensuring the language and terminology was suited to a range of academic, policy and practice partners.
In regard to the review, equality, diversity and inclusion were central driving priorities. We note that the overarching aim of the review was to explore how effective interventions are for a historically underserved group who experience a higher burden of mental health problems compared with the general population and how we might optimise provision in the UK context. In particular, we aimed to progress understanding of the needs of diverse care-experienced populations by not treating them as a homogenous group, instead exploring between group variations through our consideration of equity harms.
We sought to include a diverse range of stakeholders invested in the mental health and well-being of care-experienced children and young people, notably care-experienced young people themselves. In particular, we engaged young people and carers who had experience of different care types, such as foster care and kinship care. We recognise that this was limited by the COVID-19 pandemic, as detailed in the following section.
CHIMES patient and public involvement
The CHIMES review involved comprehensive stakeholder engagement throughout. With reference to the TRANSFER Framework,72 we engaged the Fostering Network in Wales in the initial identification and scoping of the review. Stakeholder groups were subsequently consulted to confirm the remit of the review. Finally, as reported in the discussion chapter, stakeholders were engaged to consider the transferability of the evidence base to the UK context. The GRIPP2 Short Form Reporting Checklist included in the project web page details the phases of stakeholder engagement. 71
CHIMES review strengths and limitations
The CHIMES review is one of the first complex-systems-informed, mixed-method systematic review conducted in relation to the health and well-being of care-experienced children and young people. As a result, in addition to identifying the evidence base for interventions targeting mental health, we provide useful methodological directions for considering the transportability and relevance of interventions across international social care and healthcare systems.
There are a number of limitations that should be considered when interpreting the findings of this review. The first set of limitations relate to the WP1–4 and conduct of the searches and method-level syntheses. First, the available literature is complex to search due to international variations in nomenclature and heterogeneity within the care-experience population, which means that it was challenging to identify all relevant reports. Second, while we undertook comprehensive searches for economic evaluations, we recognise that they may be additional partial evaluations not retrieved by the search strategy. These economic evaluations might provide useful insight moving forward on some of the challenges and rationales in existing practice. Third, the limited reporting of interventions and their associated evaluations, and the fact that they did not use reporting guidance, provided challenges in classifying and mapping study reports. Fourth, measures drew on a range of informants, including clinicians, parents and carers, and children and young people themselves. Where multiple sources were used for one outcome, findings were frequently inconsistent and, in some cases, children and young people and their carers reported opposing results. Additionally, for the meta-analysis, we chose to differentiate between ‘shorter-term’ (outcomes measured within 6 months of baseline) and ‘longer-term’ outcomes (outcomes measured more than 6 months after baseline). This involved combining studies with a range of follow-up time points. However, we felt this was necessitated by the relatively small number of studies available across the multiple different outcome domains.
The second set of limitations relate to the review-level synthesis and stakeholder consultation. First, the identified interventions could not be constructed into an overarching programme theory, so later stakeholder consultations discussed individual interventions. Second, as a consequence of the ongoing COVID-19 pandemic, the number of attendees at the stakeholder events was lower than intended. We had also planned to conduct consultation in England but struggled to recruit participants. Third, while working with pre-existing groups was valuable and ensured that participants had access to support following sessions, we did not receive much information on the identity (e.g. age, care history) and so we are not clear on the heterogeneity within these groups. Fourth, while we provided the discussion questions to all stakeholder groups, they were led by different facilitators and sessions were of different durations, meaning that there were variations in content in the consultations and not all themes were covered by each group.
Conclusion
The CHIMES review synthesised evidence on the effectiveness of interventions targeting subjective well-being, mental health, and suicide-related outcomes in care-experienced children and young people, in addition to evidence of intervention theory, key context factors, implementation and stakeholder acceptability. There was limited evidence for economic evaluations.
Overall, the evidence base is mixed, and the available evidence is primarily from the USA. There is some indication of effectiveness for skills curriculum, mentoring and parenting programmes for carers, which supports findings from a 2021 NICE review that recommended similar approaches. 51,54 There is more limited evidence for organisational and community interventions that support wraparound services, interprofessional working and culture change. Both of these were recommended as priority interventions by stakeholders.
Key context factors that might challenge the implementation of interventions in the UK, and thus need to be attended to, include lack of resources, intervention burden, interprofessional communication and relationships, care-experienced young people’s identities and carers’ identities. These factors are relevant as some priority interventions for stakeholders have been implemented in the UK to date (e.g. mentoring) but have not demonstrated effectiveness or progressed to outcome evaluation due to implementation and acceptability issues. Further development, optimisation and adaptation work is required to support delivery of these approaches in this context, with key methodological guidance having the potential to support a robust approach.
Additional information
CRediT contribution statement
Rhiannon Evans: Conceptualisation; Methodology; Formal analysis; Investigation; Writing – original draft; Writing – review and editing; Visualisation; Project administration; Funding acquisition.
Sarah MacDonald: Formal analysis; Investigation; Writing – original draft; Writing – review and editing; Visualisation; Project administration; Funding acquisition.
Robert Trubey: Formal analysis; Investigation; Writing – original draft; Writing – review and editing; Visualisation; Project administration; Funding acquisition.
Jane Noyes: Conceptualisation; Methodology; Writing – review and editing; Funding acquisition.
Michael Robling: Conceptualisation; Methodology; Writing – review and editing; Funding acquisition.
Simone Willis: Formal analysis; Investigation; Writing – review and editing.
Soo Vinnicombe: Resources; Writing – review and editing; Funding acquisition; Other (co-ordination of stakeholder engagement).
Maria Boffey: Resources; Writing – review and editing; Funding acquisition; Other (co-ordination of stakeholder engagement).
Charlotte Wooders: Resources; Writing – review and editing; Funding acquisition; Other (co-ordination of stakeholder engagement).
Asmaa El-Banna: Resources.
GJ Melendez-Torres: Conceptualisation; Methodology; Formal analysis; Investigation; Writing – original draft; Writing – review and editing; Visualisation; Project administration; Funding acquisition.
Acknowledgements
The work was undertaken with institutional support from the DECIPHer research centre and Centre for Trials Research at Cardiff University, the Peninsula Technology Assessment Group (PenTAG) at the University of Exeter, Bangor University, and The Fostering Network in Wales.
CHIMES Project Advisory Group
Dr Kelly Dixon, Evidence for Policy and Practice Information and Coordination Centre (EPPI-Centre), Social Research Institute, University College London.
Professor Nicky Stanley, Connect Centre for International Research on Interpersonal Violence and Harm, University of Central Lancashire.
Chris Dunn, Voices from Care Cymru.
Henry Vaile, Improving Outcomes for Children, Welsh Government.
Sarah Austin, Improving Outcomes for Children, Welsh Government.
Dr Aideen McNaughton, Safeguarding, Public Health Wales.
Joanne Maddaford, CAMHS.
Emma Phipps-Magil, Voices from Care Cymru (replaces Chris Dunn).
Dan Oliver, foster carer advisory member, the Fostering Network in Wales.
Emma Warren, Foster Care Network.
Bernadette Coppinger, foster carer.
Stakeholder Consultation Facilitators and Groups
Rachael Vaughan, CASCADE, Cardiff University.
Public Health Wales NHS Wales National Safeguarding Network.
The Fostering Network in Wales.
Voices from Care Cymru.
What Works Centre for Children’s Social Care.
Welsh Government Social Services and Integration Directorate.
Welsh Medical Group
Academic and Methodological Guidance
Dr Patty Leijten, University of Amsterdam advised on categorisation of outcome domains and outcome synthesis.
Dr Helen Morgan (systematic reviewer) advised on conception of the search strategy and conducting of the searches for study report.
CHIMES Administration and Review Support
Lindsey Allan, DECIPHer, Cardiff University.
Clare Olsen, DECIPHer, Cardiff University.
Payton Ramsey, Fulbright Scholar, Cardiff University.
Rohen Renold, DECIPHer, Cardiff University.
Lorna Stabler, CASCADE, Cardiff University.
Data-sharing statement
All data requests should be submitted to the corresponding author for consideration. Access to available anonymised data may be granted following review.
Ethics statement
The CHIMES review was exempted from ethical approval by the Cardiff University School of Social Sciences Research Ethics Committee because consultation data were not collected at primary, individual level.
Information governance statement
Cardiff University is committed to handling all personal information in line with the UK Data Protection Act (2018) and the General Data Protection Regulation (EU GDPR) 2016/679. Under the Data Protection legislation, Cardiff University is the Data Controller, and you can find out more about how we handle personal data, including how to exercise your individual rights and the contact details for our Data Protection Officer here: www.cardiff.ac.uk/public-information/policies-and-procedures/data-protection.
Disclosure of interests
Full disclosure of interests: Completed ICMJE forms for all authors, including all related interests, are available in the toolkit on the NIHR Journals Library report publication page at https://doi.org/10.3310/MKYP6299.
Primary conflicts of interest: Professor GJ Melendez-Torres reports membership of NIHR funding committee, specifically Programme Grants for Applied Research Subcommittee. Professor Jane Noyes reports membership of the Dissemination Centre Advisory Group (1 January 2015–31 December 2019) and COVID-19 Reviewing (1 June 2020–30 September 2020).
Disclaimers
This article presents independent research funded by the National Institute for Health and Care Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, the PHR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, the PHR programme or the Department of Health and Social Care.
References
- United Nations . Guidelines for the Alternative Care of Children 2010.
