

Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number 17/50/01. The contractual start date was in July 2018. The final report began editorial review in March 2021 and was accepted for publication in October 2021. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Permissions
Copyright statement
Copyright © 2022 Jago et al. This work was produced by Jago et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This is an Open Access publication distributed under the terms of the Creative Commons Attribution CC BY 4.0 licence, which permits unrestricted use, distribution, reproduction and adaption in any medium and for any purpose provided that it is properly attributed. See: https://creativecommons.org/licenses/by/4.0/. For attribution the title, original author(s), the publication source – NIHR Journals Library, and the DOI of the publication must be cited.
2022 Jago et al.
Chapter 1 Background and introduction
Parts of this chapter have been reproduced with permission from Willis et al. 1 and Jago et al. 2 These are Open Access articles distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: https://creativecommons.org/licenses/by/4.0/. The text below includes minor additions and formatting changes to the original text.
Girls’ physical activity during adolescence
Physical activity during adolescence is associated favourably with body composition, blood pressure, cholesterol and blood lipid levels,3 as well as with higher well-being, self-esteem4 and academic performance. 5 There is moderate evidence that physical activity tracks through adolescence and into adulthood,6–8 and physical activity in adulthood is strongly associated with reduced risk of heart disease, stroke, type 2 diabetes and all-cause mortality. 9
On average, children and adolescents do not meet the current international guidance of 1 hour of moderate to vigorous physical activity (MVPA) per day. 10 Girls are less physically active than boys at all ages, but especially in adolescence [difference in daily MVPA 17 minutes, 95% confidence interval (CI) 16 to 18 minutes], and are more sedentary (difference in sedentary time 22 minutes, 95% CI 19 to 25 minutes). 10 Thus, there is a need to support girls to be more physically active.
Effectiveness of physical activity interventions for girls
Increasing physical activity among girls has been identified as a public health priority,11 and a number of studies have attempted to help girls to be more active. However, systematic review evidence suggests that interventions have been only minimally effective at increasing physical activity among young people12 and, specifically, among girls. 13–15
In their meta-analysis of the effect of school-based interventions on objectively measured physical activity, Borde et al. 12 pooled data from 12 studies (two with boys only and two with girls only) and found that the effect on both overall physical activity (standardised mean difference 0.02, 95% CI −0.13 to 0.18) and MVPA (standardised mean difference 0.24, 95% CI −0.08 to 0.56) was small and non-significant. Common components of the reviewed interventions included traditional top-down strategies, such as increasing active breaks, providing health education and information, running extra lessons and distributing pedometers for self-monitoring. The authors reported that studies with higher compliance with accelerometer protocols yielded stronger positive effects. 12 A similar review and meta-analysis looking at school-based interventions targeting only girls concluded that, to date, interventions have recorded a very small effect on adolescent girls’ physical activity levels (k = 16, g = 0.07; p = 0.05); nonetheless, it also concluded that multicomponent interventions showed more promise, and interventions underpinned by theory may be more effective. 14 This is aligned with findings from an earlier review that found that multicomponent interventions were more effective at increasing physical activity; however, the findings also differed in that atheoretical interventions of higher quality yielded more positive outcomes than those of lower quality that were underpinned by theory,13 identifying the importance of trial quality on results.
A narrative review of 15 interventions (10 of which were school based) aimed at changing objectively measured health outcomes (i.e. physical activity, body mass index, body fat percentage) in adolescent girls15 identified little evidence that interventions increased objectively assessed physical activity. The authors also highlighted that the impact of the studies may have been limited by attendance rates to the interventions, as well as compliance with accelerometer measurement of physical activity. 15 Collectively, this evidence suggests that interventions to increase physical activity levels in adolescent girls, whether school based or not, are minimally effective, at best, and are potentially limited by methodological issues, such as the measurement of physical activity, intervention design and dose, or a combination of these factors.
Correlates of girls’ physical activity
Factors known to be associated with physical activity in adolescent girls are increased enjoyment, increased perceived competence, higher self-efficacy and higher socioeconomic position (SEP). 16 There is also some evidence that adolescents from lower socioeconomic groups engage in lower levels of physical activity,17 which may, in part, be explained by less favourable psychosocial determinants of physical activity. 18 Furthermore, a scoping review exploring gender norms in relation to physical activity and nutrition concluded that lifestyle components are greatly affected by feminine ideals through complex negotiations, perceptions, body-centred discourse and societal influences. 19 Similarly, changes to friendship groups, social/peer support, perceived competence, competing priorities, body-centred issues (e.g. weight status and menstruation) and ‘sporty’ gender stereotypes encountered during adolescence are factors that may contribute to the decline in girls’ physical activity. 20–23
Peers and physical activity
Peers play a central role in adolescents’ physical activity through peer support, co-participation, peer norms, friendship quality, peer affiliation and peer victimisation. 24,25 Qualitative studies among adolescent girls have shown that co-participation in physical activity with peers is an important motivating factor,23 and that a shared interest in physical activity with friends is associated with higher levels of motivation to be active, as well as greater enjoyment of being active. 26 Social network research has shown that adolescents have similar physical activity levels to their close friends, and they may adapt their physical activity behaviour over time to be more like that of their friends. 27,28 Peer-led interventions, therefore, have the potential to increase adolescents’ physical activity. There is a need to develop effective physical activity interventions, especially among girls, that capitalise on existing peer processes in schools by promoting peer support and enhancing peer communication skills. 24
Peer-led health interventions
Peer-led approaches have been used in attempts to change a range of health behaviours among young people, including tobacco, alcohol and drug use,29 nutrition education, water consumption30,31 and sexual health. 32 A small number of studies have attempted to use peer influence to change physical activity and sedentary behaviours;33 however, more recently, studies using a peer-led approach to target physical activity in young people have increased. A recent scoping review of peer-led physical activity interventions highlighted several approaches to increasing physical activity; however, the results are mixed in terms of their effectiveness, with no clear indication of specific approaches or intervention factors affecting impact. 34
The authors of this review note that many approaches use young people to deliver adult agendas. For instance, most peer-led health interventions to date have been delivered in secondary education settings; through information provision and skill development, these interventions also trained peer leaders to educate other pupils by teaching sections of the curriculum (that would otherwise be taught by adults) through buddy learning or by leading new physical activity initiatives and supporting teacher-led activities. 34,35 However, using a different approach, young people in the role of peer leader could take more control over the intervention that they delivered, which may have enhanced their credibility among their peers, in contrast to delivering a clearly adult agenda. 34,36
An alternative peer-led approach, based on diffusion of innovations theory (DOI),36 is to provide training to young people that empowers them with the information and skills to diffuse health promotion messages to their peers through informal means. DOI explains how ideas, beliefs or behaviours can be informally communicated through members of a social system in ways that are authentic to their peer group, an approach that was adopted in the effective and nationally disseminated ASSIST (A Stop Smoking in Schools Trial). 37 The findings from ASSIST demonstrated that informal school-based peer-led interventions can be effective in changing smoking behaviour. 37
Theoretical underpinning
Evidence of the influence of theory on the effectiveness of health behaviour interventions is, generally, mixed, although robust analysis of interventions, based on theories for which there are sufficient data to analyse (e.g. social cognitive theory and transtheoretical model), show that their use is unlikely to increase intervention effectiveness. 38 Overall, the evidence is restricted in several ways; notably, there is a lack of studies with a robust theoretical basis (especially a limited use of theory during intervention development), limited use of a range of theories, inadequate mapping of behaviour change techniques to theory in interventions and scant use of theory to select participants or tailor the intervention.
Conversely, theory that is used with clarity and focus, and that is well matched to the intervention design and target group (including to select participants) and underpinned by a logic model highlighting mediating mechanisms, with clear mapping of behaviour change techniques to theoretical mediators, can provide an important element of intervention design, delivery and evaluation. Using theory effectively will also contribute higher-quality theory-based interventions that can advance research into the effectiveness of the use of theory.
Few peer-led physical activity interventions integrate theoretical principles in their design or delivery. 33,34 The present trial combines two complementary theories: DOI and self-determination theory (SDT). DOI was used to inform the intervention design and the selection of key participants (i.e. peer supporters as agents of change). SDT was used to inform the content (i.e. the ‘what’ and the ‘how’) of the intervention, including behaviour change techniques to proposed mediators between the intervention (i.e. peer support) and the outcome (i.e. physical activity).
Diffusion of information uses pre-existing social systems, such as friendship networks, to diffuse information and influence behaviour. 39 Therefore, it provides a framework for harnessing the influential capacities of change agents in social networks, who can informally diffuse positive health messages to their peers. The relevance of DOI for interventions targeting adolescent girls is clear because of the role that peers play in influencing drivers of physical activity. 23,24,26
Self-determination theory40 is concerned with the personal and social conditions required to foster high-quality and sustainable motivation, and has been used extensively to understand young people’s motivation to be physically active,22,41,42 as well as to guide interventions. 43–45 SDT argues that autonomous motivation (i.e. motivation based on choice and personal value or inherent satisfaction) is associated with more positive behavioural and psychological outcomes than controlled motivation (i.e. motivation driven by external factors, such as meeting others’ expectations or guilt). Evidence points to consistent positive associations between autonomous versus controlled motivation and physical activity in children, adolescents and adults alike. 41,42,46–49 Autonomous motivation is associated with perceptions of autonomy, competence and social belonging;42,50 therefore, it is supported by social environments and interactions (e.g. interactions with peers) that satisfy these three psychological needs. SDT is, therefore, fitting for a peer-led intervention, as peers can create a social climate that either facilitates or undermines girls’ interest in,33 enjoyment of and motivation for physical activity;23,26 perceptions of competence; social support; and choice of how to be active. 20,22
Summary of formative work
The Peer-Led physical Activity iNtervention for Adolescent girls (PLAN-A) intervention design was informed by extensive formative, pilot and feasibility research, including iterative qualitative research conducted to adapt the ASSIST37 peer-led smoking intervention model to target physical activity, as well as an intervention pilot51 and a cluster-randomised feasibility trial. 52 The feasibility trial was conducted in six UK secondary schools (four intervention and two control) with girls in Year 8 of the UK education system (i.e. girls aged 12–13 years), and included a health economics assessment and a comprehensive mixed-methods process evaluation. 51–53
The intervention consisted of three stages:
-
Girls anonymously nominated the peers they felt were well suited to being a peer supporter (the peer nomination process).
-
The 18% of girls who were most frequently nominated in each school were invited to attend 3 days of specialist peer supporter training to provide them with skills and information.
-
The trained peer supporters then informally influenced the physical activity of their close peers using a range of supportive techniques over a 10-week diffusion period.
The intervention design was based on DOI, and SDT was layered into the delivery, resources and content of the peer supporter training. Pupils’ physical activity was measured at baseline, immediately after the 10-week diffusion period and then approximately 5 months after the intervention period. 53
The results showed that the intervention was deliverable, acceptable and affordable. There was evidence of promise at the 5-month follow-up time point, at which time there was a 6.1-minute difference in weekday MVPA favouring the intervention arm, after adjustment (95% CI 1.4 to 10.8 minutes). In addition, mean sedentary time per day was 23 minutes lower (95% CI –43.7 to –2.8 minutes) in the intervention arm than in the control arm at the same time point. 51 The economic evaluation demonstrated that the programme has potential for cost-effective delivery from a public-sector perspective. The mean cost of intervention delivery equated to £37 per Year 8 girl and £6 per additional minute of weekday MVPA,45 comparing favourably with other multicomponent physical activity interventions in adolescents. 54 The mixed-methods process evaluation identified key refinements for the intervention delivery and content, including increasing participatory learning, focusing more on how to start conversations with peers and providing more support to overcome challenges to giving peer support. 55
Rationale for the current trial
Physical activity during childhood is positively associated with physical and psychological health. Physical activity declines with age and, by adolescence, few girls are sufficiently active. School-based interventions have had limited success and novel interventions are needed to mitigate girls’ lack of participation in physical activity. The power of peer influence presents a natural and sustainable intervention opportunity that has received little attention in high-quality research to date. Having followed the Medical Research Council framework for the development of complex interventions56 and made revisions to intervention content informed by robust feasibility work, the aim of this definitive trial was to test whether or not the PLAN-A intervention can increase adolescent girls’ physical activity and be cost-effective.
Chapter 2 Trial design and methods
Parts of this chapter have been reproduced with permission from Willis et al. 1 and Jago et al. 2 These are Open Access articles distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: https://creativecommons.org/licenses/by/4.0/. The text below includes minor additions and formatting changes to the original text.
Research aims
The four research aims of this trial were to determine the:
-
effectiveness of PLAN-A in increasing the objectively assessed (i.e. accelerometer-derived) mean weekday minutes of MVPA among Year 9 girls (i.e. 13–14 years old) 5–6 months after the end of a 10-week intervention
-
effectiveness of PLAN-A in improving the following secondary outcomes among Year 9 girls 5–6 months after the end of a 10-week intervention –
-
mean weekend minutes of MVPA
-
mean weekday minutes of sedentary time (accelerometer-derived)
-
mean weekend minutes of sedentary time (accelerometer-derived)
-
self-esteem (self-reported)57
-
-
extent to which any effects of the intervention on primary or secondary outcomes are mediated by autonomous and controlled motivation towards physical activity and perceptions of autonomy, competence and relatedness/peer support in physical activity
-
cost-effectiveness of PLAN-A from a public-sector perspective.
Trial design
The trial was a two-arm, school-based, cluster-randomised controlled trial to compare the PLAN-A intervention with a usual-practice control. The trial included a mixed-methods process evaluation and a health economics evaluation. The method and results are reported in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidance,58 the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist,59 the Template for Intervention Description and Replication (TIDieR) checklist60 and the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement checklist. 61 The trial was registered with the International Standard Registered Clinical/social sTudy Number (reference ISRCTN14539759) on 31 May 2018.
Protocol amendments
The original trial protocol (version 1.0) was submitted to the National Institute for Health Research (NIHR) on 31 May 2018. Version 1.1 was submitted on 28 January 2019 with one minor change, and version 1.2 was submitted on 10 April 2019 with further changes. These revisions are detailed in Table 1.
| Change made to version | Description of amendment | Submitted |
|---|---|---|
| 1.0 | Page 8: clarification of the randomisation process | Submitted to NIHR on 28 January 2019 in version 1.1 |
| 1.1 | Page 12: sample size. The lead trial statistician updated the text to correct an inconsistency in the sample size calculation and justify the decision to include 20 schools based on pragmatic power calculations. These changes were agreed with the TSC | Submitted to NIHR on 10 April 2019 in version 1.2 |
| 1.1 | Page 13: data analysis. The lead trial statistician updated text to reflect pre-specified subgroup analyses proposed and agreed in the TSC meeting dated 15 March 2019, and to explain the conditions under which a per-protocol secondary analysis would be performed. These changes were agreed with the TSC | Submitted to NIHR on 10 April 2019 in version 1.2 |
| 1.1 | Page 13: economic analysis. The lead trial health economist updated text to align with the statistical inclusion of prespecified subgroups and use of imputation in sensitivity analyses. They also further detailed how quality-of-life measures would be analysed and how extrapolation of results may be performed if the trial was effective. All changes were approved by the TSC | Submitted to NIHR on 10 April 2019 in version 1.2 |
Methods
Ethics
This trial was granted ethics approval by the School for Policy Studies Ethics and Research Committee at the University of Bristol (Bristol, UK; reference SPSREC17–18.C22) on 24 May 2018. The trial was funded by NIHR Public Health Research Programme (PHR) (project number 17/50/01). The intervention costs were funded by lottery funding from Sport England (London, UK). The University of Bristol acted as the trial sponsor (sponsorship number 2898). The occurrence of any adverse events during the project was recorded and reported to the chairperson of the School for Policy Studies Ethics and Research Committee and the chairperson of the Trial Steering Committee (TSC).
Sampling and participants
State-funded secondary schools located in south-west England with girls in Year 9 were invited to take part. Special education and independent schools were excluded. Priority was given to schools whose local pupil premium indicator was above the median (i.e. those that were more deprived) by inviting them to participate first. Schools were required to sign a trial agreement form to take part. All Year 9 girls were eligible to participate; therefore, the trial aimed to recruit all Year 9 girls in each of the 20 participating schools. Research staff members gave a standardised recruitment briefing to Year 9 girls in attendance on that day in each school to explain the purpose of the trial, the intervention, randomisation and the data collection process. The girls were given the opportunity to ask questions and were informed that they could withdraw their participation. Each girl was given a written information pack for herself and her parents, which also contained a pupil consent and parent opt-out form. Participation in the trial was contingent on providing a signed pupil consent form. Parents could opt their daughter out of the trial by providing a completed opt-out form.
Sample size
The trial was designed to achieve 90% power for the primary outcome of weekday MVPA at follow-up and was informed by the results of the feasibility trial conducted in a slightly younger cohort of girls. 51 Based on those results, the sample size calculation assumed a fixed cluster (i.e. school) size of 70 girls, an intracluster correlation coefficient of weekday MVPA of 0.01, standard deviation (SD) of 20 minutes and coefficient of variation in cluster size of 0.22. The sample size calculation allowed for 30% of girls not providing primary outcome data and the alpha was set to 5%. Informed by the feasibility trial,52 which observed a between-group difference in weekday MVPA of 6.1 minutes, we estimated that we would need 20 schools (equating to 1400 students) to detect a difference of 6 minutes in weekday MVPA with 90% power under the assumptions outlined above. Given the inherent uncertainty in many of these assumptions, two reserve schools were recruited to mitigate school withdrawal prior to completion of baseline measures.
Data collection
The PLAN-A feasibility trial52 found that including a measurement point at the end of the 10-week intervention period increased participant burden and did not allow sufficient time for behavioural changes to take root, thus showing nothing. Therefore, to maximise the possibility of observing an intervention effect and simultaneously reducing participant burden, data were collected from Year 9 girls in all schools at just two time points: baseline [time 0 (T0); October 2018 to February 2019] and at 5–6 months post intervention, approximately 12 months post baseline [time 1 (T1)]:
-
school level –
-
T0:
-
county/region
-
total number of pupils
-
total number of Year 9 pupils
-
total number of Year 9 girls
-
proportion of pupils taking free school meals
-
-
T1:
-
school-context measures
-
-
-
participant level –
-
T0:
-
accelerometer data for 7 days
-
psychosocial questionnaire (on tablet device)
-
KIDSCREEN-10 score (on tablet device)
-
EuroQol 5-Dimensions, Youth version (EQ-5D-Y), score (on tablet device)
-
demographics and family affluence (on tablet device)
-
home postcode (on paper)
-
-
T1:
-
accelerometer data for 7 days
-
psychosocial questionnaire (on tablet device)
-
KIDSCREEN-10 score (on tablet device)
-
EQ-5D-Y score (on tablet device)
-
date of birth (on paper).
-
-
All questionnaire measures at T0 and T1 were collected using a Samsung® Galaxy Tab A 10.1 (Samsung Electronics Limited, Surrey, UK) device and Research Electronic Data Capture (REDCap®) software (Vanderbilt University, Nashville, TN, USA). 62 All demographic data were self-reported and collected using the Samsung device or reported to research staff at T0 (i.e. home postcode) or T1 (i.e. date of birth). Process evaluation measures were completed during the project at each intervention school (i.e. at observations and evaluations of training between March 2019 and June 2019) and post intervention (i.e. during qualitative work between June 2019 and July 2019). At both time points, participants who completed data collection were given a £10 shopping voucher in appreciation of their contributions to the trial. Following completion of the T1 data collection, all participating schools received £500 for taking part in PLAN-A and were provided with a summary report of the findings.
Physical activity and sedentary time
To assess physical activity levels, participants wore an ActiGraph GT3X+ accelerometer (ActiGraph, LLC, Pensacola, FL, USA) during waking hours for 7 days at both time points. Participants were asked to remove the accelerometer when sleeping, showering/bathing or participating in water or contact sports. The devices were set to record data at 30 Hz and raw data were accumulated into 10-second epochs using ActiLife 6 (ActiGraph LLC).
Measures
The specific measures used for variable generation are detailed in Table 2.
| Variable | How it was assessed |
|---|---|
| Age at baseline | Age at baseline was calculated from the self-reported date of birth and date of baseline measurement |
| Ethnicity | Ethnic background was self-reported by selecting one of 13 descriptions, based on the UK Census |
| SEP | The participant’s SEP was estimated using the following parameters:
|
| Mean accelerometer-determined minutes of MVPA on weekdays | Physical activity was assessed using ActiGraph GT3X+ accelerometers, which are small devices that record bodily acceleration and have been used and validated among young people.65 Participants were asked to wear an accelerometer for 7 days at T0 and T1. Periods of ≥ 60 minutes of zero counts were recorded as ‘non-wear’ and removed. Participants were included in analysis if they provided ≥ 2 valid days (i.e. 500 minutes of data between 05.00 and 23.59). Mean minutes of daily MVPA were estimated using the Evenson66 cut-off point of ≥ 2296 CPM, which is the most accurate threshold for adolescents67 |
| Mean weekend minutes of MVPA | This was calculated as above, but across Saturday and Sunday at T0 and T1. Participant data were included in weekend analyses if they provided valid data for one or more weekend day |
| Mean weekday minutes of sedentary time | Sedentary time was calculated as for MVPA but using a cut-off point of ≤ 100 CPM66 at T0 and T1 |
| Mean weekend minutes of sedentary time | This was calculated as the mean weekday minutes of sedentary time, but across Saturday and Sunday at T0 and T1 |
| Self-esteem | Self-esteem was derived from the Self-Description Questionnaire II,57 issued at T0 and T1. The questionnaire contains four positively worded (e.g. ‘Most things I do, I do well’) and five negatively worded (e.g. ‘I don’t have much to be proud of’) items. Pupils rated how ‘true’ or ‘false’ each description was for them using a six-point Likert scale ranging from 1 (‘False – not like me at all’) to 6 (‘True – very much like me’). A mean item score was then calculated |
| Physical activity motivation (autonomous and controlled) | Pupils completed a 19-item version of the Behavioural Regulations in Exercise Questionnaire 2,68 assessing (1) intrinsic motivation (four items, e.g. ‘I value the benefits of exercise’), (2) identified motivation (four items, e.g. ‘I am physically active because it’s fun’), (3) introjected motivation (three items, e.g. ‘I feel guilty when I’m not physically active’), (4) external motivation (four items, e.g. ‘I am physically active because other people say I should be’) and (5) amotivation (four items, e.g. ‘I think being physically active is a waste of time’). Pupils indicated their agreement with each statement using a five-point Likert scale ranging from 0 (‘Not true for me’) to 4 (‘Very true for me’). Composite autonomous (i.e. the mean of intrinsic and identified) and controlled (i.e. the mean of introjected and external) were then calculated |
| Physical activity psychological need satisfaction | Pupils’ perceptions of autonomy (six items, e.g. ‘I feel I’m active because I want to be’), competence (six items, e.g. ‘I am pretty skilled at different physical activities’) and relatedness (five items, e.g. ‘I feel understood’) were assessed using a seven-point Likert scale ranging from 1 (‘Not at all true’) to 7 (‘Very true’)46,69 at T0 and T1. Participants rated how ‘like them’ each statement was. Item means for each need variable were then calculated |
| Physical activity self-efficacy | Eight items were used to assess participants’ self-efficacy to be physically active in different situations (e.g. ‘I can be physically active most days after school’) at T0 and T1.70 Pupils indicated their endorsement of each statement by giving one of three responses (‘No’, ‘Not sure’ or ‘Yes’). A mean item score was then calculated |
| Physical activity social support |
Six items assessing social support from friends for physical activity were taken from a broader questionnaire measuring factors associated with physical activity in adolescents71 at T0 and T1. Pupils read the stem ‘Thinking about your close friendship group how often do they do the following’ and rated each item (e.g. ‘Invite you to engage in physical activity with them’) using a four-point Likert scale ranging from 0 (‘Never’) to 3 (‘Always’). Items cover social support in the form of encouragement, involvement, co-participation, talking about physical activity and giving positive comments. A mean of the items was then calculated Pupils were asked two questions to assess their perceptions that others in their year (1) spoke to them about physical activity (‘Has anyone in your year group talked with you recently about physical activity?’, response options: ‘Yes’, ‘No’, ‘Not sure’) and (2) whether or not they felt it helped them be more active (‘Did talking to anyone in your year help you to be more active?’, response options: ‘Yes’, ‘No’, ‘Not sure’, ‘N/A’) |
| Peer norms for physical activity | The six-item Social Support Scale72 was used to measure three factors of peer-based social support at T0 and T1. Prevalence of friends’ physical activity was assessed with two items (e.g. ‘How many of your close friends would you say are physically active?’), scored using a four-point scale (0 = ‘None’ to 3 = ‘All’). Perceived importance placed on physical activity by peers was measured using two items (e.g. ‘How important do you think it is to your close friends to be physically active?’), scored using a three-point scale (0 = ‘Not important at all’ to 2 = ‘Very important’). Peer acceptance of the participant’s level of physical activity was assessed using two items (e.g. ‘My friends encourage me to be physically active’), scored using a four-point scale (0 = ‘Disagree a lot’ to 3 = ‘Agree a lot’). A mean item score was then calculated for prevalence, importance and acceptance |
Randomisation
The school was the unit of randomisation. Following the completion of T0 data collection, schools were randomised to the control (n = 10) or intervention (n = 10) arm, stratified by county (Avon, Devon or Wiltshire) and the England Index of Multiple Deprivation (IMD) score for the lower-layer super output area in which the school was located (dichotomised as less than the median of sampled schools in the county versus greater than or equal to that median) to ensure balance in each stratum. Schools were allocated, using a computer-generated algorithm, to either the control or intervention arm by a member of the Bristol Randomised Trials Collaboration (BRTC) who was blinded to the school identity and worked separately to the fieldwork team. Also blinded to the allocation were the lead statistician and all other team members, other than the trial manager, research associate and fieldworkers.
Intervention
The intervention design was adapted from the ASSIST model37 and comprised four components: peer nomination, train the trainers, peer supporter training and a 10-week diffusion period. The intervention components and theoretical enactment that were developed and tested in the feasibility trial have been described in detail elsewhere. 52
Refinements to the intervention
Prior to the intervention, members of the trial team made refinements to both the train-the-trainers and peer supporter training materials that were used in the feasibility trial,52 using feedback from the feasibility trainers and peer supporters (Table 3). In addition, patient and public involvement focus groups were conducted with adolescent girls between September 2018 and November 2018, exploring issues around menstruation and being physically active, the perceived and real barriers, and strategies to overcome them. The findings of these focus groups73 were woven through new intervention content during intervention refinement.
| Area of refinement | Objective of changes | Details of change |
|---|---|---|
| Train the trainers | Reinforce the principles of SDT to further trainer understanding | Additional time was added to the top-up training day to reinforce SDT |
| Peer supporter training | ||
| Logistics | Improve training venues and equipment | Venues were required to have suitable outdoor spaces, and a wider variety of equipment for peer supporters was made available |
| Structure | Improve peer supporter concentration and understanding of key message of why you should be active | Activities were reordered to promote understanding of concepts, followed by practical reinforcement |
| Material and resources |
Improve the use of the peer supporter booklet Make group size more visible to the trainers |
When to use the peer supporter booklet was highlighted in the session plan manual and a space for notes was added to the booklet Activity descriptions were simplified |
| Training content |
Reinforcing the peer supporter role Increase knowledge about being active during menstruation Allow peer supporters to feel comfortable about their role Make top-up day less repetitive Improve peer supporter engagement and enjoyment of activities Help peer supporters overcome challenges Promote peer supporter teambuilding and teamwork Make the activities easier for the peer supporters to understand |
A new, shorter activity was added Several activities were adapted to include menstruation The top-up day introduction game was adapted The ‘how, who, when, where’ activity was removed A number of the activities were made more active Activities were more focused on problem-solving Games that promoted teamwork were added to the training The terminology in the activities was simplified |
| Individual activities |
Make the concept of goal setting easier to understand for the peer supporters Improve the explanation of tasks Provide a more realistic approach to problem-solving |
Active games were added to these activities, in addition to promoting variety in answers given More guidance was provided along with activities being simplified Redundant statements were replaced with more relevant examples |
Peer nomination
To identify those girls who were influential within their year and, therefore, whom to invite to become peer supporters, all girls in Year 9 in each participating school were asked to complete a peer nomination questionnaire at the same time as the baseline measures. This questionnaire (see Report Supplementary Material 1) asked the girls to anonymously nominate up to five girls whom they respected, trusted, listened to and looked up to. The highest scoring 18% of the girls who were nominated were invited to become a peer supporter in the schools randomised to the intervention arm (with the aim of ≥ 15% agreeing to take on the role). Following feedback from the feasibility trial,52 in schools where the year group was split and the two halves shared no curriculum time, this process was conducted separately in each half to ensure fair representation of peer supporter nominations across the year group.
The nominated girls attended a briefing and were provided with an information pack for themselves and their parents, which outlined the training and their role as a peer supporter. The girls were required to provide both parental and pupil informed consent if they wished to attend the training. The girls who did not opt-in to the data collection aspect of the trial were still eligible to opt in as a peer supporter. The peer supporter and parent consent rates were recorded by the field team. Any nominated peer supporters who opted out, either before the training began or during, were asked to fill in a form at T1 to provide a reason. This was voluntary and all of the girls understood that this was optional. The reasons for non-consent were reported descriptively.
Train the trainers
Female trainers were recruited via advertisement through local authority health improvement teams and recruited as freelancers to deliver the peer supporter training component of the intervention. Trainers from the feasibility trial who had expressed interest in continued involvement were also contacted. Those expressing an interest were screened by the trial manager for availability and suitability (i.e. a background in physical activity or coaching, experience working with young people and being good communicators). Seven trainers were appointed in total, including a ‘lead trainer’, who was an experienced PLAN-A trainer from the feasibility trial with extensive teaching experience. All appointed trainers had at least a master’s degree in a physical activity research discipline plus coaching experience, or > 5 years’ practical experience in youth work.
All trainers were required to attend a training course (i.e. train the trainers) to prepare them for delivery. This course was delivered over 3 days, mimicking the peer supporter training. It was held in a studio space at the University of Bristol. To closely replicate an intervention model that would be used in a community setting, the train-the-trainers course was led by two trainers: the lead trainer and a member of the research team, who had been extensively involved in the development and refinement of the intervention. The lead trainer met with the research team beforehand for half a day to prepare. The train-the-trainers course was dedicated to the aims and design of PLAN-A, their role as a trainer, how the activities and the trainer’s delivery style aligned with DOI and SDT, and working with challenging young people. There was also a chance for the trainers to choose how they spent the last hour of the training on each day, whether this involved going over activities on their own or with a trainer they were partnered with, or leading activities themselves.
Each trainer was provided with resources to aid them in delivering the peer supporter training, including a ‘trainers’ guide’ that contained information about the principles behind PLAN-A and its concept, PLAN-A’s approach to motivation and the underpinning theories, the practicalities and logistics of delivery, and more detailed reasoning behind each of the activities. They were also provided with a ‘session plan booklet’ that detailed how to deliver each activity, the resources needed and the key messages/objectives to achieve. All resources are described in detail elsewhere. 52 In addition, trainers were provided with a resource pack for each school delivery.
Peer supporter training
All consenting peer supporters attended a 3-day training session as a school group, which was led by two trainers; the training comprised an initial 2 days of training, followed by a top-up training day 5 weeks later. Where possible, the training sessions were held at suitable venues away from school (on-site training was an option when schools were unable to provide a chaperone to attend the training and if they could offer a suitable space; schools, n = 2). To minimise school staff burden, a member of the trial team arranged venue bookings and refreshments and co-ordinated travel (if necessary) with each school. Based on the experience in the feasibility trial,52 venues needed to have ample floor space (e.g. to accommodate group games and activities), chairs, space and power to project slides, bathroom facilities, and, preferably, a food preparation area and safe outside space to use for breaks.
The training sessions had two themes. The first involved increasing the peer supporter’s knowledge around physical activity and addressed how to fit in activity, what counts as being active, the barriers to physical activity for Year 9 girls and the importance of being physically active. The second theme involved developing and improving peer supporters’ communication skills; content included how to start conversations about being active, methods of peer support and recognising opportunities to encourage, support and motivate peers to be active. The purpose of the top-up day was to provide a refresher on core topics, to discuss actions that peer supporters had taken to support their peers and to tackle any challenges that they may have faced.
Each peer supporter was provided with a ‘peer supporter booklet’ that contained worksheets used in the peer supporter training and resources to support the peer supporters outside the training. The booklet also contained a diary that offered the peer supporters the option to record conversations that they had started or support that they had provided to encourage their peers to be active. To promote continued peer support, each peer supporter wrote herself a postcard with personal motivation reminders at the end of the training that the trial team posted back to them 2 weeks after the training finished.
The training content was developed and refined to be interactive, engaging the girls both mentally and physically (see Table 3). The intervention framework was based on DOI, allowing the resources, content and delivery to harness the potential of peer influence, as well as uphold the key principles of SDT. It was designed to nurture the peer supporters’ autonomy, belonging and competence for physical activity and peer support. The framework also helped the peer supporters to promote autonomous, rather than controlled, motivation for physical activity among their peers.
The 10-week diffusion period
Once the peer supporters completed the training, their role was to support and encourage physical activity among their close peers for a period of 10 weeks. The training encompassed multiple methods of providing support, including holding conversations about being active, co-participation and providing opportunities to be active. As the intervention was based around an informal, peer-led approach, the peer supporters were encouraged to carry out their role in a way that they felt comfortable with and was most effective, taking into consideration their peers’ needs, preferences and confidence.
Control group provision
The eligible participants of the control schools participated in both data collection and peer nomination at T0. A total of 10 schools were randomly assigned to the control condition. These schools continued with normal practice [normal physical education (PE) provision and physical activity opportunities during teaching and co-curricular activities], before completing T1 data collection.
Statistical analyses
All analyses were performed using Stata® (StataCorp LP, College Station, TX, USA), version 15.
Baseline characteristics
The baseline characteristics of schools and pupils were compared between arms by reporting relevant summary statistics to identify any potentially influential imbalance. The baseline characteristics were summarised using means and SDs, medians and interquartile ranges (IQRs), or numbers and percentages, depending on the nature of the data and its respective distribution. Where the baseline characteristics of the groups differed by > 10% or half a SD, the effect of this variable on the outcome was investigated in sensitivity analyses.
Analysis of intervention effect
Two-tailed tests were used, with effect estimates, 95% CIs and p-values presented. No adjustment for multiple testing took place. Analyses using regression models adjusted for stratification variables, as well as the baseline values of the outcome studied. The primary approach for analysis was on an intention-to-treat (ITT) basis, defined as analysing participants as randomised.
The primary outcome was the accelerometer-determined minutes of MVPA on weekdays collected at T1. This was described in each group using means and SDs. Comparisons between arms used a multivariable, mixed-effects, linear regression model to allow for clustering within schools, adjusting for baseline MVPA scores (i.e. random school effects to account for clustering), and the number of valid days of accelerometer data and randomisation variables.
Secondary outcomes consisted of mean weekend and weekday minutes of sedentary time, mean weekend minutes of MVPA and self-esteem. These were continuous measures and were analysed using the same modelling approach as that used for the primary outcome.
Sensitivity analyses
Exploratory sensitivity analyses that were part of the pre-agreed statistical analysis plan,74 which was approved by the TSC prior to any analyses being conducted, were presented alongside the primary analysis to assess the sensitivity of the primary analysis to the following conditions:
-
Imbalance between groups. Where imbalance between the arms was evident at baseline, the primary analysis was repeated, adjusting for the variables showing an imbalance.
-
Missing outcome data. Patterns of missing MVPA data were explored and missing values were imputed by using the MI command in Stata to perform multiple imputation by chained equations (MICE). Analyses using imputed data were compared with the primary analysis.
-
Month of data measurement (i.e. seasonal bias). The primary analysis was repeated, adjusting for the month of the year in which the MVPA measurements were taken.
Subgroup analyses
Pre-agreed subgroup analyses were performed to estimate whether or not the intervention was differentially effective in subgroups of SEP, nominated peer supporters (peer supporters vs. non-peer supporters) and the proportion of sedentary time at baseline. This involved including interaction terms between the arms and moderator (i.e. SEP, peer supporter training or proportion of sedentary time at baseline) in the primary analysis models and using the likelihood ratio test for hypothesis testing.
As the trial was not powered to detect effectiveness in subgroups, these analyses were treated as exploratory and interpreted with caution.
Mediation analysis
Mediation analysis was conducted to explore whether or not any effect of the intervention was mediated by self-determined physical activity autonomous motivation,68 autonomy,46 competence69 or relatedness. 46 The MEDEFF command in Stata was used to estimate the causal mechanisms. Mediators were treated as continuously measured variables and described using the mean scores, stratified by arm.
Compliance and missing data
The following criteria have been used in previous studies. 75 Accelerometer compliance was calculated at each time point using the number of valid days of accelerometer data provided by each girl enrolled in the trial at that time. For participants to be considered compliant, valid accelerometer data for at least two weekdays were required. At each time point, the number and percentage of girls enrolled in the trial who provided questionnaire data were used to calculate questionnaire compliance. Rates of provision of accelerometer data (missing, invalid and valid) and questionnaire data (missing and not missing) were recorded for T0 and T1. Data were classified as missing when the valid wear time condition was not achieved or if an accelerometer was not returned. (See Table 12 for details of data provision at each time point.)
Process evaluation methods
The process evaluation for the definitive trial used a combination of qualitative and quantitative methods to examine the intervention delivery and how implementation and the resulting impact on participants were connected. Specifically, this examined the:
-
intervention implementation and fidelity
-
receipt of the intervention by pupils (peer supporters and non-peer supporters)
-
potential sustainability of the intervention and roll-out, if effectiveness was demonstrated in analyses of the primary and secondary outcomes.
We also assessed school context using physical and social environment audit tools76,77 that were piloted in the feasibility trial55 and then adapted. Data collection was carried out by the trial team with informant groups that included peer supporters, non-peer supporters, peer supporter trainers, school contacts and external stakeholders (e.g. public health commissioners).
Measures
The process evaluation measures with pupils, trainers and teachers were conducted during or straight after the intervention period in each intervention school (March–July 2019).
Peer supporter training attendance
Peer supporters’ attendance at all three of the training days was recorded by the trainers, along with reasons for absences, if known, using attendance registers. Trainers were also asked to record any adverse events that occurred.
Fidelity to PLAN-A session plans
Direct observation of the intervention sessions in each school was conducted by a member of the trial team using an observation form (see Report Supplementary Material 2) and a copy of the ‘session plan manual’ for reference. For each activity, the observer recorded whether any activities were missed or changed, how engaged the pupils were, and whether or not the learning objectives for each activity were achieved (scale ranging from 0, objective fulfilled ‘not at all’, to 3, objective fulfilled ‘mostly/all’). Fulfilment of activity objectives and pupil engagement were reported by school for each activity section using means and SDs. The observing researcher also commented on what did and did not work during the activity, potential improvements, things affecting delivery and the extent to which it supported the three needs underpinning SDT: autonomy, relatedness and competence. These qualitative data were analysed thematically to compare delivery between schools.