- Mannay D, Evans R, Staples E, Hallett S, Roberts L, Rees A, et al. The consequences of being labelled ‘looked-after’: exploring the educational experiences of looked-after children and young people in Wales. Br Educ Res J 2017;43:683-99. https://doi.org/10.1002/berj.3283.
- NSPCC . Looked After Children 2023. https://learning.nspcc.org.uk/children-and-families-at-risk/looked-after-children (accessed 12 March 2024).
- Stein M. Supporting young people from care to adulthood: international practice. Child Fam Soc Work 2019;24:400-5. https://doi.org/10.1111/cfs.12473.
- Office for National Statistics . Children Looked After in England Including Adoptions: Reporting Year 2021 n.d. https://explore-education-statistics.service.gov.uk/find-statistics/children-looked-after-in-england-including-adoptions/2021 (accessed 12 March 2024).
- StatsWales . Children Looked After at 31 March by Local Authority, Gender and Age 2021. https://statswales.gov.wales/Catalogue/Health-and-Social-Care/Social-Services/Childrens-Services/Children-Looked-After/childrenlookedafterat31march-by-localauthority-gender-age (accessed 12 March 2024).
- Engler AD, Sarpong KO, Van Horne BS, Greeley CS, Keefe RJ. A systematic review of mental health disorders of children in foster care. Trauma Violence Abuse 2022;23:255-64. https://doi.org/10.1177/1524838020941197.
- Bronsard G, Alessandrini M, Fond G, Loundou A, Auquier P, Tordjman S, et al. The prevalence of mental disorders among children and adolescents in the child welfare system: a systematic review and meta-analysis. Medicine (Baltimore) 2016;95. https://doi.org/10.1097/MD.0000000000002622.
- Ford T, Vostanis P, Meltzer H, Goodman R. Psychiatric disorder among British children looked after by local authorities: comparison with children living in private households. Br J Psychiatry 2018;190:319-25. https://doi.org/10.1192/bjp.bp.106.025023.
- Long SJ, Evans RE, Fletcher A, Hewitt G, Murphy S, Young H, et al. Comparison of substance use, subjective well-being and interpersonal relationships among young people in foster care and private households: a cross sectional analysis of the School Health Research Network survey in Wales. BMJ Open 2017;7. https://doi.org/10.1136/bmjopen-2016-014198.
- Evans R, White J, Turley R, Slater T, Morgan H, Strange H, et al. Comparison of suicidal ideation, suicide attempt and suicide in children and young people in care and non-care populations: systematic review and meta-analysis of prevalence. Child Youth Serv Rev 2017;82:122-9.
- Jones R, Everson-Hock ES, Papaioannou D, Guillaume L, Goyder E, Chilcott J, et al. Factors associated with outcomes for looked-after children and young people: a correlates review of the literature. Child Care Health Dev 2011;37:613-22. https://doi.org/10.1111/j.1365-2214.2011.01226.x.
- O’Higgins A, Sebba J, Gardner F. What are the factors associated with educational achievement for children in kinship or foster care: a systematic review. Child Youth Serv Rev 2017;79:198-220. https://doi.org/10.1016/j.childyouth.2017.06.004.
- Tessier NG, O’Higgins A, Flynn RJ. Neglect, educational success, and young people in out-of-home care: cross-sectional and longitudinal analyses. Child Abuse Negl 2018;75:115-29. https://doi.org/10.1016/j.chiabu.2017.06.005.
- Murray ET, Lacey R, Maughan B, Sacker A. Association of childhood out-of-home care status with all-cause mortality up to 42-years later: Office of National Statistics Longitudinal Study. BMC Public Health 2020;20:1-10. https://doi.org/10.1186/s12889-020-08867-3.
- James S. Why do foster care placements disrupt? An investigation of reasons for placement change in foster care. Soc Serv Rev 2004;78:601-27. https://doi.org/10.1086/424546.
- Rubin DM, Alessandrini EA, Feudtner C, Mandell DS, Localio AR, Hadley T. Placement stability and mental health costs for children in foster care. Pediatrics 2004;113:1336-41. https://doi.org/10.1542/peds.113.5.1336.
- Rock S, Michelson D, Thomson S, Day C. Understanding foster placement instability for looked after children: a systematic review and narrative synthesis of quantitative and qualitative evidence. Br J Soc Work 2015;45:177-203.
- Holmes L. Children’s Social Care Cost Pressures and Variations in Unit Costs 2021. www.gov.uk/government/publications/childrens-social-care-cost-pressures-and-variation-in-unit-costs (accessed 12 March 2024).
- Department for Education . Promoting the Health and Well-Being of Looked-After Children. Statutory Guidance for Local Authorities, Clinical Commissioning Groups and NHS England 2015.
- National Institute for Health and Care Excellence . Looked-After Children and Young People 2021. www.nice.org.uk/guidance/ng205 (accessed 12 March 2024).
- House of Commons Education Committee . Mental Health and Well-Being of Looked-After Children. Fourth Report of Session 2015–16 2016.
- McKeough A, Bear K, Jones C, Thompson D, Kelly PJ, Campbell LE. Foster carer stress and satisfaction: an investigation of organisational, psychological and placement factors. Child Youth Serv Rev 2017;76:10-9. https://doi.org/10.1016/j.childyouth.2017.02.002.
- Taussig HN, Culhane SE. Impact of a mentoring and skills group program on mental health outcomes for maltreated children in foster care mentoring/skills group program and foster care. JAMA Pediatr 2010;164:739-46. https://doi.org/10.1001/archpediatrics.2010.124.
- Taussig H, Weiler L, Rhodes T, Hambrick E, Wertheimer R, Fireman O, et al. Fostering healthy futures for teens: adaptation of an evidence-based program. J Soc Social Work Res 2015;6:617-42. https://doi.org/10.1086/684021.
- Taussig HN, Culhane SE. Impact of a mentoring and skills group program on mental health outcomes for maltreated children in foster care. Arch Pediatr Adolesc Med 2010;164:739-46. https://doi.org/10.1001/archpediatrics.2010.124.
- Mezey G, Meyer D, Robinson F, Bonell C, Campbell R, Gillard S, et al. Developing and piloting a peer mentoring intervention to reduce teenage pregnancy in looked-after children and care leavers: an exploratory randomised controlled trial. Health Technol Assess 2015;19:1-509, v. https://doi.org/10.3310/hta19850.
- Price JM, Chamberlain P, Landsverk J, Reid J. KEEP foster-parent training intervention: model description and effectiveness. Child Fam Soc Work 2009;14:233-42. http://dx.doi.org/10.1111/j.1365-2206.2009.00627.x.
- Price JM, Roesch S, Burce Cleo M. The effects of the KEEP foster parent training intervention on child externalizing and internalizing problems. Dev Child Welf 2019;1:5-21. https://doi.org/10.1177/2516103218812092.
- Chamberlain P. The Oregon multidimensional treatment foster care model: features, outcomes, and progress in dissemination. Cogn Behav Pract 2003;10:303-12. https://doi.org/10.1016/S1077-7229%2803%2980048-2.
- Green JM, Biehal N, Roberts C, Dixon J, Kay C, Parry E, et al. Multidimensional treatment foster care for adolescents in English care: randomised trial and observational cohort evaluation. Br J Psychiatry 2014;204:214-21. https://doi.org/10.1192/bjp.bp.113.131466.
- Lang JM, Campbell K, Shanley P, Crusto CA, Connell CM. Building capacity for trauma-informed care in the child welfare system: initial results of a statewide implementation. Child Maltreat 2016;21:113-24. https://doi.org/10.1177/1077559516635273.
- Messer EP, Greiner MV, Beal SJ, Eismann EA, Cassedy A, Gurwitch RH, et al. Child adult relationship enhancement (CARE): a brief, skills-building training for foster caregivers to increase positive parenting practices. Child Youth Serv Rev 2018;90:74-82. https://doi.org/10.1016/j.childyouth.2018.05.017.
- Murphy K, Moore Kristin A, Redd Z, Malm K. Trauma-informed child welfare systems and children’s well-being: a longitudinal evaluation of KVC’s bridging the way home initiative. Child Youth Serv Rev 2017;75:23-34. https://doi.org/10.1016/j.childyouth.2017.02.008.
- Lipscomb ST, Pratt ME, Schmitt SA, Pears KC, Kim HK. School readiness in children living in non-parental care: impacts of head start. J Appl Dev Psychol 2013;34:28-37. https://doi.org/10.1016/j.appdev.2012.09.001.
- Luke N, Sinclair I, Woolgar M, Sebba J. London: NSPCC; 2014.
- Turner W, Macdonald G. Treatment foster care for improving outcomes in children and young people: a systematic review. Res Soc Work Pract 2011;21:501-27.
- Everson-Hock ES, Jones R, Guillaume L, Clapton J, Goyder E, Chilcott J, et al. The effectiveness of training and support for carers and other professionals on the physical and emotional health and well-being of looked-after children and young people: a systematic review. Child Care Health Dev 2012;38:162-74. https://doi.org/10.1111/j.1365-2214.2011.01247.x.
- Hambrick EP, Oppenheim-Weller S, N’Zi AM, Taussig HN. Mental health interventions for children in foster care: a systematic review. Child Youth Serv Rev 2016;70:65-77. https://doi.org/10.1016/j.childyouth.2016.09.002.
- Everson-Hock ES, Jones R, Guillaume L, Clapton J, Duenas A, Goyder E, et al. Supporting the transition of looked-after young people to independent living: a systematic review of interventions and adult outcomes. Child Care Health Dev 2011;37:767-79. https://doi.org/10.1111/j.1365-2214.2011.01287.x.