Trainers’ experience of the peer supporter training
Trainers completed an evaluation form after delivery of day 2 and the top-up day training (see Report Supplementary Material 3), assessing the suitability of training arrangements (ratings ranged from 0, ‘poor’, to 4, ‘excellent’, and included statements related to the resources provided to aid delivery of the training, refreshments and quality of the training facility); achievement of the training objectives (ratings ranged from 0, ‘not well at all’, to 3, ‘very well’, for statements related to how successful they felt the training was in achieving key objectives, e.g. increasing peer supporter knowledge or communication skills) and how well the peer supporters responded to training (ratings ranged from 0, ‘not at all’, to 3, ‘very’, for four items covering engagement, involvement, enjoyment and interest of peer supporters). Means and SDs were computed to describe data by school and trainer.
Participants’ experience of the peer supporter training
Peer supporters completed an evaluation form after completing day 2 and the top-up day of the training (see Report Supplementary Material 4), assessing enjoyment, content and logistics. Enjoyment of the training sessions was measured on a five-point Likert scale, with 1 indicating ‘not at all’ and 5 being ‘a lot’. Statements pertaining to training content, logistics and concept understanding (e.g. ‘I understand my role as a peer supporter’ and ‘the length of the training was about right’) were rated on a five-point Likert scale, ranging from 0, ‘disagree a lot’, to 4, ‘agree a lot’. For all schools, means, SDs and ranges were reported by question. The evaluation form also included qualitative items asking about what they had learned, what they enjoyed most, what they needed for them to be more confident peer supporters and suggested improvements for the training.
Fidelity to self-determination theory in the delivery of the peer supporter training
Peer supporters’ perceptions of autonomy support provided by the trainers during the training was measured using a six-item measure (the Sport Climate Questionnaire46), previously used in a PE setting, that was nested in the evaluation questionnaire administered after the training days. Peer supporters were asked to rate how much they agreed with statements related to how supportive the trainers were of their needs, ranging from 0 (‘disagree a lot’) to 4 (‘agree a lot’). The mean of the six items was derived to produce a needs-support score. The means and SDs were reported by school. Cronbach’s alpha estimates of internal consistency were reported for training days 1 and 2 (combined) and the top-up day.
Intervention fidelity
Peer supporters were asked to complete a questionnaire at the top-up day and, again, at the end of the 10-week diffusion period (see Report Supplementary Material 5); this was a self-reported record of the peer support undertaken. Ratings for how often different types of support were given ranged from 0, ‘never’, to 4, ‘very often’, and options for how many friends they gave that type of support to ranged from ‘0’ to ‘> 4’. Qualitative examples of peer-supporting behaviour provided in free-text space on the questionnaire were analysed qualitatively and triangulated with focus group data, as described below.
Interviews and focus groups
At the end of the 10-week diffusion period, members of the research team conducted focus groups and interviews with all informant groups (i.e. peer supporters, non-peer supporters, peer supporter trainers and school contacts). Interviews with public-sector stakeholders (e.g. public health commissioners) were conducted later, once the trial results were known.
Participants were invited to take part in a focus group or interview through information letters. All informants were required to provide informed consent to take part in the qualitative process measures. Focus groups and interviews were recorded using an encrypted digital recorder and audio recordings were transcribed verbatim. Transcribed data were anonymised before the analysis.
Separate interview guides were developed for each informant group. All interview and focus group topic guides were developed by Byron Tibbitts (PLAN-A trial manager, male) and Kathryn Willis (research associate, female), in consultation with Russell Jago (PLAN-A principal investigator) and Simon J Sebire (PLAN-A co-investigator). Interviews were conducted in private with one of three research team members [BT (male), KW (female) or TR (male)], who were all trained in qualitative data collection and analysis. Focus groups were conducted by two members of the research team in tandem, with one leading and the other supporting. Field notes were made by the supporting researcher. A prior rapport had been struck between the researchers conducting the interviews and the trainers and respondents in intervention schools through exposure to one another during intervention delivery and data collection phases.
At the start of each interview or focus group, the researcher (BT, KW or TR) outlined the purpose of the interview/group and disclosed their role in the project. The first interviews and focus groups served to pilot the topic guides, which were subsequently discussed and refined by the research team.
Peer supporter focus groups
One focus group was conducted at each intervention school between June 2019 and July 2019 (duration range 32–62 minutes). Six participants were chosen at random from the group of peer supporters using a random-number generator. The joint foci of the focus group guide were the peer supporter training and their experience of being a peer supporter (see Report Supplementary Material 7). Topics included recruitment, training logistics, training content, perceptions of the trainers and their delivery style, and experiences of and challenges to peer supporting.
Non-peer supporter focus groups
One focus group was conducted at each intervention school between June 2019 and July 2019 (duration range 17–40 minutes). Six participants were selected purposively from the non-peer supporter group to include girls across the range of baseline MVPA (i.e. random sampling within MVPA tertiles). The topic guide (see Report Supplementary Material 8) addressed general attitudes among their year group towards physical activity and the associated barriers; perceptions of the recruitment and data collection process; awareness of the intervention; and the perceived impact of the intervention on attitudes or behaviours within their year group and, specifically, on the peer supporters.
Trainer interviews
Face-to-face semistructured interviews were conducted with each trainer, including the lead trainer, between July 2019 and September 2019 (trainers, n = 7; duration range 53–83 minutes), after they had finished delivery in their final school. Interviews took place in a setting of the respondent’s choosing. The interview guide (see Report Supplementary Material 9) considered the training that they had received to carry out their role, as well as the peer supporter training that they delivered in schools. Topics included intervention content, logistics and support, what did and did not work, challenges to delivery and potential improvements that could be made to the intervention.
School contact interviews
The primary liaison for the research team at each intervention school (i.e. the school contact) was interviewed, either face to face or by telephone, after the intervention had been delivered (school contacts, n = 10; duration range 31–52 minutes). The school contact interview guide (see Report Supplementary Material 10) addressed their involvement in the project and the logistics of liaising with the trial team, with the aim of identifying any potential improvements to how the intervention could be implemented in schools.
Public-sector stakeholder interviews
Telephone interviews were conducted with 19 public-sector stakeholders (duration range 30–61 minutes), such as public health commissioners, school and regional sports partnership leads, advanced public health practitioners, education officers and agents from national governing bodies that promote physical activity in schools. Participants were sampled purposively using the following criteria: the person was employed in the public or private sector, and their professional role directly involved the implementation of physical activity-promoting initiatives with young people and/or working with schools to do so.
In order for the questions to be tailored to maximise the utility of the information received, the interviews were conducted between October 2020 and January 2021, after the trial outcomes were known. The interview topic guide (see Report Supplementary Material 11) sought to elicit stakeholders’ experience-driven perspectives on factors that influence the effectiveness of physical activity interventions in school settings, and the direction that research should take to support improvements in intervention adoption and impact. After 19 interviews, the three researchers agreed that no novel insights were emerging from transcripts and additional data would not add meaningful information power, so data collection ceased.
School context
Various quantitative and qualitative data were collected to establish school context and the potential effects on the implementation or efficacy of the intervention. Details of school size and pupil premium were provided by the school contact or school reception to establish pupil demographics. In addition, PLAN-A researchers made narrative records of school ‘social environment’ after data collection visits to reflect the experience of engaging with the school, the key contact(s), the pupils and any other factors that may have had an impact on implementation.
To explore any differences between schools in the physical activity environment, a quantitative school context audit (see Report Supplementary Material 6), which addressed similar constructs to those in Jones et al. ’s76 validated tool and was developed further in the PLAN-A feasibility trial52 and another school project,78 enabled members of the trial team to collect information on school-level physical activity provisions. Items in the adapted audit tool assessed the presence (i.e. count) and quality (graded on a five-point quality scale) of different physical activity facilities (e.g. courts, pitches, hard-surface playgrounds).
A second part of the school context measure asked school contacts to provide details on school policies regarding physical activity and the integration of physical activity throughout the curriculum. 77 To further explore school-level differences in physical activity provision that may affect the primary outcome of the trial, we asked all 20 school contacts to report termly on any change in physical activity provision or other lifestyle interventions in the school that were available to the girls in the trial.
School physical activity context scoring
Parts of this section have been reproduced with permission from Jago et al. 75 © Queen’s Printer and Controller of HMSO 2019. This work was produced by Jago et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
One school environment audit was completed per school at the T1 measurement time point, except for school 13 (which was split across two sites), for which one audit was completed for each site. Scoring was adapted from Jones et al. ,76 and was refined in the PLAN-A feasibility trial52 and another school project. 75 Each school was given a ‘school physical activity suitability’ score, which is a sum of the scores from the ‘cycling provision’, ‘walking provision’, ‘sports and play provision’ and ‘design of school grounds’. Where an item occurred in more than one section of the tool, it was included only once in the physical activity suitability score to avoid replication (i.e. the items in the walking provision set are already included under cycling provision, so the scores for these items were counted only once). In addition, each school was scored on ‘other facility provision’ (which included items such as benches, drinking fountains and wildlife garden provision) and ‘aesthetics’. The aesthetics items were scored out of five for ‘abundance/agreement’ and included positive features (e.g. trees, planted beds, art) and negative features (e.g. dog faeces, ambient noise, litter) that may contribute to an overall climate that is more or less enjoyable to spend time in while being active. Where a facility (i.e. marked pedestrian crossing) is marked as present, scores were weighted as yes = 1 and no = 0. If the quantity of facilities was provided, scores were weighted relative to the mean number of facilities across all schools:
-
0 = none was recorded
-
1 = the number was between 1 and the mean plus 1 SD
-
2 = the number was greater than the mean plus 1 SD.
In the case where the mean plus 1 SD equalled < 1:
-
0 = none was recorded
-
1 = up to the mean plus 1 SD (or 1, whichever is greater)
-
2 = > 1.
The mean quality scores for physical activity facilities and the mean abundance/agreement scores for environment aesthetics were reported by school. Items assessing individual school physical activity policies and physical activity throughout the curriculum were reported descriptively. Each school received a ‘policy’ score (maximum score = 13) and ‘curriculum’ score (maximum score = 8).
Qualitative analysis
Parts of this section have been reproduced with permission from Jago et al. 75 © Queen’s Printer and Controller of HMSO 2019. This work was produced by Jago et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
To synthesise the wide range of qualitative data collected, the framework method79 was used, as it produces a matrix of the data (from different participant groups) that allows comparison. The framework method also allows a combined approach to the analysis, enabling themes to emerge inductively from participant accounts and for specific issues to be explored deductively. Data were analysed using the following steps:
-
Researchers from the trial team thoroughly read and re-read each transcript, and listened back to audio recordings to become familiar with the data set. Initial impressions of the data were recorded to inform code development.
-
Initial codes were identified inductively by each researcher; these were refined as subsequent transcripts were analysed. For the deductive analyses, broad predefined codes for each informant group (see Appendix 1) were applied, with the primary purpose of categorising relevant information, which was to be further interrogated to elicit more refined codes and interpretations. Specifically, for questions relating to the central tenets of SDT,40 predefined codes were used to examine whether or not the intervention supported autonomous motivation among the participants and the three needs-support constructs:
-
autonomy: feelings of choice
-
relatedness: a feeling of connection between participants and with the instructor
-
competence.
-
-
An analytical framework that could be applied to all transcripts was agreed and developed to fit each informant group to avoid losing any key data using the following process:
-
Three researchers (KW, TR and BT) independently read and analysed the same two transcripts from each informant group, and then met, discussed and created draft frameworks for each.
-
A fourth researcher (SS) read the transcripts from each informant group alongside the draft frameworks and provided feedback.
-
Kathryn Willis, Byron Tibbitts and Tom Reid met to discuss and refine draft frameworks.
-
-
Three researchers (KW, BT, TR) then applied each framework to the remaining transcripts (with some level of double coding) using NVivo (QSR International, Warrington, UK), version 11. New, emerging codes were discussed between researchers and each framework was adjusted accordingly.
-
A framework matrix was then used to map all coded data by informant group, summarising the data by category and including descriptive quotations. Summarising techniques were compared to ensure consistency within the research team.
-
Frequent meetings were held between the researchers to review the matrix-enabled data analysis and theme generation. During this process, illustrative quotations to demonstrate the nature of each theme were agreed.
-
The level of convergence was evaluated by triangulating the frameworks and comparing the set of codes for each informant group.
To optimise the credibility and transparency of the research, the qualitative analysis was reported in accordance with the COREQ checklist. 59
Economic evaluation
Overview and aims
The aim of the economic evaluation was to determine the cost-effectiveness of PLAN-A.
The primary questions most relevant to the economic analysis were:
-
What is the estimated resource use and cost associated with the peer supporter training and PLAN-A intervention?
-
What is the mean cost of the PLAN-A intervention per school and per Year 9 girl?
-
What is the cost-effectiveness, in terms of (a) cost per unit increase in weekday MVPA and (b) cost per pupil achieving a 5-minute increase (which is considered a clinically important difference)80 in weekday MVPA, of the PLAN-A intervention in adolescent girls?
-
What is the effect of the PLAN-A intervention on health-related quality of life (HRQoL), measured using the EQ-5D-Y and KIDSCREEN-10?
-
What is the effect of the PLAN-A intervention in terms of the mapped Child Health Utility Instrument, nine dimensions (CHU-9D), utility scores (as derived from the KIDSCREEN-10)?
-
What is the cost–utility, in terms of cost per quality-adjusted life-year (QALY), of the PLAN-A intervention? (This was an exploratory analysis using mapped CHU-9D scores.)
Furthermore, if there is evidence of promise that PLAN-A improves MVPA at T1, what is the potential longer-term cost-effectiveness of the intervention? (For our analysis, we consider that there is evidence of promise if the point estimate of weekday MVPA is positive and the 95% CI includes the possibility of a meaningful, i.e. 5 minutes of weekday MVPA, positive intervention effect.) The within-trial economic analysis was performed using individual participant-level data on physical activity and quality of life, and school-level data on intervention costs from the PLAN-A trial. The within-trial analysis reports results 5–6 months after the end of the PLAN-A intervention and 12 months after baseline (T0). Therefore, the economic time horizon corresponds to 1 year.
Methods for costing intervention resource
To estimate a mean cost per school and per Year 9 girl, the set-up and delivery of the PLAN-A intervention in intervention schools was costed. The resources used for other physical activity initiatives, used as part of the normal curriculum, in intervention and control schools were not measured. This assumed that the PLAN-A intervention was additional to normal practice (i.e. ‘physical activity education as usual’) and that schools did not adjust their physical activity initiatives to compensate for being allocated or not being allocated to the PLAN-A intervention. The costs were collected from a public-sector perspective, using the cost year 2019, in Great British pounds (£).
The main components of resource use were school staff, trainer (including lead trainer) and pupil time, travel and materials, venue hire and administration. In the trial, some intervention activities were supported by members of the research team and the trainers were employed by the research trial. To approximate the ‘real-world’ costs for if the intervention were scaled up to all local schools, we assumed that all intervention-related tasks would be conducted by trainers and that the trainers would be employed by local authorities. In brief, resources were logged using staff time logs [which documented the role of the school staff member/trainer, the activity, the purpose and the time spent on the activity (recorded in minutes)], expense claims (i.e. mileage/travel claims) and invoices (i.e. venue, refreshment and material costs). Where possible, resource use records were completed at the time of set-up/delivery events (i.e. the train-the-trainers, peer nomination and peer supporter events). Table 4 provides an overview of the resource captured as part of intervention cost. The intervention costs exclude the cost of intervention development during the feasibility trial. We assumed that this was a ‘sunk cost’ that would not be relevant to other schools and local authorities that were considering providing training and delivering the PLAN-A intervention in the future, if PLAN-A were to become standard practice.
| Resources measured (how collected) | Source of data | Resource units |
|---|---|---|
| Train the trainers | ||
| Lead trainer and trainers’ time | Staff timesheet | Hours per trainer |
| Venue hire | Invoice | £/venue |
| Refreshments | Invoice | £/event/day |
| Travel costs | Travel expense claim | Miles, parking charges (where applicable) |
| Peer nomination with pupils | ||
| Trial staff timea | Peer nomination log | Hours/trainer |
| Travel costs | Travel expense claim | Miles |
| Pupil time | Peer nomination log | Hours |
| PLAN-A intervention consumables | ||
| Printing and other consumables (including resource kits for peer supporter training) | Invoices and PLAN-A trial budget database | £ per resource kit and additional £ per school for any disposable itemsb |
| PLAN-A intervention administration (non-face to face) | ||
| Trial staff timea | Research staff time log | Hours/trainer |
| Peer supporter intervention delivery in schools | ||
| Trainer time | Intervention delivery log | Hours/trainer |
| School staff time | School staff time log | Hours per teacher/leadership teacher/teaching support staff |
| Venue hire | Invoice | £/venue |
| Refreshment | Invoice | £/event/day |
| Travel costs | Travel expense claim | Miles, parking charges (where applicable) |
Salary band information was used to calculate school staff costs using the national teaching union main pay scale81 (Table 5). The unit cost per hour for school staff considered was calculated based on 195 contractual days for a teacher (in line with the National Association of Schoolmasters Union of Women Teachers, the teaching union for the UK)81 and ‘in-school’ hours. This includes salary on-costs (i.e. pension and national insurance). Because the logs also identified who in the school was involved with delivering the PLAN-A intervention (e.g. qualified teacher, teaching administrator or teacher with leadership responsibilities), we estimated the national average rate of pay for that role to determine the cost. The unit cost for trainers also included salary on-costs and was based on the published local government pay scale82 and assumed working days/hours for local government employees. Staff costs were calculated by multiplying the units of staff time (i.e. hours) by the appropriate unit cost for each staff member.
| Cost item | Unit cost (£)a | Source of unit cost, price year 2019 |
|---|---|---|
| Staff costs | ||
| Lead trainer | 30/hour | Based on reimbursement within trial (assumes lead trainer is self-employed) |
| Assistant lead trainer (research associate in PLAN-A trial) | 13.51/hour | Assumption that, post implementation, this work could be undertaken by a local government trainer or equivalent role |
| Trainer | 13.51/hour | Sports coach,b based on local government pay scale:87 £26,345, inclusive of pay and NI |
| PE/health education teacher | 22.76/houra | Based on mid-point (m4) on main school pay scale:82£33,288, inclusive of pay and NI |
| Head or senior teacher with leadership responsibilities | 58.35/houra | Based on national leadership and head teacher’s pay scale, 2019. Head Group 4, Spine L27: £85,338, inclusive of NI and pension contributions |
| Non-qualified teaching support staffc | 16.55/houra | Based on salary of £24,201, inclusive of pension and NI |
| Other resource costs | ||
| Travel costs (e.g. car, motoring cost) | 0.45/mile | Expense claims mileage (local government-approved rate) |
| Venue hire | Variable | Receipt of trial expenses |
Outcomes
Health-related utility score measurement in adolescents is difficult because of a lack of validated measures. Although the EuroQol 5-Dimensions (EQ-5D) is a widely used measure for calculating QALYs, there is no UK value set validated for use in children/adolescents. The youth version of the EQ-5D (the EQ-5D-Y)83,84 categorises health on five domains, but has no accompanying value set for scoring. The EQ-5D-Y also includes a visual analogue scale (VAS) that asks respondents to rate their health on a thermometer-like scale from 0 (worst) to 100 (best) health. Another instrument, the CHU-9D, has a value set for calculating utility,85 but was originally developed in primary school-aged children. This has, more recently, been validated in older children and adolescents (i.e. 11- to 17-year-olds),86 but was not collected in this trial.
General HRQoL was also collected using the KIDSCREEN-10 index. 88 Where item responses to trait parameters were complete, KIDSCREEN-10 scale raw scores were based on the sum of item scores (ranging from one to five), where a high value corresponds to a higher HRQoL. Scale raw scores can be transformed into T-values, with scale means around 50 and SDs around 10, again, with higher values corresponding to a higher HRQoL. If there is item-level missingness, the KIDSCREEN-10 can still be scored based on the remaining items. We used a published mapping algorithm,89 validated in adolescents, to indirectly estimate CHU-9D scores and QALYs from the KIDSCREEN-10 responses.
Scope of the within-trial economic evaluation
The PLAN-A intervention has the potential to affect extracurricular physical activity events that girls and families pay for (e.g. sports clubs, gyms). Given our public-sector perspective, we did not cost these activities. Indeed, recall bias between T1 and T0 would have hampered measurement. However, focus groups conducted with girls in intervention schools probed for cost implications of the intervention. If the PLAN-A intervention is effective in increasing physical activity, it may also have an impact on participants’ health-care use. However, we elected not to collect information on short-term health-care use in the trial as we wished to minimise participant burden and because of the high likelihood of recall bias at T1. If PLAN-A results in a sustained increase in MVPA, the long-term impact on health-care use, via the reduced incidence of long-term conditions that are associated with a lack of physical activity, is likely to far outweigh any short-term impact on health-care use.
Cost-effectiveness methods
To assess the cost-effectiveness of the PLAN-A intervention compared with the control group, individual pupil MVPA in intervention and control schools and the school-level incremental costs in intervention schools were calculated. The primary economic outcome for the within-trial economic evaluation was cost per pupil for a unit change in weekday MVPA at T1. This was expressed in terms of cost per additional minute of MVPA, which allows comparison with other, similar studies. 90,91 In addition, we estimated the incremental cost per 5-minute increase in MVPA at T1.
Cost and effectiveness data were combined to calculate an incremental cost-effectiveness ratio (ICER). A non-parametric bootstrapping approach was used to determine the level of sampling uncertainty surrounding the mean ICER by generating 10,000 estimates of incremental costs and benefits, and presenting results on cost-effectiveness acceptability curves (CEACs) and a cost-effectiveness plane (CEP). 92
Our primary analysis was a complete-case analysis. The patterns and potential mechanisms of missingness were examined. We planned to refer to the result relating to the multiple imputation carried out on the primary outcome measure (i.e. weekday MVPA) and to consider secondary analysis using these imputed effect data if imputation was likely to change the decision rule (see Chapter 2, Sensitivity analyses).
A secondary economic analysis took a cost–consequences approach. 93 This presented resource use, disaggregated costs and all trial outcomes in a tabular format, with outcomes and costs kept separate so that a decision-maker can draw their own conclusions on the breadth of evidence.
The exploratory analysis used mapped CHU-9D utilities in a cost–utility analysis (cost per QALY).
Governance
A Trial Management Group (TMG) was established and comprised all applicants, the trial manager, research associate and fieldworker. The TMG met on a regular basis throughout the trial (approximately monthly) to discuss progress, problems, solutions and ethical issues. A TSC was formed to oversee the conduct of the trial; it consisted of an independent chairperson, three independent members, one non-independent member and the research team. The independent members all had experience in developing and conducting complex interventions within schools, trial methodology and statistics, and public health delivery or commissioning. The TSC provided independent scientific scrutiny of the project, guidance on progression to the second follow-up measurement and support to the project team. A Local Advisory Group (LAG) was established, consisting of representatives from the local council, teachers, parents, members from third-sector organisations, Sport England and Women in Sport (London, UK). The LAG provided guidance on practical issues that related to the conduct of the research in schools, school recruitment, roll-out and dissemination. The LAG met three times throughout the project, but were regularly updated on trial progress by the trial manager.
Chapter 3 Trial results
Parts of this chapter have been reproduced with permission from Willis et al. 1 and Jago et al. 2 These are Open Access articles distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: https://creativecommons.org/licenses/by/4.0/. The text below includes minor additions and formatting changes to the original text.
Recruitment
Figure 1 presents the CONSORT diagram and the recruitment and retention to the trial.
FIGURE 1.
The CONSORT flow diagram.
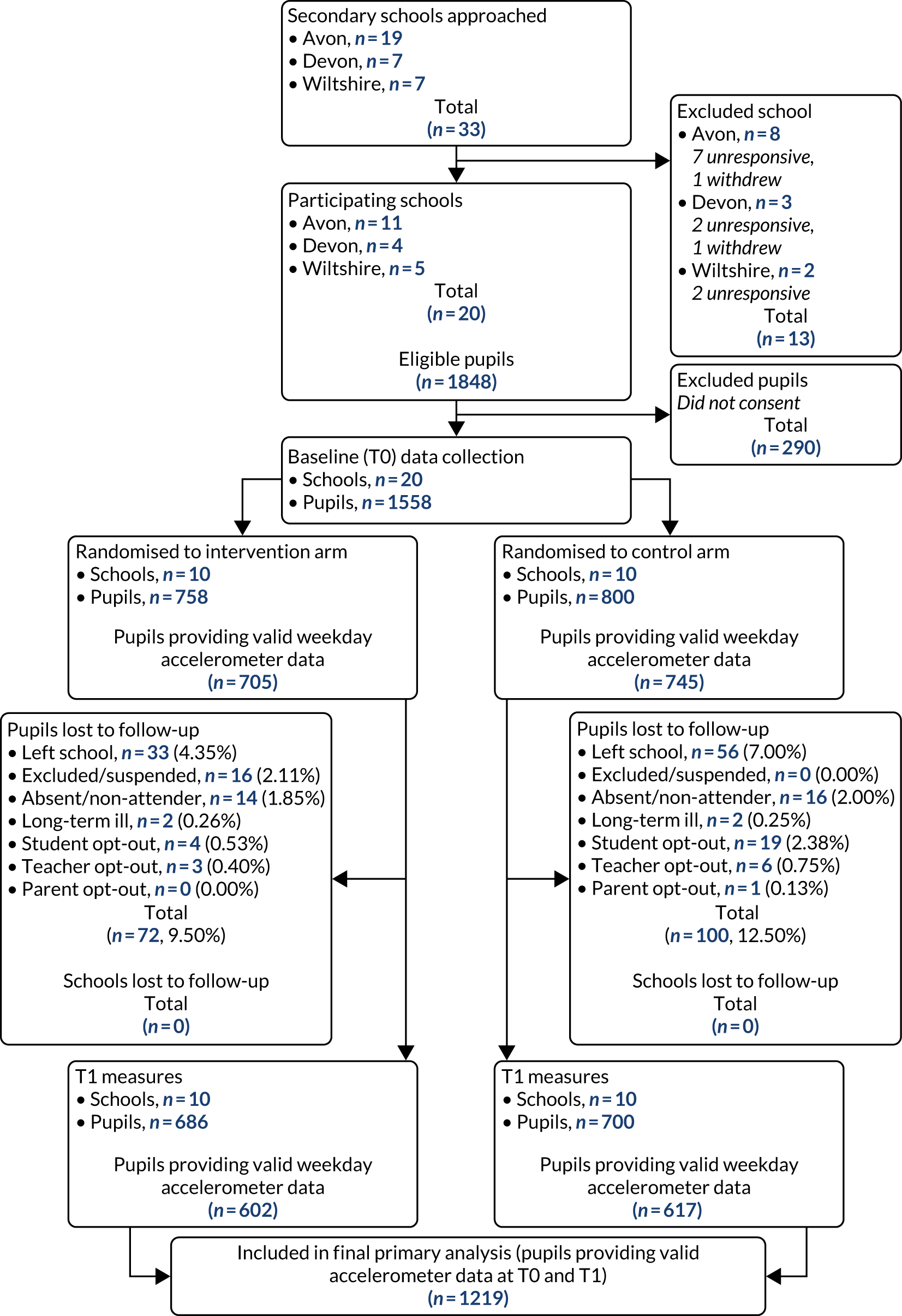
School recruitment and randomisation
Of the 33 schools that were approached to take part, 22 provided a signed school agreement (20 plus two reserve schools). Two schools withdrew before baseline measures and the reserve schools were utilised, ensuring that 20 schools were included. The two schools that withdrew cited staff capacity as the reason for doing so. Schools were grouped into three regions for the purposes of randomisation: Avon (including the local authorities of Bristol, Bath and North East Somerset, North Somerset and South Gloucestershire), Wiltshire and Devon. Table 6 presents the baseline deprivation characteristics of the schools randomised to each trial arm.
| Characteristic | Trial arm | |
|---|---|---|
| Intervention (schools, N = 10) | Control (schools, N = 10) | |
| Area, n (%) | ||
| Avon | 6 (60) | 5 (50) |
| Devon | 2 (20) | 2 (20) |
| Wiltshire | 2 (20) | 3 (30) |
| IMD rank, median (LQ, UQ) | 15,700 (4956, 24,598) | 25,977 (14,154, 30,500) |
| IMD score, median (LQ, UQ) | 19.7 (9.7, 38.5) | 8.6 (4.8, 20.1) |
| IMD quintile | ||
| Median (LQ, UQ) | 3 (1, 4) | 4.5 (3, 5) |
| Quintile 1 (most deprived), n (%) | 4 (40) | 0 (0) |
| Quintile 2, n (%) | 1 (10) | 2 (20) |
| Quintile 3, n (%) | 0 (0) | 2 (20) |
| Quintile 4, n (%) | 3 (30) | 1 (10) |
| Quintile 5 (least deprived), n (%) | 2 (20) | 5 (50) |
Schools in the intervention arm had higher IMD scores than schools in the control arm, with a median and IQR of 3 (1–4) and 4.5 (3–5), respectively.
Participant recruitment
Of the 1848 girls who received the recruitment briefing across all 20 schools, 1558 (84.31%) consented to take part. The mean number of eligible girls in each school was 92.04 (SD 24.23) and the mean number of girls who consented was 77.90 (SD 22.84). Recruitment percentages ranged from 46 to 97, but were comparable between trial arms. Table 7 presents participation rates by school and trial arm. Two schools (one in each arm) had particularly poor consent rates owing to school-specific issues (see Chapter 5, School and participant recruitment). In total, 290 girls did not provide consent to take part and were excluded from trial measures at T0. Of these, 230 opted out (intervention schools, n = 108; control schools, n = 122) and 60 did not participate for other reasons, such as absence, long-term illness, non-attendance or having left the school (intervention arm, n = 38; control arm, n = 22). Table 8 presents reasons for non-consent by school and measurement time point.
| School ID | Total Year 9 girls (N) | Opted out, n (%)a | Did not participate (other reasons), n (%) | Consenting Year 9 girls, n (%) | Invited to be peer supporter, n (%) | Consenting peer supporters, n (%) |
|---|---|---|---|---|---|---|
| 1 | 89 | 10 (11.24) | 1 (1.12) | 78 (87.64) | 19 (21.35) | 14 (15.73) |
| 2 | 78 | 7 (8.97) | 3 (3.85) | 68 (87.18) | 15 (19.23) | 14 (17.95) |
| 3 | 96 | 7 (7.29) | 6 (6.59) | 83 (86.46) | ||
| 4 | 83 | 9 (10.84) | 10 (12.05) | 64 (77.11) | 16 (19.28) | 15 (18.07) |
| 5 | 80 | 10 (12.50) | 3 (3.75) | 67 (83.75) | 17 (21.25) | 16 (20.00) |
| 6 | 64 | 1 (1.56) | 3 (4.69) | 60 (93.75) | ||
| 7 | 112 | 9 (8.04) | 3 (2.68) | 100 (89.29) | 28 (25.00) | 26 (23.21) |
| 8 | 125 | 13 (10.40) | 0 (0.00) | 112 (89.60) | ||
| 9 | 85 | 7 (8.24) | 0 (0.00) | 78 (91.76) | ||
| 10 | 87 | 8 (9.20) | 2 (2.30) | 77 (88.51) | 22 (25.29) | 18 (20.69) |
| 11 | 97 | 2 (2.06) | 1 (1.03) | 94 (96.91) | ||
| 12 | 90 | 4 (4.44) | 3 (3.33) | 83 (92.22) | ||
| 13 | 144 | 68 (47.22) | 0 (0.00) | 76 (52.78) | ||
| 14 | 152 | 7 (4.61) | 3 (1.97) | 142 (93.42) | 28 (18.42) | 22 (14.47) |
| 15 | 82 | 16 (19.51) | 1 (1.22) | 65 (79.27) | 13 (15.85) | 11 (13.41) |
| 16 | 65 | 32 (49.23) | 2 (3.08) | 31 (47.69) | 14 (21.54) | 14 (21.54) |
| 17 | 76 | 0 (0.00) | 10 (13.16) | 66 (86.84) | 19 (25.00) | 16 (21.05) |
| 18 | 83 | 13 (15.66) | 2 (2.41) | 68 (81.93) | ||
| 19 | 97 | 7 (7.22) | 2 (2.06) | 88 (90.72) | ||
| 20 | 63 | 0 (0.00) | 5 (7.94) | 58 (92.06) | ||
| School average, mean (SD) | 92.40 (24.23) | 11.50 (15.02) | 2.85 (2.81) | 77.90 (22.84) | 19.10 (5.38) | 16.60 (4.40) |
| Intervention arm | 904 | 108 (11.95) | 38 (4.20) | 758 (83.85) | 191 (21.13) | 166 (18.36) |
| Control arm | 944 | 122 (12.92) | 22 (2.33) | 800 (84.75) | ||
| Total | 1848 | 230 (12.45) | 60 (3.25) | 1558 (84.31) |
| ID | Arm | Number at T0/T1 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Withdrawals | Parent opt-out | Student opt-out | Teacher opt-out | Left school | Excluded or suspended | Absent or non-attender | Long-term illness or injury | ||
| 01 | I | 11/18 | 6/0 | 4/0 | 0/1 | 0/0 | 0/15 | 1/2 | 0/0 |
| 02 | I | 10/1 | 2/0 | 3/0 | 2/0 | 0/0 | 0/0 | 3/1 | 0/0 |
| 03 | C | 13/0 | 1/0 | 6/0 | 0/0 | 5/0 | 0/0 | 1/0 | 0/0 |
| 04 | I | 19/2 | 2/0 | 7/0 | 0/0 | 1/0 | 0/0 | 6/2 | 3/0 |
| 05 | I | 13/13 | 1/0 | 1/2 | 8/1 | 1/8 | 0/1 | 1/1 | 1/0 |
| 06 | C | 4/5 | 0/0 | 1/1 | 0/1 | 3/3 | 0/0 | 0/0 | 0/0 |
| 07 | I | 12/2 | 7/0 | 1/1 | 1/0 | 0/1 | 0/0 | 2/0 | 1/0 |
| 08 | C | 13/5 | 4/0 | 9/0 | 0/0 | 0/2 | 0/0 | 0/3 | 0/0 |
| 09 | C | 7/9 | 4/0 | 3/7 | 0/1 | 0/1 | 0/0 | 0/0 | 0/0 |
| 10 | I | 10/8 | 4/0 | 3/0 | 1/0 | 0/7 | 0/0 | 2/1 | 0/0 |
| 11 | C | 3/8 | 1/0 | 0/0 | 1/3 | 0/3 | 1/0 | 0/2 | 0/0 |
| 12 | C | 7/9 | 0/0 | 4/0 | 0/0 | 0/4 | 0/0 | 3/5 | 0/0 |
| 13 | C | 68/10 | 8/0 | 2/2 | 58/1 | 0/7 | 0/0 | 0/0 | 0/0 |
| 14 | I | 10/4 | 0/0 | 7/0 | 0/0 | 1/4 | 0/0 | 2/0 | 0/0 |
| 15 | I | 17/12 | 0/0 | 2/0 | 14/1 | 1/10 | 0/0 | 0/1 | 0/0 |
| 16 | I | 34/4 | 0/0 | 32/1 | 0/0 | 0/1 | 0/0 | 2/0 | 0/2 |
| 17 | I | 10/8 | 0/0 | 0/0 | 0/0 | 0/2 | 0/0 | 10/6 | 0/0 |
| 18 | C | 15/22 | 2/0 | 10/8 | 1/0 | 0/9 | 0/0 | 2/3 | 0/2 |
| 19 | C | 9/20 | 2/0 | 4/1 | 1/0 | 1/19 | 0/0 | 1/0 | 0/0 |
| 20 | C | 5/7 | 0/1 | 0/0 | 0/0 | 1/3 | 0/0 | 4/3 | 0/0 |
| Total | 290/167 | 44/1 | 99/23 | 87/9 | 14/84 | 1/16 | 40/30 | 5/4 | |
Peer supporter recruitment
In the intervention arm, 191 girls were invited to be peer supporters and, of those, 166 (86.91%) consented to take part in the study. Peer supporter recruitment rates are presented by school (see Table 7). Recruitment rates of Year 9 girls in intervention schools ranged from 13.41% to 23.21%. Two schools failed to meet the 15% recruitment target: one school because of a miscalculation in the peer nomination process that reduced the number of girls who were invited to be peer supporters (school 15) and the other because of unavoidable absences (school 14). Reasons for non-consent were provided by 17 of the 25 non-consenters and included not wanting to miss important lessons (n = 10) or known absence on the scheduled training dates (n = 4). Only three nominated girls specified that they did not want to become a peer supporter: one did not feel confident enough to fulfil the role, one felt that she was not active herself and the other gave no reason.
Trainer recruitment
Trainers were recruited via local authority networks to utilise a local delivery model. In total, 18 trainers expressed an interest and nine were invited to receive training after availability and suitability checks were applied. Of those nine, two were based in Wiltshire, five were based in Avon and two were based in Devon. The two Devon-based trainers withdrew prior to the training, citing changes in circumstances as a reason, leaving seven participating trainers. Participating trainers were all female, with ages ranging from 23 to 45 years and a range of experience in youth work, drama, yoga, physical activity or a combination of these: five had experience working with young people in a youth work or physical activity context, and the other two had experience of delivering drama or yoga workshops with young people and had both previously worked on PLAN-A as trainers in the feasibility trial. All had or obtained enhanced disclosure and barring services (DBS) checks to work with children for the trial.