- Kerr L, Cossar J. Attachment interventions with foster and adoptive parents: a systematic review. Child Abuse Rev 2014;23:426-39. https://doi.org/10.1002/car.2313.
- O’Higgins A, Ott EM, Shea MW. What is the impact of placement type on educational and health outcomes of unaccompanied refugee minors? A systematic review of the evidence. Clin Child Fam Psychol Rev 2018;21:354-65. https://doi.org/10.1007/s10567-018-0256-7.
- Marsh D. A Systematic Review and Meta-Analysis of Randomized Clinical Trials of Evidence-Based Practices Through Measured Change of Behavior for Children in Foster Care. Chicago, IL: Chicago School of Professional Psychology; 2017.
- Solomon DT, Niec LN, Schoonover CE. The impact of foster parent training on parenting skills and child disruptive behavior. Child Maltreat 2017;22:3-13. https://doi.org/10.1177/1077559516679514.
- Sullivan AL, Simonson GR. A systematic review of school-based social-emotional interventions for refugee and war-traumatized youth. Rev Educ Res 2016;86:503-30. http://dx.doi.org/10.3102/0034654315609419.
- Macdonald GM, Turner W. Treatment foster care for improving outcomes in children and young people. Cochrane Database Syst Rev 2008;2008. https://doi.org/10.1002/14651858.CD005649.pub2.
- Dickson K, Sutcliffe K, Gough D, Statham J. Improving the Emotional and Behavioural Health of Looked-After Children and Young People (LACYP): Research Review 2. London: Centre for Excellence and Outcomes in Children and Young People’s Services; 2009.
- Bergström M, Cederblad M, Håkansson K, Jonsson AK, Munthe C, Vinnerljung B, et al. Interventions in foster family care: a systematic review. Res Soc Work Pract 2019;30:3-18. https://doi.org/10.1177/1049731519832101.
- Greeson JKP, Garcia AR, Tan F, Chacon A, Ortiz AJ. Interventions for youth aging out of foster care: a state of the science review. Child Youth Serv Rev 2020;113. https://doi.org/10.1016/j.childyouth.2020.105005.
- Barnett ER, Concepcion-Zayas MT, Zisman-Ilani Y, Bellonci C. Patient-centered psychiatric care for youth in foster care: a systematic and critical review. J Public Child Welf 2019;13:462-89. https://doi.org/10.1080/15548732.2018.1512933.
- National Institute for Health and Care Excellence . Looked-After Children and Young People: Interventions to Promote Physical, Mental, and Emotional Health and Wellbeing of Looked After Children, Young People and Care Leavers. Looked-After Children and Young People: Evidence Review F 2021. www.ncbi.nlm.nih.gov/books/NBK575878 (accessed 12 March 2024).
- Åström T, Bergström M, Håkansson K, Jonsson AK, Munthe C, Wirtberg I, et al. Treatment Foster Care Oregon for delinquent adolescents: a systematic review and meta-analysis. Res Soc Work Pract 2020;30:355-67.
- Bellamy JL, Gopalan G, Traube DE. A national study of the impact of outpatient mental health services for children in long-term foster care. Clin Child Psychol Psychiatry 2010;15:467-79. https://doi.org/10.1177/1359104510377720.
- National Institute for Health and Care Excellence . Looked-After Children and Young People. Evidence Review G. Barriers and Facilitators for Promoting Physical, Mental and Emotional Health and Wellbeing of Looked-After Children and Young People and Care Leavers. Evidence Reviews Underpinning Recommendations 1.2.14 to 1.2.17, 1.3.18, 1.4.1 to 1.4.8, 1.5.1, 1.5.9, 1.5.17 to 1.5.21, and 1.5.35 to 1.5.36 2021. www.ncbi.nlm.nih.gov/books/NBK575879 (accessed 12 March 2024).
- Petticrew M, Knai C, Thomas J, Rehfuess EA, Noyes J, Gerhardus A, et al. Implications of a complexity perspective for systematic reviews and guideline development in health decision making. BMJ Glob Health 2019;4. https://doi.org/10.1136/bmjgh-2018-000899.
- Booth A, Moore G, Flemming K, Garside R, Rollins N, Tunçalp O, et al. Taking account of context in systematic reviews and guidelines considering a complexity perspective. BMJ Glob Health 2019;4. https://doi.org/10.1136/bmjgh-2018-000840.
- Moore GF, Evans RE, Hawkins J, Littlecott H, Melendez-Torres G, Bonell C, et al. From complex social interventions to interventions in complex social systems: future directions and unresolved questions for intervention development and evaluation. Evaluation 2019;25:23-45. https://doi.org/10.1177/1356389018803219.
- Hawe P, Shiell A, Riley T. Theorising interventions as events in systems. Am J Community Psychol 2009;43:267-76. https://doi.org/10.1007/s10464-009-9229-9.
- Rutter H, Savona N, Glonti K, Bibby J, Cummins S, Finegood DT, et al. The need for a complex systems model of evidence for public health. Lancet 2017;390:2602-4. https://doi.org/10.1016/s0140-6736(17)31267-9.
- O’Cathain A, Croot L, Sworn K, Duncan E, Rousseau N, Turner K, et al. Taxonomy of approaches to developing interventions to improve health: a systematic methods overview. Pilot Feasibility Stud 2019;5:1-27. https://doi.org/10.1186/s40814-019-0425-6.
- O’Cathain A, Croot L, Duncan E, Rousseau N, Sworn K, Turner KM, et al. Guidance on how to develop complex interventions to improve health and healthcare. BMJ Open 2019;9. https://doi.org/10.1136/bmjopen-2019-029954.
- Skivington K, Matthews L, Simpson SA, Craig P, Baird J, Blazeby JM, et al. Framework for the development and evaluation of complex interventions: gap analysis, workshop and consultation-informed update. Health Technol Assess 2021;25:1-132. https://doi.org/10.3310/hta25570.
- Moore GF, Audrey S, Barker M, Bond L, Bonell C, Hardeman W, et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015;350. https://doi.org/10.1136/bmj.h1258.
- Moore G, Campbell M, Copeland L, Craig P, Movsisyan A, Hoddinott P, et al. Adapting interventions to new contexts – the ADAPT guidance. BMJ 2021;374. https://doi.org/10.1136/bmj.n1679.
- Westermark PK, Hansson K, Olsson M. Multidimensional treatment foster care (MTFC): results from an independent replication. J Fam Ther 2011;33:20-41. https://doi.org/10.1111/ j.1467-6427.2010.00515.x.
- Evans R, Boffey M, MacDonald S, Noyes J, Melendez-Torres G, Morgan HE, et al. Care-experienced cHildren and young people’s Interventions to improve Mental health and wEll-being outcomes: Systematic review (CHIMES) protocol. BMJ Open 2021;11. https://doi.org/10.1136/bmjopen-2020-042815.
- Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 2009;339. https://doi.org/10.1136/bmj.b2700.
- Evans R, MacDonald S, Trubey R, Noyes J, Robling M, Willis S, et al. Interventions targeting the mental health and wellbeing of care-experienced children and young people in higher-income countries: evidence map and systematic review. Syst Rev 2023;12:1-33. https://doi.org/10.1177/15248380241227987.
- Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med 2018;169:467-73. https://doi.org/10.7326/m18-0850.
- Tong A, Flemming K, McInnes E, Oliver S, Craig J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med Res Methodol 2012;12. https://doi.org/10.1186/1471-2288-12-181.
- Staniszewska S, Brett J, Simera I, Seers K, Mockford C, Goodlad S, et al. GRIPP2 reporting checklists: tools to improve reporting of patient and public involvement in research. BMJ 2017;358. https://doi.org/10.1136/bmj.j3453.
- Munthe-Kaas H, Nøkleby H, Lewin S, Glenton C. The TRANSFER approach for assessing the transferability of systematic review findings. BMC Med Res Methodol 2020;20. https://doi.org/10.1186/s12874-019-0834-5.
- Hong QN, Pluye P, Bujold M, Wassef M. Convergent and sequential synthesis designs: implications for conducting and reporting systematic reviews of qualitative and quantitative evidence. Syst Rev 2017;6. https://doi.org/10.1186/s13643-017-0454-2.
- Noyes J, Booth A, Moore G, Flemming K, Tunçalp O, Shakibazadeh E. Synthesising quantitative and qualitative evidence to inform guidelines on complex interventions: clarifying the purposes, designs and outlining some methods. BMJ Glob Health 2019;4. https://doi.org/10.1136/bmjgh-2018-000893.
- UNICEF . The United Nations Convention on the Rights of the Child 1989. www.journalslibrary.nihr.ac.uk/phr/phr07170 (accessed 12 March 2024).
- El-Banna A, Petrou S, Yiu HHE, Daher S, Forrester D, Scourfield J, et al. Systematic review of economic evaluations of children’s social care interventions. Child Youth Serv Rev 2021;121. https://doi.org/10.1016/j.childyouth.2020.105864.
- Ames HM, Glenton C, Lewin S. Parents’ and informal caregivers’ views and experiences of communication about routine childhood vaccination: a synthesis of qualitative evidence. Cochrane Database Syst Rev 2017;2. https://doi.org/10.1002/14651858.CD011787.pub2.
- Ames H, Glenton C, Lewin S. Purposive sampling in a qualitative evidence synthesis: a worked example from a synthesis on parental perceptions of vaccination communication. BMC Med Res Methodol 2019;19:1-9. https://doi.org/10.1186/s12874-019-0665-4.
- van Vliet P, Hunter SM, Donaldson C, Pomeroy V. Using the TIDieR checklist to standardize the description of a functional strength training intervention for the upper limb after stroke. J Neurol Phys Ther 2016;40:203-8. https://doi.org/10.1097/NPT.0000000000000133.
- Tancred T, Melendez-Torres GJ, Paparini S, Fletcher A, Stansfield C, Thomas J, et al. Public Health Research. Southampton, UK: NIHR Journals Library; n.d.
- Pfadenhauer LM, Gerhardus A, Mozygemba K, Lysdahl KB, Booth A, Hofmann B, et al. Making sense of complexity in context and implementation: the Context and Implementation of Complex Interventions (CICI) framework. Implement Sci 2017;12. https://doi.org/10.1186/s13012-017-0552-5.
- O’Neill J, Tabish H, Welch V, Petticrew M, Pottie K, Clarke M, et al. Applying an equity lens to interventions: using PROGRESS ensures consideration of socially stratifying factors to illuminate inequities in health. J Clin Epidemiol 2014;67:56-64. https://doi.org/10.1016/ j.jclinepi.2013.08.005.
- Drummond MF, Sculpher MJ, Claxton K, Stoodart GL, Torrance G. Methods for the Economic Evaluation of Health Care Programmes. USA: Oxford University Press; 2015.
- Rees R, Oliver K, Woodman J, Thomas J. The views of young children in the UK about obesity, body size, shape and weight: a systematic review. BMC Public Health 2011;11. https://doi.org/10.1186/1471-2458-11-188.
- Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane Handbook for Systematic Reviews of Interventions. Chichester (UK): John Wiley & Sons; 2019.
- Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implement Sci 2010;5. https://doi.org/10.1186/1748-5908-5-69.
- Miake-Lye IM, Hempel S, Shanman R, Shekelle PG. What is an evidence map? A systematic review of published evidence maps and their definitions, methods, and products. Syst Rev 2016;5:1-21. https://doi.org/10.1186/s13643-016-0204-x.
- Clapton J, Rutter D, Sharif N. SCIE Systematic Mapping Guidance. London: SCIE; 2009.
- Barnett-Page E, Thomas J. Methods for the synthesis of qualitative research: a critical review. BMC Med Res Methodol 2009;9. https://doi.org/10.1186/1471-2288-9-59.
- Brunton G, Oliver S, Thomas J. Innovations in framework synthesis as a systematic review method. Res Synth Methods 2020;11:316-30. https://doi.org/10.1002/jrsm.1399.
- Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol 2013;13. https://doi.org/10.1186/1471-2288-13-117.
- van Grootel L, van Wesel F, O’Mara-Eves A, Thomas J, Hox J, Boeije H. Using the realist perspective to link theory from qualitative evidence synthesis to quantitative studies: broadening the matrix approach. Res Synth Methods 2017;8:303-11. https://doi.org/10.1002/jrsm.1241.
- Munabi‐Babigumira S, Glenton C, Lewin S, Fretheim A, Nabudere H. Factors that influence the provision of intrapartum and postnatal care by skilled birth attendants in low‐and middle‐income countries: a qualitative evidence synthesis. Cochrane Database Syst Rev 2017. https://doi.org/10.1002/14651858.CD011558.pub2.
- Balshem H, Helfand M, Schunemann HJ, Oxman AD, Kunz R, Brozek J, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol 2011;64:401-6. https://doi.org/10.1016/j.jclinepi.2010.07.015.
- Guyatt GH, Oxman AD, Vist G, Kunz R, Brozek J, Alonso-Coello P, et al. GRADE guidelines: 4. Rating the quality of evidence–study limitations (risk of bias). J Clin Epidemiol 2011;64:407-15. https://doi.org/10.1016/j.jclinepi.2010.07.017.
- Lewin S, Bohren M, Rashidian A, Munthe-Kaas H, Glenton C, Colvin CJ, et al. Applying GRADE-CERQual to qualitative evidence synthesis findings – paper 2: how to make an overall CERQual assessment of confidence and create a summary of qualitative findings table. Implement Sci 2018;13. https://doi.org/10.1186/s13012-017-0689-2.
- Ryan R, Hill S. How to GRADE the Quality of the Evidence. Version 3.0. Melbourne: La Troube; 2016.
- Skivington K, Matthews L, Simpson SA, Craig P, Baird J, Blazeby JM, et al. A new framework for developing and evaluating complex interventions: update of Medical Research Council guidance. BMJ 2021;374. https://doi.org/10.1136/bmj.n2061.
- Moore G, Audrey S, Barker M, Bond L, Bonnell C, Hardeman W. Process Evaluation of Complex Interventions: Medical Research Council Guidance. London: MRC Population Health Science Research Network; 2014.
- Bachi K, Terkel J, Teichman M. Equine-facilitated psychotherapy for at-risk adolescents: the influence on self-image, self-control and trust. Clin Child Psychol Psychiatry 2012;17:298-312. https://doi.org/10.1177/1359104511404177.
- Chamberlain P, Leve LD, Smith DK. Preventing behavior problems and health-risking behaviors in girls in foster care. Int J Behav Consult Ther 2006;2:518-30. https://doi.org/10.1037/h0101004.
- Chamberlain P, Roberts R, Jones H, Marsenich L, Sosna T, Price Joseph M. Three collaborative models for scaling up evidence-based practices. Adm Policy Ment Health 2012;39:278-90. https://doi.org/10.1007/s10488-011-0349-9.
- DeGarmo DS, Reid JB, Fetrow BA, Fisher PA, Antoine KD. Preventing child behavior problems and substance use: the pathways home foster care reunification intervention. J Child Adolesc Subst Abuse 2013;22:388-406. https://doi.org/10.1080/1067828X.2013.788884.
- Farmer EMZ, Lippold MA. The need to do it all: exploring the ways in which treatment foster parents enact their complex role. Child Youth Serv Rev 2016;64:91-9. https://doi.org/10.1016/j.childyouth.2016.03.005.
- Fisher PA, Ellis BH, Chamberlain P. Early intervention foster care: a model for preventing risk in young children who have been maltreated. Child Serv 1999;2:159-82. https://doi.org/10.1207/s15326918cs0203_3.
- James S, Meezan W. Refining the evaluation of treatment foster care. Fam Soc J Contemp Hum Serv 2002;83:233-44. https://doi.org/10.1606/1044-3894.24.
- Leve LD, Fisher PA, Chamberlain P. Multidimensional treatment foster care as a preventive intervention to promote resiliency among youth in the child welfare system. J Pers 2009;77:1869-902. https://doi.org/10.1111/j.1467-6494.2009.00603.x.
- Nilsen W. Fostering futures: a preventive intervention program for school-age children in foster care. Clin Child Psychol Psychiatry 2007;12:45-63. https://doi.org/10.1177/135910450 7071055.
- Pithouse A, Hill-Tout J, Lowe K. Training foster carers in challenging behaviour: a case study in disappointment?. Child Fam Soc Work 2002;7:203-14. https://doi.org/10.1046/j.1365-2206.2002.00249.x.
- Southerland DG, Mustillo SA, Farmer EMZ, Stambaugh LF, Murray M. What’s the relationship got to do with it? Understanding the therapeutic relationship in therapeutic foster care. Child Adolesc Soc Work J 2009;26:49-63. https://doi.org/10.1007/s10560-008-0159-4.
- Taussig HN, Culhane SE, Garrido E, Knudtson MD, Petrenko CLM. Does severity of physical neglect moderate the impact of an efficacious preventive intervention for maltreated children in foster care?. Child Maltreat 2013;18:56-64. https://doi.org/10.1177/1077559512461397.
- Taussig HN, Culhane SE, Hettleman D. Fostering healthy futures: an innovative preventive intervention for preadolescent youth in out-of-home care. Child Welfare 2007;86:113-31.
- Van Holen F, Vanschoonlandt F, Vanderfaeillie J. Evaluation of a foster parent intervention for foster children with externalizing problem behaviour. Child Fam Soc Work 2017;22:1216-26. https://doi.org/10.1111/cfs.12338.
- Vanschoonlandt F, Vanderfaeillie J, Van Holen F, De Maeyer S. Development of an intervention for foster parents of young foster children with externalizing behavior: theoretical basis and program description. Clin Child Fam Psychol Rev 2012;15:330-44. https://doi.org/10.1007/s10567-012-0123-x.
- Weiler LM, Lee SK, Zhang J, Ausherbauer K, Schwartz Sarah EO, Kanchewa Stella S, et al. Mentoring children in foster care: examining relationship histories as moderators of intervention impact on children’s mental health and trauma symptoms. Am J Community Psychol 2021;69:100-13. https://doi.org/10.1002/ajcp.12549.
- Weiler LM, Taussig HN. The moderating effect of risk exposure on an efficacious intervention for maltreated children. J Clin Child Adolesc Psychol 2019;48:S194-201. https://doi.org/10.1080/15374416.2017.1295379.
- Chamberlain P, Price J, Leve LD, Laurent H, Landsverk JA, Reid JB. Prevention of behavior problems for children in foster care: outcomes and mediation effects. Prev Sci 2008;9:17-2. https://doi.org/10.1007/s11121-007-0080-7.
- Alderson H, Kaner E, Brown R, Howel D, McColl E, Smart D, et al. Behaviour change interventions to reduce risky substance use and improve mental health in children in care: the SOLID three-arm feasibility RCT. Public Health Res 2020;8:1-162. https://doi.org/10.3310/phr08130.
- Izzo Charles V, Smith EG, Sellers DE, Holden MJ, Nunna MA. Improving relationship quality in group care settings: the impact of implementing the CARE model. Child Youth Serv Rev 2020;109. https://doi.org/10.1016/j.childyouth.2019.104623.