Data provision
Baseline and follow-up measures were completed 12 months apart and, at T1, schools were measured 12 months ± 2 weeks after T0 to ensure seasonal consistency across time points. The timing of the measures is displayed in Table 9. Baseline data provision rates were high. Of the 1558 girls who consented to take part in the trial, 1511 (96.92%) provided baseline accelerometer data and 1557 (99.94%) girls provided complete questionnaire data. These completion rates were consistent across intervention and control arms. Participants lost to follow-up totalled 172 (control arm, n = 100; intervention arm, n = 72). Reasons for drop out are presented by school (see Table 8). Follow-up data provision rates were lower, but still > 85% for both accelerometer and questionnaire data, which is better than the age-group norms for research projects using accelerometers. 94 Accelerometer and questionnaire data provision rates by school at each time point are presented in Table 10.
| Measurement | Intervention arm | Control arm |
|---|---|---|
| Baseline | ||
| School sample size | 10 | 10 |
| Pupil sample size | 758 | 800 |
| Accelerometer measurements, n (%) of schools; n (%) of pupils | ||
| October 2018 | 2 (20.00); 142 (18.73) | 0 (0.00); 0 (0.00) |
| November 2018 | 4 (40.00); 293 (38.65) | 4 (40.00); 330 (41.25) |
| December 2018 | 0 (0.00); 0 (0.00) | 2 (20.00); 176 (22.00) |
| January 2019 | 3 (30.00); 233 (30.74) | 2 (20.00); 158 (19.75) |
| February 2019 | 1 (10.00); 64 (8.44) | 2 (20.00); 115 (14.38) |
| Follow-up | ||
| School sample size | 10 | 10 |
| Pupil sample size | 686 | 700 |
| Accelerometer measurements, n (%) of schools; n (%) of pupils | ||
| October 2019 | 2 (20.00); 128 (18.66) | 0 (0.00); 0 (0.00) |
| November 2019 | 3 (30.00); 212 (30.90) | 4 (40.00); 304 (43.43) |
| December 2019 | 1 (10.00); 69 (10.06) | 2 (20.00); 160 (22.86) |
| January 2020 | 2 (20.00); 192 (27.99) | 3 (30.00); 182 (26.00) |
| February 2020 | 2 (20.00); 85 (12.39) | 1 (10.00); 54 (7.71) |
| School ID | Arm | Number of pupils consented | Provided data, n (%) | |||
|---|---|---|---|---|---|---|
| Baseline (T0) accelerometer | Baseline (T0) questionnaire | Follow-up (T1) accelerometer | Follow-up (T1) questionnaire | |||
| 1 | I | 78 | 76 (97.44) | 78 (100.00) | 60 (76.92) | 60 (76.92) |
| 2 | I | 68 | 66 (97.06) | 67 (98.53) | 64 (94.12) | 67 (98.53) |
| 3 | C | 83 | 81 (97.59) | 83 (100.00) | 78 (93.98) | 78 (93.98) |
| 4 | I | 64 | 59 (92.19) | 64 (100.00) | 60 (93.75) | 61 (95.31) |
| 5 | I | 67 | 65 (97.01) | 67 (100.00) | 53 (79.10) | 54 (80.60) |
| 6 | C | 60 | 59 (98.33) | 60 (100.00) | 55 (91.67) | 55 (91.67) |
| 7 | I | 100 | 96 (96.00) | 100 (100.00) | 97 (97.00) | 98 (98.00) |
| 8 | C | 112 | 112 (100.00) | 112 (100.00) | 105 (93.75) | 107 (95.54) |
| 9 | C | 78 | 78 (100.00) | 78 (100.00) | 69 (88.46) | 69 (88.46) |
| 10 | I | 77 | 73 (94.81) | 77 (100.00) | 68 (88.31) | 69 (89.61) |
| 11 | C | 94 | 93 (98.94) | 94 (100.00) | 85 (90.43) | 86 (91.49) |
| 12 | C | 83 | 83 (100.00) | 83 (100.00) | 74 (89.16) | 74 (89.16) |
| 13 | C | 76 | 75 (98.68) | 76 (100.00) | 66 (86.84) | 66 (86.84) |
| 14 | I | 142 | 142 (100.00) | 142 (100.00) | 138 (97.18) | 138 (97.18) |
| 15 | I | 65 | 60 (92.31) | 65 (100.00) | 47 (72.31) | 54 (83.08) |
| 16 | I | 31 | 31 (100.00) | 31 (100.00) | 27 (87.10) | 27 (87.10) |
| 17 | I | 66 | 64 (96.97) | 66 (100.00) | 53 (80.30) | 58 (87.88) |
| 18 | C | 68 | 61 (89.71) | 68 (100.00) | 42 (61.76) | 45 (66.18) |
| 19 | C | 88 | 83 (94.32) | 88 (100.00) | 66 (75.00) | 68 (77.27) |
| 20 | C | 58 | 54 (93.10) | 58 (100.00) | 49 (84.48) | 50 (86.21) |
| All schools | 1558 | 1511 (96.92) | 1557 (99.94) | 1356 (87.03) | 1384 (88.83) | |
| Intervention arm | 758 | 732 (96.44) | 757 (99.87) | 667 (87.99) | 686 (90.50) | |
| Control arm | 800 | 779 (97.38) | 800 (100.00) | 689 (86.13) | 698 (87.25) | |
At baseline, 36 accelerometers were not returned and 11 files were corrupt or recorded no data and were, therefore, labelled ‘invalid’ files. Of the 1511 files available at baseline, 1431 (94.70%) met the inclusion criteria of ≥ 500 minutes of valid wear time on at least two weekdays. At follow-up, 21 accelerometers were not returned and nine files were invalid. Of the 1356 files available at T1, 1219 (89.90%) met the inclusion criteria and were included in the final analysis. Table 11 presents the proportion of participants meeting the accelerometer inclusion criteria by arm at each time point. Missingness is displayed by trial arm in Table 12.
| Inclusion criterion | Control arm | Intervention arm | Overall |
|---|---|---|---|
| Baseline (T0) | |||
| No. of accelerometer files available | 779 | 732 | 1511 |
| Criterion of two or more valid weekdays met?, n (%) | |||
| No | 41 (5.26) | 39 (5.33) | 80 (5.29) |
| Yes | 738 (94.74) | 693 (94.67) | 1431 (94.71) |
| Median (IQR) number of valida days overall | 6 (4–7) | 5 (4–6) | 6 (4–6) |
| Median (IQR) number of valida weekdays | 4 (4–5) | 4 (4–5) | 4 (4–5) |
| Follow-up (T1) | |||
| No. of accelerometer files available | 689 | 667 | 1356 |
| Criteria two or more weekdays met?, n (%) | |||
| No | 72 (10.44) | 65 (9.75) | 137 (10.10) |
| Yes | 617 (89.56) | 602 (90.25) | 1219 (89.90) |
| Median (IQR) number of valida days overall | 5 (3–6) | 5 (3–6) | 5 (3–6) |
| Median (IQR) number of valida weekdays | 4 (3–5) | 4 (3–5) | 4 (3–5) |
| Data type | Intervention arm | Control arm | Total |
|---|---|---|---|
| Baseline (T0) | |||
| Participants (n) | 758 | 800 | 1558 |
| Accelerometer data, n (%) | |||
| Returned with data | 732 (96.57) | 779 (97.38) | 1511 (96.98) |
| Returned corrupt/with no data | 8 (1.06) | 3 (0.38) | 11 (0.71) |
| Not returned | 18 (2.37) | 18 (2.25) | 36 (2.31) |
| Complete questionnaire data, n (%) | |||
| PLAN-A survey | 757 (99.87) | 800 (100.00) | 1557 (99.94) |
| KIDSCREEN-10 | 757 (99.87) | 800 (100.00) | 1557 (99.94) |
| EQ-5D-Y | 757 (99.87) | 800 (100.00) | 1557 (99.94) |
| Missing/incomplete questionnaire data | 1 (0.13) | 0 (0.00) | 1 (0.06) |
| Follow-up (T1) | |||
| Withdrawals, n (%) | 72 (9.50) | 100 (12.50) | 172 (11.04) |
| Participants (n) | 686 | 700 | 1386 |
| Accelerometer data, n (%)a | |||
| Returned with data | 667 (97.23) | 689 (98.43) | 1356 (97.84) |
| Returned corrupt/with no data | 3 (0.44) | 6 (0.86) | 9 (0.65) |
| Not returned | 16 (2.33) | 5 (0.71) | 21 (1.52) |
| Complete questionnaire data, n (%)a | |||
| PLAN-A survey | 686 (100.00) | 698 (99.71) | 1384 (99.86) |
| KIDSCREEN-10 | 686 (100.00) | 698 (99.71) | 1384 (99.86) |
| EQ-5D-Y | 686 (100.00) | 698 (99.71) | 1384 (99.86) |
| Missing/incomplete questionnaire data, n (%) | 0 (0.00) | 2 (0.29) | 2 (0.14) |
Baseline data
Participant-level baseline data split by treatment arm are presented in Table 13. Overall, the trial arms were well balanced; however, the distribution of participants between the three geographical areas differed slightly. IMD scores were slightly higher in the intervention arm than the control arm, and the proportion of students claiming free school meals was slightly larger, suggesting a slight imbalance in deprivation, favouring the control arm. Accelerometer-assessed weekday and weekend physical activity scores were very similar between arms, with both groups achieving, on average, 51 minutes of weekday MVPA and 31% of each group meeting the Chief Medical Officer (CMO)’s guidelines of an average of 60 minutes of MVPA on weekdays. 9 Active travel to and from school was more prevalent in the control arm than the intervention arm. Psychosocial variables were balanced between arms. The KIDSCREEN-10 T-scores, reflecting HRQoL, were balanced between arms, but were notably lower than the UK norm values for girls aged 12–18 years. 95
| Variable | Intervention arm (N = 758 pupils) | Control arm (N = 800 pupils) |
|---|---|---|
| Sociodemographic characteristics | ||
| Age, n, mean (SD) | 624, 13.80 (0.33) | 687, 13.80 (0.31) |
| Area, n (%) | ||
| Avon | 387 (51.06) | 381 (47.63) |
| Devon | 207 (27.31) | 164 (20.50) |
| Wiltshire | 164 (21.64) | 255 (31.88) |
| Ethnicity, n (%) | ||
| White | 659 (87.52) | 716 (89.50) |
| Mixed | 54 (7.17) | 54 (6.75) |
| Asian/Asian British | 19 (2.52) | 16 (2.00) |
| Black/African/Caribbean/black British | 20 (2.66) | 13 (1.63) |
| Othera | 1 (0.13) | 1 (0.13) |
| IMD | ||
| Rank, n, median (IQR) | 674, 17,302 (7982–23,172) | 741, 20,689 (14,366–26,917) |
| Score, n, median (IQR) | 674, 16.39 (10.86–30.52) | 741, 12.98 (7.86–19.87) |
| Quintile, n (%) | ||
| 1 (most deprived) | 145 (21.51) | 65 (8.77) |
| 2 | 111 (16.47) | 99 (13.36) |
| 3 | 149 (22.11) | 172 (23.21) |
| 4 | 166 (24.63) | 200 (26.99) |
| 5 (least deprived) | 103 (15.28) | 205 (27.67) |
| Family affluence, n, mean (SD) | 758, 6.67 (1.89) | 800, 7.01 (1.68) |
| Receiving free school meals, n (%) | ||
| No | 637 (84.59) | 734 (91.75) |
| Yes | 106 (14.08) | 61 (7.63) |
| Rather not say | 10 (1.33) | 5 (0.63) |
| Measures of physical activity | ||
| MVPA (minutes), n, mean (SD) | ||
| Weekday | 693, 51.03 (20.47) | 738, 51.41 (20.10) |
| Weekend | 496, 34.37 (25.42) | 526, 35.71 (27.09) |
| Overall | 693, 47.67 (18.38) | 738, 48.33 (18.57) |
| Sedentary time (minutes), n, mean (SD) | ||
| Weekday | 693, 590.80 (93.74) | 738, 591.73 (92.82) |
| Weekend | 496, 527.12 (110.06) | 526, 521.05 (101.08) |
| Overall | 693, 574.51 (85.54) | 738, 575.64 (84.24) |
| An average of at least 60 minutes MVPA per day across weekdays, n provided data, n in group (%) | 732, 228 (31.15) | 779, 242 (31.07) |
| An average of at least 60 minutes MVPA per day across weekend days; n provided data, n in group (%) | 732, 81 (11.07) | 779, 77 (9.88) |
| Travel mode to school, n (%) | ||
| Walk | 365 (48.28) | 459 (57.38) |
| Cycle | 13 (1.72) | 8 (1.00) |
| Car | 227 (30.03) | 216 (27.00) |
| Bus/train | 151 (19.97) | 117 (14.63) |
| Travel mode from school, n (%) | ||
| Walk | 428 (56.61) | 521 (65.13) |
| Cycle | 13 (1.72) | 7 (0.88) |
| Car | 153 (20.24) | 137 (17.13) |
| Bus/train | 162 (21.43) | 135 (16.88) |
| Psychosocial variables, n, mean (SD) | ||
| Self-esteem | 729, 4.30 (1.10) | 773, 4.38 (1.11) |
| Autonomous motivation | 740, 2.49 (0.99) | 788, 2.49 (1.01) |
| Controlled motivation | 749, 1.36 (0.81) | 795, 1.30 (0.82) |
| Amotivation | 750, 0.47 (0.72) | 791, 0.43 (0.68) |
| Autonomy need satisfaction | 747, 5.08 (1.39) | 795, 5.14 (1.38) |
| Competence need satisfaction | 753, 4.48 (1.58) | 795, 4.39 (1.58) |
| Relatedness need satisfaction | 743, 4.80 (1.73) | 788, 4.84 (1.75) |
| Physical activity self-efficacy | 744, 1.38 (0.42) | 795, 1.40 (0.44) |
| Peer physical activity norm: importance | 755, 1.44 (0.86) | 799, 1.49 (0.89) |
| Peer physical activity norm: acceptance | 755, 1.21 (0.75) | 798, 1.21 (0.71) |
| Peer physical activity norm: prevalence | 754, 1.47 (0.63) | 796, 1.47 (0.64) |
| Physical activity social support from friends | 751, 1.45 (0.68) | 789, 1.41 (0.64) |
| KIDSCREEN-10 (T-score) | 755, 39.97 (9.48) | 799, 40.09 (9.40) |
| KIDSCREEN-10 (R-score) | 755, 0.54 (0.97) | 799, 0.55 (0.96) |
| EQ-5D-Y | 752, 0.75 (0.27) | 797, 0.75 (0.27) |
| EQ-5D-Y VAS | 731, 70.62 (19.89) | 783, 70.10 (20.11) |
Table 14 presents baseline characteristics of the girls in all 20 schools who were nominated by their peers to be peer supporters, compared with the characteristics of the rest of the sample. Demographically, there was balance between peer supporters and non-peer supporters (those who were not nominated). Peer supporters recorded more daily MVPA across the week than non-peer supporters by ≈ 4 minutes per day (51.01 ± 17.99 vs. 47.11 ± 18.53 minutes); however, sedentary time was very similar. A larger proportion of nominated peer supporters than of non-peer supporters achieved the CMO guidelines on weekdays (35.84% vs. 27.70%). Travel mode to and from school was similar. Peer supporters reported slightly higher self-esteem, physical activity-based autonomous motivation, need satisfaction and KIDSCREEN-10 T-scores than non-peer supporters.
| Variable | Non-peer supporters (N = 1201 pupils) | Peer supporters (N = 357 pupils) |
|---|---|---|
| Sociodemographic characteristics | ||
| Age, n, mean (SD) | 994, 13.79 (0.32) | 317, 13.83 (0.31) |
| Area, n (%) | ||
| Avon | 591 (49.21) | 177 (49.58) |
| Devon | 293 (24.40) | 78 (21.85) |
| Wiltshire | 317 (26.39) | 102 (28.57) |
| Ethnicity, n (%) | ||
| White | 1058 (88.39) | 317 (89.04) |
| Mixed | 79 (6.60) | 29 (8.15) |
| Asian/Asian British | 29 (2.42) | 6 (1.69) |
| Black/African/Caribbean/black British | 29 (2.42) | 4 (1.12) |
| Othera | 2 (0.17) | 0 (0.00) |
| IMD | ||
| Rank, n, median (IQR) | 1084, 19,197 (10,613–25,553) | 331, 19,267 (10,041–25,093) |
| Score, n, median (IQR) | 1084, 14.44 (8.92–25.43) | 331, 14.37 (9.30–26.45) |
| Quintile, n (%) | ||
| 1 (most deprived) | 161 (14.85) | 49 (14.80) |
| 2 | 161 (14.85) | 49 (14.80) |
| 3 | 248 (22.88) | 73 (22.05) |
| 4 | 277 (25.55) | 89 (26.89) |
| 5 (least deprived) | 237 (21.86) | 71 (21.45) |
| Family affluence, n, mean (SD) | 1201, 6.77 (1.82) | 357, 7.12 (1.66) |
| Receiving free school meals, n (%) | ||
| No | 1047 (87.47) | 324 (91.01) |
| Yes | 137 (11.45) | 30 (8.43) |
| Rather not say | 13 (1.09) | 2 (0.56) |
| Measures of physical activity | ||
| MVPA (minutes), n, mean (SD) | ||
| Weekday | 1101, 50.45 (20.36) | 330, 53.78 (19.79) |
| Weekend | 781, 32.98 (25.54) | 241, 41.80 (27.58) |
| Overall | 1101, 47.11 (18.53) | 330, 51.01 (17.99) |
| Sedentary time (minutes), n, mean (SD) | ||
| Weekday | 1101, 592.70 (95.26) | 330, 586.53 (86.12) |
| Weekend | 781, 526.95 (105.96) | 241, 514.40 (103.74) |
| Overall | 1101, 576.39 (86.88) | 330, 570.77 (77.65) |
| An average of at least 60 minutes MVPA per day on weekdays, n provided data, n in group (%) | 1165, 346 (27.70) | 346, 124 (35.84) |
| An average of at least 60 minutes MVPA per day on weekend days, n provided data, n in group (%) | 1165, 105 (9.01) | 346, 53 (15.32) |
| Travel mode to school, n (%) | ||
| Walk | 631 (52.63) | 193 (54.06) |
| Cycle | 19 (1.58) | 2 (0.56) |
| Car | 335 (27.94) | 108 (30.25) |
| Bus/train | 214 (17.85) | 54 (15.13) |
| Travel mode from school, n (%) | ||
| Walk | 723 (60.30) | 226 (63.31) |
| Cycle | 18 (1.50) | 2 (0.56) |
| Car | 226 (18.85) | 64 (17.93) |
| Bus/train | 232 (19.35) | 65 (18.21) |
| Psychosocial variables, n, mean (SD) | ||
| Self-esteem | 1159, 4.24 (1.12) | 343, 4.68 (0.99) |
| Autonomous motivation | 1177, 2.34 (0.98) | 351, 3.00 (0.88) |
| Controlled motivation | 1190, 1.32 (0.83) | 354, 1.37 (0.74) |
| Amotivation | 1185, 0.51 (0.73) | 356, 0.25 (0.56) |
| Autonomy need satisfaction | 1185, 4.96 (1.39) | 357, 5.61 (1.22) |
| Competence need satisfaction | 1194, 4.19 (1.54) | 354, 5.24 (1.44) |
| Relatedness need satisfaction | 1177, 4.66 (1.76) | 354, 5.36 (1.55) |
| Physical activity self-efficacy | 1188, 1.35 (0.44) | 351, 0.53 (0.38) |
| Peer physical activity norm: importance | 1198, 1.40 (0.86) | 356, 1.65 (0.92) |
| Peer physical activity norm: acceptance | 1198, 1.18 (0.74) | 355, 1.32 (0.70) |
| Peer physical activity norm: prevalence | 1193, 1.42 (0.64) | 357, 1.63 (0.61) |
| Physical activity social support from friends | 1188, 1.38 (0.67) | 352, 1.60 (0.59) |
| KIDSCREEN-10 (T-score) | 1197, 39.35 (9.24) | 357, 42.30 (9.74) |
| KIDSCREEN-10 (R-score) | 1197, 0.48 (0.94) | 357, 0.78 (1.00) |
| EQ-5D-Y | 1193, 0.73 (0.28) | 356, 0.79 (0.24) |
| EQ-5D-Y VAS | 1164, 68.75 (20.39) | 350, 75.69 (17.65) |
Baseline characteristics of participants who did or did not provide weekday physical activity data at T0 (Table 15) and T1 (Table 16) reflect that, in both comparisons, those who failed to provide usable weekday physical activity data had slightly higher IMD scores (a larger proportion were in the most deprived quintile and a smaller proportion were in the least deprived quintile, and more were claiming free school meals). Those missing weekday MVPA data at baseline presented very slightly, but consistently, lower scores on all psychosocial variables, except for physical activity-related amotivation. They also walked home from school more and used public transport for the journey home less often. The same pattern was observed among those for whom MVPA data were missing at T1.
| Variable | Missing data (N = 127 pupils) | Non-missing data (N = 1431 pupils) |
|---|---|---|
| Sociodemographic characteristics | ||
| Age, n, mean (SD) | 59, 13.87 (0.29) | 1225, 13.80 (0.32) |
| Area, n (%) | ||
| Avon | 70 (55.12) | 698 (48.78) |
| Devon | 27 (21.26) | 344 (24.04) |
| Wiltshire | 30 (23.62) | 389 (27.18) |
| Ethnicity, n (%) | ||
| White | 114 (89.76) | 1261 (88.43) |
| Mixed | 9 (7.09) | 99 (6.94) |
| Asian/Asian British | 1 (0.79) | 34 (2.38) |
| Black/African/Caribbean/black British | 3 (2.36) | 30 (2.10) |
| Othera | 0 (0.00) | 2 (0.14) |
| IMD | ||
| Rank, n, median (IQR) | 109, 16,649 (9400–23,172) | 1306, 19,348 (10,935–25,747) |
| Score, n, median (IQR) | 109, 17.12 (10.86–27.60) | 1306, 14.29 (8.77–24.89) |
| Quintile, n (%) | ||
| 1 (most deprived) | 18 (16.51) | 192 (14.70) |
| 2 | 24 (22.02) | 186 (14.24) |
| 3 | 23 (21.10) | 298 (22.82) |
| 4 | 39 (35.78) | 337 (25.80) |
| 5 (least deprived) | 15 (13.76) | 293 (22.43) |
| Family affluence, n, mean (SD) | 127, 6.73 (1.68) | 1431, 6.86 (1.80) |
| Receiving free school meals, n (%) | ||
| No | 102 (80.31) | 1269 (88.99) |
| Yes | 22 (17.32) | 145 (10.17) |
| Rather not say | 3 (2.36) | 12 (0.84) |
| Measures of physical activity | ||
| Travel mode to school, n (%) | ||
| Walk | 69 (54.33) | 755 (52.83) |
| Cycle | 0 (0.00) | 21 (1.47) |
| Car | 43 (33.86) | 400 (27.99) |
| Bus/train | 15 (11.81) | 253 (17.70) |
| Travel mode from school, n (%) | ||
| Walk | 90 (70.87) | 859 (60.11) |
| Cycle | 0 (0.00) | 20 (1.40) |
| Car | 22 (17.32) | 268 (18.75) |
| Bus/train | 15 (11.81) | 282 (19.73) |
| Psychosocial variables, n, mean (SD) | ||
| Self-esteem | 123, 4.01 (1.15) | 1379, 4.37 (1.10) |
| Autonomous motivation | 121, 2.15 (1.07) | 1407, 2.52 (0.99) |
| Controlled motivation | 125, 1.21 (0.89) | 1419, 1.34 (0.81) |
| Amotivation | 125, 0.57 (0.78) | 1416, 0.44 (0.69) |
| Autonomy need satisfaction | 126, 4.82 (1.38) | 1416, 5.14 (1.38) |
| Competence need satisfaction | 127, 4.15 (1.61) | 1421,4.46 (1.57) |
| Relatedness need satisfaction | 124, 4.56 (1.78) | 1407, 4.84 (1.74) |
| Physical activity self-efficacy | 126, 1.30 (0.47) | 1413, 1.40 (0.43) |
| Peer physical activity norm: importance | 127, 1.31 (0.83) | 1427, 1.47 (0.88) |
| Peer physical activity norm: acceptance | 127, 1.20 (0.81) | 1426, 1.21 (0.72) |
| Peer physical activity norm: prevalence | 126, 1.36 (0.69) | 1424, 1.48 (0.63) |
| Physical activity social support from friends | 122, 1.43 (0.69) | 1418, 1.43 (0.66) |
| KIDSCREEN-10 (T-score) | 127, 38.56 (8.45) | 1427, 40.16 (9.51) |
| KIDSCREEN-10 (R-score) | 127, 0.40 (0.86) | 1427, 0.56 (0.97) |
| EQ-5D-Y | 127, 0.74 (0.27) | 1422, 0.75 (0.27) |
| EQ-5D-Y VAS | 119, 66.79 (21.19) | 1395, 70.65 (19.87) |
| Variable | Missing (N = 339 pupils) | Non-missing (N = 1219 pupils) |
|---|---|---|
| Sociodemographic characteristics | ||
| Age, n, mean (SD) | 146, 13.81 (0.31) | 1138, 13.80 (0.32) |
| Area, n (%) | ||
| Avon | 193 (56.93) | 575 (47.17) |
| Devon | 87 (25.66) | 284 (23.30) |
| Wiltshire | 59 (17.40) | 360 (29.53) |
| Ethnicity, n (%) | ||
| White | 298 (87.91) | 1077 (88.71) |
| Mixed | 29 (8.55) | 79 (6.51) |
| Asian/Asian British | 4 (1.18) | 31 (2.55) |
| Black/African/Caribbean/black British | 7 (2.06) | 26 (2.1) |
| Othera | 1 (0.29) | 1 (0.08) |
| IMD | ||
| Rank, n, median (IQR) | 301, 15,981 (7390–22,257) | 1114, 19,717 (12,024–26,041) |
| Score, n, median (IQR) | 301, 17.90 (11.61–31.81) | 1114, 13.92 (8.56–23.03) |
| Quintile, n (%) | ||
| 1 (most deprived) | 66 (21.93) | 144 (12.93) |
| 2 | 54 (17.94) | 156 (14.00) |
| 3 | 69 (22.92) | 252 (22.62) |
| 4 | 73 (24.25) | 293 (26.30) |
| 5 (least deprived) | 39 (12.96) | 269 (24.15) |
| Family affluence, n, mean (SD) | 339, 6.60 (1.91) | 1219, 6.92 (1.75) |
| Receiving free school meals, n (%) | ||
| Yes | 69 (20.35) | 98 (8.07) |
| No | 264 (77.88) | 1107 (91.19) |
| Rather not say | 6 (1.77) | 9 (0.74) |
| Measures of physical activity | ||
| MVPA (minutes), n, mean (SD) | ||
| Weekday | 268, 49.83 (20.93) | 1163, 51.54 (20.11) |
| Weekend | 148, 39.89 (32.94) | 874, 34.24 (24.92) |
| Overall | 268, 47.90 (19.70) | 1163, 48.03 (18.19) |
| Sedentary time (minutes), n, mean (SD) | ||
| Weekday | 268, 555.19 (100.30) | 1163, 599.60 (89.54) |
| Weekend | 148, 501 (112.72) | 874, 527.73 (103.86) |
| Overall | 268, 543.94 (92.79) | 1163, 582.27 (81.27) |
| An average of at least 60 minutes MVPA per day on weekdays, n provided data, n in group (%) | 313, 103 (32.91) | 1198, 367 (30.63) |
| An average of at least 60 minutes MVPA per day on weekend days, n provided data, n in group (%) | 313, 37 (11.82) | 1198, 121 (10.10) |
| Travel mode to school, n (%) | ||
| Walk | 178 (52.51) | 646 (53.08) |
| Cycle | 3 (0.88) | 18 (1.48) |
| Car | 107 (31.56) | 336 (27.61) |
| Bus/train | 51 (15.04) | 217 (17.83) |
| Travel mode from school, n (%) | ||
| Walk | 227 (66.96) | 722 (59.33) |
| Cycle | 3 (0.88) | 17 (1.40) |
| Car | 57 (16.81) | 233 (19.15) |
| Bus/train | 52 (15.34) | 245 (20.13) |
| Psychosocial variables, n, mean (SD) | ||
| Self-esteem | 319, 4.17 (1.14) | 1183, 4.39 (1.09) |
| Autonomous motivation | 324, 2.27 (1.08) | 1204, 2.55 (0.97) |
| Controlled motivation | 333, 1.20 (0.85) | 1211, 1.36 (0.80) |
| Amotivation | 331, 0.50 (0.75) | 1210, 0.43 (0.69) |
| Autonomy need satisfaction | 335, 4.91 (1.44) | 1207, 5.16 (1.36) |
| Competence need satisfaction | 336, 4.27 (1.60) | 1212, 4.48 (1.57) |
| Relatedness need satisfaction | 332, 4.51 (1.79) | 1199, 4.90 (1.72) |
| Physical activity self-efficacy | 332, 1.38 (0.43) | 1207, 1.39 (0.43) |
| Peer physical activity norm: importance | 339, 1.32 (0.87) | 1215, 1.50 (0.88) |
| Peer physical activity norm: acceptance | 339, 1.14 (0.78) | 1214, 1.23 (0.72) |
| Peer physical activity norm: prevalence | 336, 1.33 (0.65) | 1214, 1.51 (0.63) |
| Physical activity social support from friends | 333, 1.37 (0.69) | 1207, 1.45 (0.65) |
| KIDSCREEN-10 (T-score) | 338, 38.30 (9.40) | 1216, 40.51 (9.39) |
| KIDSCREEN-10 (R-score) | 338, 0.37 (0.96) | 1216, 0.60 (0.96) |
| EQ-5D-Y | 338, 0.71 (0.29) | 1211, 0.76 (0.26) |
| EQ-5D-Y VAS | 321, 68.04 (21.83) | 1193, 70.97 (19.44) |
Primary outcome
The primary outcome of this trial was accelerometer-measured minutes of weekday MVPA at T1, 5–6 months after the end of the 10-week intervention period. Table 17 presents the primary outcome analysis using an ITT regression approach. After adjustment for baseline weekday MVPA, the number of days of valid data and the stratification variables (i.e. area and weighted IMD), the difference between arms was estimated as –2.84 (95% CI –5.94 to 0.25; p = 0.071) minutes, meaning that no statistically meaningful difference was found between the two groups. After additional adjustment for imbalanced variables at baseline (i.e. free school meals, travel mode to and from school, and IMD quintile), the difference increased to –3.57 (95% CI –6.75 to –0.39; p = 0.028) minutes in a negative direction. When adjusting further for the month that MVPA measurements were taken to account for seasonality, the difference in means across the intervention and control arms decreased to –2.96 (95% CI –5.98 to 0.062; p = 0.055) minutes and is, once again, not statistically meaningful. With a CI spanning zero, this would suggest weak to no evidence of a negative treatment effect that is ameliorated by seasonality.
| Outcome | Mean (SD or 95% CI) | p-value |
|---|---|---|
| Mean MVPA (minutes), mean (SD) | ||
| Intervention arm (n = 603) | 45.19 (18.43) | |
| Control arm (n = 616) | 48.89 (20.85) | |
| Difference in MVPA (minutes), mean (95% CI) | ||
| ITT analysis adjusted for baseline mean weekday MVPA, the number of days of valid data and the stratification variables | –2.84 (–5.94 to 0.25) | 0.071 |
| ITT analysis adjusted further for additional variables that show an imbalance between groups at baseline | –3.57 (–6.75 to –0.39) | 0.028 |
| ITT analysis adjusted further for month in which MVPA measurement was taken | –2.96 (–5.98 to 0.062) | 0.055 |
The primary analysis was rerun to assess the sensitivity of the results to missing data. As demonstrated in Table 16, most baseline characteristics were comparable between those with and without missing MVPA data at T1. The group that diverged furthest from the mean SEP (i.e. IMD score) was that with missing follow-up data; participants in this group were more likely to come from socioeconomically deprived areas. Missing MVPA at follow-up was estimated using MICE. The imputation model included treatment arm, baseline weekday MVPA, the number of days of valid data, region, school-level IMD score, whether or not the child received free school meals at baseline, how the child travelled to school at baseline and IMD score based on home postcode. When comparing the primary analysis using complete cases with the analysis using the imputed data (Table 18), the between-group difference was smaller in the latter analysis and its CI included the null. These results are, of course, subject to assumptions inherent to the multiple imputation approach: chiefly, that the incomplete MVPA data are missing at random such that the missingness is associated with the observed data only.
| Analysis | n | Difference in meansa | 95% CI | p-value |
|---|---|---|---|---|
| Complete case | 1062 | –3.57 | –6.75 to –0.39 | 0.028 |
| Multiple imputation | 1558 | –2.54 | –5.67 to 0.59 | 0.110 |
We can conclude that, in this trial, the PLAN-A intervention was not associated with an increase in weekday MVPA in 13- to 14-year-old girls compared with usual practice.
Secondary outcomes
This trial also set out to determine the effectiveness of PLAN-A to improve four secondary outcomes, as listed in Chapter 2, Analysis of intervention effect. No statistically meaningful difference was observed at T1 between arms in minutes of weekend MVPA or weekday or weekend sedentary time or self-esteem scores (Table 19). The normality of the weekend MVPA data was improved when data were log-transformed. Analysis of weekend MVPA was therefore conducted using log-transformed data. The ratio of geometric means is presented, with 95% CIs and p-values.
| Variable | Control arm | Intervention arm | Difference in means (95% CI) | Ratio of geometric means (95% CI) | p-value | ||
|---|---|---|---|---|---|---|---|
| n | Mean (SD) | n | Mean (SD) | ||||
| Mean weekend MVPA (minutes) | 386 | 35.66 (31.68) | 347 | 41.50 (55.57) | – | 0.94 (0.76 to 1.16)a | 0.558 |
| – | 0.95 (0.78 to 1.15)b | 0.582 | |||||
| Mean weekday sedentary time (minutes) | 616 | 589.95 (96.70) | 603 | 595.88 (100.28) | 2.51 (–12.37 to 17.38)c | – | 0.741 |
| 8.61 (–2.58 to 19.81)d | – | 0.132 | |||||
| Mean weekend sedentary time (minutes) | 386 | 535.79 (115.78) | 347 | 528.45 (122.56) | 3.44 (–22.03 to 28.91)c | – | 0.791 |
| 0.65 (–22.96 to 24.26)d | – | 0.957 | |||||
| Mean self-esteem score | 677 | 4.15 (1.11) | 669 | 4.14 (1.19) | 0.022 (–0.11 to 0.16)e | – | 0.741 |
| 0.022 (–0.13 to 0.18)d | – | 0.778 | |||||
Mediation analyses
Table 20 presents the mean scores of each motivational construct considered as a potential mediator by arm and measurement time point. Potential mediators were balanced between arms and decreased equally between T0 and T1. No meaningful correlations between potential mediators and the primary outcome were observed (Table 21), nor was there evidence of mediation, as the CI of the average causal mediated effect (ACME) for each potential mediator included zero (Table 22).
| Variable | Intervention arm | Control arm | ||
|---|---|---|---|---|
| n | Mean (SD) | n | Mean (SD) | |
| Physical activity motivation: autonomous | ||||
| T0 | 731 | 2.49 (0.99) | 779 | 2.49 (1.01) |
| T1 | 677 | 2.39 (1.02) | 687 | 2.35 (1.01) |
| Physical activity motivation: controlled | ||||
| T0 | 739 | 1.35 (0.81) | 786 | 1.31 (0.82) |
| T1 | 681 | 1.35 (0.85) | 692 | 1.37 (0.84) |
| Physical activity psychological need satisfaction: autonomy | ||||
| T0 | 737 | 5.08 (1.39) | 786 | 5.14 (1.37) |
| T1 | 675 | 4.89 (1.32) | 696 | 4.97 (1.35) |
| Physical activity psychological need satisfaction: competence | ||||
| T0 | 743 | 4.49 (1.58) | 786 | 4.38 (1.58) |
| T1 | 678 | 4.31 (1.49) | 690 | 4.12 (1.49) |
| Physical activity psychological need satisfaction: relatedness | ||||
| T0 | 733 | 4.80 (1.74) | 779 | 4.83 (1.75) |
| T1 | 681 | 4.68 (1.75) | 686 | 4.64 (1.71) |
| Physical activity self-efficacy | ||||
| T0 | 734 | 1.38 (0.42) | 786 | 1.40 (0.44) |
| T1 | 675 | 1.29 (0.47) | 684 | 1.31 (0.46) |
| Physical activity social support | ||||
| T0 | 741 | 1.46 (0.68) | 781 | 1.41 (0.64) |
| T1 | 679 | 1.33 (0.65) | 691 | 1.25 (0.66) |
| Peer norms for physical activity: prevalence | ||||
| T0 | 744 | 1.48 (0.63) | 787 | 1.47 (0.64) |
| T1 | 681 | 1.35 (0.66) | 697 | 1.38 (0.68) |
| Peer norms for physical activity: importance | ||||
| T0 | 745 | 1.44 (0.86) | 790 | 1.49 (0.89) |
| T1 | 681 | 1.34 (0.85) | 693 | 1.30 (0.87) |
| Peer norms for physical activity: acceptance | ||||
| T0 | 745 | 1.22 (0.74) | 789 | 1.21 (0.71) |
| T1 | 676 | 1.11 (0.76) | 695 | 1.09 (0.73) |
| Mediator | T0 | T1 |
|---|---|---|
| Physical activity motivation: autonomous | 0.1228 | 0.0703 |
| Physical activity motivation: controlled | –0.0003 | 0.0132 |
| Physical activity psychological need satisfaction: autonomy | 0.0945 | 0.0185 |
| Physical activity psychological need satisfaction: competence | 0.1046 | 0.0557 |
| Physical activity psychological need satisfaction: relatedness | 0.0369 | 0.0338 |
| Physical activity self-efficacy | 0.0844 | 0.0589 |
| Physical activity social support | 0.0529 | 0.041 |
| Peer norms for physical activity: prevalence | 0.0553 | 0.0597 |
| Peer norms for physical activity: importance | 0.0184 | 0.0242 |
| Peer norms for physical activity: acceptance | 0.0459 | 0.0073 |
| Outcome at T1 | Mediator | Average direct effect (95% CI) | ACME (95% CI) | Total effect (95% CI) | Proportion of effect mediated, % (95% CI) |
|---|---|---|---|---|---|
| Weekday MVPA | Physical activity motivation: autonomous | –2.68 (–4.56 to –0.74) | –0.04 (–0.19 to 0.04) | –2.72 (–4.56 to –0.79) | 0.01 (0.01 to 0.05) |
| Physical activity motivation: controlled | –2.57 (–4.45 to –0.64) | 0.02 (–0.06 to 0.13) | –2.55 (–4.43 to –0.58) | –0.01 (–0.02 to 0.00) | |
| Physical activity psychological need satisfaction: autonomy | –2.74 (–4.62 to –0.80) | 0.01 (–0.08 to 0.12) | –2.73 (–4.60 to –0.76) | 0.00 (–0.01 to 0.00) | |
| Physical activity psychological need satisfaction: competence | –2.58 (–4.46 to –0.64) | –0.03 (–0.22 to 0.11) | –2.61 (–4.46 to –0.68) | 0.01 (0.01 to 0.05) | |
| Physical activity psychological need satisfaction: relatedness | –2.77 (–4.65 to –0.83) | 0.00 (–0.10 to 0.09) | –2.76 (–4.62 to –0.83) | 0.00 (0.00 to 0.00) | |
| Physical activity self-efficacy | –2.85 (–4.74 to –0.91) | 0.00 (–0.09 to 0.06) | –2.86 (–4.73 to –0.90) | 0.00 (0.00 to 0.00) | |
| Physical activity social support | –2.73 (–4.62 to –0.79) | 0.02 (–0.13 to 0.15) | –2.72 (–4.57 to –0.79) | –0.01 (–0.02 to 0.00) | |
| Peer norms for physical activity: prevalence | –2.59 (–4.47 to –0.65) | –0.02 (–0.15 to 0.05) | –2.61 (–4.46 to –0.68) | 0.01 (0.00 to 0.03) | |
| Peer norms for physical activity: importance | –2.72 (–4.60 to –0.79) | –0.02 (–0.16 to 0.07) | –2.74 (–4.60 to –0.81) | 0.01 (0.00 to 0.02) | |
| Peer norms for physical activity: acceptance | –2.58 (–4.46 to –0.65) | –0.02 (–0.16 to 0.09) | –2.60 (–4.46 to –0.66) | 0.01 (0.00 to 0.02) |
The average direct effect is the effect of the intervention on weekday MVPA that is not explained by the mediators (i.e. the amount of the total effect that is not explained by the mediator). The ACME is the effect of the intervention on the weekday MVPA that is explained by the mediator (i.e. the amount of the total effect that can be explained by the mediator). For instance, the row ‘Physical activity motivation: autonomous’ in Table 22 indicates that 1% of the intervention effect on MVPA is likely to be mediated by autonomous motivation.
Subgroup analyses
Subgroup analyses were performed by including an interaction term with the treatment arm and the subgroup variable. The results of these subgroup analyses should be interpreted with caution because of a lack of statistical power.