- Aventin A, Houston S, Macdonald G. Utilising a computer game as a therapeutic intervention for youth in residential care: some preliminary findings on use and acceptability. Child Youth Serv Rev 2014;47:362-9. https://doi.org/10.1016/j.childyouth.2014.10.012.
- Baginsky M. The New Orleans Intervention Model: Early Implementation in a London Borough Evaluation Report 2017. https://assets.publishing.service.gov.uk/media/5a82b9ffe5274a2e87dc2acf/New_Orleans_intervention-model.pdf (accessed 12 March 2024).
- Biehal N, Dixon J, Parry E, Sinclair I, Green J, Roberts C, et al. The Care Placements Evaluation (CaPE) evaluation of Multidimensional Treatment Foster Care for Adolescents (MTFC-A) 2012;8. https://dera.ioe.ac.uk/id/eprint/13829/ (accessed 12 March 2024).
- Blair K, Topitzes J, Mersky JP. Brief, group-based parent-child interaction therapy: examination of treatment attrition, non-adherence, and non-response. Child Youth Serv Rev 2019;106. https://doi.org/10.1016/j.childyouth.2019.104463.
- Brown CH, Chamberlain P, Saldana L, Padgett C, Wang W, Cruden G. Evaluation of two implementation strategies in 51 child county public service systems in two states: results of a cluster randomized head-to-head implementation trial. Implement Sci 2014;9. https://doi.org/10.1186/s13012-014-0134-8.
- Buchanan R, Chamberlain P, Price JM, Sprengelmeyer P. Examining the equivalence of fidelity over two generations of KEEP implementation: a preliminary analysis. Child Youth Serv Rev 2013;35:188-93. https://doi.org/10.1016/j.childyouth.2012.10.002.
- Callaghan J, Young B, Richards M, Vostanis P. Developing new mental health services for looked after children: a focus group study. Adopt Foster 2003;27:51-63. https://doi.org/10.1177/030857590302700408.
- Chamberlain P, Price J, Reid J, Landsverk J. Cascading implementation of a foster and kinship parent intervention. Child Welfare 2008;87:27-48.
- Conn AM, Szilagyi MA, Alpert-Gillis L, Webster-Stratton C, Manly JT, Goldstein N, et al. Pilot randomized controlled trial of foster parent training: a mixed-methods evaluation of parent and child outcomes. Child Youth Serv Rev 2018;89:188-97. https://doi.org/10.1016/ j.childyouth.2018.04.035.
- Dorsey S, Conover KL, Revillion C. Improving foster parent engagement: using qualitative methods to guide tailoring of evidence-based engagement strategies. J Clin Child Adolesc Psychol 2014;43:877-89. https://doi.org/10.1080/15374416.2013.876643.
- Furlong M, McLoughlin F, McGilloway S. The incredible years parenting program for foster carers and biological parents of children in foster care: a mixed methods study. Child Youth Serv Rev 2021;126. https://doi.org/10.1016/j.childyouth.2021.106028.
- Haight W, Black J, Sheridan K. A mental health intervention for rural, foster children from methamphetamine-involved families: experimental assessment with qualitative elaboration. Child Youth Serv Rev 2010;32:1446-57. https://doi.org/10.1016/j.childyouth. 2010.06.024.
- Hall SF, Semanchin JA. Implementation of intensive permanence services: a trauma-informed approach to preparing foster youth for supportive relationships. Child Adolesc Soc Work J 2018;35:587-98. https://doi.org/10.1007/s10560-018-0550-8.
- Hutchings J, Bywater T. Delivering the incredible years parent programme to foster carers in Wales: reflections from group leader supervision. Adopt Foster 2013;37:28-42. https://doi.org/10.1177/0308575913477075.
- Briskman J, Castle J, Blackeby K, Bengo C, Slack K, Stebbens C, et al. Randomised Controlled Trial of the Fostering Changes Programme. London: King’s College London; 2012.
- Jee SH, Couderc JP, Swanson D, Gallegos A, Hilliard C, Blumkin A, et al. A pilot randomized trial teaching mindfulness-based stress reduction to traumatized youth in foster care. Complement Ther Clin Pract 2015;21:201-9. https://doi.org/10.1016/j.ctcp.2015.06.007.
- Kirton D, Thomas C. A suitable case? Implementing multidimensional treatment foster care in an English local authority. Adopt Foster 2011;35:5-17. https://doi.org/10.1177/030857591103500202.
- Lee BR, Phillips DR, Steward RK, Kerns SEU. Equipping TFC parents as treatment providers: findings from expert interviews. J Child Fam Stud 2021;30:870-80. https://doi.org/10.1007/s10826-020-01808-z.
- Lotty M, Bantry-White E, Dunn-Galvin A. The experiences of foster carers and facilitators of fostering connections: the trauma-informed foster care program: a process study. Child Youth Serv Rev 2020;119. https://doi.org/10.1016/j.childyouth.2020.105516.
- McDermid S, Trivedi H, Holmes L, Boddy J. Foster carers’ receptiveness to new innovations and programmes: an example from the introduction of social pedagogy to UK foster care. The Br J Soc Work 2021;52:1213-30. https://doi.org/10.1093/bjsw/bcab152.
- Midgley N, Besser SJ, Fearon P, Wyatt S, Byford S, Wellsted D. The Herts and Minds study: feasibility of a randomised controlled trial of mentalization-based treatment versus usual care to support the wellbeing of children in foster care. BMC Psychiatry 2019;19. https://doi.org/10.1186/s12888-019-2196-2.
- Murray M, Culver T, Farmer E, Jackson Leslie A, Rixon B. From theory to practice: one agency’s experience with implementing an evidence-based model. J Child Fam Stud 2014;23:844-53. https://doi.org/10.1007/s10826-013-9738-x.
- Reddy SD, Negi LT, Dodson-Lavelle B, Ozawa-de SB, Pace TWW, Cole SP, et al. Cognitive-based compassion training: a promising prevention strategy for at-risk adolescents. J Child Fam Stud 2013;22:219-30. https://doi.org/10.1007/s10826-012-9571-7.
- Schuurmans AAT, Nijhof KS, Rutger CMEE, Granic I. Using a videogame intervention to reduce anxiety and externalizing problems among youths in residential care: an initial randomized controlled trial. J Psychopathol Behav Assess 2018;40:344-54. https://doi.org/10.1007/s10862-017-9638-2.
- Silva IS, Gaspar MFF, Anglin JP. Webster-Stratton incredible years basic parent programme (IY) in child care placements: residential staff carers’ satisfaction results. Child Fam Soc Work 2016;21:198-20. https://doi.org/10.1111/cfs.12129.
- Spencer R, Drew Alison L, Gowdy G, Horn John P. ‘A positive guiding hand’: a qualitative examination of youth-initiated mentoring and the promotion of interdependence among foster care youth. Child Youth Serv Rev 2018;93:41-50. https://doi.org/10.1016/j.childyouth. 2018.06.038.
- Spielfogel Jill E, Leathers Sonya J, Christian E, McMeel Lorri S. Parent management training, relationships with agency staff, and child mental health: urban foster parents’ perspectives. Child Youth Serv Rev 2011;33:2366-74. https://doi.org/10.1016/j.childyouth.2011.08.008.
- Taussig HN, Weiler LM, Garrido EF, Rhodes T, Boat A, Fadell M. A positive youth development approach to improving mental health outcomes for maltreated children in foster care: replication and extension of an RCT of the fostering healthy futures program. Am J Community Psychol 2019;64:405-17. https://doi.org/10.1002/ajcp.12385.
- Triantafillou N. Solution-Focused Parent Groups: A New Approach to the Treatment of Youth Disruptive Behavioural Difficulties 2002.
- Turner-Halliday F, Kainth G, Young-Southward G, Cotmore R, Watson N, McMahon L, et al. Clout or doubt? Perspectives on an infant mental health service for young children placed in foster care due to abuse and neglect. Child Abuse Negl 2017;72:184-95. https://doi.org/10.1016/j.chiabu.2017.07.012.
- Turner-Halliday F, Watson N, Minnis H. London: NSPCC; 2016.
- Vallejos EP, Ball MJ, Brown P, Crepaz-Keay D, Haslam-Jones E, Crawford P. Kundalini yoga as mutual recovery: a feasibility study including children in care and their carers. J Child Serv 2016;11:261-82. https://doi.org/10.1108/JCS-11-2015-0034.
- Walsh NE. Participant Engagement in a Foster Parent Training Intervention 2016.
- Ziviani J, Darlington Y, Feeney R, Meredith P, Head B. Children with disabilities in out-of-home care: perspectives on organisational collaborations. Child Youth Serv Rev 2013;35:797-805. https://doi.org/10.1016/j.childyouth.2013.02.003.
- Alderson H, Kaner E, McColl E, Howel D, Fouweather T, McGovern R, et al. A pilot feasibility randomised controlled trial of two behaviour change interventions compared to usual care to reduce substance misuse in looked after children and care leavers aged 12-20 years: the SOLID study. PLOS ONE 2020;15. https://doi.org/10.1371/journal.pone. 0238286.
- Alderson H, McGovern R, Copello A, McColl E, Kaner E, Smart D, et al. Implementation factors for the delivery of alcohol and drug interventions to children in care: qualitative findings from the SOLID feasibility trial. Int J Environ Res Public Health 2021;18. https://doi.org/10.3390/ijerph18073461.
- Shklarski L. Understanding individual and organizational factors related to the implementation fidelity of the family finding intervention to support youth in foster care who are transitioning to independent living. Child Welfare 2020;98:103-36. https://www.jstor.org/stable/48623690 (accessed 15 October 2024).