Subgroup analysis showed that only two interaction terms warranted further exploration: nominated peer supporters (p-value = 0.047) and the proportion of sedentary time at baseline (p-value ≤ 0.001). However, the individual measures of SEP (i.e. proportion of free school meals, median distance of home to school, and school- and pupil-level IMD score) showed that no further exploration was required. Table 23 presents the subgroup analysis comparing peer supporters (i.e. those nominated by their friends across all 20 schools) between treatment arms and non-peer supporters between treatment arms. The treatment effect among nominated peer supporters was estimated to be –5.98 minutes of MVPA (95% CI –10.34 to –1.61 minutes of MVPA; p = 0.007), meaning that nominated peer supporters in the intervention arm accrued fewer minutes of daily MVPA at T1 than the nominated peer supporters in the control arm. This contrasts with the feasibility trial finding that the intervention had a beneficial effect on peer supporters’ daily MVPA. 51 The treatment effect among non-peer supporters was estimated as –1.90 minutes of MVPA (95% CI –5.18 to 1.37 minutes of MVPA; p = 0.23), meaning that non-peer supporters in the intervention arm had fewer minutes of daily MVPA at T1 than non-peer supporters in the control arm; however, the CI spans zero, so there is no evidence of a difference among non-peer supporters in the intervention and the control schools.
| Nominated peer supporter | Coefficient | 95% CI | p-value |
|---|---|---|---|
| Treatment effect in nominated peer supporters (minutes of MVPA) | –5.98 | –10.34 to –1.61 | 0.007 |
| Treatment effect in non-peer supporters (minutes of MVPA) | –1.90 | –5.18 to 1.37 | 0.255 |
| Difference in treatment effect (minutes of MVPA) | –4.08 | –8.14 to –0.0) | 0.049 |
The difference in treatment effects across peer supporters and non-peer supporters was –4.08 minutes of MVPA (95%CI –8.14 to –0.01 minutes of MVPA; p = 0.049), suggesting weak evidence of a difference in treatment effect in nominated peer supporters versus non-peer supporters, with the nominated peer supporters having a larger negative treatment effect than the non-peer supporters.
Because proportion of sedentary time at baseline is a continuous measure, the treatment effect is a function of the proportion of sedentary time at baseline. As displayed in Figure 2, for cases where baseline sedentary time was approximately > 85% (i.e. for 4.7% of the sample), the estimated treatment effect implies that the intervention arm had higher MVPA than the control group at T1. This can be interpreted as the fact that for ‘high-sedentary’ girls, being in the intervention arm resulted in higher physical activity. Those who had baseline sedentary time between 75% and 85% (i.e. ≈ 60.7% of the sample) had a treatment effect that showed no evidence of a difference in MVPA at T1. Those who had smaller proportions of sedentary time at baseline, that is sedentary time between 45% and 75% (i.e. 34.5% of sample), had a negative estimate, meaning that those in the intervention group achieved fewer minutes of MVPA than those in the control arm at T1. This suggests that the PLAN-A intervention is more effective in pupils who are highly inactive; however, the trial was not powered to detect differences in this subgroup analysis, so estimates and CIs should be interpreted with caution.
FIGURE 2.
Treatment effect over differing levels of proportion of sedentary time at baseline. LB, lower bound; UB, upper bound.
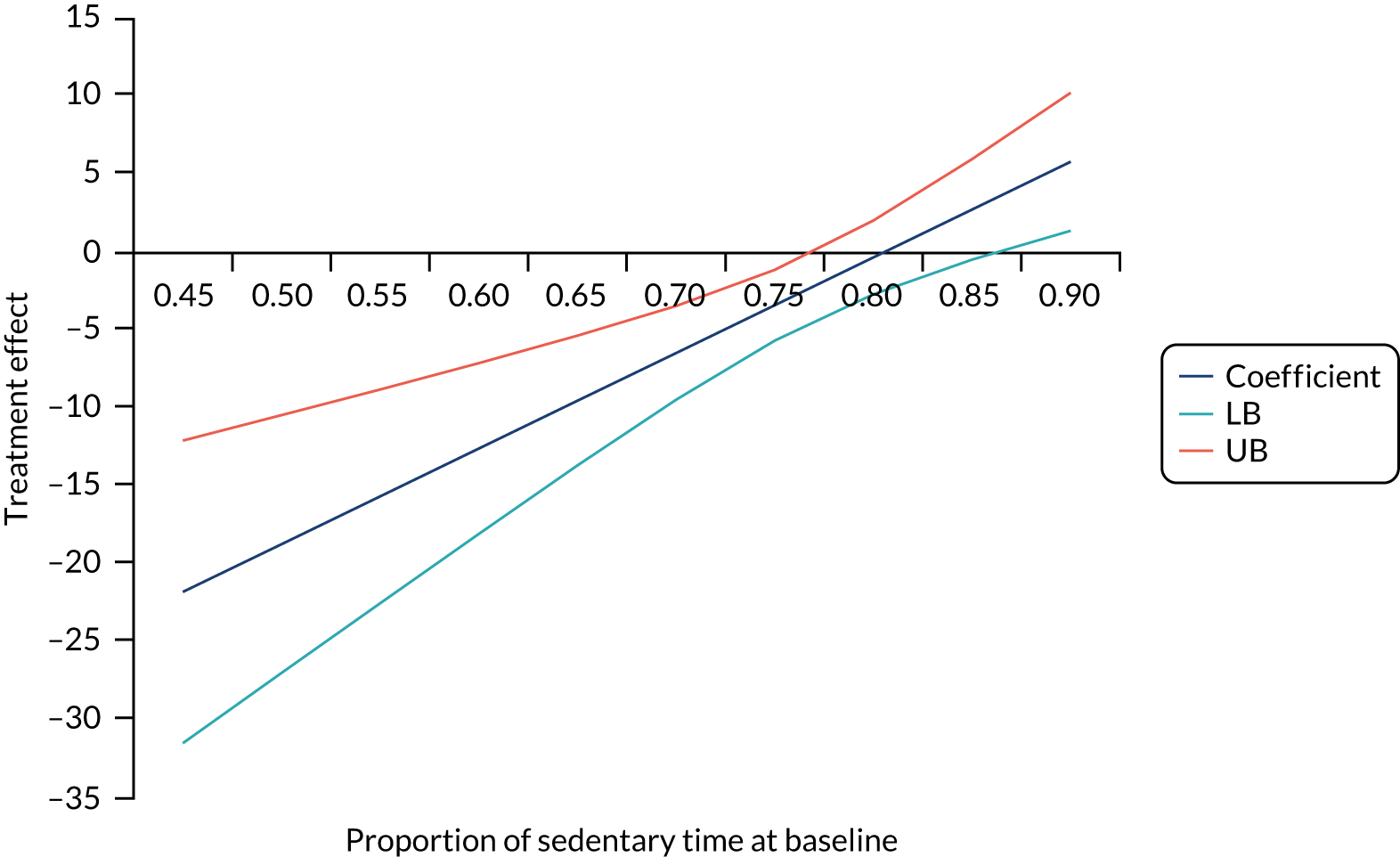
Adverse events
There were two minor adverse events during intervention delivery. Both were reported to the chairperson of the ethics committee, the TSC and the funder (for details, see Report Supplementary Material 12).
Post hoc analyses
All of the planned analyses were performed, and the results were presented to the TMG. The group discussed further areas of interest in the data and a few additional analyses were agreed to inform the results. These additional analyses included further subgroup analyses, analysis of additional outcomes, school-level data exploration and further investigation into the peer supporter treatment effect.
Additional subgroup analyses
Two additional subgroup analyses (i.e. pupils meeting CMO guidelines and pupils’ mode of transport from school to home) were performed. There was no evidence of a difference in treatment effect between those who did and those who did not meet CMO guidelines (p-value = 0.138), or between those who did and those who did not use active travel as a mode of transport from school (p-value = 0.658).
Repeating the primary analysis using counts per minute as the outcome
After adjustment, at T1, the counts per minute (CPM) (weekday, weekend and average across all valid days) were lower in the intervention arm than in the control arm. Mimicking the primary outcome analysis, there was some evidence of a difference in mean weekday CPM, favouring the control arm (difference in means –22.23, 95% CI –44.43 to –0.05; p = 0.05) (see Appendix 2).
School-level change in moderate to vigorous physical activity from time 0 to time 1
Figure 3 presents a school-by-school comparison of change in mean weekday MVPA from T0 to T1. This figure shows that the mean weekday MVPA for all schools decreased between the time points, with the only exception being school 6 (mean change 2.52 minutes, SD 18.13 minutes). The largest decline was observed in school 1 (mean change –11.81 minutes, SD 19.87 minutes) and school 2 (mean change –12.27 minutes, SD 17.53 minutes).
FIGURE 3.
School-by-school change in the primary outcome between T0 and T1. Navy indicates the intervention; aqua indicates the control. Error bars depict 95% CIs.
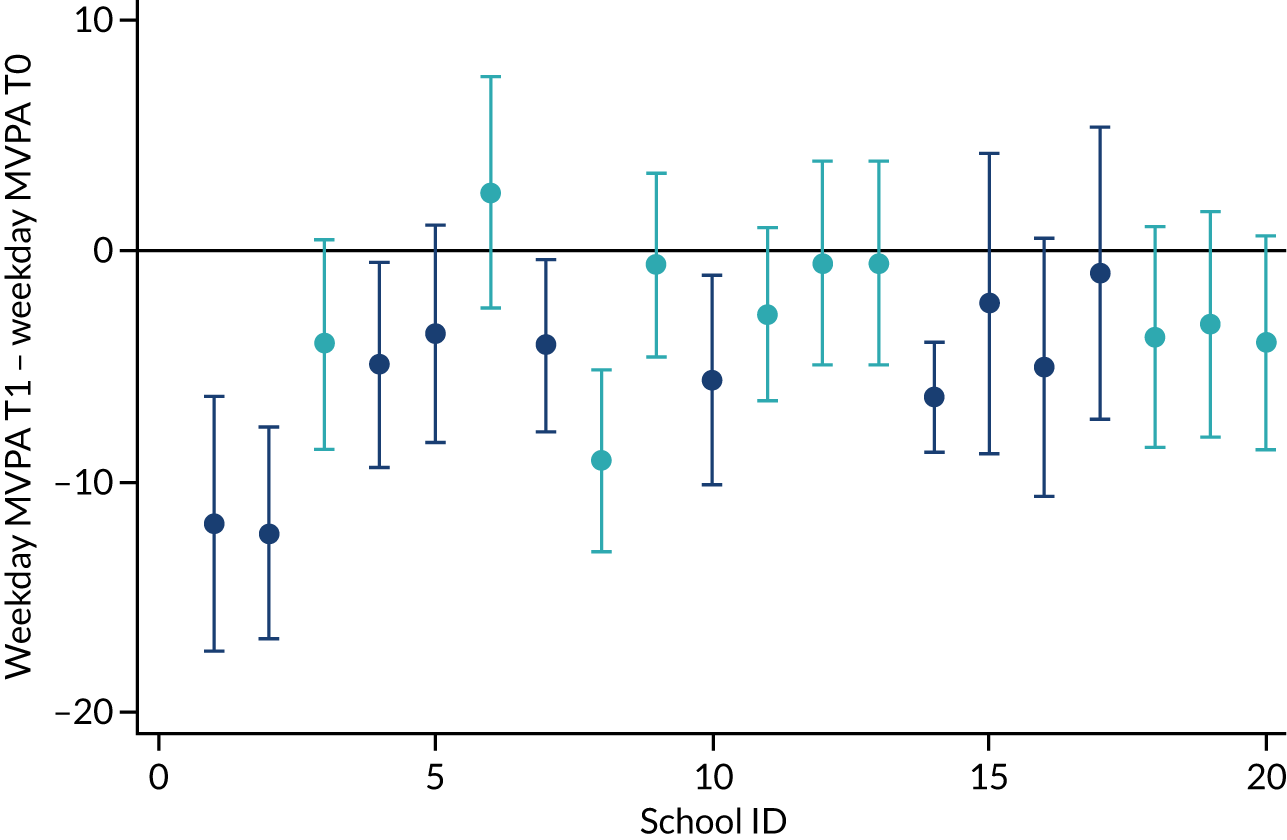
Peer supporters versus non-peer supporters in intervention schools only
Comparison of weekday MVPA data between peer supporters and non-peer supporters (Appendix 3), showed that there is very weak to no evidence that there is a difference in weekday MVPA minutes at T1 when comparing trained peer supporters with non-peer supporters (adjusted difference –2.25, 95% CI –5.27 to 0.22; p = 0.071). At baseline, peer supporters had a higher mean level of weekday MVPA than non-peer supporters, but both groups had similar levels at T1. Both groups showed a decrease in their MVPA between the time points, with peer supporters having a greater reduction in MVPA than non-peer supporters. The adjusted difference in T1 MVPA between peer supporters and non-peer supporters also showed weak to no evidence of an intervention effect.
Chapter 4 Economic evaluation results
Parts of this chapter have been reproduced with permission from Willis et al. 1 and Jago et al. 2 These are Open Access articles distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: https://creativecommons.org/licenses/by/4.0/. The text below includes minor additions and formatting changes to the original text.
Introduction
This chapter provides an overview of the results relating to the economic analysis of the PLAN-A programme. We report the resource use and costs (both school and local authority) associated with setting up and delivering the PLAN-A intervention to Year 9 girls, as well as the outcomes of HRQoL (as measured using the EQ-5D-Y, KIDSCREEN-10 and mapped CHU-9D) and minutes of MVPA per weekday.
Intervention-costing results
Resources captured as part of the intervention cost include:
-
Set-up costs for the PLAN-A programme. These comprised train-the-trainer costs and PLAN-A intervention consumables. In the main, set-up costs represent fixed costs and, therefore, the mean cost per school and pupil would decrease in proportion with the number of schools that receive peer supporter training.
-
Programme delivery costs related to individual schools. These comprised staff costs (local authority and school staff) associated with the delivery of peer nomination and peer supporter training. Programme delivery costs (which, in the main, represent variable costs) were captured and presented at the level of the individual school. All 10 intervention schools contributed to the cost data collection.
Intervention set-up costs
Train-the-trainer costs
The train-the-trainers course was a 3-day event held in one location for all of the trainers. Two trainers (the lead trainer and one member of the research team) delivered the course to a group of six trainers, with a resultant event cost of £319.09 per school and £3.53 per pupil (where a pupil is defined as a girl on the register at the start of Year 9; Table 24).
| Type of cost | Unit | Cost (£) | |||
|---|---|---|---|---|---|
| Unit | Total | Per school | Mean per pupila | ||
| Lead trainer time | One-off training courseb | 26 hours × £30.00 | 780.00 | 78.00 | 0.86 |
| Assisting trainer time | One-off training coursec | 18 hours × £13.51 | 243.18 | 24.32 | 0.27 |
| New trainer staff time | Attendance at training course lasting for 15 hours, six new trainers | 15 hours × 6 × £13.51 | 1215.90 | 121.59 | 1.35 |
| Travel (all trainers)d | Travel by private car: miles travelled | 648 miles × £0.45 per mile | 291.60 | 29.16 | 0.32 |
| Car parking | Daily parking charge | £24.00 daily rate × 3 days | 72.00 | 7.20 | 0.08 |
| Venue | Cost of venue (09.00–16.00) | 3 days × £137.50 | 412.50 | 41.25 | 0.46 |
| Refreshment | Refreshment costs | 3 days’ refreshments | 175.72 | 17.57 | 0.19 |
| Total per train-the-trainer event | 3190.90 | 319.09 | 3.53 | ||
Intervention consumables
Details on intervention consumables associated with the production of the PLAN-A resource kits were captured from invoices and entered on the PLAN-A trial budget database (Table 25). Intervention consumables (print and related resources) equate to £250.76 per school or £2.77 per pupil.
| Type of cost | Units | Cost (£) | |||
|---|---|---|---|---|---|
| Unit | Total | Per school | Mean per pupila | ||
| Printing and materials | Information packs for up to seven trainers (including one for lead trainer) | Variable, based on actual costs from invoices | 348.58 | 34.86 | 0.39 |
| Five boxes of materials for schools (reusable) | Variable, based on actual costs from invoices | 879.28 | 87.93 | 0.97 | |
| Production of resources and posters for 10 schools (not reusable) | Variable, based on actual costs from invoices | 116.60 | 11.66 | 0.13 | |
| Information packs for up to 180 peer supporters | Variable, based on actual costs from invoices | 1163.12 | 116.13 | 1.28 | |
| Total resources cost | 2507.58 | 250.58 | 2.77 | ||
Intervention delivery costs
Local authority staff time
Staff time associated with the co-ordination and delivery of peer nomination and peer supporter training was valued. In the real world, it is assumed that these activities would be carried out by a local authority-employed delivery agent. In total, the local authority staff time (circa 58 hours, on average) and resource to deliver the intervention equated to £1651 per school and £18.26 per pupil (Table 26).
| School ID (number of Year 9 girls on register) | Staff time (minutes) | Cost (£) | |||
|---|---|---|---|---|---|
| Peer nomination | Peer supporter training | Co-ordination of intervention delivery | Per schoola | Per pupil | |
| 1 (89) | 395 | 2475 | 395 | 1360.07 | 15.28 |
| 2 (78) | 350 | 2430 | 340 | 1526.14 | 19.57 |
| 4 (83) | 405 | 2760 | 365 | 1640.16 | 19.76 |
| 5 (80) | 305 | 2820 | 250 | 1645.20 | 20.57 |
| 7 (112) | 530 | 2715 | 255 | 1387.32 | 12.39 |
| 10 (87) | 465 | 2400 | 305 | 1408.52 | 16.19 |
| 14 (152) | 760 | 2610 | 795 | 2587.26 | 17.02 |
| 15 (82) | 495 | 2640 | 565 | 1916.38 | 23.37 |
| 16 (65) | 265 | 2640 | 270 | 1464.06 | 22.52 |
| 17 (76) | 355 | 2520 | 620 | 1572.74 | 20.69 |
| Mean | 432.50 | 2601 | 416 | 1650.78 | 18.26 |
School staff time
Within schools, school staff resource varied by the grade of the staff member involved (i.e. leadership, PE or administration/support teacher). In addition, the PLAN-A school contact time varied. At the extremes, school 10 recorded very little (240 minutes) school staff contact with the intervention, whereas school 16 recorded 1275 minutes. Overall, school staff time equated to a mean of £595.88 per school and £6.59 per pupil (Table 27). Although PLAN-A was delivered in usual school hours and these costs do not represent additional budgetary costs for the school, it is still the case that the teacher’s input in other PE or school activities (on average, around 18 hours) will have been displaced by involvement in PLAN-A activities.
| School ID (number of girls) | Staff time (minutes) | Staff cost (£) | Cost per pupil (£)a | |||||
|---|---|---|---|---|---|---|---|---|
| PE teacher | Leadership teacher | Administration support | PE teacher | Leadership teacher | Administration support teacher | Total school | ||
| 1 (89) | 1345 | 10 | 0 | 510.20 | 9.73 | 0.00 | 519.93 | 5.84 |
| 2 (78) | 1265 | 0 | 0 | 479.86 | 0.00 | 0.00 | 479.86 | 6.15 |
| 4 (83) | 0 | 205 | 1080 | 0.00 | 199.36 | 297.90 | 497.26 | 5.99 |
| 5 (80) | 1200 | 155 | 0 | 455.20 | 150.74 | 0.00 | 605.94 | 7.57 |
| 7 (112) | 650 | 135 | 0 | 246.57 | 131.29 | 0.00 | 377.85 | 3.37 |
| 10 (87) | 200 | 40 | 0 | 75.87 | 38.90 | 0.00 | 114.77 | 1.32 |
| 14 (152) | 0 | 1215 | 0 | 0.00 | 1181.59 | 0.00 | 1181.59 | 7.77 |
| 15 (82) | 0 | 130 | 1105 | 0.00 | 126.43 | 304.80 | 431.22 | 5.26 |
| 16 (65) | 0 | 1275 | 0 | 0.00 | 1239.94 | 0.00 | 1239.94 | 19.01 |
| 17 (76) | 1320 | 10 | 0 | 500.72 | 9.73 | 0.00 | 510.44 | 6.72 |
| Mean | 598 | 318 | 219 | 226.84 | 308.77 | 60.27 | 595.88 | 6.59b |
Total costs of intervention delivery
Table 28 presents the total cost of intervention delivery for each of the 10 intervention schools. The variable school staff costs (per hour) affected overall costs per school. There was variation in per-pupil costs between the schools, with costs ranging from £20.85 to £48.86. As the intervention involved high fixed costs, the cost per pupil was associated with the size of the school.
| School ID (number of girls) | Cost (£) | |
|---|---|---|
| Per school | Per pupila | |
| 1 (89) | 2449.85 | 27.53 |
| 2 (78) | 2575.85 | 33.02 |
| 4 (83) | 2707.27 | 32.62 |
| 5 (80) | 2820.98 | 35.26 |
| 7 (112) | 2335.03 | 20.85 |
| 10 (87) | 2093.13 | 24.06 |
| 14 (152) | 4338.70 | 28.54 |
| 15 (82) | 2917.45 | 35.58 |
| 16 (65) | 3273.85 | 50.37 |
| 17 (76) | 2653.03 | 34.91 |
| Mean cost (SD)b | 2816.51 (625.61) | 31.16c (7.75) |
Table 29 shows how the mean intervention cost per school (see Table 28) is broken down. The bulk of the costs came from the peer supporter training days and the staff time used to support the intervention.
| Type of cost | Mean cost (£) | |
|---|---|---|
| Per school | Per pupila | |
| Per train-the-trainer event | 319.09 | 3.53 |
| Intervention consumables | 250.76 | 2.77 |
| Peer nomination | 163.55 | 1.81 |
| Peer supporter training with pupils (2-day training and top-up day) | 1393.56 | 15.42 |
| Co-ordination of intervention delivery | 93.67 | 1.04 |
| School staff time (i.e. arranging/attending training, peer nomination and intervention delivery) | 595.88 | 6.59 |
| Totalb | 2816.51 | 31.16 |
EQ-5D-Y VAS, KIDSCREEN-10 and CHU-9D scores
Overall, the percentage of girls on the register who completed the EQ-5D-Y VAS, KIDSCREEN-10 and CHU-9D instruments was 82%, 84% and 75%, respectively, at T0, and 74%, 75% and 74%, respectively, at T1. Of these, 72%, 75% and 73%, respectively, had no missing data at either T0 or T1.
Quality-of-life scores (measured using the EQ-5D-Y VAS, KIDSCREEN-10 raw scores and T-scores, and the mapped CHU-9D) deteriorated slightly from T0 to T1 in both the intervention and control arm (Table 30). Appendix 4 presents the mapped data for those with complete CHU-9D questionnaires by time point and trial arm.
| Variable | Intervention arm | Control arm | ||
|---|---|---|---|---|
| n | Mean (SD) | n | Mean (SD) | |
| EQ-5D-Y VAS | ||||
| T0 | 731 | 70.62 (19.89) | 783 | 70.10 (20.11) |
| T1 | 676 | 68.45 (20.67) | 689 | 65.85 (22.55) |
| KIDSCSREEN-10 (raw score) | ||||
| T0 | 755 | 0.540 (0.968) | 799 | 0.552 (0.960) |
| T1 | 683 | 0.331 (0.939) | 694 | 0.251 (0.946) |
| KIDSCREEN-10 (T-score) | ||||
| T0 | 755 | 39.97 (9.48) | 799 | 40.09 (9.40) |
| T1 | 683 | 37.92 (9.19) | 694 | 37.15 (9.26) |
| Mapped CHU-9D | ||||
| T0 | 741 | 0.832 (0.097) | 792 | 0.831 (0.097) |
| T1 | 677 | 0.807 (0.097) | 681 | 0.802 (0.098) |
Inspection of the profile responses of the EQ-5D-Y for each dimension of the instrument showed a similar pattern in both arms (Figures 4–8). A large percentage of girls (around 45%) at both time points and in both the intervention and control arms reported some or a lot of problems with pain or discomfort. The majority of girls (87–88%) in both groups reported that they were a bit or very worried, sad or unhappy; this proportion increased slightly at T1. It was unclear whether this was an age-related phenomenon or indicative of factors not measured in this trial, but consistency between arms suggests it was not related to the intervention. The intervention and control groups reported mean baseline CHU-9D index scores of 0.83; these scores declined by T1 (see Table 30).
FIGURE 4.
Profile of the population: percentage reporting problems with mobility.
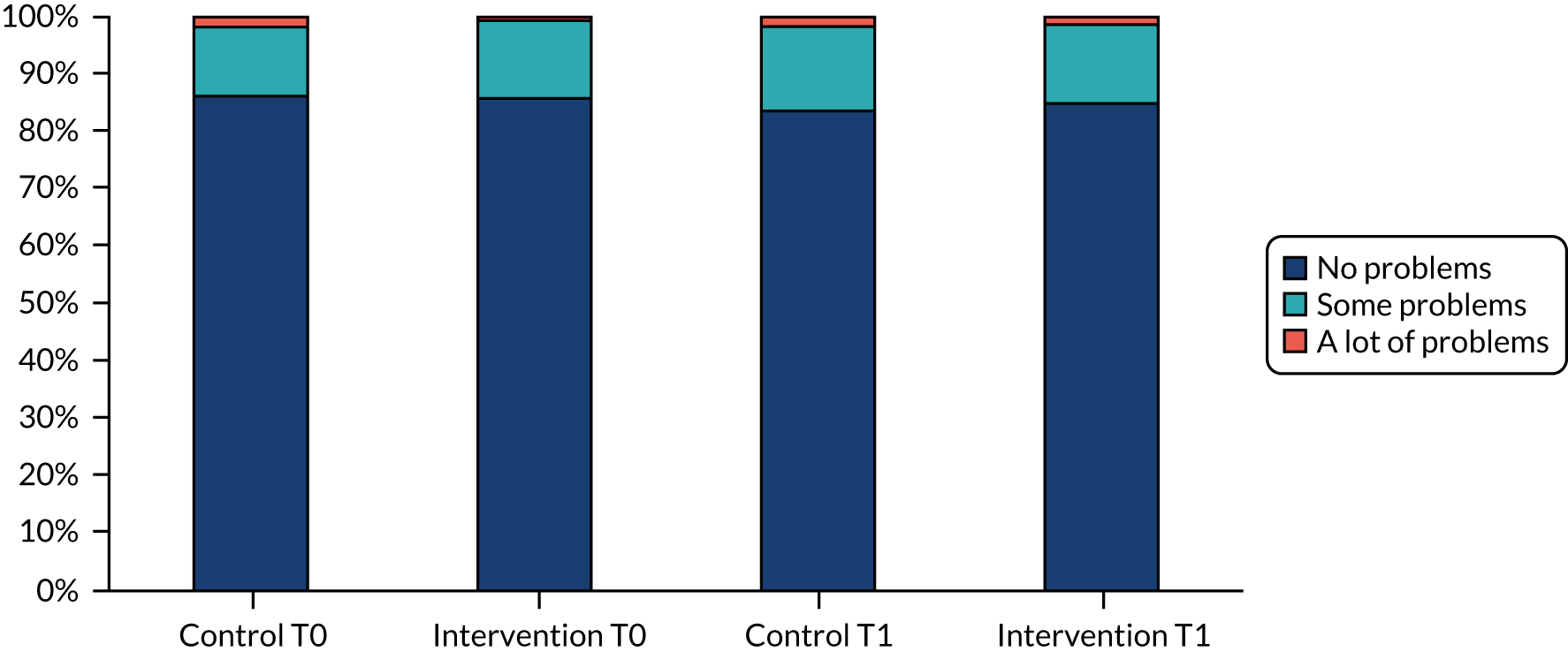
FIGURE 5.
Profile of the population: percentage reporting problems with looking after themselves.
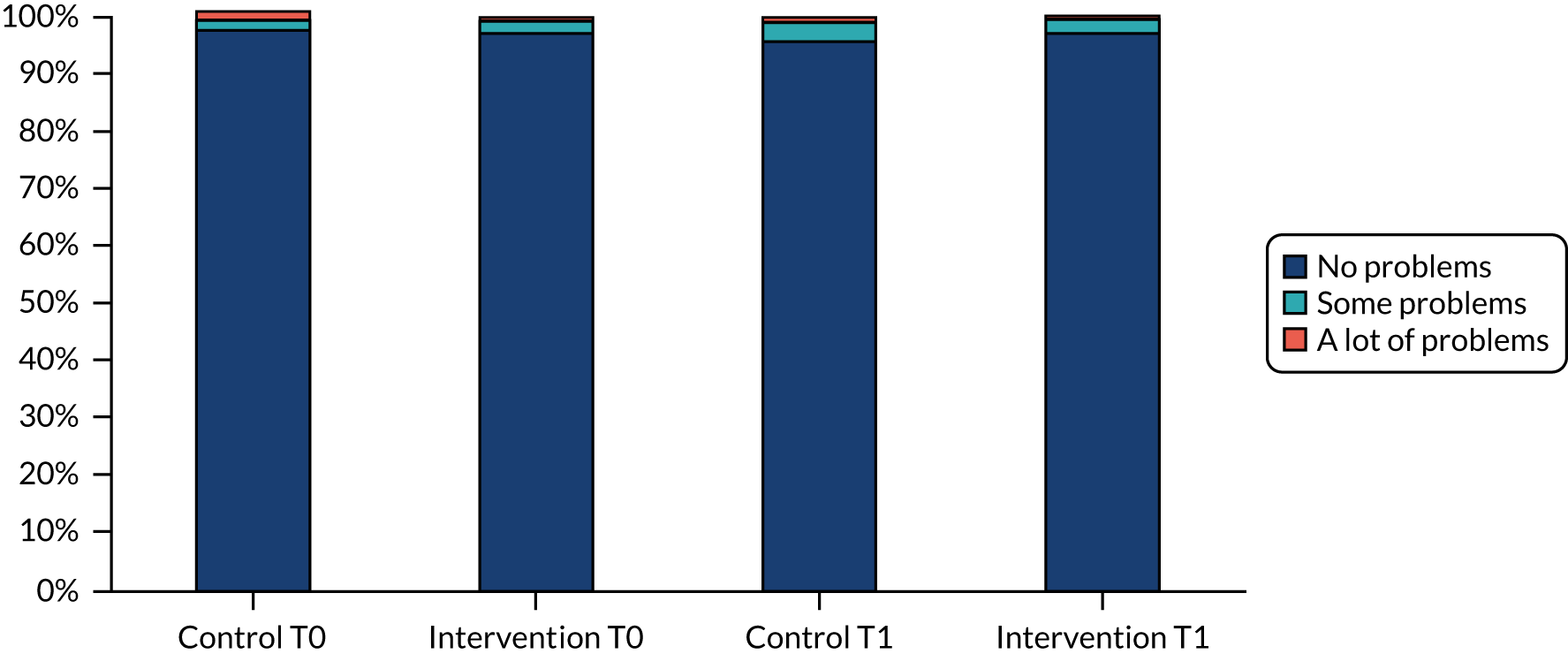
FIGURE 6.
Profile of the population: percentage reporting problems with doing usual activities.
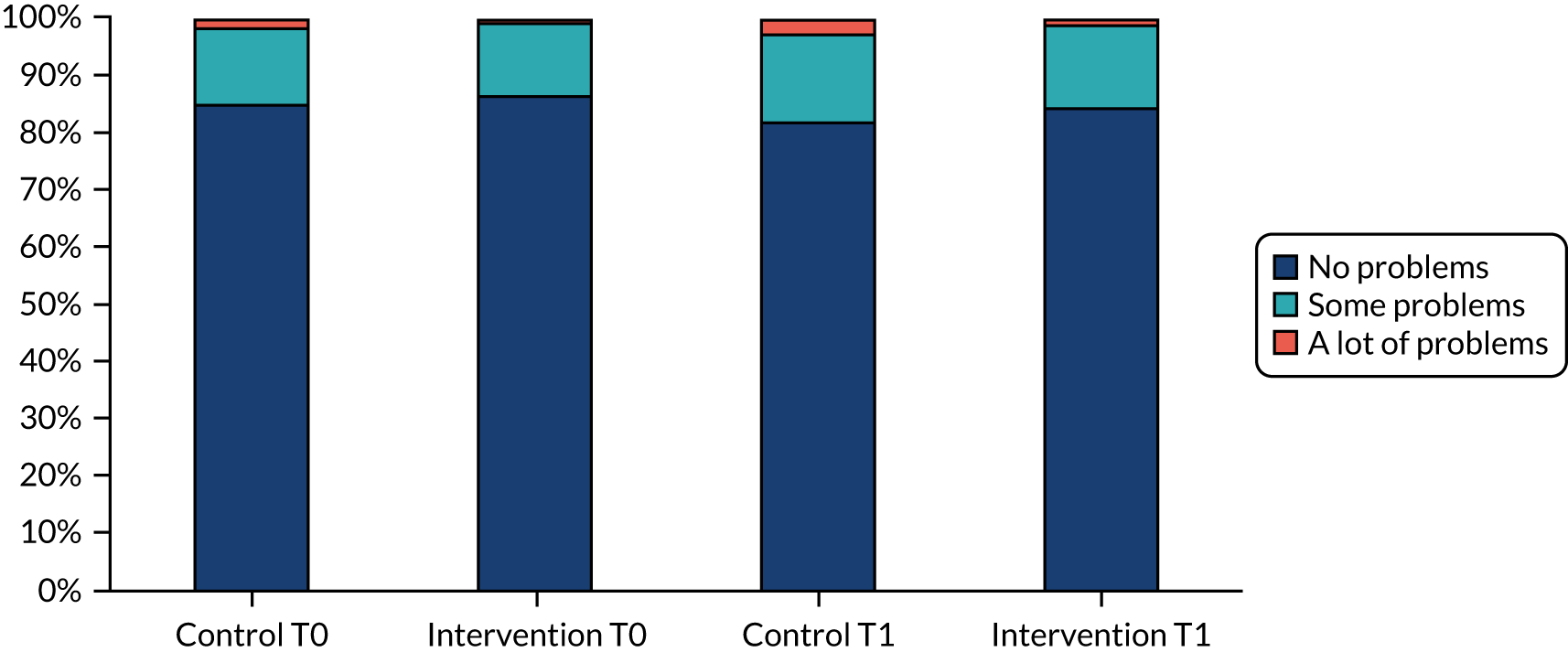
FIGURE 7.
Profile of the population: percentage reporting problems with pain or discomfort.
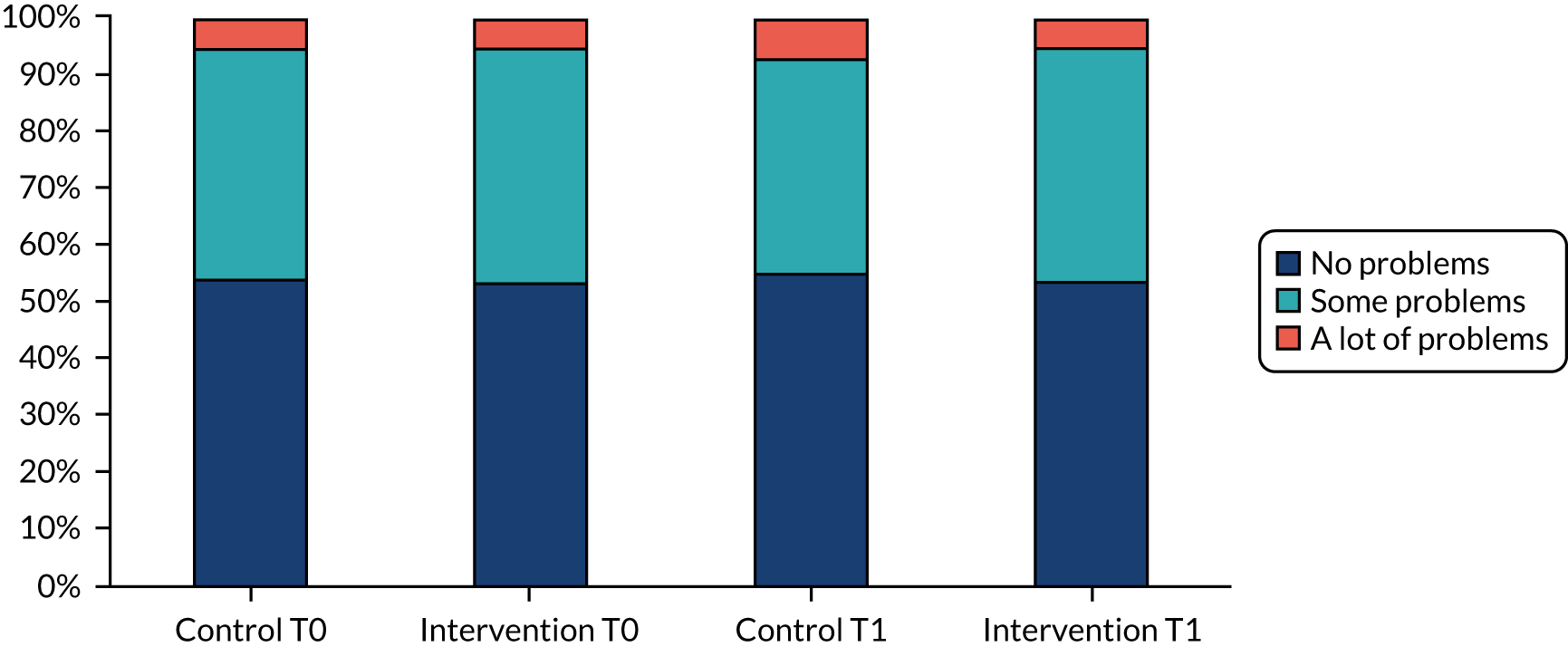
FIGURE 8.
Profile of the population: percentage reporting problems with feeling worried, sad or unhappy.
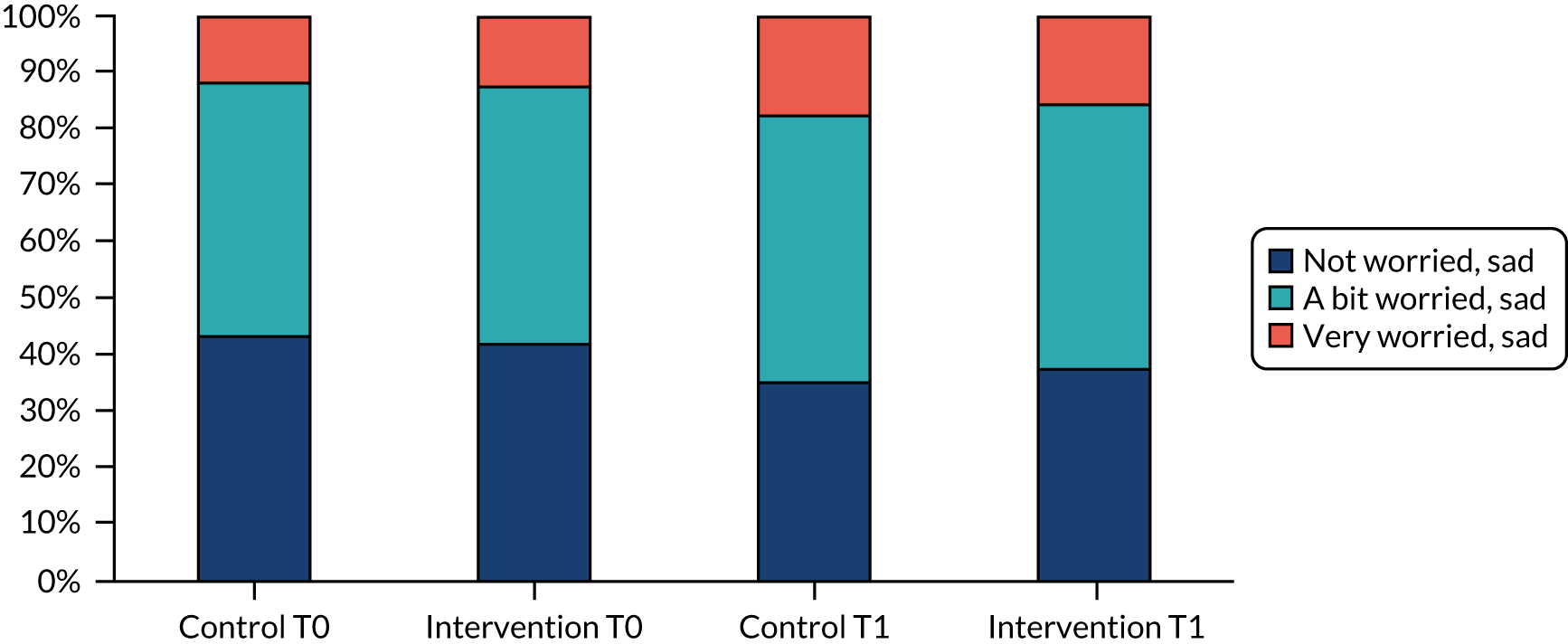
Primary economic analysis
Cost per unit change in moderate to vigorous physical activity and cost per 5-minute increase in moderate to vigorous physical activity
The bootstrapped estimate of mean incremental costs was £30.50 and the mean incremental benefit was –3.54 minutes of MVPA. The mean estimate of the ICER, calculated as the ratio of the bootstrapped cost-effect replicates, was –£37.24, with the negative ICER, in this instance, indicating that the intervention is dominated (i.e. more costly and less beneficial than the control). The majority of the bootstrapped replications were in the north-west quadrant of the CEP (Figure 9), indicating that the intervention is probably more costly and less effective at improving weekday MVPA than the control. The scatterplot crosses the y-axis, indicating that there is, however, a high degree of uncertainty surrounding the effect on weekday MVPA. The CEAC (Figure 10) shows that the probability that the intervention was cost-effective is low over a range of willingness-to-pay thresholds for a unit change in MVPA. In secondary analysis, estimating the cost per 5-minute increase in weekday MVPA, the estimate of the ICER was –£186.22.
FIGURE 9.
Mean cost and weekday MVPA and associated uncertainty (1000 bootstrap replications).
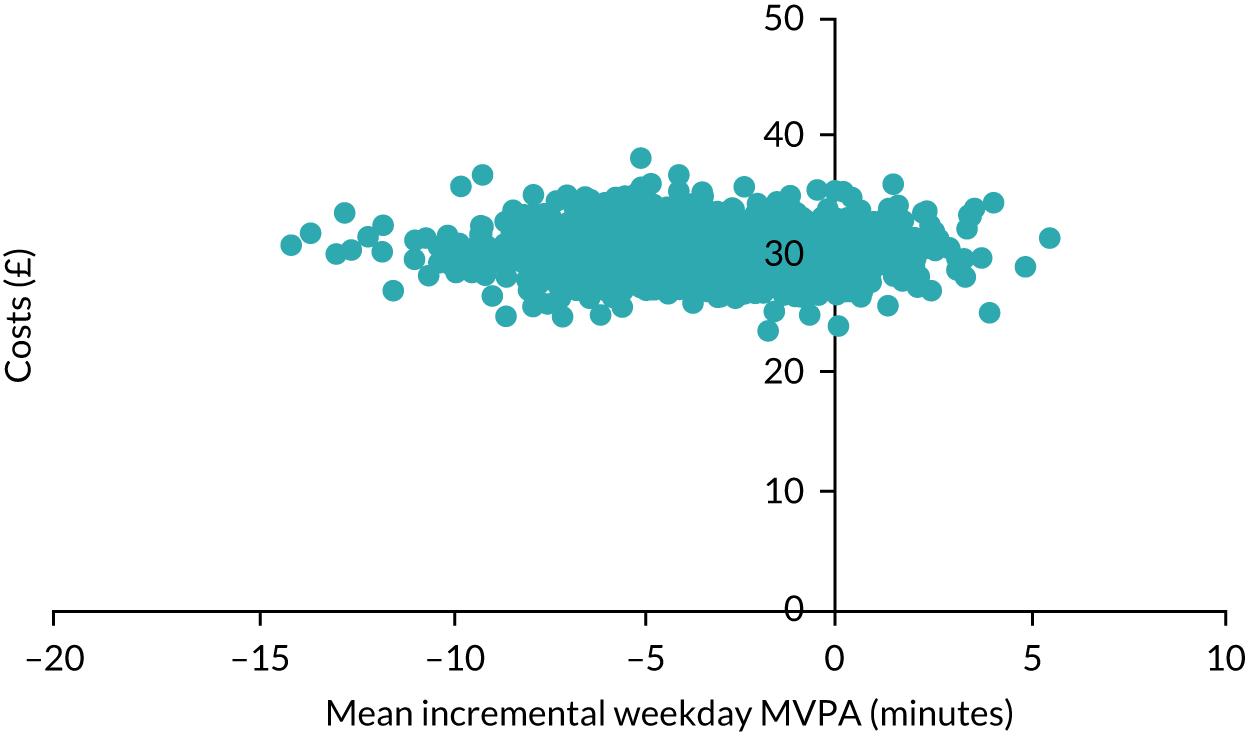
FIGURE 10.
The CEAC over a range of hypothetical willingness-to-pay thresholds for MVPA.
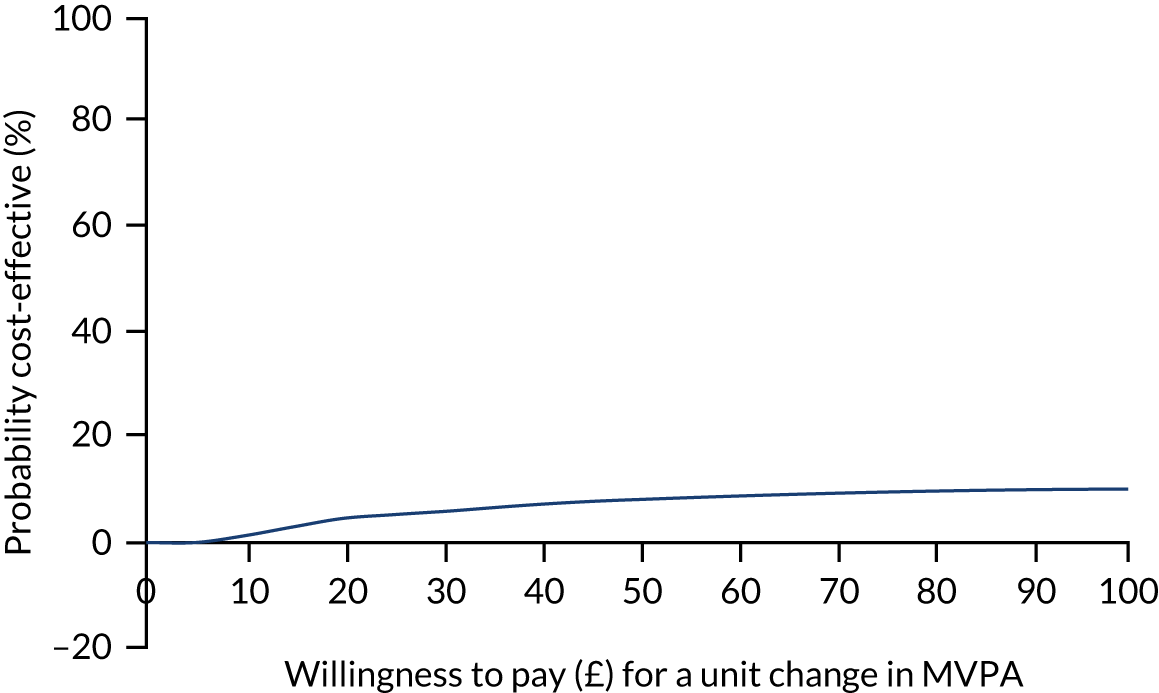
Cost–consequences analysis
As has already been reported (see Table 17), pupils in the intervention and control arms achieved, on average, 45 and 49 minutes of MVPA per weekday, respectively. After adjustment, the difference between arms was estimated as –2.84 (95% CI –5.94 to 0.25; p = 0.071) minutes, a trend suggesting that those in the intervention arm performed fewer minutes of weekday MVPA than those in the control group, on average.
There was no evidence of a statistically significant difference in incremental effects between arms for (the mapped) CHU-9D or QALYs (Table 31). In unadjusted analyses, there was some evidence that the KIDSCREEN-10 and EQ-5D-Y VAS scores were better in the intervention group (see Table 31). However, differences were small and consistent with no effect of the intervention in adjusted analyses.
| Measure (control, n; intervention, n) | Mean (SD) score | Difference between groups (incremental costs/effects) (95% CI) | ||
|---|---|---|---|---|
| Control arm | Intervention arm | Unadjusted (1000 bootstrapped 95% CI) | Adjusted for baseline level and stratification variables (1000 bootstrapped 95% CI)a | |
| KIDSCREEN-10 change in score from T0 to T1 (694; 680)b | –0.340 (0.830) | –0.229 (0.888) | 0.111 (0.016 to 0.195) | 0.095 (–0.120 to 0.202) |
| CHU-9D change in score from T0 to T1 (676; 662)b | –0.035 (0.085) | –0.029 (0.088) | 0.006 (–0.004 to 0.015) | 0.005 (–0.005 to 0.016) |
| EQ-5D-Y VAS change in score from T0 to T1 (678; 656)b | –4.643 (22.999) | –2.238 (21.678) | 2.405 (0.106 to 4.705) | 1.136 (–2.807 to 5.080) |
| QALYs (674; 662)b | 0.819 (0.088) | 0.820 (0.087) | 0.001 (–0.008 to 0.011) | 0.003 (–0.003 to 0.008) |
| Per-pupil intervention cost (944; 904)b | N/A | £31.16 | £30.50 | N/A |
Cost per quality-adjusted life-year
In the exploratory cost–utility analysis using the mapped CHU-9D scores, the point estimate of the probabilistic ICER was £35,748 per QALY, which is above the £20,000-per-QALY threshold conventionally applied in the UK. The bootstrapped replications of the cost–effect pairs in Figure 11 show a similar pattern to the primary economic analysis; however, the replications are split more evenly between the north-west (i.e. more costly, less effective) and north-east (i.e. more costly, more effective) quadrants of the CEP. Figure 12 identifies that at conventional willingness-to-pay threshold values of £20,000 and £30,000 per QALY, the intervention has a 48% and 51% chance of being cost-effective, respectively. At lower thresholds, the intervention is much less likely to be cost-effective.
FIGURE 11.
Mean cost and QALY and associated uncertainty (1000 bootstrap replications).
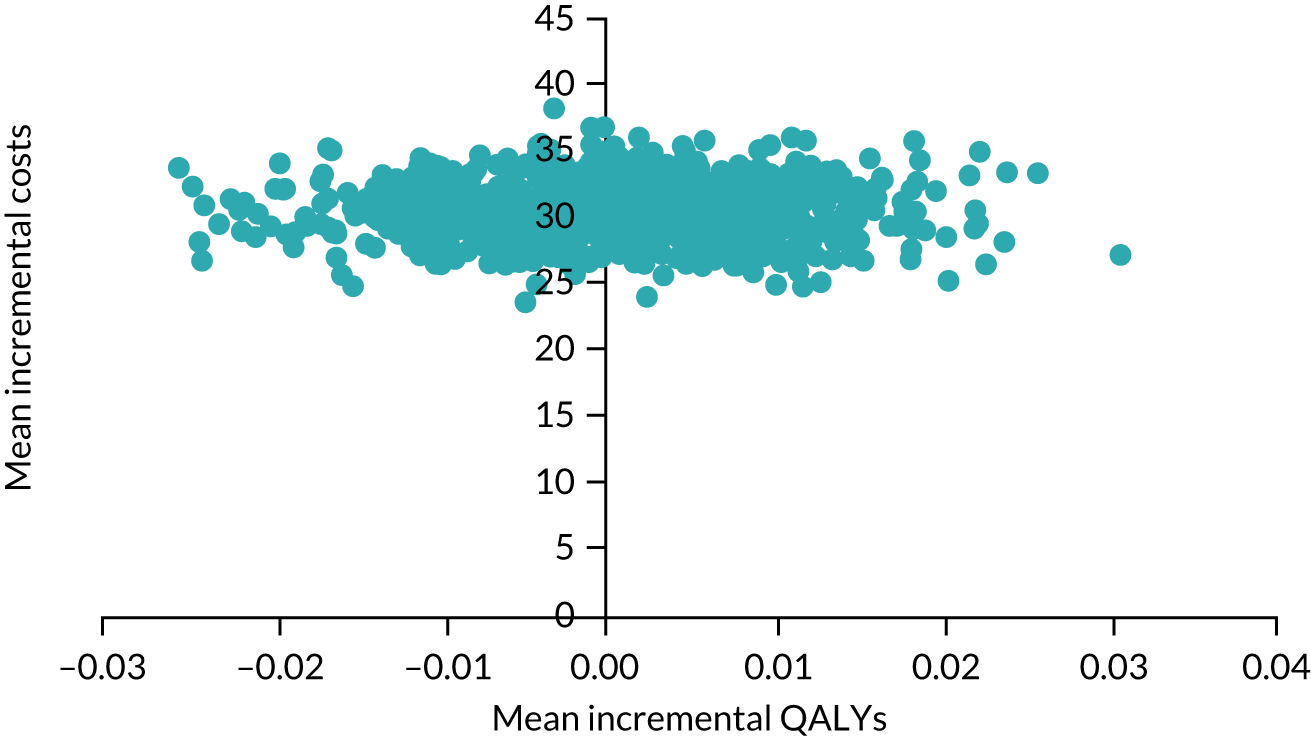
FIGURE 12.
The CEAC over a range of hypothetical willingness-to-pay thresholds.
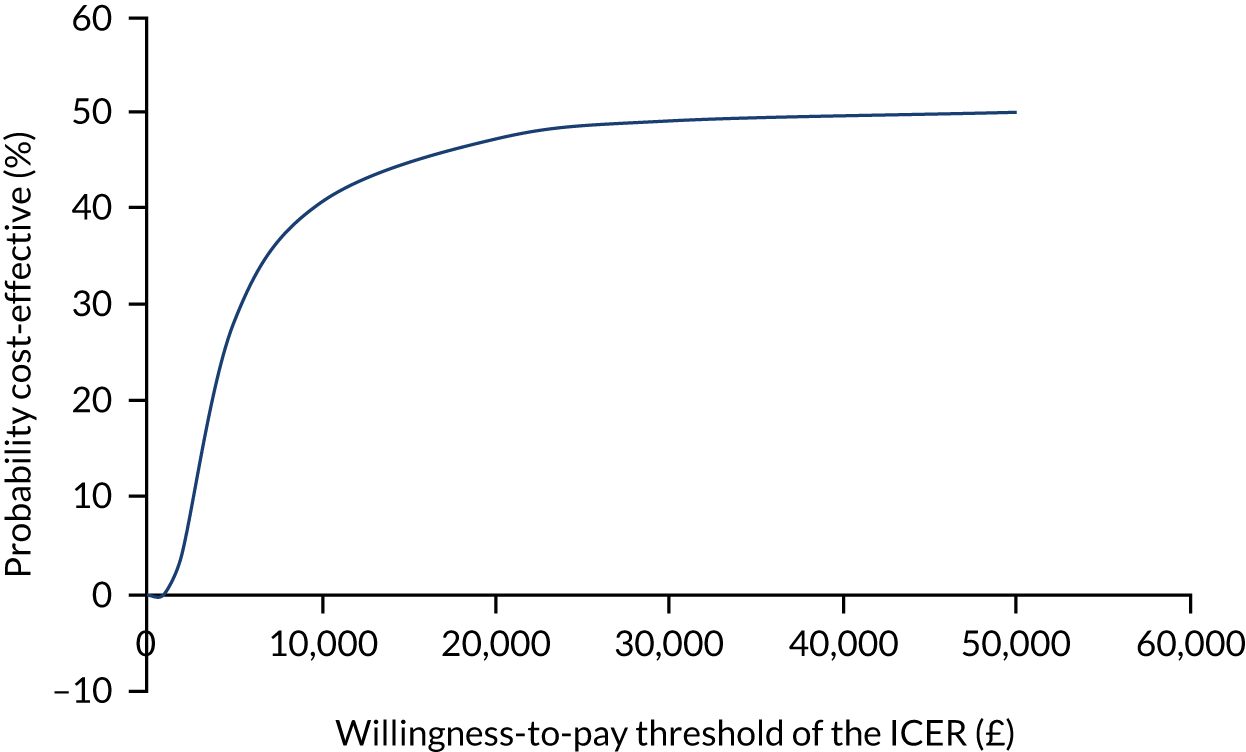
Consideration of long-term consequences
Our published health economics analysis plan96 considered long-term consequences on the basis of the intervention meeting two conditions: (1) evidence of promise and (2) availability of a model linking changes in adolescent physical activity to long-term health outcomes. Evidence of promise required that the point estimate of MVPA was positive and the 95% CI included the possibility of a meaningful (5 minutes of weekday MVPA) positive intervention effect. As this criterion was not met and there was no available model linking changes in adolescent physical activity and health outcomes, an extrapolation model is not presented.
Chapter 5 Process evaluation results
Parts of this chapter have been reproduced with permission from Willis et al. 1 and Jago et al. 2 These are Open Access articles distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: https://creativecommons.org/licenses/by/4.0/. The text below includes minor additions and formatting changes to the original text.
The aim of this process evaluation was to understand how the intervention was delivered, whether or not it was delivered as intended, whether delivery or receipt differed by setting and what factors affected delivery fidelity. A mixed-methods process evaluation was conducted, and the findings are structured to address (a) fidelity and quality of intervention delivery, (b) receipt of the intervention and the experience of being a peer supporter, (c) perceived intervention effects and (d) school context. Quantitative data comprise questionnaire data, attendance records and observations of the intervention delivery. Qualitative data comprise interviews with school contacts and trainers and focus groups with peer supporters and non-peer supporters at each intervention school. In addition, interviews were conducted with public health commissioners, education leads, and regional and national organisations to explore potential implications for public health policy and practice.
Quantitative data provision
All intervention sessions were observed by a member of the research team. In total, 158 (95.18%) and 137 (82.53%) peer supporters completed the evaluation questionnaire following the 2-day and top-up day training, respectively. Peer supporters reported the type and frequency of peer supporting that they had undertaken (as a measure of fidelity) at the top-up day and at the end of the 10-week intervention period (by mail). In total, 132 (79.52%) peer supporters provided this information at the 5-week time point, but only 23 (13.86%) responded at 10 weeks. Therefore, these data cannot be used to make representative statements about peer supporter fidelity at week 10.
Qualitative data provision
Peer supporter and non-peer supporter focus groups and school contact interviews were completed in all 10 intervention schools. Quotations have been anonymised and are presented by informant group and school identification number (ID) or trainer ID [e.g. peer supporter (PS) 7, non-peer supporter (NPS) 2, school contact (SC) 10, trainer G].
Fidelity and quality of intervention delivery
School and participant recruitment
There were no stated barriers to taking part in the project for girls or school contacts. However, in two schools, the consent rate was low (46.27% and 52.78%) compared with the average consent rate of 88.58% in the other 18 schools. Very few non-consenting girls provided a reason for not taking part and so there are few pupil data to understand this issue. However, in one school with a low consent rate, the school contact described a pupil mind-set within the school that deterred girls from putting themselves forward for opportunities because of a lack of confidence and fear of the unknown.
Train the trainers
The trainers perceived their training for the intervention to be comprehensive, enjoyable and successful in preparing and motivating them to deliver the content to the peer supporters in line with the theoretical principles of SDT. The format, delivery style and bonding time with the other trainers were praised, as well as the opportunity to check understanding and ask questions about delivery style:
The trainers [who delivered the train the trainers] were really good. I think it was really effective, us pretending to be the girls, because you got to go through every activity, how it would be run, and then you can, kind of, go through it in your head, things that might be changed, or things you think that they would pick up quicker or need more time on. I think it was good to go through the theory side of it, to understand that, and I think enough time was spent on that.
Trainer D
The importance of being trained in broader teaching techniques was highlighted, including reading the audience, relating the activities to the peer supporter role and emphasising key objectives:
. . . you guys were saying it over and over again, ‘this is the one thing I want you to summarise. Make sure that everything you’re doing is in the context of peer supporting’ . . . But I had your voices in my head saying ‘always bring it back to the peer supporting’ . . .
Trainer C
Using the peer supporter training resources at the train-the-trainers event was an important learning aid. The resources and delivery aids were rated ‘excellent’ for all training days (see Appendix 5).
Spending 1 full day on the material for each of the peer supporter training days was praised by trainers as it gave them the time to focus on the content for each day. Two trainers would have liked the top-up day content to be covered closer to the actual delivery of the top-up days to maintain trainer confidence:
I think that it was the right amount of time. Also good for it to mirror the amount of time that we would have with the girls. So we had quite a real-life experience of what they would be doing, so that’s good.
Trainer A
Peer nomination
Outcome of peer nomination
Although some peer nominations came as a surprise to school contacts because the girls were ‘less sporty’ or shy, and several were known for disruptive behaviour, most peer supporters were described as the confident, influential, kind, sporty and supportive girls in their year. It was believed that some peer supporters already upheld the key principles of the peer supporter role and encouraged their peers to be active. In certain schools, they were described as conscientious and future leaders in their school, suggesting that the process successfully selected appropriate peer supporters in most schools.
Representation of the year group among the peer supporters varied between schools. In some schools, most peer supporters were part of the same friendship group, whereas, in others, peer supporters represented a range of friendship groups. Most non-peer supporters had a friend who was a peer supporter or at least knew a peer supporter. Therefore, the process yielded a potentially representative sample.
Consenting to be a peer supporter
Consent rates and reasons for not signing up to be a peer supporter are reported in Chapter 3, Peer supporter recruitment. Peer supporters felt that there were few barriers to opting to be a peer supporter. The two most common drivers for agreeing to become a peer supporter were to be able to help and motivate others to become more active, and to be more active themselves.
Peer supporters at three schools were motivated by receiving nominations that indicated support from their peers, highlighting the perceived value of a peer-nomination process:
It wasn’t like your teacher picked you. It was that people within your year thought you were fit for the role, and that made you feel better about yourself and want to do it more because your friends and people around you thought that you could do it.
PS 10
Impact of not being nominated as a peer supporter
Most peer supporters and non-peer supporters felt that not being nominated did not have a negative impact:
. . . nobody really seemed annoyed, which, I think, is good.
PS 2
I wasn’t really bothered to be fair because it’s one of those things.
NPS 1
However, a few peer supporters believed that some non-peer supporters felt annoyed or disappointed that they were not nominated because they saw themselves as more active than some of the girls who were peer supporters. This was echoed by some school contacts:
When I was talking to my friends about it, some of them, two of them, seemed a bit annoyed. That’s people that were a bit more active than me.
PS 2
You could hear them saying ‘oh, why can’t we do that?’ or ‘we’re not on that’ . . . They weren’t that upset, but I just think it was just something that they might have liked to have been involved in.
SC 10
This view was not reflected in non-peer supporter focus groups, although some girls did speculate that others may have been jealous. Some did want to be a peer supporter, but did not mind that they did not get nominated; only one member of a non-peer supporter focus group from one school felt annoyed and thought it was unfair.
Peer supporter training
Attendance
Table 32 shows that 84.33% of consented peer supporters attended all 3 days of training (ranging from 66.67% to 100.00% across all schools). In six schools, all peer supporters attended both training days 1 and 2. The school with the lowest mean attendance was affected by absence for a school event on the top-up day. Conflict with important lessons was another reason for non-attendance in some schools. Two girls dropped out of the training because they no longer wanted to be a peer supporter.
| School ID | Peer supporters (N) | Attendance, n (%)a | ||||
|---|---|---|---|---|---|---|
| Training day 1 | Training day 2 | Training days 1 and 2 | Top-up training | All 3 days of training | ||
| 1 | 14 | 14 (100.00) | 14 (100.00) | 14 (100.00) | 12 (85.71)b | 12 (85.71) |
| 2 | 14 | 14 (100.00) | 14 (100.00) | 14 (100.00) | 11 (78.57)b,d | 11 (78.57) |
| 4 | 15 | 15 (100.00) | 14 (93.33)b | 14 (93.33) | 14 (93.33)b | 13 (86.67) |
| 5 | 16 | 16 (100.00) | 13 (81.25)b,d | 13 (81.25) | 15 (93.75)d | 13 (81.25) |
| 7 | 26 | 26 (100.00) | 26 (100.00) | 26 (100.00) | 23 (88.46)c,d | 23 (88.46) |
| 10 | 18 | 18 (100.00) | 17 (94.44)c | 17 (94.44) | 12 (66.67)b | 12 (66.67) |
| 14 | 22 | 22 (100.00) | 20 (90.91)b,c | 20 (90.91) | 18 (81.82)b | 18 (81.82) |
| 15 | 11 | 11 (100.00) | 11 (100.00) | 11 (100.00) | 10 (90.91)b | 10 (90.91) |
| 16 | 14 | 14 (100.00) | 14 (100.00) | 14 (100.00) | 12 (85.71)b | 12 (85.71) |
| 17 | 16 | 16 (100.00) | 16 (100.00) | 16 (100.00) | 16 (100.00) | 16 (100.00) |
| Total | 166 | 166 (100.00) | 159 (95.78) | 159 (95.78) | 143 (86.14) | 140 (84.33) |
Training logistics
School contacts were happy that the training logistics were arranged by the trial team as it minimised the amount of work required by the school – a crucial factor in achieving buy-in from schools. School contacts found the process ‘easy’ because the trial team communicated clearly and worked around the needs of the school:
I think with school staff, if it’s going to work, it needs to be as minimal as you can make it. So the fact that you guys did all of that made my life loads easier . . .
SC 14
The duration and number of breaks throughout the training days were acceptable to peer supporters and trainers. Peer supporters liked the food, but would have preferred more simple sandwiches and crisps from the options available.
Training structure
Eighty-five per cent of peer supporters rated the length of training as acceptable (Table 33). The qualitative data support this and suggests that most peer supporters and school contacts felt that the structure (2 consecutive days, followed by a top-up day after 5 weeks) of the training was also appropriate, allowing the peer supporters to take on board information and feel prepared:
It wasn’t too long. It stuck with the school day, so they were happy to be able to leave at the same time as everyone else . . . it was like a normal school day.
SC 1
I think the fact that we had 2 days, one after the other, just made it easier for us to understand stuff.
PS 5
| Statement | School ID | All schools | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 4 | 5 | 7 | 10 | 14 | 15 | 16 | 17 | ||
| Evaluation after 2-day training, mean (SD) score | |||||||||||
| The length of training was about right (2 days) | 3.50 (0.65) | 2.93 (0.73) | 3.64 (0.50) | 1.63 (1.20) | 3.00 (1.13) | 3.06 (1.20) | 2.95 (1.18) | 2.90 (0.99) | 3.21 (1.12) | 3.50 (0.52) | 3.01 (1.10) |
| The training was interesting | 3.57 (0.51) | 3.21 (0.70) | 3.50 (0.85) | 2.81 (0.66) | 2.81 (0.57) | 2.35 (1.17) | 3.37 (0.60) | 2.70 (0.95) | 3.86 (0.36) | 3.67 (0.49) | 3.15 (0.83) |
| I learned some new things about physical activity | 3.50 (0.76) | 3.64 (0.50) | 3.57 (0.76) | 3.25 (0.58) | 3.40 (0.71) | 3.29 (0.77) | 3.74 (0.56) | 3.50 (0.53) | 3.86 (0.36) | 3.75 (0.45) | 3.54 (0.64) |
| The venue was a good place to do the training | 3.00 (1.11) | 3.50 (1.16) | 2.86 (0.66) | 2.25 (1.13) | 2.46 (1.21) | 2.65 (1.06) | 2.58 (1.07) | 2.50 (1.08) | 3.43 (0.65) | 3.08 (1.00) | 2.79 (1.09) |
| I enjoyed the games | 3.50 (0.65) | 3.64 (0.63) | 3.64 (0.63) | 2.81 (1.11) | 3.15 (0.78) | 3.18 (0.81) | 3.84 (0.37) | 3.50 (0.71) | 3.86 (0.36) | 3.75 (0.45) | 3.46 (0.76) |
| I had enough time to practise being a peer supporter | 3.43 (0.76) | 3.00 (1.11) | 3.29 (0.91) | 2.19 (0.91) | 3.04 (0.87) | 3.29 (0.85) | 3.47 (0.70) | 3.30 (0.48) | 3.50 (0.85) | 3.50 (0.67) | 3.18 (0.90) |
| I am confident that I can pass positive messages on to my friends about getting active | 3.21 (0.70) | 3.14 (0.86) | 3.29 (0.47) | 2.81 (1.05) | 3.35 (0.69) | 3.18 (0.39) | 3.26 (0.73) | 3.10 (0.88) | 3.43 (0.65) | 3.42 (0.51) | 3.22 (0.71) |
| I understand my role as a peer supporter | 3.71 (0.47) | 3.64 (0.50) | 4.00 (0.00) | 3.63 (0.50) | 3.73 (0.53) | 3.76 (0.44) | 3.74 (0.45) | 3.60 (0.52) | 3.86 (0.36) | 3.83 (0.39) | 3.75 (0.45) |
| The trainers were helpful | 3.71 (0.47) | 3.50 (0.94) | 3.79 (0.43) | 3.06 (0.57) | 3.23 (0.76) | 3.35 (0.70) | 3.79 (0.42) | 3.40 (0.84) | 4.00 (0.00) | 3.67 (0.49) | 3.53 (0.67) |
| The trainers were friendly | 3.79 (0.43) | 3.79 (0.43) | 3.86 (0.36) | 3.00 (0.52) | 3.46 (0.71) | 3.47 (0.62) | 4.00 (0.00) | 3.40 (0.84) | 4.00 (0.00) | 3.83 (0.39) | 3.65 (0.58) |
| Evaluation after top-up day training, mean (SD) score | |||||||||||
| 1 top-up day was about the right amount | 3.50 (0.52) | 3.20 (0.92) | 3.79 (0.58) | 2.77 (1.24) | 2.95 (1.28) | 3.48 (1.04) | 3.56 (0.92) | 3.40 (0.52) | 3.25 (1.22) | 2.93 (1.07) | 3.27 (1.02) |
| I enjoyed the games | 3.50 (0.67) | 3.50 (0.71) | 3.93 (0.27) | 3.75 (0.45) | 3.43 (0.75) | 3.14 (1.29) | 3.83 (0.38) | 3.80 (0.42) | 3.67 (0.49) | 2.50 (1.29) | 3.45 (0.87) |
| The training gave me new tips and help on being a peer supporter | 3.42 (0.79) | 3.00 (1.25) | 3.86 (0.36) | 3.46 (0.66) | 3.05 (0.86) | 2.90 (1.17) | 3.11 (0.90) | 3.40 (0.52) | 3.50 (0.52) | 2.71 (0.73) | 3.22 (0.85) |
| I learned some new things about physical activity | 3.33 (0.49) | 2.40 (1.26) | 3.71 (0.47) | 3.54 (0.66) | 2.95 (0.86) | 2.71 (0.90) | 3.00 (0.97) | 3.11 (0.78) | 3.58 (0.67) | 2.29 (1.38) | 3.07 (0.97) |
| The training reminded me of important things about being active | 3.50 (0.52) | 3.50 (0.71) | 3.93 (0.27) | 3.77 (0.44) | 3.33 (0.66) | 3.48 (0.69) | 3.50 (0.71) | 3.50 (0.53) | 3.58 (0.67) | 3.00 (0.68) | 3.50 (0.63) |
| I had enough time to practice being a peer supporter | 3.25 (0.62) | 3.30 (0.95) | 3.50 (0.65) | 3.38 (0.77) | 3.05 (1.16) | 3.14 (0.89) | 3.22 (0.94) | 3.30 (0.67) | 3.58 (0.67) | 2.50 (1.02) | 3.19 (0.90) |
| I understand my role as a peer supporter | 3.83 (0.39) | 3.60 (0.52) | 4.00 (0.00) | 3.92 (0.28) | 3.71 (0.56) | 3.81 (0.65) | 3.89 (0.32) | 3.80 (0.42) | 3.92 (0.29) | 3.54 (0.66) | 3.80 (0.46) |
| I am confident that I can pass positive messages on to my friends about getting active | 3.33 (0.49) | 3.50 (1.27) | 3.36 (0.50) | 3.38 (0.77) | 2.95 (0.67) | 3.05 (0.83) | 3.06 (0.80) | 2.75 (1.04) | 3.50 (0.67) | 3.07 (0.62) | 3.19 (0.77) |
| The trainers were helpful | 3.83 (0.39) | 3.40 (1.07) | 4.00 (0.00) | 3.69 (0.48) | 3.33 (0.66) | 3.48 (1.03) | 3.72 (0.46) | 3.40 (0.52) | 3.83 (0.39) | 3.29 (0.61) | 3.59 (0.64) |
| The trainers were friendly | 3.83 (0.39) | 3.50 (0.71) | 4.00 (0.00) | 3.92 (0.28) | 3.52 (0.68) | 3.71 (0.69) | 3.94 (0.24) | 3.40 (0.52) | 3.92 (0.29) | 3.43 (0.65) | 3.71 (0.53) |
Training content
Stakeholders felt that there were no gaps in the peer supporter training content, it flowed well and had a suitable format with a good balance of interactive, active and quieter writing activities built in:
There was a range of different things. We did some desk work on what we needed and then we did some fun games and getting to know each other, it was a good fun day, or 2 days . . .
PS 14
I thought it was really varied. Sometimes, they were sat down, watching a video and doing stuff on worksheets. Then, other times, they were really active.
SC 10
Conversely, some peer supporters felt this balance was in favour of sitting and writing, which they viewed as negative. The overarching opinion was that more games would have increased peer supporter enjoyment. The second most common suggestion was to make the training more active overall:
. . . a lot of writing compared to actually moving.
Yes, considering it’s about being more sporty, we did more writing than anything.
PS 15
Sometimes, trainers found it hard striking this balance:
They were like ‘we’re peer supporting and trying to get people to be active, but we’re not very active in terms of activities,’ which is fine, because they need to get the content across as well . . . Sometimes, there’s just no pleasing them.
Trainer C
Peer supporters and school contacts agreed that the training was pitched at the right level and was relevant to the aims of the project. However, some peer supporters felt that there was a lot of information to take on board, which made the days tiring:
I think the training, as such, and the training the girls had was very detailed. It was all relevant. I think the girls enjoyed that.
SC 7
I think, in the training, they threw a lot of information at us. There was a lot thrown at us, and it’s a lot to take in to be honest, over the 2 days.
PS 1
Some school contacts felt that it would not suit older age groups, but would work well with Year 8:
I think, for that year group, it was probably . . . I don’t think you’d be able to do it with any older year group, but maybe Year 8s would benefit from it as well.
SC 10
To some extent, all stakeholders thought that some of the training content was repetitive, particularly during the top-up day (see Chapter 5, Top-up day). Although practising peer supporter scenarios was enjoyable and aided learning, these activities were repeated too often:
. . . it felt like the second day was just going over what we’d done on the first day.
PS 7
Some trainers thought that this repetition was needed to reinforce information, as one trainer said that the peer supporters had forgotten a lot between the 2-day and the top-up day training:
I think all the activities were really good. I think day 2 is a little bit repetitive, but it’s also a good thing because they really do need to understand. I think it does take them a whole day to really get to grips with the conversations.
Trainer D
Training venues
Off-site venues to hold the peer supporter training that were within a mile of the school were secured for 8 out of 10 schools. In most cases, the venue was at a convenient location and was a suitable size with appropriate facilities. However, Table 33 shows that overall satisfaction mean score ± SD with the venue was low: mean score ± SD 2.79 ± 1.09 (maximum score 5). Low scores at schools 5, 7 and 15 were due to the space being too small and/or there being little/no outdoor space. Having a ‘breakout’ space or somewhere to be outdoors was important, as peer supporters did not like to feel ‘cooped up like a chicken’ (PS 16). Trainers rated the suitability (mean score ± SD 2.80 ± 0.89) and quality of facilities (2.55 ± 1.00) as ‘very good’ (maximum score 4; see Appendix 5). Despite the training spaces being more suitable on the top-up day, the quality decreased quite substantially (mean score ± SD 1.89 ± 1.02); this was probably due to difficulties in securing suitable venues.
All interviewed stakeholders felt that having the training off-site was important and preferable; it made it feel ‘more special’ (SC 14), promoted a better learning environment, meant that the peer supporters could be themselves and provided a break from school. In the two schools that hosted the intervention on-site, it was reported that peer supporters were often distracted, which led to disruptive behaviour. The ideal venue was described as off-site, with access to outdoor space, and the size of a sports or village hall:
I think we would have enjoyed it a bit more if it was in a different [venue], because, I think, it’s like, when you go out, you can take it more seriously.
PS 10
Despite school contacts understanding the importance of having an off-site venue, some still suggested that it would be more convenient to hold training at school because of the school policies on organising trips off-site (which differed between schools). Some schools required 6 weeks’ notice, others a detailed risk assessment of the intended venue or additional parental consultation, and some schools were unable to release a member of staff to act as a chaperone for the training. This presented challenges for three school contacts and was the main reason for on-site delivery in schools 7 and 10.
The delivery of the peer supporter training on-site at school 10 demonstrated how this approach can negatively affect the intervention. Safeguarding procedures at this school meant that trainers could not leave the room reserved for the training, but the girls could. On day 1, this led to the peer supporters leaving the training venue during breaks without supervision (some for meetings with teachers, others to collect equipment), which resulted in peer supporters being distracted from the training and causing disruption to lessons in school:
Having worked in several schools, it did feel a little bit like the administration of that school was interfering a bit and trying to hold us back from what we were doing.
Trainer A
The disruption prompted complaints from school staff about the peer supporters not being in uniform (although this was part of PLAN-A) and the disturbance to lessons. This led to the school contact interrupting the peer supporter training to discipline the peer supporters. She spoke to the girls in a demeaning way and made an example out of one of the peer supporters for the clothes she was wearing (this girl subsequently dropped out of the training). The girls were told by the school to wear uniform or PE kit for the rest of the training. This incident led to feelings of defiance from the peer supporters and made the trainers uncomfortable and led them to feel that the peer supporters had lost trust in them:
. . . going back to the initial 2 days is when there was that bit of upset with the school, they seemed to lose a bit of trust in us, I think.
Trainer B
One trainer felt that this incident could have been prevented if they were more explicit with the peer supporters about the boundaries, especially with the training being on-site. As a result, the peer supporters became disengaged and harder to manage:
. . . the real disruption happened on day 1. When they came back for day 2, we’d kind of lost them already at the beginning of the day.