- Job AK, Ehrenberg D, Hilpert P, Reindl V, Lohaus A, Konrad K, et al. Taking care triple P for foster parents with young children in foster care: results of a 1-year randomized trial. J Interpers Violence 2022;37:322-48. https://doi.org/10.1177/0886260520909196.
- Dorsey S, Pullmann MD, Berliner L, Koschmann E, McKay M, Deblinger E. Engaging foster parents in treatment: a randomized trial of supplementing trauma-focused cognitive behavioral therapy with evidence-based engagement strategies. Child Abuse Negl 2014;38:1508-20. https://doi.org/10.1016/j.chiabu.2014.03.020.
- Geenen S, Powers Laurie E, Powers J, Cunningham M, McMahon L, Nelson M, et al. Experimental study of a self-determination intervention for youth in foster care. Career Dev Transit Except Individ 2012;36:84-95. https://doi.org/10.1177/2165143412455431.
- Leathers SJ, Spielfogel JE, McMeel LS, Atkins MS. Use of a parent management training intervention with urban foster parents: a pilot study. Child Youth Serv Rev 2011;33:1270-9. https://doi.org/10.1016/j.childyouth.2011.02.022.
- Tullberg E, Vaughon W, Muradwij N, Kerker BD. Unpacking ‘support’: understanding the complex needs of therapeutic foster parents. Child Youth Serv Rev 2019;105. https://doi.org/10.1016/j.childyouth.2019.104420.
- Pasalich DS, Moretti MM, Hassall A, Curcio A. Pilot randomized controlled trial of an attachment- and trauma-focused intervention for kinship caregivers. Child Abuse Negl 2021;120. https://doi.org/10.1016/j.chiabu.2021.105178.
- Maaskant AM, van Rooij FB, Overbeek GJ, Oort FJ, Hermanns JMA. Parent training in foster families with children with behavior problems: follow-up results from a randomized controlled trial. Child Youth Serv Rev 2016;70:84-9. https://doi.org/10.1016/ j.childyouth.2016.09.005.
- McMillen JC, Narendorf SC, Robinson D, Havlicek J, Fedoravicius N, Bertram J, et al. Development and piloting of a treatment foster care program for older youth with psychiatric problems. Child Adolesc Psychiatry Mental Health 2015;9. https://doi.org/10.1186/s13034-015-0057-4.
- Adkins T, Reisz S, Hasdemir D, Fonagy P. Family minds: a randomized controlled trial of a group intervention to improve foster parents’ reflective functioning. Dev Psychopathol 2021;34:1177-91. https://doi.org/10.1017/S095457942000214X.
- Akin BA, Lang K, Yan YQ, McDonald TP. Randomized trial of PMTO in foster care: 12-month child well-being, parenting, and caregiver functioning outcomes. Child Youth Serv Rev 2018;95:49-63. https://doi.org/10.1016/j.childyouth.2018.10.018.
- Akin BA, Lang K, McDonald Thomas P, Yan Y, Little T. Randomized trial of PMTO in foster care: six-month child well-being outcomes. Res Soc Work Pract 2019;29:206-22. https://doi.org/10.1177/1049731516669822.
- Betzalel N, Shechtman Z. Bibliotherapy treatment for children with adjustment difficulties: a comparison of affective and cognitive bibliotherapy. J Creat Mental Health 2010;5:426-39. https://doi.org/10.1080/15401383.2010.527816.
- Bittman B, Dickson L, Coddington K. Creative musical expression as a catalyst for quality-of-life improvement in inner-city adolescents placed in a court-referred residential treatment program. Adv Mind Body Med 2009;24:8-19.
- Clark HB, Prange ME, Lee B, Boyd LA, McDonald BA, Stewart ES. Improving adjustment outcomes for foster children with emotional and behavioral disorders: early findings from a controlled study on individualized services. J Emot Behav Disord 1994;2:207-18. https://doi.org/10.1177/106342669400200403.
- Dozier M, Peloso E, Lindhiem O, Gordon MK, Manni M, Sepulveda S, et al. Developing evidence-based interventions for foster children: an example of a randomized clinical trial with infants and toddlers. J Soc Issues 2006;62:767-85. https://doi.org/10.1111/j.1540-4560. 2006.00486.x.
- Farmer EMZ, Burns BJ, Wagner HR, Murray M, Southerland DG. Enhancing ‘usual practice’ treatment foster care: findings from a randomized trial on improving youths’ outcomes. Psychiatr Serv 2010;61:555-61. https://doi.org/10.1176/ps.2010.61.6.555.
- Jonkman CS, Schuengel C, Oosterman M, Lindeboom R, Boer F, Lindauer RJL. Effects of Multidimensional Treatment Foster Care for Preschoolers (MTFC-P) for young foster children with severe behavioral disturbances. J Child Fam Stud 2017;26:1491-503. https://doi.org/10.1007/s10826-017-0661-4.
- Linares LO, Montalto D, Li M, Oza VS. A promising parenting intervention in foster care. J Consult Clin Psychol 2006;74:32-41. https://doi.org/10.1037/0022-006X.74.1.32.
- Maaskant AM, van Rooij FB, Overbeek GJ, Oort FJ, Arntz M, . Effects of PMTO in foster families with children with behavior problems: a randomized controlled trial. J Child Fam Stud 2017;26:523-39. https://doi.org/10.1007/s10826-016-0579-2.
- Marquis R. The Gender Effects of a Foster Parent-Delivered Tutoring Program on Foster Children’s Academic Skills and Mental Health: A Randomized Field Trial 2014.
- Mersky JP, Topitzes J, Grant-Savela SD, Brondino MJ, McNeil CB. Adapting parent-child interaction therapy to foster care: outcomes from a randomized trial. Res Soc Work Pract 2016;26:157-67. https://doi.org/10.1177/1049731514543023.
- Minnis H, Pelosi AJ, Knapp M, Dunn J. Mental health and foster carer training. Arch Dis Child 2001;84:302-6. https://doi.org/10.1136/adc.84.4.302.
- Moody G, Coulman E, Brookes-Howell L, Cannings-John R, Channon S, Lau M, et al. A pragmatic randomised controlled trial of the fostering changes programme. Child Abuse Negl 2020;108. https://doi.org/10.1016/j.chiabu.2020.104646.
- N’Zi A, Stevens ML, Eyberg SM. Child directed interaction training for young children in kinship care: a pilot study. Child Abuse Negl 2016;55:81-9. https://doi.org/10.1016/ j.chiabu.2016.03.001.
- Oxford ML, Marcenko M, Fleming CB, Lohr MJ, Spieker SJ. Promoting birth parents’ relationships with their toddlers upon reunification: results from promoting first relationships home visiting program. Child Youth Serv Rev 2016;61:109-16. https://doi.org/10.1016/j.childyouth.2015.12.004.
- Price JM, Roesch S, Walsh NE, Landsverk J. Effects of the KEEP foster parent intervention on child and sibling behavior problems and parental stress during a randomized implementation trial. Prev Sci 2015;16:685-95. https://doi.org/10.1007/s11121-014-0532-9.
- Smith DK, Leve LD, Chamberlain P. Preventing internalizing and externalizing problems in girls in foster care as they enter middle school: impact of an intervention. Prev Sci 2011;12:269-77. https://doi.org/10.1007/s11121-011-0211-z.
- Sprang G. The efficacy of a relational treatment for maltreated children and their families. Child Adoles Mental Health 2009;14:81-8. https://doi.org/10.1111/j.1475-3588.2008.00499.x.
- Van Holen F, Vanderfaeillie J, Omer H, Vanschoonlandt F. Training in nonviolent resistance for foster parents: a randomized controlled trial. Res Soc Work Pract 2018;28:931-42. https://doi.org/10.1177/1049731516662915.
- Vandivere S, Malm KE, Allen TJ, Williams SC, McKlindon A. A randomized controlled trial of family finding: a relative search and engagement intervention for youth lingering in foster care. Eval Rev 2017;41:542-67. https://doi.org/10.1177/0193841X17689971.
- Bellamy J. Mental Health Services for Vulnerable Children and Young People: Supporting Children Who Are, or Have Been, in Foster Care. London: Routledge; 2013.
- Bronz KD. Effects of a therapeutic playgroup intervention on the social competence and executive functioning of young children in foster care. Diss Abstr Int A Humanit Soc Sci 2004;65.
- Greeno EJ, Lee BR, Uretsky MC, Moore JE, Barth RP, Shaw TV. Effects of a foster parent training intervention on child behavior, caregiver stress, and parenting style. J Child Fam Stud 2016;25:1991-2000. https://doi.org/10.1007/s10826-015-0357-6.
- Hayduk I. The effect of kinship placement laws on foster children’s well-being. BE J Econ Anal Policy 2017;17:1-51. https://doi.org/10.1515/bejeap-2016-0196.
- Izzo CV, Smith EG, Holden MJ, Norton CI, Nunno MA, Sellers DE. Intervening at the setting level to prevent behavioral incidents in residential child care: efficacy of the CARE program model. Prev Sci 2016;17:554-64. https://doi.org/10.1007/s11121-016-0649-0.
- Kessler RC, Pecora PJ, Williams J, Hiripi E, O’Brien K, English D, et al. Effects of enhanced foster care on the long-term physical and mental health of foster care alumni. Arch Gen Psychiatry 2008;65:625-33. https://doi.org/10.1001/archpsyc.65.6.625.