Trainer A
The top-up day delivery in school 10 was also restricted to one half-day because of an unforeseen school request for girls to be released early to receive exam results, an issue that would probably not have occurred off-site. The school contact was aware that the top-up day was cut short, compromising fidelity to the peer supporter training session plans. Observation data confirmed that the training was delivered in full in all other schools:
I know that ours was cut short, because the top-up day didn’t work fully . . .
SC 10
Delivery of the peer supporter training
Delivery in pairs
Having two trainers deliver the training had certain advantages in that each trainer acted as a form of support for the other and trainers had different delivery styles:
I normally, just, as an individual, tend to be a bit more concise and a bit more to the point . . . [Trainer name], on the other hand, I was paired with quite a lot, tends to do the other way around. So we were a good balance.
Trainer C
It was preferable to have the same pair of trainers deliver the training at multiple schools, as this allowed trainers to adapt to each other’s teaching styles, to build a rapport with each other and, therefore, to optimise delivery. However, each of the trainers delivered with more than one partner and reported being well prepared to adapt as long as they had time to discuss who would lead which activities ahead of time:
I thought [when working with a different trainer] ‘oh no, I’ve got a good thing with [trainer name], we get the timings,’ you know, ‘we’ve got it perfectly’. But, actually, we all were so well-practised and informed from the training days that I think we knew how it would work anyway, and it just all flowed together really well . . .
Trainer C
Where possible, the same trainer pair delivered all 3 days of training in a school. Where this was not the case (i.e. in four schools), a different trainer stood in for the top-up day. Although it was desirable for the same pair to deliver the top-up day training to maintain consistency and take advantage of the rapport already established with the peer supporters, it was felt that having at least one of the same trainers was sufficient to ensure continuity from the 2-day training:
I think it’s important to have at least one of the same trainers on the top-up day. But I don’t think it’s a massive problem if the second trainer is not the same person.
Trainer D
Group size
In two schools, the number in the peer supporter group exceeded 20 (n = 26 and 22). Larger groups challenged the quality of delivery, how activities were delivered and the girls’ confidence in participating in discussions. No trainers mentioned any delivery challenges associated with smaller groups:
It [a large group] just felt like crowd control rather than being able to deliver it and being happy with our own delivery. I certainly wasn’t.
Trainer E
Delivery of content
Observation data indicated that, in general, there was good fidelity to the intervention content. Training activities were delivered in line with each of the objectives, at least ‘to some extent’ (Figure 13). The exceptions were the top-up day training in school 10, which was not delivered as intended (see Chapter 5, Training venues), and school 17, where the peer supporters’ level of engagement was low.
FIGURE 13.
Average observed fulfilment of manualised activity objectives per school for all training days. 0 = not at all, 1 = a little, 2 = to some extent, 3 = mostly/all.
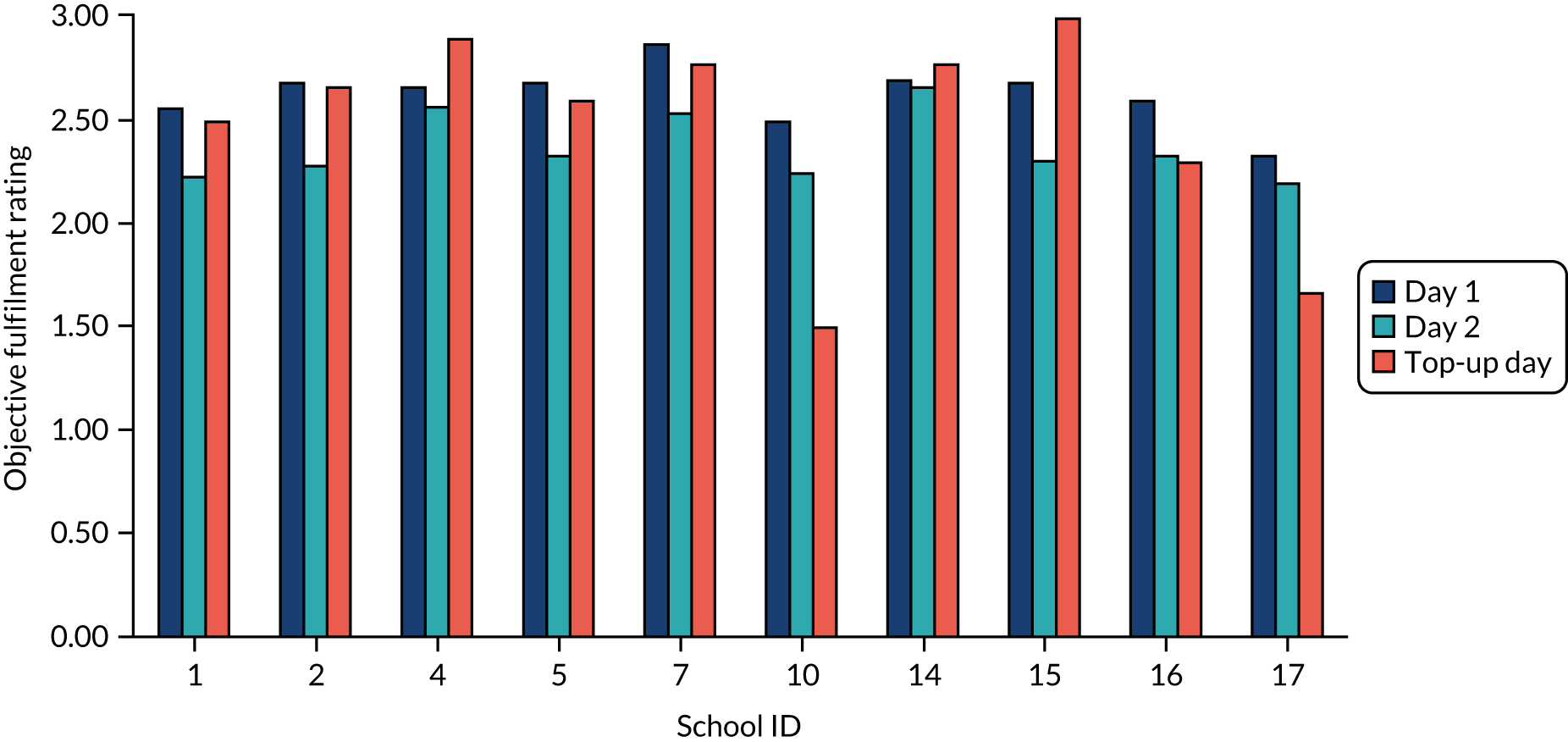
Trainers felt that key aspects of the training were achieved throughout both training sessions across all schools (see Appendix 6). The lowest scoring aspect for both the 2-day and top-up training was how well the training enhanced the peer supporters’ interpersonal skills (mean ± SD score 2.15 ± 0.75 and 2.22 ± 0.55, respectively; maximum score 3). Peer supporters at school 17 scored the lowest across all aspects, particularly in the success of the training in enhancing interpersonal skills (2-day training, 0.50 ± 0.71; top-up training, 2.00 ± 0.00) and helping the peer supporters understand their role (2-day training, 0.50 ± 0.71; top-up training, 1.00 ± 0.00). However, both aspects improved after the top-up day. All trainers reported finding the delivery of the training an enjoyable and rewarding experience.
Supportive learning environment
Observation and focus group data indicated that, overall, the trainers were successful in creating a supportive environment for learning. They achieved this by managing the pace of delivery, making the content clear and relatable, and checking understanding. This also enabled them to respond to arising topics and develop a person-centred approach to delivery:
I think they went through everything quite thoroughly because every time we went back they would quiz us on what we would learnt before. And then, if we couldn’t really remember stuff, they would refresh us.
PS 4
The trainers’ enthusiasm and friendly manner were key in fostering this environment, as well as making the girls feel confident to share their ideas and opinions:
I think because they were really interested in what they were teaching us, it made it easier to learn about it.
PS 7
Peer supporters from schools 10 and 16 perceived that the activities were not well linked and that the trainers ran out of ideas. Specifically, they felt that the trainers were not well prepared or did not work well together, and they made the training feel like it dragged. For school 10, this may, in part, be explained by the fact that this was the first peer supporter training that the trainers delivered (see Chapter 5, Adaptation):
. . . we did very separate tasks, but we didn’t actually link them together much . . . If everything we did was linked in together, it would show us what we’re supposed to do.
PS 10
I don’t know if this was new to them as well. It just seemed like, at some points, they didn’t know, in terms of, we would just be sat there, going to do something and they’d just, like, stare and it would just be silent for about 2 minutes and we didn’t know what to do.
PS 16
Adaptation
Trainers noted that there was considerable variation between the groups of peer supporters in terms of confidence levels, engagement and understanding, and reported successfully tailoring activities to the individuals’ and groups’ needs. The activities that were affected the most by these aspects involved role play:
You can see it [losing concentration] happening at the time and maybe adapt, if you are quick enough, get the activity to be a little bit more active and move things around.
Trainer E
. . . we did try and get across to them that these conversations and the scenarios, that we weren’t getting them to act. It wasn’t about acting, it was trying to be normal conversations that you would have. Some of them, I think, did feel a little bit nervous about standing up in front of the groups and reading out their scripts or acting it out.
Trainer D
Being able to modify activities effectively relied on the trainers’ ability to read the room, an ability that developed over time, as well as a more natural approach to delivery. Some trainers reported feeling quite nervous for their first session, which may have contributed to the initial scripted style of delivery. This also influenced the trainers’ ability to support the needs of the peer supporters (see Chapter 5, Challenges of delivering the peer supporter training in line with self-determination theory):
. . . it was just lack of experience and lack of confidence and that [being able to adapt the training] was OK. I was quite, sort of, like ‘we need to get this done,’ you know, ‘this is what we need to deliver’ and I need to do it. Sticking by the rules . . . if we had noticed that they were getting a bit frustrated and bored and we’d moved on, that probably would have been better. So that was a learning thing for us.
Trainer B
Fidelity to self-determination theory
Self-determination theory39 was woven throughout the intervention design: in the delivery style coached to the trainers, the content of the peer supporter training and the recommended peer-supporting techniques. 52 A crucial component of the theoretical underpinning was the promotion and support of the three inherent psychological needs: autonomy, relatedness and competence. The subsequent section utilises qualitative focus group data and questionnaire data to assess fidelity to the theoretical principles behind the design, and reports the perceived challenges to delivery of the intervention in line with SDT.
Needs supportiveness of trainers and peer supporters’ perceptions of need support
There was evidence from focus groups, interviews, questionnaire data and intervention observations that all trainers were successful in delivering the training in line with SDT: they supported the peer supporters’ autonomy, belonging and competence using a variety of techniques.
Autonomy support
The quantitative perceptions of the trainers’ provision of autonomy support were similar for both the 2-day and top-up training (Table 34), showing that peer supporters felt that, overall, the trainers were supportive of autonomy at all of the training days.
| Time point | School ID | Overall | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 4 | 5 | 7 | 10 | 14 | 15 | 16 | 17 | ||
| Days 1 and 2 | 3.38 (0.73) | 3.36 (0.91) | 3.69 (0.49) | 2.88 (0.76) | 3.26 (0.81) | 3.11 (0.82) | 3.61 (0.57) | 3.41 (0.65) | 3.79 (0.41) | 3.67 (0.53) | 3.39 (0.75) |
| Top-up day | 3.57 (0.67) | 3.45 (0.87) | 3.76 (0.51) | 3.83 (0.38) | 3.35 (0.87) | 3.26 (0.77) | 3.64 (0.57) | 3.23 (0.67) | 3.74 (0.47) | 2.95 (0.69) | 3.48 (0.72) |
Observation records confirm that trainers provided choice as to how certain aspects of the peer supporter training should be run by involving peer supporters in decision-making about the topics covered, game rules, activity length, working groups and timing/duration of breaks. This was largely supported by qualitative data:
They said very clearly from the start ‘How do you want to be treated? How can we get your attention?’. It wasn’t like school. It was very much from that moment ‘You’re part of this, it’s a two-way thing’. That had an impact on the girls and their involvement.
SC 16
They didn’t try and control us.
PS 14
Observation data indicated that girls were primarily offered options; however, sometimes opportunities to involve girls in decision-making were missed. Several girls felt that they had little choice; however, others understood that, given the nature of the training, the trainers gave them choice when the opportunity arose and it was appropriate:
I think everything we had the opportunity to have a say in, like, what we did, because we couldn’t lead it because we didn’t know what to do. They had to take some form of leadership and they did. But anything we could get a say in, we did . . .
PS 14
Trainers supported learning by encouraging the peer supporters to share their opinions and views, as well as recognising when to adapt the training to the needs of the peer supporters, giving clear rationale for changes:
So, giving them the choice on what they could do helped. You know, ‘so we can move onto the next activity because you are doing really, really well or we can have a little break or a slightly longer break if we carry on with this activity’.
Trainer E
Two trainers felt that failure to do this undermined the peer supporters’ autonomy. Observation data corroborate the belief that, in the occasional instances when only one opinion was gathered or prescriptive language was used, autonomy was undermined, although it was unclear whether or not this affected engagement:
Actually, I think that was one of the mistakes that [trainer name] and I made in [school name], was that, although we did mix it up and we gave them some breaks, we didn’t actually involve them in that process.
Trainer B
Relatedness support
In creating an open, relaxed and supportive atmosphere, the trainers helped the peer supporters feel that they could share and talk freely, allowing the girls to bond with each other and with the trainers. Common approaches to achieving this included being friendly and inclusive, joining in with activities, showing personal interest in peer supporters’ lives to build rapport, using personal experience to relate to the peer supporters, addressing concerns directly using supportive language and learning the girls’ names:
I think they didn’t try and act like teachers, they just acted themselves and just communicated with us as if we’re just all the same.
PS 14
I just think, yes, building that rapport on that first day, just those little bits of first names, and giving them the options, yes, I would say worked well.
Trainer F
Comments from school contacts suggested that the trainers worked with the peer supporters, communicating with them on the same level rather than talking down to them and teaching them like children. This finding was supported by a trainer who reported that she fostered ‘friendship’ rather than a teacher–pupil relationship:
They [the peer supporters] didn’t feel like you [the trainers] were there to teach them. I think they thought you were there to actually work with them, rather than talk down to them . . .
SC 10
They just then didn’t treat us like teachers. I think they saw us a bit more like peers, a little bit more, because we weren’t in uniform, we weren’t in anything like that, and we weren’t in their school.
Trainer C
Collectively, the trainers were described as non-judgemental, good listeners, interested and relatable:
. . . they were trying to relate to us, it was quite easy for us to talk about stuff with them.
PS 4
However, peer supporters from two different schools felt that they did not bond with one of the trainers. At one school, it was felt that the trainer’s body language made her seem unapproachable. No clear reason was given for the lack of rapport with the trainer at the other school:
She always had this look on her face: if we looked over to her, she’d have this stern face, and it wouldn’t make someone approach you, because you’re like ‘oh, they’re a bit, don’t want to be there.’
PS 17
Observation data suggested that, in a few instances, trainers could have used names more often, to strengthen relatedness and rapport; however, relatedness was actively undermined on only two occasions, when the actions of the school contacts compromised the peer supporters’ relationship with the trainers. These occasions were the incident in school 10 (see Chapter 5, Training venues) and when the school contact at school 17 spoke to the peer supporters in a negative way about the trainers:
We said [to the school contact] ‘Do you mind if we finish early, because,’ and I didn’t even say this, but, ‘they’re not very engaged’ . . . She went to the girls and, basically, started talking about us in a very negative way, and saying ‘they’re saying that you have to finish early,’ like, ‘They can’t be bothered to keep you here for as long as’ . . . That was early on in the day as well. So then, obviously, the girls then were a bit annoyed with us . . . So, that really didn’t help the day . . .
Trainer C
The training was successful in helping the peer supporters relate to other pupils/peers and build a sense of empathy for those who do not like being active or who found it hard. One school contact felt that this was helped by the fact that some peer supporters were inactive themselves:
. . . just seeing how, perhaps, other people might think or how they can help them to be more positive, I think will just naturally, hopefully, be something they take as part of them into the future.
SC 4
It has given me a new point of view and perspective to other people’s lives and the barriers and boundaries they could put up and make me understand more about other people.
PS 2
Competence support
Observation data showed that the trainers were helpful and aided learning by answering questions, fully explaining activities and linking them to the role of a peer supporter, as well as adapting activities when the peer supporters were struggling (see Chapter 5, Adaptation). They often prompted girls to find their own solutions to questions and praised their attempts:
. . . they’d explain it really well so we knew what they were saying.
PS 7
It’s difficult when you are explaining things but trying to prompt them to be the ones that are giving the information and talking. I think that was key.
Trainer E
Trainers also worked closely with small groups and provided targeted support, set achievable targets and used progression in activities. This contributed to the peer supporters feeling well prepared to perform their role outside of the training:
Giving some more small and achievable realistic kinds of ideas of what they could do to peer support.
Trainer C
Trainers would reiterate to the peer supporters why they were nominated by helping them recognise the qualities in themselves that made them good peer supporters; this was supported by the content of the training:
. . . that constant reminder that it’s really important, it’s really a great thing you’re about to do. I tried to say that ‘you’re so special, you’re so fortunate, you’ve been chosen, you’ve got the skills; you’re in such a great position to help your friends’.
Trainer B
In hindsight, trainers felt that they could have done more to support some aspects, including greater focus on how peer supporters had been carrying out their roles, who they could support and trying to relate the training activities to their peer supporter role more. Observation data suggested that isolated cases of failing to relate a skill or activity to the peer supporter role were the only examples of undermined competence in the training:
I think we just could work a little bit more on . . . competence . . . So, just like I said, try and highlight the small things that they’re doing, so they really do genuinely feel that they can be a peer supporter and it’s actually quite easy, or it can be.
Trainer C
Peer supporters from two schools felt that the pace of training was too fast (see Chapter 5, Top-up day), which hampered their learning.
Challenges of delivering the peer supporter training in line with self-determination theory
Delivering the training across multiple schools challenged trainers’ ability to remember all of the peer supporters’ names, which compromised their ability to build rapport quickly:
I tried really hard to use everyone’s names, but it was quite difficult because you were going into different schools.
Trainer D
Supporting the peer supporters’ psychological needs during the trainers’ first delivery was a challenge because they needed to follow the ‘session plan guide’ closely and found it harder to respond to cues from the peer supporters (e.g. when to move on; see Chapter 5, Adaptation). This challenge diminished as they delivered more sessions:
In the first one [school], I was desperately worried about keeping to time and everything being perfect . . . and then you just realised that it doesn’t work that way. There’s nothing really that you can do about it apart from . . . be sensitive to the fact that actually, they are tailing off now and they need 5 minutes [a break] . . . delivering something where they are not engaged is just as good as not delivering it at all. So for the second, third and fourth deliveries, not that we were kind of lax, but you just were a bit more organic about things.
Trainer E
Large groups and disruptive behaviour challenged the boundaries of managing the group, and building relationships and a supportive environment:
I think the bigger the group, the harder it is. Just for that quality of conversation and quality of engagement with the exercise . . . You can create more of a cohesive, supportive environment, maybe, with less people. Less potential for disruption and all of those sorts of things.
Trainer G
One trainer felt that delivering the training in school or with a teacher present made it difficult to give the peer supporters autonomy over the training:
Again, it goes back to them being at school, having teachers there and it just felt very, very scripted. They didn’t have much choice. We weren’t able to move them around in groups because of the space and so, yes . . . the idea that they have autonomy, it didn’t really, that wasn’t exercised in the group, certainly.
Trainer E
Peer supporter autonomy support
There was evidence that peer supporters at one school thought carefully about how to approach conversations with peers, approaching conversations in a way that was more collaborative and less didactic:
You don’t want to seem, kind of, superior than them, saying, like, ‘You need to do this’. Most of us probably didn’t know that we had to do that in the first place. So when we started doing it and encouraging people, ‘Come on, I’m doing it, let’s do it together’ . . .
PS 14
There was little evidence from non-peer supporters on the extent to which the peer supporters were supportive of autonomy. Some non-peer supporters described being encouraged to be active, but in a less autonomy-supportive style; others felt that peer supporters had been supportive:
It’s like everyone is encouraging us to be more active.
Yes. And how are they doing that?
Just telling us ‘be more active’.
NPS 2
They’re a lot more supportive in PE, I think, like cheering you on and stuff and trying to make you get more active.
NPS 4
Non-peer supporters in school 1 felt that the peer supporters had not been supportive and had not considered what their peers might enjoy or their preferences for being active:
I would have liked it if they asked you ‘Are you doing anything fitness-wise outside of school?’ and then actually have a conversation with you about it . . . maybe one of them could have come up to me and helped me out with it and be like ‘you’re doing all right’ and everything like that, but they didn’t.
NPS 1
Overall, the extent to which the peer supporters in all schools used autonomy-supportive approaches was unclear; however, the fact that one school demonstrated a considered approach indicated that the training did promote an autonomy-supportive approach.
Receipt of the intervention and the experience of being a peer supporter
Peer supporters reflected positively on their experience, with many enjoying their role. In particular, they enjoyed learning about the importance of physical activity, the skills the training provided them with that improved their communication with others and being able to help their peers. Peer supporters also reported feeling proud to be a peer supporter and having a sense of reward when helping their peers:
I love being a peer supporter.
PS 16
It was good because everyone stayed active and healthy. So you learn how you can allow your friends to stay healthy and yourself.
Do you guys enjoy it?
Yes. When I learnt about it I was passionate about it, but I realised how important it was to me and for other people as well, which I enjoyed . . .
PS 14
Views on trainers
Most of the peer supporters liked the trainers, and both the peer supporters and school contacts thought that they were nice, friendly, helpful (see Table 33), approachable, non-judgemental and ‘found a way to make us have a laugh’ (PS 14):
I think they were really, like, nice and if you ever had anything to talk about and they’d be open to listen, and that was nice.
PS 1
They were just really relaxed and had that relaxed atmosphere and it was something they had to do, but they approached it really well and it was never forced.
PS 4
I thought they were great . . . they built up a really nice rapport with all of the students that were there which, again, for our students, is quite important.
SC 5
The fact that the trainers were relatable and from different backgrounds to those the girls were used to (e.g. teachers and sports coaches) helped them to engage with the peer supporters:
I think that relationship [peer supporter and trainer] worked really well because, obviously, they’re going to be more engaged if it’s people that they can relate to . . . So that, obviously, had the girls interested from the beginning.
SC 1
Only a small number of peer supporters from three different schools made negative remarks about the trainers. These involved perceptions about the body language, temperament and interpersonal connection with a trainer:
She was not really approachable.
Kind of moody.
PS 17
Receipt of content
Peer supporters felt that the training was active, relaxed and included a wide variety of activities, making it more enjoyable and engaging than peer supporters had expected:
Yes, it wasn’t classroom work where you sit there and you have to write it. It was more, everyone was moving and active.
PS 10
Most peer supporters found the 2-day training interesting (mean score ± SD 3.15 ± 0.83; maximum score 4) across all schools. However, peer supporters from schools 5, 7, 10 and 15 perceived the training to be less interesting than peer supporters at other schools, with mean scores of < 3 (see Table 33). The trainers’ ratings indicated agreement with the peer supporters that the peer supporters at schools 7 and 10 may have lacked interest in the training (see Appendix 7); however, the trainers felt that peer supporters at school 17 had very little interest in both the 2-day (mean score ± SD 0.00 ± 0.00) and top-up day (mean score ± SD 1.00 ± 0.00) training (maximum score: 3), which contradicted the peer supporter’s rating of their interest (mean score ± SD 3.67 ± 0.49).
Overall, the training was perceived to be successful in increasing the peer supporters’ knowledge and understanding of physical activity and preparing the peer supporters to carry out their role. Role play using realistic scenarios and practising peer support were particularly valuable:
I thought we were very prepared, well, we were prepared as we could be for what was going to happen. We done loads of different scenarios.
PS 14
. . . we’ve learnt how to bring it up and how to apply it to people we may know.
PS 10
As in the feasibility trial,52 peer supporters and trainers perceived both the ‘peer supporter booklet’ and post box as useful to have in the training days, but they were not widely used.
Enjoyment
Most peer supporters enjoyed the training days (Figure 14); this is concurrent with the trainers’ perceptions (see Appendix 7). Enjoyment increased from day 1 to day 2 and was similar between day 1 and the top-up day. Enjoyment scores were low on all 3 days in schools 10 and 15, and on day 1 and the top-up day in school 7. For school 10, this may reflect the delivery issues that were encountered.
FIGURE 14.
Peer supporter enjoyment of the training on day 1, day 2 and the top-up day. 1 = not at all, 5 = a lot.
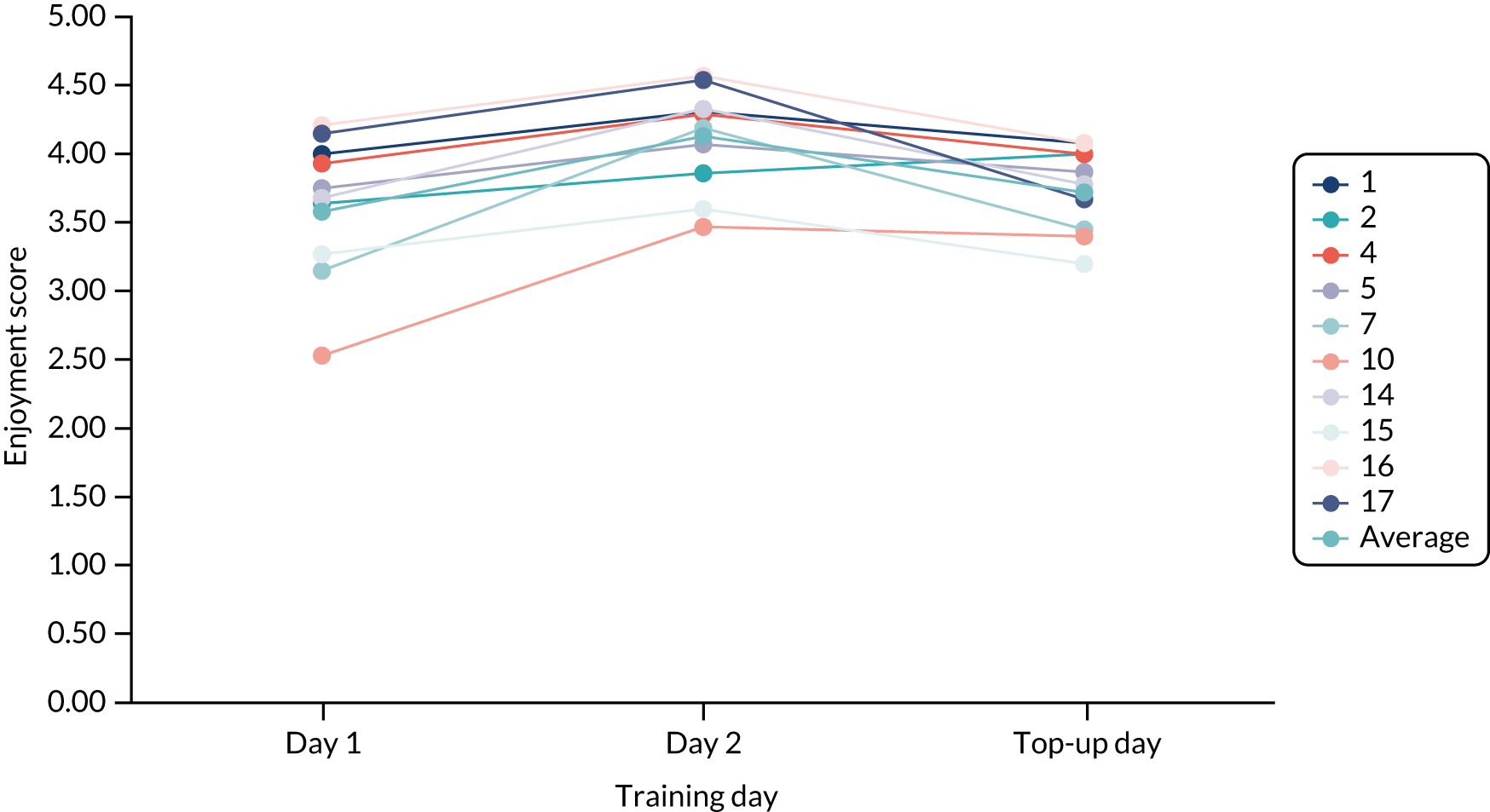
The informal environment, the practical/active activities, being able to learn something new, and the novelty of the training all contributed to their enjoyment:
. . . it was very relaxed and it wasn’t a very formal setting and I really liked that.
PS 14
[When asked what they most enjoyed] Probably like the activities and stuff like that, because we actually got to practise it [peer support] as well, which really helped.
PS 2
A small number of peer supporters also liked the activities that involved teamwork because it allowed them to bond, which they would not have experienced outside the training:
[The] training days were really enjoyable, especially when you got on a break and you got to socialise with people that you wouldn’t normally even see around school and get to chat with, which is really nice.
PS 2
Peer supporters highlighted their enjoyment of the level of autonomy they were given throughout the training, having ‘freedom of speech’ (PS 5) and being given ownership of the tasks, which demonstrated fidelity to the training and its theoretical basis:
. . . it gave you a chance to speak to everyone and find out everyone’s different opinion on the situation.
PS 2
The peer supporters enjoyed the games on all of the training days (see Table 33); however, specific activities were commonly raised as particularly enjoyable across evaluation methods: the ‘listening train’, ‘self-esteem tree’, ‘like a girl’ and ‘peer supporter pyramid’. These activities set a positive tone and focused on building self-esteem and confidence, something which the girls said that they did not often consider when thinking about themselves or their peers.
Peer supporter attitude and engagement
The observed quantitative ratings showed good engagement across each training day in 8 out of 10 schools (mean ± SD: day 1 training, 2.43 ± 0.64; day 2 training, 2.39 ± 0.30; top-up day, 2.47 ± 0.69; maximum score 3). The trainers felt that the peer supporters were somewhat engaged (mean ± SD: 2-day training, 2.30 ± 0.80; top-up training, 2.39 ± 0.78) and involved (mean ± SD: 2-day training, 2.55 ± 0.51; top-up training, 2.61 ± 0.61; maximum score 3) (see Appendix 7). Observations and trainers agreed that the engagement levels of peer supporters in schools 7, 10 and 17 were low.
Across all schools, the school contacts thought that the peer supporters had a positive attitude towards the training. However, trainers made it clear that this varied greatly by school. Some peer supporters were excited and felt privileged to be there, were ready to learn, behaved well, and were focused and enthusiastic during activities. Others were uninterested and did not take it seriously, and some saw it as an opportunity to not attend school; engaging girls with these perspectives was a challenge:
They [PSs at school 10] just weren’t engaged at all. From the beginning, you could just tell there was nothing there . . . It was such a different experience at [school 4]. We couldn’t have got more different [girls]. From the minute they walked in the room they seem excited to be there. They sat down and they were giving you eye contact and they were looking, and they were ready to learn. It was a different group of girls completely.
Trainer B
Two trainers suggested that the variation in attitude was partly because of age, and that older peer supporters were more likely to lack engagement. Reinforcing the school contacts’ view that the intervention would work well in younger year groups (see Chapter 5, Training content), trainers who had also delivered the intervention in the feasibility trial drew parallels between the different attitudes of the girls in the trials:
The first thing is that I was struck by the difference in the age that they are, in what that brought, just inherently. When I did it 3 years ago [during the feasibility trial] it was with Year 8 girls, and this time it was Year 9 girls. [There was] another level of being ever so slightly removed or slightly aloof to it . . . There was just a slightly different level of engagement. It felt like there was, perhaps, a little percentage of innocence that had been lost in that one year group.
Trainer A
Overall, the trainers and school contacts felt that there was a good level of engagement from the peer supporters, although this fluctuated during the training days:
I think there’s always a slight nervousness of not quite knowing what they’re going to be doing and a slight . . . Always, by the end of day 1, they’re a bit louder and more confident.
Trainer G
The interactive nature and variety of the activities (i.e. game-like activities, debate/discussion and teamwork), the relaxed manner and enthusiasm of the trainers, the degree of autonomy and the sense of responsibility that having the role of peer supporter provided the girls with were highlighted as factors that increased engagement and enjoyment:
. . . they enjoyed being trained up as a bit of a leader and being given a bit of responsibility.
SC 1
Top-up day
The top-up day was perceived as important because it reinforced the 2-day training and prompted continued peer support. Alongside reinforcing their peer supporter skills and addressing how to deal with challenging scenarios, the peer supporters valued the opportunity to ask questions and share their experiences of peer supporting up to that point:
I think it was definitely something that was needed. There were some guys that had tried to peer support and had come up against a couple of problems and so having that space to discuss it . . .
Trainer E
I like the top-up day because if you didn’t know how to deal with a certain situation you could ask, so it meant if there was an issue in the weeks before, you weren’t just left on your own. You could talk to somebody else about how to deal with that in the future.
PS 14
The peer supporters’ understanding of their role was broadly similar after the 2-day (mean ± SD 3.75 ± 0.45) and top-up day (mean ± SD 3.80 ± 0.46) training (maximum score 4), and they learned new information (see Table 33). However, all stakeholders agreed that there was not enough top-up day content and that it was repetitive and not active enough. The data in Appendix 8 support this, showing that activities were delivered faster than planned on the top-up day. One school suggested that all content could fit in 2 days, which should be spread out:
The only thing I would say about the top-up day was it felt like there wasn’t quite enough content to fill the time.
Trainer B
Evidence of peer support: fidelity to diffusion of innovations theory
Evidence of peer-supporting activities was obtained using a self-report questionnaire (see Appendix 9) and discussed in focus groups. The most commonly cited types of support offered (‘often’ or ‘very often’) were being active with friends (62.12%), being an active role model (48.48%) and inviting friends to be active with them (43.94%):
I was sort of saying that ‘I really want to do more sports clubs, do you want to join with me?’. So making it not about them, like they’re doing something wrong, so it was about me, ‘will you come with me?’. It’s a technique we learnt at the training.
PS 14
Some peer supporters reported using facts in conversations (others felt that this approach might bring an awkwardness to conversations; see Chapter 5, Challenges to being a peer supporter), which shocked some non-peer supporters, as well as encouraging their friends to be active by making physical activity fun:
Finding a fun way to do it, so, I find peer supporting – well, I don’t really call it that. I’ll make it into a game, so if we’re going to do running in PE, we’ll go on a mad one, like running around the field and we’re actually being active, but you don’t realise it. It’s a way of disguising it.
PS 16
I think people were quite shocked when they found out you need like an hour a day. They were like ‘that’s so much’ and I was like ‘I know, you need to get running,’ and things like that which are shocking facts that nobody really knows.
PS 14
Peer supporters preferred to adopt a subtle approach to their encouragements and felt that peer supporting was quite natural and aligned with their identity:
. . . being quite subtle about it [peer supporting] . . . So not letting them know there’s a reason why you’re telling them all of this.
PS 7
Sometimes it’s like a natural thing you do, to help them to do PE or try and encourage them to do it. It’s like part of who you already are, to try and encourage people as it is.
PS 15
When asked about the types of support provided and the number of friends they had supported, being active with friends was again the most prevalent type of support (40.15% reported providing this type of support to four or more friends); however, the strategy with the second largest reach was talking to friends about the benefits of being active (28.03% reported providing this type of support to four or more friends). The least popular types of support offered by peer supporters were those that involved encouraging friends to adopt more or new activities.
Peer supporters encouraged participation in sports, active travel, walking, running, cycling, after-school clubs and going to the gym. At least one non-peer supporter in the focus groups in each of the seven schools indicated that the peer supporters had been encouraging or supportive in these activities (see Chapter 5, Peer supporter autonomy support) or by using the strategies mentioned above:
. . . me and my friend were going to get the bus to go out, but then I convinced her to walk with me . . .
PS 5
My friend, she talks about being active more now than before she went [to the training]. She wanted me to run with her to work so she could get more active . . .
NPS 15
Peer supporting was made easier when peer supporters were in one-on-one situations with close friends and during PE. Several peer supporters expressed the importance of trust and identifying when conversations needed to be confidential:
I only really stick to my close friends, so I just basically say what I know they can take.
PS 15
I feel like if someone came to you about something, you would want that to be kept to yourself because they come to you about something, you don’t want to then tell other people. That person purposely came to you because they trust you.
PS 4
Other peer supporters felt that working together to encourage their peers to be active was a form of support for each other, boosting their confidence. This was perceived to hold more persuasive power when convincing peers to be active:
. . . when you’re in a friendship group and you’re bringing something up, if the peer supporter is there they can help that plan go forward if the person . . . they can go along with it, I guess, and help you push it . . .
PS 14
If there are more people who have that opinion, like, ‘it’s good to run,’ then it’ll be like ‘oh, it is actually good to run,’ so there’s more . . .
People take it in more.
PS 5
Although we have clear evidence of peer supporters’ attempts at encouraging physical activity among their peers, conflicting accounts from various stakeholders also suggest that peer supporter activity was inconsistent. Almost every school had peer supporters who reported that they had performed no peer supporting, with the majority of peer supporters in school 17 stating that they had done ‘not a lot’ (PS 17) to get messages to friends about being active. This is a direct contradiction of the results from the peer support fidelity questionnaire (see Appendix 9):
I haven’t done any [peer supporting].
PS 1
The non-peer supporters across all intervention schools gave the overarching impression that most peer supporters had not undertaken any work to carry out their role, or at least that they had not witnessed ‘active’ peer supporting by their friends. Some suggested that the peer supporters forgot about the project after the training. The non-peer supporters felt that the peer supporters should have done more to support their friends:
If anything, you wouldn’t notice that they’re trying to be supportive with you because, like, if they’ve been trained to be supportive with sport and anything else, they just genuinely have not been supportive at all. I know for a fact that one of my mates, like, [PS name], she just hasn’t been supportive of anything.
NPS 1
. . . I just don’t think they put any effort into trying to get people who aren’t as active or aren’t as sporty, to try and encourage them to do anything, which I thought was going to be part of it . . . I haven’t seen them making a real effort to try and encourage a broader spectrum of pupils.
NPS 14
On the other hand, it could be argued that the application of a more subtle approach to peer supporting, in line with the training that the peer supporters had received, would preclude the non-peer supporters from noticing some peer supporter activity:
They wouldn’t worry because they don’t realise, which is quite good, because it’s just like having a conversation.
PS 16
Many trainers and school contacts questioned whether or not some peer supporters had done anything to support their peers to be active. Trainers believed that, despite peer supporters providing realistic examples of peer support during the top-up day, some examples may have given the impression that they had provided peer support more than was in fact the case. Most school contacts suspected that this could be true, but believed that the majority of peer supporters would have tried to embrace their role using the strategies from the PLAN-A training:
And then it comes to the top-up day and it was like ‘How have you got on?’. Hadn’t done a thing. Hadn’t done a thing.
Trainer B
I think some of them had [peer supported]. I think some of them probably just said stuff because they knew they had to. But some stuff, like, they couldn’t have just thought that up on the spot.
Trainer D
However, it was also suggested that many peer supporters were supporting their peers naturally, without realising they were doing so; it was only through discussion with the trainers at the top-up day that peer supporters realised how they had been peer supporting:
I didn’t realise I was doing it, but I was being a peer supporter, but I wasn’t consciously thinking ‘Oh, I need to do it and then go and write it in my book’ . . . I didn’t make a conscious decision to go and peer support, I was just doing it more naturally.
PS 2
Others had said ‘we haven’t done anything. We haven’t done anything and we are desperately guilty about it’. Then, actually, when you tweaked a little bit more, they had actually done a few things, they just hadn’t considered that to be peer supporting.
Trainer E
Aside from supporting peers, some peer supporters provided support to their family members more than their friends at school, potentially because they felt more comfortable doing so. It was unclear if, by peer supporting their family, they felt that their role was being executed and, therefore, did not attempt to encourage their peers at school:
I tried to, I think, once with my sister, and I ended up making her walk around [place name] with me. But she enjoyed it, which I guess is the only time it really worked. That’s because I think it’s family.
PS 2
Some of them talked, specifically, about things they’d done with family. There were a couple that had talked quite specifically about that, and maybe because they were the examples that they could remember, or they might have been the times when they felt comfortable to try it out a bit more.
Trainer A
Challenges to being a peer supporter
Challenges to providing peer support included not having the opportunity to do so, peer resistance, a lack of confidence or time, and the distance between home and school.
Peer supporters suggested that a principal barrier was the lack of convenient opportunities to provide support. If their friendship group did not talk about being active or their friends did not express a desire to be more active, the girls felt reluctant to raise the issue for fear of it sounding contrived. This often led to the peer supporters forgetting to peer support, as it was not at the forefront of their minds:
The situation hasn’t really come up [to be able to peer support], but if it did, I think we would be quite prepared because, obviously, we did lots of different situations.
PS 4
It’s like, how to go up to someone and say that they need to be more active without it being taken the wrong way. They’re going to take it the wrong way.
PS 17
Peer supporters found their role particularly difficult, and sometimes disheartening, when peers were stubborn, resistant to suggestions or did not listen. School contacts added that attempts to support could be construed as patronising unless approached carefully and with a co-participation angle:
Some of them can be stubborn and they just think, ‘I’ll do it my way, I don’t need your help.’
PS 4
. . . every other time I asked somebody I got told ‘no’. They said they’d rather do something like watch Netflix [Netflix, Inc., Los Gatos, CA, USA] or play a game or something like that. And it was really frustrating. It made me want to give up, but I didn’t.
PS 2
Peer supporters expressed concern that starting conversations with non-peer supporters, and especially citing facts about physical activity, would seem contrived and be received poorly. This deterred some from trying this approach. Despite fears of causing offence, there was no evidence that this happened:
I think they’d find it a bit offensive, like, ‘Whoa, why are you saying that to me?’
PS 16
. . . if I have a conversation about how not everyone is going to exercise, you can still do an hour a week, I think people just, kind of, get a bit annoyed.
PS 10
Lacking confidence to be a peer supporter or be active themselves held some peer supporters back from overcoming these barriers with their friends. Trainers also noted that confidence in different situations was a concern for many of the girls:
A lot of them still had that barrier [to peer supporting], they said ‘well, my friends still don’t want to do it’ and even though we’d gone through it so much in the first 2 days. So, it just felt like the barriers were that much harder to overcome, or they didn’t have the confidence to try and overcome them, maybe.
Trainer C
. . . they all felt that these stereotypes were in existence, but having the confidence and the tools to actually challenge people about it they lacked.
Trainer E
Trainers felt that some peer supporters did not understand the informal nature of peer supporting, instead believing that peer supporting was a structured, planned event, making them feel like they did not have time to peer support:
I think they still sort of felt, like, that they were required to have these big conversations with facts in and they felt a bit uncomfortable. They felt a bit silly.
Trainer B
I suppose, just the time seemed to be a massive issue. Obviously, this time of year was probably a difficult one for some of them. They’ve got exams or they’ve got other stuff going on. Weirdly, they didn’t feel like they could fit it into their day . . . But that was the common worry and anxiety.
Trainer C
Some peer supporters in school 14 felt that living far from school made it difficult to support their friends. In other schools, girls could suggest active travel or co-participation, whereas peer supporters in school 14 felt that those options were not available to them. The school contact agreed that this limited peer-supporting opportunities within the school:
I live in the middle of nowhere with no city or town anywhere near me. None of my school friends live there, so it’s quite difficult to bring out those conversations because they’re like ‘Shall we do parkrun [parkrun Ltd, London, UK]’ because I’ve got some of my friends to do parkrun on like Saturdays and things. That’s about it. There are no buses where I live on Sundays and it’s just quite difficult.
PS 14
Other challenges included finding it more difficult to peer support around boys, having a limited friend network and having friends that were already active:
. . . have there been any times where being a peer supporter has been challenging?
Yes, PE with the boys is the worst because none of the girls want to do it.
PS 5
. . . it’s almost as if I spoke to all my friends that I talked to and I spoke to all of them about it at the lunch table or on the way home and then that was it. There was nothing else I could really do, because I’d already tried doing it.
PS 2
Overcoming the challenges to peer supporting could have been made easier by working together, but this was difficult if they were the only peer supporter in their social circle (Chapter 5, Outcome of peer nomination, reports that the desired reach of peer nomination was not achieved in all schools):
It was quite difficult for me because I only had one other person in my form who was doing it and I don’t really speak to her very much because she’s not one of my close friends. So it was more difficult to – obviously, it would have been a bit weird if one of us just to go to the other person’s friendship group or something like that because then it would make it more noticeable and obvious.
PS 14
Perceived intervention effects
Effect on peer supporters
Impact of being nominated
The nomination method was praised by peer supporters and school contacts because it was conducted by peers rather than teachers. This meant that the girls who were nominated had a higher sense of peer endorsement and it increased their self-esteem/confidence, especially for those who did not expect the nomination:
It wasn’t like your teacher picked you. It was that people within your year thought you were fit for the role, and that made you feel better about yourself.
PS 10
Impact of the training
Peer supporters from all schools understood their role after the 2-day (mean score ± SD 3.75 ± 0.45) and top-up day (mean score ± SD 3.80 ± 0.46; maximum score 4) training sessions (see Table 33). Some peer supporters reported becoming more active as a result of a greater awareness of their own physical activity levels:
I’ve become more aware of how much I have to do, and not just telling others.
PS 10
I’ve also been doing more exercise since I’ve learnt all the facts and things like that. I think it’s influenced me as well.
PS 14
The training also positively impacted peer supporters’ confidence, communication and social skills, resulting in a more empathetic approach to their peers:
. . . a lot of them were saying that they just felt more self-confident in themselves.
Trainer D
The girls, from my point of view, came out of that knowing exactly what they should be doing, exactly how to support and support in a nice manner, rather than just holding that everybody has to do more exercise. So, the training side of the peer supporters worked really well.
SC 14
I feel like I’ve learnt how to communicate with people and how to support people better than I already could.
PS 1
. . . now I’ve learned how to go with a nicer approach and more advise people and be like ‘come on, I understand, let’s do it together’.
PS 16
However, after the training, confidence to pass positive physical activity messages to their friends varied between schools, and in half of the schools the average score was lower after the top-up day (see Table 33).
Finally, training strengthened peer connections and helped the girls to develop as leaders:
There’s probably little groups that don’t actually know each other. So it was nice that they got to interact because that’s maybe something that they don’t necessarily do while they’re at school.
SC 5
I think it helped them develop, almost, their leadership skills, in a way. It helped develop them as role models.
SC 7
Impact of being a peer supporter
The act of being a peer supporter impacted the girls in different ways depending on their experience; however, many reported that it motivated them to keep active. It also helped them to develop broader transferable skills, such as kindness, empathy and the ability to build new relationships. School contacts felt that the training fostered social maturity:
I feel like I’m doing more sport. Obviously, I did stuff before, but I feel like I’m more conscious, ‘oh, I haven’t done anything today, I need to go for a walk’.
PS 14
Another one [impact of being a peer supporter] is building a relationship, because I wasn’t really close to this girl in my science class. And then I was like ‘do you want to go swimming?’ just out of the blue. And then we ended up going swimming, and we built a decent sort of friendship.
PS 1
Although non-peer supporters believed that they had not witnessed peer supporting in action, there were some indications that they had seen changes in the peer supporters. They felt that their attitudes towards being active themselves had changed in that they wanted to be more involved in active opportunities and their confidence had increased. Non-peer supporters from one school said that the peer supporters had started to interact with girls they did not know before:
In PE, say for sports day, they’re volunteering for more things and stuff and they’re more active in PE.
NPS 15
She [a peer supporter] wasn’t confident contacting people out there and stuff like that. And now that, after PLAN-A, I feel like she contacts more people and she’s more active with people and stuff.
NPS 5
The non-peer supporters in the other half of schools said that they had not noticed any changes in the peer supporters, particularly those who were already active:
The people that you took there are group of them who are quite sporty already, so they just stayed as they were . . .
NPS 1
Effect on other girls in Year 9
Many peer supporters felt that they were successful at encouraging and supporting their friends to be active and could give examples of how they did this (see Chapter 5, Evidence of peer support: fidelity to diffusion of innovations theory).
Some peer supporters felt that many non-peer supporters were more open to being active and enjoyed physical activity more. Two school contacts agreed that Year 9 girls were now more engaged and supportive of each other in PE:
I think we’ve definitely seen an increase in engagement in lessons. I think they’ve [all Year 9 girls] all been a lot more supportive . . . they’ve all been so supportive of each other and cheering each other on. Some of them have run extra laps with the slow ones, to keep them going, which would never have happened before we did this at all.
SC 10
Non-peer supporters at school 7 felt that girls in their year may have become more confident in PE and in front of boys since the intervention began:
The boys, they would just play normally, but the girls, I think they would just stand back because they were too embarrassed or something if they fall over or anything like that.
And, since PLAN-A, has that changed at all?
I’d say for just half of the girls, yes.
Non-peer supporters at another school said that there is now less pressure to be good at PE. A small number of non-peer supporters and school contacts from different schools reported uptake of new activities since the intervention began, including walking, running, going to the gym and being outside together, as well as increased sign-up to school clubs. Nevertheless, they were unsure whether this was due to PLAN-A or seasonal variation. Conversely, many non-peer supporters stated that they had not started new physical activity since the intervention began:
[When asked how girls’ confidence has changed in PE after PLAN-A] it’s just that we don’t feel that we have to do well in PE. That might be a teacher or it might be just in general, the people. We don’t feel like we’re pressured to be amazing sports people.
NPS 10
After you did PLAN-A, a lot more girls will go to the gym or try it and a lot of people liked it, so they kept on going back.
NPS 4
I know there are a few Year 9 girls that now want to join the cricket after school as well, but then I don’t know whether that’s just because it’s warm weather now and they’re a lot happier to be outside than inside.
SC 1
Some peer supporters were unable to or did not carry out their role and were therefore unsure whether or not they had had any impact on their peers. Some peer supporters who did peer support did not think they had any impact and did not notice any changes in physical activity. Any impact they may have had was described as not significant or long-lasting. Some attributed this to the fact that non-peer supporters were unaware of the project and what the peer supporters were trying to do:
Not really [been successful in encouraging others to be active], just because it’s quite hard to just go up to someone and start the conversation with them if you’re not sure why they have that barrier.
PS 17
I’ve had some success, but it’s not been an overwhelming amount where people have suddenly gone up the amount of activity they’ve done. It’s normally a one-time thing that happens. And then it doesn’t happen again.
PS 2
At most schools, peer supporters going to the training days initially sparked interest among non-peer supporters, but this diminished with time. Most non-peer supporters did not know why certain girls went away for the training unless the peer supporters told them, which they found hard to explain or understand:
I think some people do know where we went, because when they go ‘Where’d you go?’ some of us went ‘Well, we did this, and these are the facts,’ but I think they just forgot about it over time.
PS 5
Some school contacts corroborated non-peer supporter claims that taking part in data collection, specifically wearing the accelerometers, made them more aware of and thus increased their physical activity:
I think when we used the belts, definitely. I think when the belts came in, the girls were actively thinking ‘Actually, I’m being tracked, and I’m not doing very much’. I think that would’ve helped participation. I really liked that side of it.
SC 7
The consensus from non-peer supporters was that the intervention had no social effects, stating that there were no differences in friendship groups or how they interacted. However, comments from school contacts challenged this view, as some felt that conversations between different girls had increased:
We didn’t really have a change in our friendship group.
NPS 14
I think a social one in terms of them having the conversations. The freedom between the PLAN-A students and the non-PLAN-A students to have those conversations.
SC 16
Overall, all stakeholder groups were uncertain about whether the intervention had resulted in any social or attitude changes in other girls in Year 9, although this would be difficult to detect or measure robustly in any case. None had observed pervasive changes in attitude towards, confidence in or talking about physical activity since taking part in PLAN-A:
Do you think there has been an impact on the other girls in Year 9 who weren’t peer supporters?
I honestly don’t know. I don’t think I could say either way. Without talking to them, I don’t think I could say outright ‘Yes, it has,’ or ‘No, it hasn’t,’ if I’m honest.
School context
School attitude, curriculum and policies
The project aligned with key aims within the PE departments of most schools around improving participation and leadership and was therefore considered a priority within PE in those schools. In several schools, PLAN-A aligned with the school ethos, as healthy lifestyles and physical activity were embedded in their school values; however, only one school (school 14) saw supporting the project as a school-level priority:
In terms of the PE department, our aim is to make sure we’re giving the skills and the confidence to all of our students to, hopefully, instil life-long involvement in physical activity and healthy lifestyles.
SC 16
It was ideal and it brought in everything that we want to push forward to the girls, with the added bonus that, actually, if it did work, which you guys decide, we get the added bonus of increased fitness and health of our girls as well, so it was perfect.
SC 14
In one school, the project was not seen as a priority because lessons and exams were of higher importance:
It wasn’t really very high in our priorities as a department or a school. Yes, the day-to-day running of lessons and exam results and things like that were a higher priority.
SC 17
In school 10, the leadership’s attitude to the trial as a whole was described as ‘poor’ (SC 10) by the school contact, which they contextualised by explaining that the senior leadership team (SLT) had not properly read the trial information and did not fully understand what was required of the school or the benefits to the participants:
Maybe, the head teacher and SLT, I don’t think they fully understand the benefits and what you’re trying to get out of it.
SC 10
Just because they lost the paperwork. I don’t even know who actually signed all the paperwork and who, actually, was the first person. Because our staff turnover last year was really high. I reckon at least three other people who took it forward to SLT have probably left.
SC 10
Appendix 10 shows that school policy scores (with higher scores indicating that the policy is more supportive of physical activity) were largely similar between intervention (mean score ± SD 7.50 ± 1.51) and control schools (mean score ± SD 7.40 ± 2.62; maximum score 12). However, three schools (control, n = 2; intervention, n = 1) received very low policy scores (i.e. ≤ 6).
Appendix 11 shows the level of physical activity throughout the wider curriculum of each school. The mean score ± SD for the control schools (3.80 ± 1.62) was marginally higher than that in the intervention schools (3.20 ± 1.62; maximum score 8); however, the difference was small and there was high school-to-school variability, so any difference between arms would not have been consistent across all schools in each arm.
Physical activity provision
School environment audit data (see Appendix 12) that examined the facility provision at each school to support active travel, sports and general play (see Chapter 2, School context) were highly variable between schools, but did not show meaningful differences between the intervention (mean score ± SD 81.90 ± 12.61) and control group (mean score ± SD 84.55 ± 15.00; maximum score = 164). Comparing baseline school-level physical activity data with physical activity provision scores showed that a low score for physical activity provision (e.g. schools 12 and 17) appeared to be crudely associated with low levels of physical activity (Figure 15).
FIGURE 15.
School-by-school comparison of facility provision scores over baseline MVPA minutes.
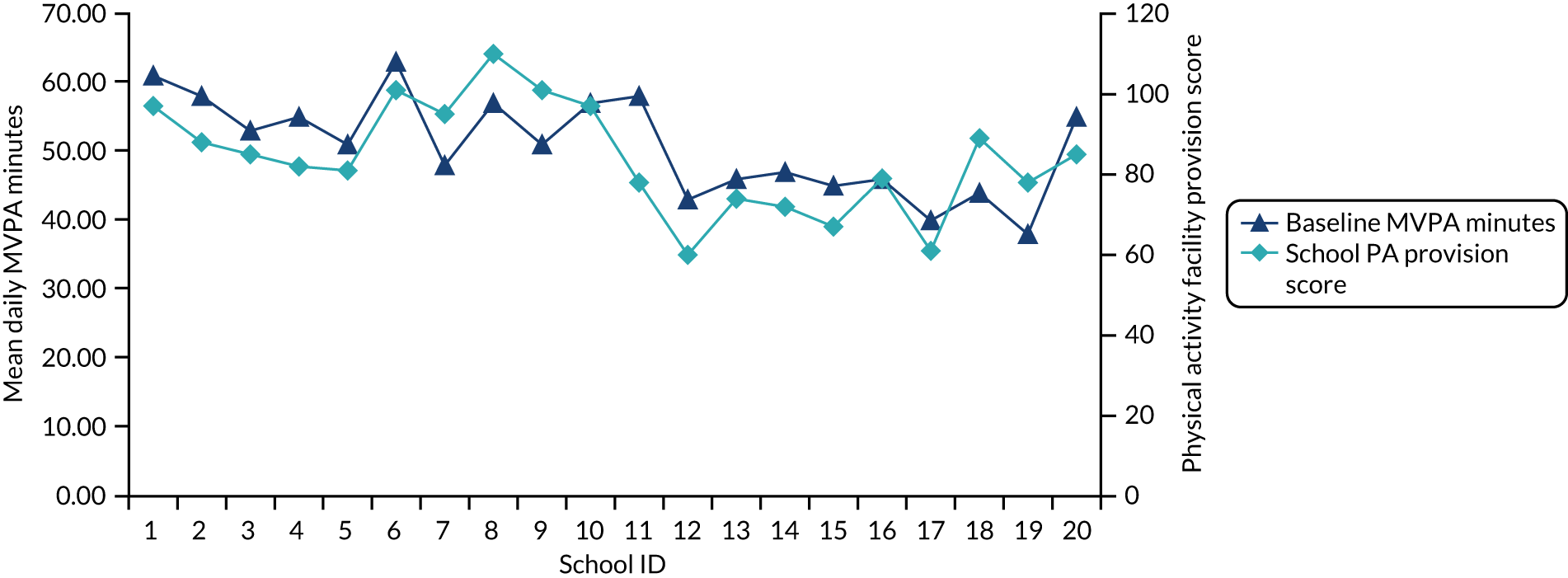
No schools took part in any other physical activity research projects during this trial, and just three (control, n = 2; intervention, n = 1) had any involvement with local initiatives that might have influenced physical activity behaviours (see Appendix 13). Termly changes to PE provision or extracurricular opportunities between T0 and T1 were balanced between trial arms; however, four control schools described a change in the focus of PE for girls, moving away from competitive sport and towards well-being and health. School contacts in those schools described a gender-specific consideration not just for what girls enjoyed, but also for what would motivate them to continue to be active beyond school. No intervention schools reported a similar change:
We also look at modern influences such as the interest girls have in exercise to music and dance. So, ‘Fitness Marshall’- and ‘Body Pump’-type exercises have been incorporated into the health and fitness sessions of our PE curriculum. For one of their 2-hour PE lessons, there is a ‘mass fitness activity’ that has been influenced by modern fitness trends, such as HIIT [high-intensity interval training] or exercise to music, with the aim of inspiring them to exercise once they leave school.
SC 3
Public stakeholder interviews
Intervention weaknesses
When asked about potential factors limiting the effectiveness of school-based, individual-level interventions to increase physical activity in young people, respondents described a range of interconnected factors. These stemmed from the school as the setting, because the priorities of individual schools do not necessarily allow space for an agenda that facilitates increases in physical activity or a culture that promotes it throughout the school:
I think, obviously, the pressures upon schools in terms of standards, progress and achievements, obviously, has a significant factor as well, when it comes to making decisions on what schools prioritise and what resource they put behind that.
External stakeholder (ES) 8
Additional issues were highlighted, including failure to consult the end user and engage parents in design stages, and a lack of wider support for change:
We’ve made the mistake for years of putting on activities for young people, as opposed to understanding what the needs of the young people are and delivering what they want.
ES 2
There was an overall view that many individual-level interventions were reliant on isolated champions, were implemented in environments in which physical activity was not a priority and failed to consider the scaffolding that is necessary for sustained change within and outside of school.
Whole-school approach considerations
The consensus among stakeholders was that adoption of a whole-school approach to promoting physical activity is contingent on sympathetic school leadership, with leaders needing to be convinced of the value of the approach for their school and students. Of primary concern to school leadership is the criteria that the Office for Standards in Education, Children’s Services and Skills (Ofsted) in the UK use to evaluate schools, so several stakeholders recommended aligning school assessment criteria with well-being outcomes to increase adoption of whole-school approaches to physical activity:
. . . if you’re going to have a whole-school approach, it has to relate to those wider measures for schools to really buy into it, certainly at senior level.
ES 8
Stakeholders reported that any whole-school approach must work around school-specific challenges at the point of implementation, including, but not limited to, resource issues, staff capacity and confidence to adapt lessons, and pressure to deliver against existing Ofsted criteria. Consultation in design is therefore vital to creating a flexible and sustainable offer for schools that meets the needs of their community and is deliverable by their staff:
. . . making sure we can be as flexible as possible for schools, to enable them to take an approach that best suits their circumstances.
ES 8
Culture change within schools was discussed at length and framed as both a crucial component in any whole-school approach and the main objective of the approach itself. All respondents agreed that there must be a united approach within the school to create culture change, but that the support and cooperation of the wider community around each school is also crucial to creating an environment in which behaviour change could be maintained:
Because if your environment and your structures and your attitudes aren’t changing, I’m not sure you get any real meaningful change either.
ES 9
Research used and needed
The interviews highlighted that the use of research differed by organisation, and some stakeholders expressed a lack of confidence to source and apply high-quality relevant research to underpin intervention design or evaluation. Providing robust research that was easily accessible and linked physical activity to measurable educational outcomes was highlighted as a key need:
I need to present data that shows that engagement has produced that educational outcome that has improved their chances of educational success or social mobility . . .
ES 10
Respondents reported that case studies are a preferred research model for schools to see if and, crucially, how programmes work in practice. This is an important finding as the majority of research focuses on summary data and does not follow the case-study approach. There is an appetite for a united approach between research institutions and public-sector organisations to co-produce useful evidence to drive the physical activity agenda forward:
I think there has got to be a more coordinated approach to influence the government as well. I think we need to be looking at potential policy recommendations and initiatives . . .
ES 6
Impact of COVID-19 and post-COVID considerations
At an unprecedented level, schools have had to change how they operate in the face of the COVID-19 pandemic. Respondents felt that these changes had reduced the opportunities to be active at school and added barriers, thereby exacerbating existing health inequalities and increasing the complexity of implementing school-based physical activity interventions of any kind. It was also felt, however, that the importance of physical activity for well-being had been highlighted during this time and that this should be harnessed to encourage uptake from schools by reframing the benefits of physical activity to aid post-COVID recovery and linking it with school attainment objectives:
I suppose, the opportunity, you can argue, is to reframe the role of physical activity as a real positive in terms of what we’re trying to do now within schools.
ES 4
Post COVID, virtual physical activity offers could be used as a strategy for schools and organisations to engage a broader range of pupils and address provision inequalities:
We’re always going to run a virtual element because we’re attracting children that wouldn’t do that in a team.
ES 2
Summary of process evaluation key findings
This chapter has provided a lot of information about the delivery and receipt of the PLAN-A intervention. Table 35 presents the key findings of the process evaluation.
| Domain | Findings |
|---|---|
| Reach |
Peer nomination was largely effective at identifying appropriate girls, but some questions remain about representativeness across social networks in some schools 86.39% of invited peer supporters consented to take part. The main reason for non-consent was concern over missing lessons |
| Dose |
84.33% of consented peer supporters attended all 3 days of training All 3 days of training were fully delivered in nine schools. In school 10, issues on the top-up day meant that the dose was reduced |
| Delivery fidelity | Objective fulfilment scores from observations and trainer-rated evaluations of delivery indicate good fidelity to session plans and intervention objectives overall |
| Delivery quality |
Overall, delivery quality was perceived to be high Schools 10 and 17 were perceived to have a lower quality of delivery than others An autonomy-supportive delivery style was evident in all schools, although disruptive behaviour in schools 7, 10 and 17 made this challenging In two schools (schools 7 and 10), delivery was conducted on the school site. This caused some behaviour issues and had negative effects on engagement, interest and enjoyment, according to the trainers, school contacts and peer supporters In two schools (schools 7 and 14), the group size was > 20, which presented delivery challenges for trainers and affected engagement |
| Intervention receipt |
Enjoyment of training was high, and comparable to that in the feasibility trial52 Enjoyment scores were lowest in schools 7, 10 and 15, particularly on training days 1 and the top-up day Engagement varied between schools, but was generally good across all 3 days |
| Mapping to trial outcomes |
Process data indicate that schools 15 and 10 had low enjoyment scores and school 17 had relatively low delivery-quality ratings. Schools 15 and 17 recorded the lowest reduction in weekday MVPA at T1 out of the intervention schools School 10 had intervention delivery issues, resulting in a lower dose and poorer engagement and enjoyment of training; however, their mean T1 weekday MVPA minutes were equivalent to those of other schools that did not cite any issues, suggesting that implementation was not the leading cause of a difference in the primary and secondary outcomes between schools Overall, the process data do not correlate with the school-by-school change in weekday MVPA minutes, suggesting that delivery factors do not explain why intervention schools saw no positive intervention effect on weekday MVPA Schools 1 and 2 recorded the lowest levels of weekday MVPA at T1 out of all 20 schools: an average decrease from T0 of 11.81 and 12.27 minutes, respectively. There is no evidence that the intervention was poorly delivered or received in these schools. However, historical weather data show that, during the T1 data collection period, both areas experienced extreme adverse weather conditions and heavy flooding that may have prevented children from participating in normal physical activity opportunities |
Comparison with the PLAN-A feasibility trial
There were several differences between the process evaluation of the feasibility trial55 and the definitive trial of the PLAN-A intervention. We think that it is useful to present the data that might inform our understanding of these differences, as well as the perspectives of one researcher (KW) who observed intervention delivery and two trainers who delivered the intervention in both trials.
The two trials produced very similar results in terms of dose, fidelity and quality of intervention delivery, suggesting that the intervention is scalable. However, certain factors in the definitive trial may have led to differences in how the intervention was received compared with how it was received in the feasibility trial. 52 The principal difference between the two trials was the age of the participants: girls were in Year 8 (i.e. aged 12–13 years) in the feasibility trial and in Year 9 (i.e. aged 13–14 years) in the definitive trial. The transition to the General Data Protection Regulations (GDPR)97 between the two trials meant that the consenting procedures and age of participants had to change to be GDPR compliant. This presented a conflict between the theoretical underpinning of the intervention (i.e. DOI, effectively, that the trial is conducted within a naturally occurring social network, e.g. a school year group) and the GDPR rules on use of opt-out consent. 97 To use an informed, opt-out consenting procedure, girls had to be aged 13 years and, therefore, in Year 9. Trainers and researchers alike felt that this had a significant impact on delivery factors and receipt of the intervention.
In the definitive trial, 9.58% fewer girls consented to be a peer supporter than in the feasibility trial52 (86.91% vs. 96.49%, respectively). The main reason for this was not wanting to miss important lessons. This may be a product of Year 9 participants (and their parents) placing greater emphasis on academic focus. Being slightly older, the peer supporters in the full trial were able to understand activity explanations and grasp the key purpose of the training more quickly than the younger peer supporters in the feasibility trial. 52 The trainers who had delivered the intervention in both trials suggested that this may have led to the peer supporters perceiving the training as repetitive and lacking sufficient content. By contrast, during the pilot phase of the feasibility trial,52 refinements were made based on participant feedback to ensure key themes and activities were reiterated. A perception that activities were repetitive may have contributed to reduced engagement and interest during the training in the definitive trial, which was found to be an issue in some schools.
Being 1 year older also seemed to impact the girls’ attitude to the project. Year 9 peer supporters appeared to be slightly more indifferent during the training than those in Year 8, as if they did not want to be seen as too ‘keen’ or to care too much about the training for fear of appearing ‘uncool’. Despite being interested in what they were learning, they appeared to lack the motivation to overcome the barriers to peer supporting, that is when their peers were stubborn or resistant; the peer supporters in Year 8 seemed more invested, and more willing to follow the trainer’s instruction and carry out their peer supporter role.
Year group sizes were larger in the schools in the definitive trial than in the feasibility trial52 (mean 92.05 vs. 75.16, respectively), which could be a result of delivering across more schools (20 vs. 6, respectively) and/or Year 9 being an intake year for many secondary schools. This resulted in larger peer supporter groups in the definitive trial than in the feasibility trial. 52 This was a key challenge to delivery for the trainers in the full trial, mainly through challenges to behaviour management that undermined the quality of delivery. It was also difficult to find community training venues that were large enough, which presented challenges with regard to space constraints.
The training being held on site in one school in the feasibility trial presented challenges of frequent disruption from other pupils and peer supporters being able to leave for other school commitments. 52 In the two schools that delivered on site in the full trial, these challenges were similar, yet more pronounced, with the addition of more disruptive behaviour from the peer supporters. This could also be related to the older age group, as they may have been more confident and familiar in their school setting to behave in such a manner.
Chapter 6 Discussion
Parts of this chapter have been reproduced with permission from Willis et al. 1 and Jago et al. 2 These are Open Access articles distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: https://creativecommons.org/licenses/by/4.0/. The text below includes minor additions and formatting changes to the original text.
The main objective of this trial was to assess whether the PLAN-A programme was effective and cost-effective at increasing objectively measured physical activity among Year 9 girls (i.e. those aged 13–14 years). ITT analysis found that there was no intervention effect on the primary outcome of weekday MVPA minutes at T1, with weak evidence of a negative treatment effect in the intervention arm (–2.84 minutes, 95% CI –5.94 to 0.25; p = 0.071). Further adjustment for variables imbalanced at baseline (i.e. free school meals, travel to and from school, and IMD score) slightly changed the magnitude of this difference (–3.57 minutes, 95% CI –6.75 to –0.39; p = 0.028). These results show that there was no evidence that the PLAN-A intervention was effective in increasing adolescent girls’ physical activity. These findings contrasted with the feasibility trial outcomes, for which evidence of promise to increase MVPA at 12 months’ follow-up was observed (a 6.1-minute difference in weekday MVPA favouring the intervention arm over the control arm). 51 Because of the relatively small size of the feasibility trial, this definitive trial was conducted to determine whether or not this promise would hold true at scale and therefore merit widespread dissemination. There were also no between-arm differences in the secondary outcomes of weekend MVPA and weekday and weekend sedentary time. These findings are comparable to those in the feasibility trial,52 except for weekday sedentary time, for which, at the 12-month follow-up in the feasibility trial, girls in the intervention arm were sedentary for 23 minutes fewer per weekday than girls in the control arm. The data reported here highlight that dissemination of the PLAN-A programme would not be beneficial to the physical activity levels of adolescent girls.
An embedded process evaluation was conducted during and after the implementation of PLAN-A to provide insight into the fidelity, quality and receipt of the intervention. All 10 schools randomised to the intervention arm received all 3 days of the intervention (i.e. the peer supporter training). However, school 10 received a reduced dose on the top-up training day, which was attributed to a request from the school for the peer supporters to leave early. This school also experienced delivery issues on day 1, which the trainers felt had a significant effect on the engagement of the peer supporters. Training attendance varied between schools, but, on average, was high across all 3 days (84.33%). The target of training 15% of the year group to be peer supporters (the required amount for sufficient peer-group diffusion) was achieved across the schools in the intervention arm.
Fidelity to the peer supporter training session plans and overall intervention design was good. All sessions were delivered in line with underpinning theoretical principles, but trainers had difficulties upholding these at their first sessions, when the group size was large or when peer supporter behaviour was disruptive. Overall, the training content was engaging, albeit slightly repetitive, the peer supporters enjoyed the sessions and had positive feedback for the trainers. The training prepared the peer supporters to carry out their role, in which they used a variety of strategies. These included being active with peers or inviting them to be active together, talking about being active and being subtle in their approach in doing so.
The intervention training and delivery costs were modest, ranging from £20.85 to £48.86 per pupil, with the majority of the cost being borne by the local authority providing the training. In unadjusted analyses, there was some evidence that, at T1, the deterioration in the KIDSCREEN-10 and EQ-5D-Y VAS scores was less in the intervention group than in the control group. However, the differences were small and consistent with no effect of the intervention in adjusted analyses. The primary economic analysis indicated that the intervention was both more costly and less effective at increasing MVPA than usual practice. Exploratory analyses demonstrated a low probability that the intervention was cost-effective at conventional National Institute for Health and Care Excellence (NICE) cost per QALY willingness-to-pay thresholds.
There were two findings of note in the current trial. First, the percentage (31%) of girls in the sample who met the CMO guidelines of an average of 60 minutes of MVPA per day across the week was higher than the national average of 9%, according to Health Survey for England data. 98 Second, the subgroup analysis revealed a positive treatment affect among girls who had a high proportion (i.e. > 85%; 4.7% of the sample) of sedentary time at baseline, meaning that ‘high-sedentary’ girls in the intervention arm had higher MVPA than those in the control group at T1. These findings suggest that participants in this trial were more active than the general population and that there is a potential benefit among those who were the most sedentary, but, as this was not the primary analysis, this should be treated with caution and as an interesting observation only.
Post hoc exploration of mitigating factors
Post hoc analyses of school-by-school outcomes indicated that two schools in the intervention arm (i.e. schools 1 and 2) exhibited significantly greater decreases in MVPA between T0 and T1 than the other schools in the trial (see Figure 4). Examination of the process evaluation data provided no obvious explanation for this marked difference as both schools demonstrated good fidelity to the intervention delivery, and focus groups in these schools did not highlight any issues among the year group. However, further analysis showed that these two schools experienced extreme weather (i.e. sustained storm systems and severe flooding) in their local areas during the T1 data collection period. This could have restricted opportunities for children in these two schools to be active outdoors, such as after-school and community sport, informal leisure time play with peers in and out of school, and active travel to and from school. These weather events may have accounted for an unexpectedly steep decline in observed MVPA in the two schools that exhibited good adherence to the intervention and had school environments that were supportive of physical activity (see Appendices 6–8). Therefore, these data highlight the challenge of using single periods of assessment to capture complex behaviours such as physical activity. 99,100
Although this probable explanation may account for the severity of the decline in physical activity in these two intervention schools, it does not account for the fact that no overall intervention effect was observed in the ITT analyses. Moreover, review of Figure 4 would suggest that, although these two schools logged noticeably poorer average MVPA at T1 than the other eight intervention schools, there is no difference in the overall pattern across all intervention schools. Furthermore, post hoc analyses indicate that, in the peer supporter subgroup, the decline in MVPA was more pronounced (although small in magnitude) than in the non-peer supporter group (an adjusted difference in T1 MVPA between peer supporters and non-peer supporters in intervention schools of –2.25 minutes, 95% CI –5.27 to 0.22; p = 0.071), suggesting a possible negative treatment effect. This finding is in contrast with the findings of the feasibility trial,51 as well as early research into peer-delivered interventions, which found that the peer supporters were often more positively affected than the non-peer supporter group. 101
Participants in this trial were 1 year older than those in the feasibility trial,52 in which evidence of promise was found. The participant age group in this trial was changed from Year 8 (i.e. aged 12–13 years) to Year 9 (i.e. aged 13–14 years) to allow participants to provide their own consent and meet new ethics requirements that came into force because of the European Union GDPR legislation,97 which was introduced in 2018. Although we cannot be certain what effect this had on the outcomes of the trial, trainers and a researcher who had delivered the intervention in both the feasibility trial and definitive trial believed that engagement was poorer with the older year group, and that the older pupils were more indifferent to the training and the peer supporter role, which could have compromised the DOI delivery model.
Using school-level process, environment and policy data, we explored the convergence with school-by-school change in the primary outcome to further understand the trial findings. In the intervention schools, process data evaluating the delivery quality of peer supporter training sessions showed that perceived delivery quality, pupil engagement and enjoyment scores showed little correlation with MVPA change at a school level (see Table 35). Even on-site delivery, which the process evaluation highlighted as a key factor that negatively affected pupil engagement, enjoyment and delivery quality, did not predicate poorer MVPA outcomes in those schools that were affected by it, such as school 10 (the associated delivery issues are described above).
In the control arm, schools 6, 9, 12 and 13 accrued the smallest reduction in weekday MVPA from T0 to T1 out of all 20 schools (e.g. school 6 saw a 2-minute improvement). School environment and policy audit data indicated that schools 6 and 9 were well provisioned for physical activity, although no more so than some intervention schools that exhibited greater declines in MVPA between time points, but that schools 12 and 13 were not well provisioned. Similarly, the number and range of termly physical activity opportunities, as reported by school contacts, did not change meaningfully between T0 and T1 in any of these schools (see Appendix 4), shedding no further light on what makes these schools different from others in the trial that would account for the reduced decline in physical activity compared with that of other schools in the trial.
One operational difference between schools in the trial arms in PLAN-A was that four control schools changed the focus of their PE curriculum for girls away from competitive sport and towards health and well-being in the time between T0 and T1 measurements, but no intervention schools reported doing so. School 6, which saw a 2-minute increase in mean weekday MVPA between T0 and T1, was one of these schools and underwent a change to become an academy trust during that time. The rebranding of the school came with a shift in school priorities towards pupil well-being. Reportedly, this shift included changing the types of activities undertaken with girls in PE to align more closely with current group-based, health-focused exercise trends that are ‘popular with girls their age’. Collectively, these data provide a range of possible explanations for the differences between the results of the feasibility trial52 and the findings reported here, but there is no clear single factor, and the results could also be a function of something that we did not assess. As a result, there are a number of possible explanations for the project findings, but a degree of uncertainty remains.
Health economics
The direct cost of physical inactivity to global health systems in 2013 was conservatively estimated to be $53.8B (international dollars),102 with an additional $13.7B in productivity losses. 102 Effective prevention during adolescence is urgently needed to reduce health system costs, improve health and prevent premature mortality.
The mean cost of the PLAN-A intervention per school was similar to that estimated in the feasibility trial52 (£2817 vs. £2685, respectively) and in other school-based physical activity interventions (GoActive,91 The Bristol Girls Dance Project103 and Girls Active104) targeted at a similar age group. As the PLAN-A intervention was targeted at girls in Year 9 only, the cost per pupil was higher than that in the Girls Active104 or GoActive91 interventions, which were targeted at all secondary school girls and all Year 9 pupils, respectively. Nevertheless, the mean cost per pupil (£31) of the PLAN-A intervention was considerably lower than that of the Physical Activity 4 Everyone intervention, which involved more intensive classroom-based physical activity and implementation strategies ($394 per pupil in 2014 Australian dollars). 105 Providing peer supporter training to encourage physical activity in girls has the potential to be affordable for schools and cost-effective for society, if it results in a sustained improvement in MVPA.