- Leloux-Opmeer H, Kuiper C, Swaab H, Scholte E. Similarities and differences in the psychosocial development of children placed in different 24-h settings. J Child Fam Stud 2018;27:1299-310. https://doi.org/10.1007/s10826-017-0955-6.
- Leon SC, Saucedo DJ, Jachymiak K. Keeping it in the family: the impact of a family finding intervention on placement, permanency, and well-being outcomes. Child Youth Serv Rev 2016;70:163-70. https://doi.org/10.1016/j.childyouth.2016.09.020.
- Livheim F, Tengström A, Andersson G, Dahl J, Björck C, Rosendahl I. A quasi-experimental, multicenter study of acceptance and commitment therapy for antisocial youth in residential care. J Context Behav Sci 2020;16:119-27. https://doi.org/10.1016/j.jcbs.2020.03.008.
- Lotty M, Dunn-Galvin A, Bantry-White E. Effectiveness of a trauma-informed care psychoeducational program for foster carers: evaluation of the fostering connections program. Child Abuse Negl 2020;102. https://doi.org/10.1016/j.chiabu.2020.104390.
- McCrae JS, Lee BR, Barth RP, Rauktis ME. Comparing three years of well-being outcomes for youth in group care and nonkinship foster care. Child Welfare 2010;89:229-49. https://www.jstor.org/stable/45400463 (accessed 15 October 2024).
- Muela A, Balluerka N, Amiano N, Caldentey Miguel A, Aliri J. Animal-assisted psychotherapy for young people with behavioural problems in residential care. Clin Psychol Psychother 2017;24:O1485-94. https://doi.org/10.1002/cpp.2112.
- Portwood SG, Boyd SA, Nelson EB, Murdock TB, Hamilton J, Miller AD. A comparison of outcomes for children and youth in foster and residential group care across agencies. Child Youth Serv Rev 2018;85:19-25. https://doi.org/10.1016/j.childyouth.2017.11.027.
- Pozo-Breen A. The Effectiveness of Individualized and Rehabilitative Therapies for Children in Foster Care 2018.
- Price JM, Roesch S, Walsh NE. Effectiveness of the KEEP foster parent intervention during an implementation trial. Child Youth Serv Rev 2012;34:2487-94. https://doi.org/10.1016/j.childyouth.2012.09.010.
- Rivard JC, Bloom SL, Abramovitz R, Pasquale LE, Duncan M, McCorkle D, et al. Assessing the implementation and effects of a trauma-focused intervention for youths in residential treatment. Psychiatr Q 2003;74:137-54. https://doi.org/10.1023/ A:1021355727114.
- Scholte EM, van der PJD. Residential treatment of adolescents with severe behavioural problems. J Adolesc 2006;29:641-54. https://doi.org/10.1016/j.adolescence.2005.05.010.
- Silva AD, Coelho P, Taveira MDC. Effectiveness of a career intervention for empowerment of institutionalized youth. Vulnerable Child Youth Stud 2017;12:171-81. https://doi.org/10.1080/17450128.2017.1282070.
- Timmer SG, Urquiza AJ, Zebell N. Challenging foster caregiver–maltreated child relationships: the effectiveness of parent–child interaction therapy. Child Youth Serv Rev 2006;28:1-19. https://doi.org/10.1016/j.childyouth.2005.01.006.
- Williams NJ, Sherr ME. Children’s psychosocial rehabilitation: clinical outcomes for youth with serious emotional disturbance living in foster care. Child Adolesc Soc Work J 2009;26:225-34. https://doi.org/10.1007/s10560-008-0160-y.
- Wood JN, Dougherty SL, Long J, Messer EP, Rubin D. A pilot investigation of a novel intervention to improve behavioral well-being for children in foster care. J Emot Behav Disord 2019;27:3-13. https://doi.org/10.1177/1063426617733715.
- Pereira AI, Ferreira C, Oliveira M, Evangelista ES, Ferreira J, Roberto MS, et al. Effectiveness of a combined surf and psychological preventive intervention with children and adolescents in residential childcare: a randomized controlled trial. Rev Psicol Clín Niños Adolesc 2020;7:22-31. https://doi.org/10.21134/rpcna.2020.07.2.3.
- Suomi A, Lucas N, McArthur M, Humphreys C, Dobbins T, Taplin S. Cluster randomized controlled trial (RCT) to support parental contact for children in out-of-home care. Child Abuse Negl 2020;109. https://doi.org/10.1016/j.chiabu.2020.104708.
- Yan Y, De Luca S. Heterogeneity of treatment effects of PMTO in foster care: a latent profile transition analysis. J Child Fam Stud 2021;30:17-28. https://doi.org/10.1007/s10826-020-01798-y.
- Johnson S, Pryce JZM. The role of therapeutic mentoring in enhancing outcomes for youth in foster care. Child Welf 2010;90:51-69.
- Mersky JP, Topitzes J, Janczewski CE, Lee C-TP, McGaughey G, McNeil CB. Translating and implementing evidence-based mental health services in child welfare. Adm Policy Ment Health 2020;47:693-704. https://doi.org/10.1007/s10488-020-01011-8.
- Boyd KA, Balogun MO, Minnis H. Development of a radical foster care intervention in Glasgow, Scotland. Health Promot Int 2016;31:665-73. https://doi.org/10.1093/heapro/dav041.
- Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014;348. https://doi.org/10.1136/bmj.g1687.
- Baginsky M, Moriarty J, Manthorpe J, Ougrin D, Middleton K. Evaluation of the Early Implementation of the New Orleans Intervention Model in a London Borough London. London: Department for Education; 2017.
- Crespo C, Roberto M, Pereira A. Effectiveness of a combined surf and psychological preventive intervention with children and adolescents in residential childcare: a randomized controlled trial. Rev Psicol Clín Niños Adolesc 2020;7. https://doi.org/10.21134/rpcna.2020.07.2.3.
- Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 2019;366. https://doi.org/10.1136/bmj.l4898.
- Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016;355. https://doi.org/10.1136/bmj.i4919.
- National Academy for Parenting Research . The Fostering Changes Programme n.d. www.isrctn.com/ISRCTN58581840 (accessed 12 March 2024).
- Meader N, King K, Llewellyn A, Norman G, Brown J, Rodgers M, et al. A checklist designed to aid consistency and reproducibility of GRADE assessments: development and pilot validation. Syst Rev 2014;3. https://doi.org/10.1186/2046-4053-3-82.
- Bartoš F, Maier M, Quintana D, Wagenmakers EJ. Adjusting for publication bias in JASP & R: selection models, PET-PEESE, and robust Bayesian meta-analysis. Adv Methods Pract Psychol Sci 2022;5. https://doi.org/10.1177/25152459221109259.
- Cochrane Collaboration . PROGRESS-Plus n.d. https://methods.cochrane.org/equity/projects/evidence-equity/progress-plus (accessed 12 March 2024).
- Tancred T, Paparini S, Melendez-Torres GJ, Fletcher A, Thomas J, Campbell R, et al. Interventions integrating health and academic interventions to prevent substance use and violence: a systematic review and synthesis of process evaluations. Syst Rev 2018;7. https://doi.org/10.1186/s13643-018-0886-3.
- Roberts L, Rees A, Mannay D, Bayfield H, Corliss C, Diaz C, et al. Corporate parenting in a pandemic: considering the delivery and receipt of support to care leavers in Wales during Covid-19. Child Youth Serv Rev 2021;128. https://doi.org/10.1016/j.childyouth.2021.106155.
- Bretherton I. The origins of attachment theory: John Bowlby and Mary Ainsworth. Dev Psychol 1992;28:759-75. https://doi.org/10.1037/0012-1649.28.5.759.
- Waid J, Uhrich M. A scoping review of the theory and practice of positive youth development. Br J Soc Work 2020;50:5-24. https://doi.org/10.1093/bjsw/bcy130.
- Bandura A, Walters RH. Social Learning Theory. Englewood Cliffs: Prentice Hall; 1977.
- Children’s Commissioner for Wales . No Wrong Door: Bringing Together Services to Meet Children’s Needs 2020. www.childcomwales.org.uk/publications/no-wrong-door-bringing-services-together-to-meet-childrens-needs/ (accessed 12 March 2024).
- Wight D, Wimbush E, Jepson R, Doi L. Six steps in quality intervention development (6SQuID). J Epidemiol Community Health 2016;70:520-5. https://doi.org/10.1136/jech-2015-205952.
Appendix 1 Protocol amendments
| Protocol version | Comments and key changes | Approval date |
|---|---|---|
| 1.1 | CHIMES protocol | 30 March 2020 |
| 1.2 | The protocol includes one key change undertaken since version V1.1. In consultation with the project advisory group (via e-mail) we have decided to not a priori specify secondary outcomes. Rather, we will map the secondary outcomes reported in each study report, prioritising those identified through our patient and public involvement work. The logic model is track changed to reflect this. | 15 December 2020 |
| 2.0 | Updated Gantt chart to reflect changes in provisional project plan to account for COVID-19 delays. | 11 March 2021 |
| 2.1 | We have amended the inclusion criteria to specify inclusion in relation to biomedical markers. Some retrieved studies indicate that they use cortisol as a measure of stress in the population. This was not explicitly included in the protocol and was not included in the search strategy. As such, we have partial coverage of the outcome. We have been clearer in the protocol that we are not including measurements of cortisol where it is the primary outcome measure. Where an eligible outcome is included, and cortisol is a secondary outcome we have mapped it at the mapping stage. | 11 October 2021 |
| 2.2 | We have made four amendments to the protocol. (1) In the protocol appendix, we have cross-referenced with the project plan update, which includes the 6-month costed extension. (2) We have specified that the inclusion criteria for subjective well-being also included quality of life and life satisfaction. (3) We noticed an error on the included screening tool. Orphans and unaccompanied asylum seekers were initially intended to be included but were removed at the start of the review to ensure feasibility. We have moved these to the exclusion list. (4) For the equity harms, we have specified that we included data from study reports that conducted moderation analysis or interaction effects. | Draft for approval 7 February 2022 |
Appendix 2 Search strategy (developed and tested in OVID MEDLINE)
-
exp Child/
-
exp Infant/
-
Young Adult/
-
Adolescent/
-
(teen or teens or teenager*).tw.
-
(adolesc* or preadolesc* or pre-adolesc* or juvenile*).tw.
-
(youth or youths or youngster*).tw.
-
((young adj (person or persons or people)) or ‘early adult*’).tw.
-
(student or students or schoolchild*).tw.
-
(girl* or boy* or child or children or infant or infants or kid or kids).tw.
-
(pediatri* or paediatric*).tw.
-
(pubescen* or puberty or prepubescen* or pre-pubescen*).tw.
-
orphan*.tw.
-
Child, Foster/
-
Child, Orphaned/
-
‘Child of Impaired Parents’/
-
1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16
-
((substitute or ‘local authority’ or state or statutory or public or ‘out of home’ or order or place* or group*) adj (care or placement*)).tw.
-
((nonparent or non-parent) adj3 care).tw.
-
((children’s or childrens) adj home).tw.
-
((institution* or residential or foster or kinship or group) adj3 (care or home* or placement*)).tw.
-
(‘support* living’ or ‘supported lodging*’ or ‘care leaver*’).tw.
-
(leaving adj2 care).tw.
-
((in or welfare or social or respite) adj care).tw.
-
looked after.tw.
-
Special guardian*.tw.
-
Foster Home Care/
-
Child, Institutionalized/
-
18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28
-
‘Quality of Life’/
-
personal satisfaction/
-
(wellbeing or well-being or ‘well being’).tw.
-
(illbeing or ill-being or ‘ill being’).tw.
-
hedoni*.tw.
-
(eudaimoni* or eudaemoni* or eudemoni*).tw.
-
happiness.tw.
-
((positive or negative) adj affect).tw.
-
flourish*.tw.
-
(‘life satisfaction’ or ‘satisfaction with life’).tw.
-
(‘positive and negative affect schedule’ or PANAS).tw.
-
(‘Warwick-Edinburgh Mental Wellbeing’ or WEMWBS).tw.
-
(‘State Trait Anxiety Inventory’ or STAI).tw.
-
‘Perceived Stress Scale’.tw.
-
SWLS.tw.
-
30 or 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38 or 39 or 40 or 41 or 42 or 43 or 44
-
Mental Health/
-
exp Mental Disorders/
-
Catatonia/
-
Self-Injurious Behavior/
-
Self Mutilation/
-
Suicide/
-
Suicidal Ideation/
-
Suicide, Attempted/
-
Suicide, Completed/
-
‘mental health’.tw.
-
(‘bodily distress’ or paraphilic or paraphilia or catatonia or catatonic or dissociation or ‘impulse control’).tw.
-
(schizophrenia or psychotic or psychosis or OCD or ‘obsessive compulsive disorder’).tw.
-
suicid*.tw.
-
(self adj2 (harm or injur* or cutting or mutilation or poison* or burn*)).tw.
-
((‘post traumatic’ or post-traumatic or posttraumatic) adj2 (stress or disorder*)).tw.
-
((grief or adjustment or ‘reactive attachment’ or ‘disinhibited social engagement’) adj2 (disorder* or condition* or problem*)).tw.
-
(disruptive adj2 behavio?r*).tw.
-
((behavio?r* or neurodevelopmental or mood or fear or anxiety or personality or disruptive or dissocial or impulse or factitious or neurocognitive or feeding or eating or elimination or disruptive or dissocial or anxiety or depressive) adj3 (disorder* or condition* or problem*)).tw.
-
46 or 47 or 48 or 49 or 50 or 51 or 52 or 53 or 54 or 55 or 56 or 57 or 58 or 59 or 60 or 61 or 62 or 63
-
45 or 64
-
exp Controlled Clinical Trial/
-
Double-Blind Method/
-
exp ‘Costs and Cost Analysis’/
-
random allocation/
-
((‘pre-test’ or pretest or posttest or ‘post-test’ or ‘pre-intervention’ or ‘post-intervention’ or ‘controlled before’ or ‘before and after’ or ‘follow-up assessment’) and (controlled or control or ‘comparison participants’ or ‘comparison group’ or ‘usual care’ or placebo)).tw.
-
(‘quasi-experiment*’ or quasiexperiment* or ‘quasi-randomi*’ or ‘quasirandomi*’ or ‘natural* experiment’ or ‘time series’ or ‘interrupted time’).tw.
-
((controlled or control or intervention or comparison) adj3 (group or groups or study or trial or evaluation or cohort or cohorts or longitudinal or matched or matching or experiment or experimental)).tw.
-
(‘difference in difference’ or ‘instrumental variable*’ or ‘propensity score matching’ or ‘process evaluation’).tw.
-
((cost or costs or costing or economic) adj1 (analysis or effectiveness or benefit or evaluation or utility or savings or measure or measures)).tw.
-
(trial or ‘randomi?ed controlled trial’ or rct or ‘cross-over design’ or ‘cross over design’ or ‘crossover design’ or ‘cross-over study’ or ‘cross over study’ or ‘crossover study’ or ‘factorial design’ or ‘controlled study’ or ‘controlled design’ or ‘single-blind’ or ‘single blind’ or ‘double-blind’ or ‘double blind’ or ‘triple-blind’ or ‘triple blind’).tw.
-
effectiveness.tw.
-
program evaluation/
-
(program* adj (effect* or efficacy)).tw.
-
((theor* or mechanism*) adj3 (change or impact or program*)).tw.
-
((‘mixed method*’ or ‘mixed-method*’ or process or qualitative) adj3 evaluation*).tw.
-
(causal adj2 (assumption* or process*)).tw.
-
66 or 67 or 68 or 69 or 70 or 71 or 72 or 73 or 74 or 75 or 76 or 77 or 78 or 79 or 80 or 81
-
17 and 29 and 65 and 82
-
limit 83 to yr=’1990 -Current’
List of abbreviations
- ABC
- attachment and biobehavioural catchup
- ACE
- adverse childhood experience
- ADHD
- attention deficit hyperactivity disorder
- CAMHS
- Child and Adolescent Mental Health Services
- CARE
- Children and Residential Experiences
- CBCL
- Child Behaviour Checklist
- CBT
- cognitive–behavioural therapy
- CERQual
- Confidence in the Evidence from Reviews of Qualitative Research
- CICI
- context and implementation of complex interventions
- EEP
- equine-facilitated psychotherapy
- FHF
- Fostering Healthy Futures
- FIAP
- Fostering Individualized Assistance Program
- GIFT
- Glasgow Infant and Family Team
- GRADE
- Grading of Recommendations Assessment, Development and Evaluation
- GRIPP
- Guidance for Reporting Involvement of Patients and the Public
- ICC
- intracluster correlation coefficient
- ICD-11
- International Classification of Diseases, 11th Edition
- IPS
- Intensive Permanence Services
- IQ
- intelligence quotient
- KEEP
- keeping foster carers and kinship carers supported
- LIFT
- London Infant and Family Team
- MTFC
- multi-dimensional treatment foster care
- MST
- multisystem therapy
- NICE
- National Institute for Health and Care Excellence
- NIHR
- National Institute for Health and Care Research
- PCIT
- parent–child interaction therapy
- PHR
- Public Health Research
- PMT
- parent management training
- PMTO
- Parent Management Training Treatment Oregon
- PRISMA
- Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- PTSD
- post-traumatic stress disorder
- QED
- quasi-experimental design
- RCT
- randomised controlled trials
- REC
- Research Ethics Committee
- RoB
- risk of bias
- ROBINS-I
- Risk Of Bias In Non-randomized Studies – of Interventions
- RQ
- research question
- SDQ
- Strengths and Difficulties Questionnaire
- SOLID
- Supporting Looked-After Children in Decreasing Drugs and Alcohol
- TFC
- treatment foster care
- TFTC
- Together Facing the Challenge
- TF-CBT
- trauma focused-cognitive–behavioural therapy
- TIDieR
- Template for Intervention Description and Reporting
- TST
- trauma systems therapy
- WP
- work package
- YIM
- youth initiated mentoring
Notes
-
Randomised controlled trial study design data extraction and quality appraisal
-
Non-randomised study design extraction and quality appraisal
-
Description of intervention outcome domains of subjective well-being, mental health, neurodevelopmental and behavioural disorders, and suicide-related outcomes
-
Description of intervention outcome domains for additional outcomes
-
Study characteristics of RCT outcome evaluations included in outcome synthesis
-
Study characteristics of QED outcome evaluations included in outcome synthesis
-
Effect size for mental, behavioural and neurodevelopmental disorder outcome domains
-
GRADE assessment of outcome evaluations – short-term outcomes
-
GRADE assessment of outcome evaluations – long-term outcomes
-
Summary of thin process evaluations – context, implementation and acceptability
Supplementary material can be found on the NIHR Journals Library report page (https://doi.org/10.3310/MKYP6299).
Supplementary material has been provided by the authors to support the report and any files provided at submission will have been seen by peer reviewers, but not extensively reviewed. Any supplementary material provided at a later stage in the process may not have been peer reviewed.