School-based physical activity interventions might demonstrate cost-effectiveness in the short term if the initial intervention costs are justified by improvements in HRQoL or are offset by reduced use of health services. Observational and experimental studies have demonstrated the association between physical activity and higher levels of psychological well-being, and the potential for physical activity interventions to improve adolescents’ mental health. 106 Our data highlight the scope for improving the mental health of girls in this age group, with more than half of girls reporting feeling ‘a bit’ or ‘very’ worried, sad or unhappy at the baseline assessment. However, this potential has not been borne out in economic evaluations91,103,104,107 of school-based physical activity interventions that have used preference-based measures of HRQoL, such as the CHU-9D or EQ-5D. In large part, this is because of the lack of a meaningful effect of these interventions on physical activity. There are also concerns that these outcome measures might not be sensitive enough to detect the small improvements in mental health that might be expected from school-based physical activity interventions. 108
As with most other evaluations of school-based interventions, we did not assess whether or not the intervention costs were offset by reduced use of health services during the trial. In the Girls Active trial, which elicited this information from girls at 7 and 14 months post baseline, analysis was hampered by high levels of missing data and concerns about the accuracy of recall. 104 Given this, the use of routine data from electronic health records might be the most efficient and unbiased way to capture this information in future work.
Most economic evaluations of school-based physical activity interventions that have evaluated short-term cost-effectiveness in terms of cost per QALYs have concluded, as we do, that there is insufficient evidence that the intervention costs are justified by initial improvements in HRQoL. One exception to this is the Daily Mile evaluation in primary school (i.e. aged 4–11 years) children, which found that there was a high probability that the intervention was cost-effective in girls, but not boys. 109
A second pathway for school-based physical activity interventions to be cost-effective is through the long-term prevention of activity-related health conditions, such as cardiovascular disease, type 2 diabetes and some types of cancer. This would require that any short-term changes in physical activity and sedentary behaviour are sustained for long enough after the intervention period to have an impact on disease incidence later in life. For many years, work in this area has been restricted by the lack of high-quality models that would allow the intermediate outcomes measured in trials, such as MVPA or body mass index in adolescents, to be extrapolated over the life course to predict disease incidence and associated health-care costs, morbidity and mortality. More recently, decision analysis models have been developed to simulate the lifetime costs and outcomes of changes in body mass index110 and MVPA111 in adolescence. These models demonstrate the potential for interventions with a similar cost to PLAN-A to be cost-effective even if the impact on MVPA is modest (i.e. approximately a 5-minute improvement) and the effect is relatively short-lived (i.e. tapering to no effect by 7 years). 111 This is a moot point for PLAN-A, in which we did not observe any short-term effect on MVPA. However, it does demonstrate the importance of conducting long-term follow-up of participants in trials of interventions that do find evidence of short-term improvements in physical activity.
Psychosocial variables
There was no evidence that the intervention affected girls’ self-esteem, which was specified as a secondary psychosocial outcome. This is not dissimilar to the Girls Active intervention,112 which reported a very small increase in self-esteem in favour of the intervention group 7 months post intervention but a null effect at the 14-month follow-up. In both the intervention and control groups, psychosocial variables decreased between Year 9 and Year 10, reflecting a tendency for girls’ motivation, self-efficacy and peer support towards physical activity to decline with age. There was no evidence that the PLAN-A intervention was sufficient to stem this trajectory, although we did not include shorter-term interim measures (e.g. an immediately post-intervention period) so are not able to determine short-term effects. It could be that intervening in Years 9 and 10 is too late into adolescence to meaningfully compete with the multitude of other factors (i.e. biological, social, educational and emotional) that are changing simultaneously and potentially contribute to a decline in girls’ physical activity113 and perceptions, such as physical activity motivation, competence, enjoyment, peer value and acceptance.
In terms of the theoretical model underpinning the intervention’s content (i.e. SDT), the process evaluation confirmed that the peer supporter trainers used an autonomy-supportive style. There was qualitative evidence to suggest that in their role as peer supporters the girls developed confidence/competence; autonomy-supportive techniques, such as empathy, communication and cooperation; and new social bonds. This agrees with the findings of the feasibility trial and previous studies showing that intervention agents (both adults and young people) can be trained to use a motivational style that promotes need satisfaction. 51,78,114,115 However, there was limited evidence from peer supporters and non-peer supporters as to whether or not and how peer supporters used positive motivational techniques to influence their peers’ physical activity.
Intercorrelations between psychosocial factors at both time points were as hypothesised in SDT (e.g. the simple pattern of the behavioural regulation subscales and associations between behavioural regulations and autonomy, competence and relatedness need satisfaction, and other psychosocial variables; see Appendix 14). For example, autonomous motivation showed a moderate positive association with physical activity self-efficacy, whereas the equivalent correlation with controlled motivation was near zero. However, like the feasibility trial,52 we found no evidence that the intervention affected the psychosocial variables as hypothesised, and there was no evidence of meaningful associations between the psychosocial variables and MVPA. Furthermore, there was no evidence that the psychosocial variables functioned as mediators. These findings were broadly consistent when run as regression models, which adjusted for the same variables as specified in the primary analysis (see Appendix 15). However, a model that included the five subtypes of motivation showed a small positive association between intrinsic motivation and MVPA.
The data presented in this trial agree with a meta-analysis of 46 studies that reported that children’s and adolescents’ intrinsic motivation for leisure-time (i.e. non-PE) physical activity was positively associated with their leisure-time physical activity. 116 This evidence synthesis also reported a null association between identified motivation and physical activity in studies that used objective measures of physical activity. These findings add to the evidence base for the positive role played by adolescent girls’ motivation based on enjoyment and inherent value for physical activity.
The SDT framework has been used extensively to study associations between motivation and physical activity in children and adolescents,116 and numerous school-based physical activity interventions have used SDT as a theoretical foundation. 114,117–120 Furthermore, the principles of SDT are integrated into frameworks for the design and delivery of organised physical activity sessions for children and adolescents. 121 However, the effectiveness of SDT-based interventions on motivational mediators and/or physical activity is mixed.
Like PLAN-A, the ‘Girls Active’112 and ‘Girls on the Move’118 interventions also showed no effect on girls’ motivation and other psychological mediators, such as enjoyment or self-efficacy towards physical activity. In contrast, Lonsdale et al. 120 and Ha et al. 115,117 have reported positive effects of SDT-based interventions situated within PE lessons on secondary school-aged children’s MVPA time in PE. However, neither intervention found effects on participants’ broader leisure time MVPA. Although Ha et al. 115,117 found a positive effect of the PE-based intervention on girls’ (but not boys’) autonomous motivation, Lonsdale et al. 120 found no effect on the hypothesised motivational mediators.
A reason for the differences in the findings of these studies might be the setting in which they were implemented. Despite sharing similar theoretical foundations, PE lesson interventions could be considered more discrete and structured in nature than PLAN-A, Girls Active112 and, to a lesser extent, Girls on the Move,118 which were implemented in more informal and global settings (e.g. changing school or peer culture and expecting girls to develop their own ways to increase their physical activity). It may be easier to explicitly implement SDT principles and measure the effects on motivation and physical activity in discrete contexts (e.g. a PE lesson) than in interventions, such as PLAN-A, that operate and measure constructs at broader levels. For example, Lonsdale et al. 120 suggest that their Activity and Motivation in Physical Education (AMPED) intervention would be ‘best implemented as an enhancement component of a comprehensive school PA [physical activity] programme that also includes other “expansion” and “extension” initiatives’.
The efficacy of health improvement interventions based on SDT has been shown in a recent evidence synthesis, with evidence mainly derived from studies promoting physical activity, including school-based trials. 122 Furthermore, basing physical activity interventions for young people on theories such as SDT seems intuitive (i.e. it seems logical and morally appropriate to promote motivation based on enjoyment and positive values, rather than guilt and external demands), is recommended121 and aligns with evidence for a positive association between intrinsic and identified motivation and physical activity. 116 However, the literature demonstrates that it is challenging to quantify intervention effects on theoretical/psychosocial mediators within school-based physical activity interventions. We have carefully mapped SDT to several interventions,51,78,123 which we have tested in robust trial designs, and used a combination of qualitative and quantitative measures (often from multiple stakeholders) to try to quantify theoretical mechanisms of action. A consistent finding was qualitative results that generally support theoretical fidelity and efficacy, but also quantitative findings that fail to show intervention effects on outcomes or mechanisms of action. Although we endeavour to collect and analyse qualitative process evaluation data with appropriate rigour, confirmation bias is a possibility. Equally, the measures used to quantify psychosocial mechanisms of action may not be sufficiently sensitive to detect change. It is also possible that the intervention simply did not affect the mechanisms of action as proposed.
Implications for policy and practice
Intervention delivery versus intervention model
Neither our measurable indicators of intervention implementation success (i.e. pupil engagement and enjoyment, fidelity to intervention design and theories) nor our measures of school environment (i.e. physical activity facility provision and policy audit) converged with or could explain a lack of intervention effectiveness (as determined by improvement in weekday MVPA) at the school level. This raises the question ‘If the intervention was delivered as planned, with good fidelity to underpinning theory, did insufficient peer supporting take place to bring about positive improvements in physical activity, or is it realistic to expect a(ny) single intervention to bring about meaningful change?’.
Existing literature in this area suggests that other peer-led interventions delivered at scale had no lasting effect on MVPA levels in adolescent girls112,124 or in a mixed-gender school setting. 125 Harrington et al. 112 found evidence of a small (i.e. 2–3 additional minutes of MVPA per day), short-term (i.e. 7-month) effect of the ‘Girls Active’ intervention among adolescent girls in English schools, but this was not maintained at the 14-month follow-up. In a randomised controlled trial of an intervention that trained older adolescents (i.e. mentors) and in-class peer leaders to encourage classes to undertake two new weekly activities, Corder et al. 125 reported no difference in MVPA between the control and intervention groups at follow-up. Moreover, although a peer-led walking intervention in schools124 resulted in an increase in daily light-intensity physical activity of 8.27 minutes among adolescent girls, it had no significant effect on MVPA.
Many elements of Harrington et al. ’s112 Girls Active intervention focused on changing school culture around physical activity, but not adding new opportunities to be active, which was hypothesised to be insufficient to increase MVPA. PLAN-A relies on a similar model, changing peer culture and expecting girls to find their own ways to increase their physical activity. Indeed, in a recent feasibility trial exploring peer-mentoring in conjunction with new physical activity opportunities, Owen et al. 126 reported that, when using peer mentoring alone, physical activity declined, whereas, when used in combination with an after-school club, the same peer mentoring intervention increased physical activity by 3.2 minutes per day (p = 0.007); however, this was not a fully powered trial. Collectively, these studies highlight a need to explore alternative intervention approaches.
Peer-led delivery models and associated measure sensitivity
The process evaluation in this trial and in our earlier feasibility trial52 demonstrate that peer-led interventions such as PLAN-A can be delivered with good fidelity to intervention design and theory. However, challenges identified around behaviour management with larger groups and the intervention setting resulted in a ‘drift’ from important design elements, such as the identification of influential peer leaders. There are questions regarding the suitability of the individuals selected to be peer supporters and how well represented social groups are within the cohort,127 which reflect limitations of the peer-nomination process itself. Recent research has tested a social network analysis (SNA) approach to peer nomination using a closeness centrality selection criterion. 128 This selection criterion is predicated on establishing how closely each pupil is connected to all of their peers via a SNA and then selecting those needing the fewest intermediaries to reach everyone in the network. 129 This approach differs from the approach used in this trial and ASSIST,37 in which the overall number of nominations a person received was the criterion for selection, and presents a more data-driven approach to peer nomination that has been shown to be successful at selecting more effective agents for change, who are capable of influencing physical activity in their peers,130 namely those with higher ‘sociometric popularity’ rather than ‘prestige popularity’. 131 Nevertheless, establishing the efficacy of a peer nomination process for selecting pupils with the greatest influence over their peers is only part of the peer-led approach. Once identified, these agents for change must also diffuse new behavioural norms.
In this trial, we experienced difficulties in determining the extent to which trained peer supporters engaged in supportive conversations and other peer support strategies (see Chapter 5, Evidence of peer support: fidelity to diffusion of innovations theory). Participants in this trial and the previous feasibility work52 demonstrated that diaries are not an effective way to capture this information, and qualitative evidence suggests that the subtle nature of much of peer supporting makes it hard to recall, harder still to quantify and, potentially, very difficult for recipients to notice. In a roll-out of the ASSIST programme, it was also a challenge to measure the peer-supporting conversations that took place. 132 In contrast to ASSIST, the outcome of interest in PLAN-A (i.e. weekday MVPA minutes) was a much more complex behaviour to measure (comprising type, volume, intensity and context) than a discrete behaviour, such as smoking and, therefore, it was not possible to use a binary variable. Furthermore, the focus of ASSIST for most children was not smoking (for most this meant not starting to smoke), whereas for PLAN-A it was being more active; the latter is, arguably, comparatively amorphous and, perhaps, not as strongly socially linked to peer influence and social status among adolescents. Measurement considerations are twofold: measurement of the exposure (i.e. peer supporting) and of the outcome (i.e. MVPA).
Regarding the exposure, ecological momentary assessment (EMA) has been used in various settings and fields to capture real-time data through repeated measures of behaviour or behavioural contexts. Using EMA dramatically reduces the period of recall, meaning biases associated with retrospective recall are reduced and the need for participants to summarise events or experiences over extended periods of time is removed. 133 Thus, EMA could, theoretically, be used to improve measurement of peer-supporting actions, or at least to reduce the recall bias experienced in this and other peer-based trials.
However, as highlighted in a recent review of EMA studies on physical activity and sedentary behaviour,134 the methodology is vulnerable to several risks of bias that would present challenges to its use in capturing peer-supporting activity. The primary risk is the sampling approach, time-based versus event-based sampling, as either approach would be imperfect. If a time-based sampling approach was used, then peer supporters would be asked to recall peer-supporting activity and context at scheduled intervals during the day, which may lose the benefit of momentary assessment and be subject to recall bias. On the other hand, an event-based approach – which is usually self-initiated – would rely on participants logging details of peer-supporting activities at the time, which, based on feedback from peer supporters in this trial about the use of their diaries, is something that adolescents would not engage with reliably.
Furthermore, despite advances in technology that mean that EMA can be performed using participants’ smartphones, the method is burdensome for participants and is likely to blur the lines between measurement and providing an additional intervention, which would need to be replicated if the intervention were scaled up. Although many studies using EMA report high compliance,134–136 the measurement periods are usually short (between 1 day and 2 weeks) and the feasibility of using EMA continuously for extended periods of time (e.g. a 10-week diffusion period, as used in PLAN-A and ASSIST37) has not been tested.
Considering the outcome measure’s sensitivity, the use of objective means of measurement (i.e. accelerometers) has been widely accepted as a more robust way of capturing physical activity than self-report, which is prone to overestimation of higher-intensity physical activity and underestimation of sedentary time. 137,138 However, there are known limitations of using accelerometers, including an inability to identify time spent in different activities139 and the risk that the brief measurement period (7 days is typical) may be too short to reliably observe changes in ‘normal’ behaviour patterns, or it may be subject to confounding by external factors. In this trial, we hypothesised that participants in two schools exhibited lower-than-predicted physical activity because of adverse weather, reinforcing this concern. In addition, using hip placement of the accelerometer, as was used in this trial, and asking that the devices be removed when in water or when playing contact sports risked underestimating or missing certain types of physical activity, such as cycling,140 swimming and contact sports, that can account for significant amounts of MVPA. It is possible that the challenges associated with measurement of the exposure (i.e. peer supporting) or nuanced and imperfect measurement of the outcome (i.e. change in MVPA) relative to the exposure reduced our ability to accurately quantify the efficacy of a peer-led approach to changing physical activity.
Likewise, if such interventions can be delivered at scale, but are limited in their effectiveness at changing physical activity, then we may naturally question whether the reasons for that lie in the intervention model itself (using peer support to diffuse new norms) or in social factors that are hard to measure (e.g. pre-existing local cultural norms) that undermine the assumptions inherent in a peer-based DOI approach. One such social factor pertinent to adolescents today is the use of social media to interact and influence. 141 There is uncertainty about whether or not peer-led interventions in schools can fully capitalise on how adolescents interact and influence each other using social media because of challenges in measuring engagement and impact. 142 Thus, there are major challenges to designing an intervention that includes substantial smartphone and social media components (whether delivering messages, support, ideas to peer supporters and encouraging peer supporters to influence their peers through their usual social media channels, or in the assessment of peer-supporting activity) and is delivered during school time. It would be worth exploring how social media and mobile technology could be incorporated into peer-based interventions and their acceptability to schools, pupils and parents.
Issues with scaling up interventions
The data presented in this report are consistent with recent evidence on the challenges of scaling up physical activity interventions from feasibility studies to definitive trials. In a recent meta-analysis, Beets et al. 143 identified nine forms of bias in this area, of which two were relevant to this trial. We found that there were changes in intervention support between the feasibility trial52 and this trial as the group sizes were larger than those in the feasibility trial and, therefore, trainer–pupil contact was more diluted, and there was a target audience bias as we had to change the year group from Year 8 to Year 9. The data reported here reinforce the need to focus on external validity and the potential implementation of intervention results from the design stage. 144
Alternative approaches to interventions targeting individual-level change and the need to explore whole-school approaches
The ultimate target of public health interventions is behaviour change at a population level, which is logically driven by behaviour change among the individual members of a population. However, as advocated in recent papers,145,146 individual-level interventions are not sufficient to bring about individual- or population-level change because the determinants of our behaviour are diverse, complex and often beyond individual control (e.g. policy, physical environment, SEP). PLAN-A attempted to advance beyond a simple individual-level education-based intervention; instead, it was designed to harness the power of naturally existing peer groups and used informal (e.g. peer diffusion) rather than formal (e.g. educational lessons, additional structured physical activity time in school) methods to promote the uptake of physical activity. However, despite this, the intervention model is relatively constrained and one-dimensional: it does not embrace a broader system or ‘whole-school’ approach,146 which would intervene at multiple levels including, but not limited to, peer influence. Indeed, from a systems perspective, it seems somewhat unrealistic to expect a short-term intervention focused on a single determinant of physical activity (i.e. peers) to have a meaningful impact on physical activity behaviour. It is important to note that this was a relatively high-agency intervention, and it may be the case that an intervention that required lower agency would have been more successful. Low-agency interventions are consistent with the concept of whole-school interventions147 and, thus, in the future we suggest that lower-agency interventions are considered.
An important question that arises from this project is ‘What next?’. Whole-school approaches to physical activity have been advocated for some time,148 and the recently developed Creating Active Schools framework advances this work using insight from researchers, teachers and sport practitioners. 146 However, like PLAN-A, school-based interventions often focus on a single or a few components of the whole-school approach only. This is probably driven by a methodological need to:
-
define what the intervention is and design it well
-
estimate the effect of particular intervention strategies to inform future investment (e.g. active travel, enhanced PE or after-school activity clubs)
-
design interventions that could be attractive to schools (i.e. interventions that are clear, discrete, simple and not resource intensive)
-
design interventions that can be rolled out at scale.
However, these elements create a conflict between intervention depth and breadth. Many facets of good intervention design (e.g. detailed planning, iterative co-development, piloting, pre-testing, the use of logic models, theory, attention to behaviour change techniques) take considerable time and resources to perform well and often necessitate a narrowing of the intervention scope. This was the approach used in PLAN-A, and it arguably resulted in good intervention ‘depth’. However, a systems or whole-school approach requires greater ‘breadth’, with interventions operating across multiple domains simultaneously (e.g. active travel, school culture and ethos, high-quality PE, active lessons, active breaks, active extracurricular clubs). Nevertheless, it is not yet clear how multidimensional whole-school approaches can be designed in a way that balances and optimises depth and breadth.
The balance between breadth and depth is also an issue that affects intervention evaluation. It is, relatively speaking, straightforward to evaluate a well-defined, one-dimensional, school-based physical activity intervention such as those conducted in recent years by our group and others. 51,78,123,125 The intervention can be clearly described, fidelity can be assessed, and its effect compared using a control group within a traditional cluster-randomised controlled trial design; again, we can achieve good depth, but limited breadth. It is not clear how best to evaluate broader whole-school approaches, which act on multiple domains of physical activity, nor how to determine which elements are and are not effective, or how interventions may interact with pupil-level factors (e.g. age, gender, SEP), cohort effects and school-level factors (e.g. deprivation, facilities, size or location). Even if researchers can determine that a whole-school approach is effective, it may be unrealistic to expect the approach to be generalisable. Schools are like ecosystems in that no two are the same: they are in a state of constant flux; serve diverse communities with different needs; and have shifting priorities, variable budgets and resources, and changeable internal and external contexts. Effective interventions are likely to be those that can be designed and modified to accommodate these factors; therefore, an intervention that works in one school may not suit, work or be needed in another.
One approach is to focus further on depth by designing specific and discrete interventions (e.g. increasing the amount of MVPA time in PE) and very closely measuring the outcomes that are matched to the behaviour (e.g. MVPA time in PE), repeating this across multiple domains (e.g. active travel, classes, miles and clubs) and being content with the assumed additive effect of the small effects on MVPA across multiple domains, summing to a meaningful or health-enhancing level of physical activity. If multiple interventions are needed as part of a whole-school approach, testing discrete interventions would also lack external validity and would not provide insight as to whether or not schools are able to implement multiple interventions simultaneously. If we focus more on breadth, we risk developing weaker or more diluted interventions and it may be very challenging to identify which intervention actions are effective. It may be harder to convince schools and/or commissioners to adopt more resource-intensive approaches. This is a challenge that needs to be addressed in the next generation of system-focused public health interventions.
Specific research recommendations
Based on the data presented in this report and the issues covered throughout this chapter, there are several specific research issues that we recommend as the focus of future research. There is a need for a better understanding of how changes in physical activity track over time, how change can be achieved more effectively, and how change can be measured more accurately and reliably. The research needs are:
-
the need for better evidence on the sustainability of improvements in physical activity in adolescence into adulthood
-
the need to evaluate the utility of whole-school approaches to promote physical activity in schools and explore implementation options that would make such an approach feasible in a range of settings
-
the need to develop and test EMA methods for capturing peer supporting and assessing the potential impacts of peer-led interventions on behavioural outcomes
-
the need for new or revised psychosocial scales that can better capture change in physical activity motivation.
Furthermore, future research would benefit from investigating the pattern of accumulation and the potential compensatory effect or composition of daily physical activity to ascertain whether interventions simply have no effect or whether they change the manner in which physical activity is accumulated and, therefore, have an effect on associated health factors.
Strengths and limitations
The main strengths of this trial were functions of the robust cluster-randomised design. Cluster-randomised controlled trials enable the testing of an intervention’s real-world efficacy and rely on large sample sizes. Schools were the unit of allocation and the intervention was delivered to an entire year group at each school, rather than to a subgroup of pupils. Our trial successfully recruited 20 schools from across South West England; the schools varied in size and demographics, providing ample statistical power to address our research questions. Physical activity was measured using accelerometers, and a comprehensive mixed-methods process evaluation was conducted alongside the trial to gather views from each key stakeholder group that was involved in the delivery and receipt of the intervention.
The intervention delivered in this trial was a refined version of an intervention (which was itself based on a successful smoking cessation intervention) that was co-developed with adolescent girls in a robustly conducted feasibility trial,51 and has been reported in line with the TIDieR framework. 60 Refinements included an improvement to the peer-nomination process to build in the flexibility to accommodate different year group structures, and changes to the underlying programme theory by incorporating SDT. We have also ensured that our reporting of the main trial adheres to the CONSORT extension for cluster-randomised trials guidelines149 and the reporting of the qualitative process evaluation data follows the COREQ59 checklist.
Although schools were sampled to reflect a range of SEPs, this trial was limited by a geographical focus that included schools in south-west England only. In addition, although schools were assessed for their suitability for physical activity using environment audits and changes in school policies were captured at a superficial level, greater detail on school-level environment changes between time points and trial arms would have enabled greater exploration of the potential impact of school environment (including changes in school policies) on the stated trial outcomes. Several schools in the control group changed their approach to physical activity provision in the curriculum, which may have yielded changes in the year group’s physical activity for which we were unable to account. This could have been better controlled for if we had asked schools to defer any such changes for the time that they were in the trial, but this would have raised concerns over the external validity of the trial results.
This trial presented qualitative and qualitative data largely separately; however, this was a decision taken to retain the independence of the researchers analysing each type of data and to ease readability. The process evaluation was restricted to topics that were not already covered in detail in the feasibility trial;52 however, the findings were based on both the feasibility trial and this trial. Despite this, the current trial was unable to quantify the impact of delivering the intervention in an older year group than that in the feasibility trial. Additional work to understand changes in social and behavioural norms between Year 8 and Year 9 would have improved our ability to describe, if not quantify, this factor.
Furthermore, capturing fidelity to the principles of DOI, namely peer-supporting activity, was unreliable and had questionable validity because of the juxtaposition of the behaviour in question (i.e. subtle, ambiguous and intuitive) and the measures available to capture it (i.e. quantitative and definitive). We have suggested alternative approaches that warrant further exploration.
We also note that there are many options available for collecting and processing accelerometer data. It may have been the case that greater compliance would have been obtained if we had opted for a wrist-worn device. However, we opted for the waist-worn ActiGraph GT3X+ as this device has been widely used and, therefore, its use facilitates comparison with other data sets.
Finally, the economic analysis did not measure health service use and only indirectly estimated the CHU-9D scores from the KIDSCREEN-10 responses; however, given the lack of effect on MVPA, these limitations are unlikely to have altered the interpretation of the economic results.
Conclusions
This report found no evidence that the PLAN-A intervention led to increased MVPA among adolescent girls and, consequently, the intervention was not cost-effective. The process data showed that this was despite the intervention having high acceptance and being delivered with high fidelity. Challenges included the accurate measurement of peer-supporting behaviour and connecting that exposure to changes in physical activity in the face of myriad confounding factors.
Possible explanations for the lack of a positive effect of the intervention include a change in year group from the feasibility trial and the diluted intervention dose; however, it is difficult to accurately estimate the impact of these factors on the complex intersection between environment, motivation and behaviour. Therefore, the findings provide strong evidence that the PLAN-A intervention is neither an effective nor cost-effective means of increasing physical activity among adolescent girls; thus, it should not be implemented or disseminated. It has been argued that single individual-level interventions implemented in schools are insufficient to bring about increases in physical activity for the masses and further system-wide approaches may be needed. This report recommends further research exploring the implementation considerations and utility of using a whole-school approach to promote physical activity in young people.
Acknowledgements
This trial was designed and delivered in collaboration with BRTC, a United Kingdom Clinical Research Collaboration (UKCRC)-registered Clinical Trials Unit, which, as part of the Bristol Trials Centre, is in receipt of NIHR Clinical Trials Unit support funding. The sponsor of this trial is the University of Bristol, Research and Enterprise Development, One Cathedral Square, Bristol, BS1 5DD, UK (www.bristol.ac.uk/red/). The costs of delivering the intervention were funded by Sport England. Trial data were collected and managed using REDCap, hosted at the University of Bristol.
We would like to thank the members of the LAG: Nick Bolton, Healthy Schools and Personal, Social, Health and Economic Education (PSHE) support, Wiltshire Council (Trowbridge, UK); Sarah Godsell, Partnership Officer, South Gloucestershire Council; Heather Smith, Associate Head of Innovation, Women in Sport; John Lux, teacher, St Brendan’s Sixth Form College (Bristol, UK); Jo Williams, Bristol City Council (Bristol, UK); Jo Moss, Strategic Lead Children and Young People, Sport England; and Darcy Hare, Sport England.
We would like to extend our gratitude to the members of the TSC: Professor Emma McIntosh, University of Glasgow (Glasgow, UK); Dr Trish Gorely, University of the Highlands and Islands (Perth, UK); Dr Philip Pallman, Cardiff University (Cardiff, UK); and Ms Sara Blackmore, South Gloucestershire Council.
A special thank you to the PLAN-A trainers, school staff, child participants and parents for their involvement in the trial.
Contributions of authors
Russell Jago (https://orcid.org/0000-0002-3394-0176) (Professor of Physical Activity and Public Health) was the Principal Investigator for the trial, co-wrote the first version of the manuscript and, along with Simon Sebire, obtained the funds for the trial.
Byron Tibbitts (https://orcid.org/0000-0001-5818-7080) (Trial Manager) co-wrote the first version of the manuscript, managed the data collection process team, analysed the qualitative process evaluation data and co-drafted Chapter 5 with Kathryn Willis.
Kathryn Willis (https://orcid.org/0000-0002-8998-6691) (Research Associate) co-wrote the first version of the manuscript, analysed the qualitative process evaluation data, developed the process evaluation and was responsible for collecting process evaluation data, and co-drafted Chapter 5 with Byron Tibbitts.
Emily Sanderson (https://orcid.org/0000-0003-2268-4194) (Research Associate in Medical Statistics) was responsible for co-leading the statistical analysis and acted as a main link to BRTC, a UKCRC-registered Clinical Trials Unit. She also drafted Chapter 3.
Rebecca Kandiyali (https://orcid.org/0000-0001-8566-9536) (Research Fellow in Health Economics) co-designed and conducted the economic analysis for the trial and co-drafted Chapter 4.
Tom Reid (https://orcid.org/0000-0002-0254-4912) (Fieldworker) co-wrote the first version of the manuscript, cleaned and managed the survey and accelerometer data, and analysed the qualitative process evaluation data.
Stephanie MacNeill (https://orcid.org/0000-0001-6553-1433) (Lecturer in Medical Statistics) was a co-applicant. The co-applicant team co-led the development of the trial methods and design. She was responsible for co-leading the statistical analysis and acted as a main link to BRTC, a UKCRC-registered Clinical Trials Unit. She also drafted Chapter 2.
Ruth Kipping (https://orcid.org/0000-0002-5446-8077) (Associate Professor in Public Health) was a co-applicant. The co-applicant team co-led the development of the trial methods and design.
Rona Campbell (https://orcid.org/0000-0002-1099-9319) (Professor of Public Health Research) was a co-applicant. The co-applicant team co-led the development of the trial methods and design.
Simon J Sebire (https://orcid.org/0000-0001-7994-0844) (Senior Lecturer in Physical Activity and Public Health) was the Principal Investigator of the feasibility trial and, along with Russell Jago, obtained the funds for the trial.
William Hollingworth (https://orcid.org/0000-0002-0840-6254) (Professor of Health Economics) was a co-applicant. The co-applicant team co-led the development of the trial methods and design. He also co-designed and conducted the economic analysis for the trial and co-drafted Chapter 4.
All authors reviewed various sections of the monograph and made critical revisions to relevant sections. All authors approved the final submission.
Publication
Jago R, Tibbitts B, Willis K, Sanderson E, Kandiyali R, Reid T, et al. Effectiveness and cost-effectiveness of the PLAN-A intervention, a peer led physical activity program for adolescent girls: results of a cluster randomised controlled trial. Int J Behav Nutr Phys Act 2021;18:63.
Data-sharing statement
All data requests should be submitted to the corresponding author for consideration. Access to available anonymised data may be granted following review.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health and Social Care.
References
- Willis K, Tibbitts B, Sebire SJ, Reid T, MacNeill SJ, Sanderson E, et al. Protocol for a cluster randomised controlled trial of a Peer-Led physical Activity iNtervention for Adolescent girls (PLAN-A). BMC Public Health 2019;19. https://doi.org/10.1186/s12889-019-7012-x.
- Jago R, Tibbitts B, Willis K, Sanderson E, Kandiyali R, Reid T, et al. Effectiveness and cost-effectiveness of the PLAN-A intervention, a peer led physical activity program for adolescent girls: results of a cluster randomised controlled trial. Int J Behav Nutr Phys Act 2021;18. https://doi.org/10.1186/s12966-021-01133-8.
- Janssen I, Leblanc AG. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int J Behav Nutr Phys Act 2010;7. https://doi.org/10.1186/1479-5868-7-40.
- Biddle SJ, Asare M. Physical activity and mental health in children and adolescents: a review of reviews. Br J Sports Med 2011;45:886-95. https://doi.org/10.1136/bjsports-2011-090185.
- Trudeau F, Shephard RJ. Physical education, school physical activity, school sports and academic performance. Int J Behav Nutr Phys Act 2008;5. https://doi.org/10.1186/1479-5868-5-10.
- Baggett CD, Stevens J, McMurray RG, Evenson KR, Murray DM, Catellier DJ, et al. Tracking of physical activity and inactivity in middle school girls. Med Sci Sports Exerc 2008;40:1916-22. https://doi.org/10.1249/MSS.0b013e318180c390.
- Kelder SH, Perry CL, Klepp KI, Lytle LL. Longitudinal tracking of adolescent smoking, physical activity, and food choice behaviors. Am J Public Health 1994;84:1121-6. https://doi.org/10.2105/AJPH.84.7.1121.
- Twisk JWR, Kemper HCG, Mechelen WV. Tracking of activity and fitness and the relationship with cardiovascular disease risk factors. Med Sci Sports Exerc 2000;32:1455-61. https://doi.org/10.1097/00005768-200008000-00014.
- Department of Health and Social Care . Physical Activity Guidelines: UK Chief Medical Officers’ Report 2019.
- Steene-Johannessen J, Hansen BH, Dalene KE, Kolle E, Northstone K, Møller NC, et al. Variations in accelerometry measured physical activity and sedentary time across Europe – harmonized analyses of 47,497 children and adolescents. Int J Behav Nutr Phys Act 2020;17. https://doi.org/10.1186/s12966-020-00930-x.
- Department of Health and Social Care, Prime Minister’s Office: 10 Downing Street, Her Majesty’s Treasury and Cabinet Office . Childhood Obesity: A Plan for Action 2016.
- Borde R, Smith JJ, Sutherland R, Nathan N, Lubans DR. Methodological considerations and impact of school-based interventions on objectively measured physical activity in adolescents: a systematic review and meta-analysis. Obes Rev 2017;18:476-90. https://doi.org/10.1111/obr.12517.
- Biddle SJ, Braithwaite R, Pearson N. The effectiveness of interventions to increase physical activity among young girls: a meta-analysis. Prev Med 2014;62:119-31. https://doi.org/10.1016/j.ypmed.2014.02.009.
- Owen MB, Curry WB, Kerner C, Newson L, Fairclough SJ. The effectiveness of school-based physical activity interventions for adolescent girls: a systematic review and meta-analysis. Prev Med 2017;105:237-49. https://doi.org/10.1016/j.ypmed.2017.09.018.
- Voskuil VR, Frambes DA, Robbins LB. Effect of physical activity interventions for girls on objectively measured outcomes: a systematic review of randomized controlled trials. J Pediatr Health Care 2017;31:75-87. https://doi.org/10.1016/j.pedhc.2016.03.003.
- Biddle SJH, Whitehead SH, O’Donovan T, Nevill ME. Correlates of participation in physical activity for adolescent girls: a systematic review of recent literature. J Phys Act Health 2005;2:423-34. https://doi.org/10.1123/jpah.2.4.423.
- Stalsberg R, Pedersen AV. Effects of socioeconomic status on the physical activity in adolescents: a systematic review of the evidence. Scand J Med Sci Sports 2010;20:368-83. https://doi.org/10.1111/j.1600-0838.2009.01047.x.
- Hankonen N, Heino MT, Kujala E, Hynynen ST, Absetz P, Araújo-Soares V, et al. What explains the socioeconomic status gap in activity? Educational differences in determinants of physical activity and screentime. BMC Public Health 2017;17. https://doi.org/10.1186/s12889-016-3880-5.
- Spencer RA, Rehman L, Kirk SF. Understanding gender norms, nutrition, and physical activity in adolescent girls: a scoping review. Int J Behav Nutr Phys Act 2015;12. https://doi.org/10.1186/s12966-015-0166-8.
- Slater A, Tiggemann M. ‘Uncool to do sport’: a focus group study of adolescent girls’ reasons for withdrawing from physical activity. Psychol Sport Exerc 2010;11:619-26. https://doi.org/10.1016/j.psychsport.2010.07.006.
- Knowles AM, Niven A, Fawkner S. ‘Once upon a time I used to be active’. Adopting a narrative approach to understanding physical activity behaviour in adolescent girls. Qual Res Sport Exerc 2013;6:62-76. https://doi.org/10.1080/2159676X.2013.766816.
- Gillison F, Sebire S, Standage M. What motivates girls to take up exercise during adolescence? Learning from those who succeed. Br J Health Psychol 2012;17:536-50. https://doi.org/10.1111/j.2044-8287.2011.02053.x.
- Corr M, McSharry J, Murtagh E. Adolescent girl’s perceptions of physical activity: a systematic review of qualitative studies. J Phys Act Health 2018;15.
- Fitzgerald A, Fitzgerald N, Aherne C. Do peers matter? A review of peer and/or friends’ influence on physical activity among American adolescents. J Adolesc 2012;35:941-58. https://doi.org/10.1016/j.adolescence.2012.01.002.
- Smith AL. A case for peer-focused efforts to understand and promote physical activity in young people. Kinesiol Rev 2019;8:32-9. https://doi.org/10.1123/kr.2018-0058.
- Laird Y, Fawkner S, Niven A. A grounded theory of how social support influences physical activity in adolescent girls. Int J Qual Stud Health Well-Being 2018;13. https://doi.org/10.1080/17482631.2018.1435099.
- Macdonald-Wallis K, Jago R, Sterne JA. Social network analysis of childhood and youth physical activity: a systematic review. Am J Prev Med 2012;43:636-42. https://doi.org/10.1016/j.amepre.2012.08.021.
- Salway RE, Sebire SJ, Solomon-Moore E, Thompson JL, Jago R. Associations within school-based same-sex friendship networks of children’s physical activity and sedentary behaviours: a cross-sectional social network analysis. Int J Behav Nutr Phys Act 2018;15. https://doi.org/10.1186/s12966-018-0653-9.
- MacArthur GJ, Harrison S, Caldwell DM, Hickman M, Campbell R. Peer-led interventions to prevent tobacco, alcohol and/or drug use among young people aged 11–21 years: a systematic review and meta-analysis. Addiction 2016;111:391-407. https://doi.org/10.1111/add.13224.
- Yip C, Gates M, Gates A, Hanning RM. Peer-led nutrition education programs for school-aged youth: a systematic review of the literature. Health Educ Res 2016;31:82-97. https://doi.org/10.1093/her/cyv063.
- Mellanby AR, Rees JB, Tripp JH. Peer-led and adult-led school health education: a critical review of available comparative research. Health Educ Res 2000;15:533-45. https://doi.org/10.1093/her/15.5.533.
- Tolli MV. Effectiveness of peer education interventions for HIV prevention, adolescent pregnancy prevention and sexual health promotion for young people: a systematic review of European studies. Health Educ Res 2012;27:904-13. https://doi.org/10.1093/her/cys055.
- Martin Ginis KA, Nigg CR, Smith AL. Peer-delivered physical activity interventions: an overlooked opportunity for physical activity promotion. Transl Behav Med 2013;3:434-43. https://doi.org/10.1007/s13142-013-0215-2.
- Christensen JH, Elsborg P, Melby PS, Nielsen G, Bentsen P. A scoping review of peer-led physical activity interventions involving young people: theoretical approaches, intervention rationales, and effects. Youth Soc 2020;53:811-40. https://doi.org/10.1177/0044118X20901735.
- Harden A, Oakley A, Oliver S. Peer-delivered health promotion for young people: a systematic review of different study designs. Health Educ J 2001;60:339-53. https://doi.org/10.1177/001789690106000406.
- Rogers EM. Diffusion of Innovations. New York, NY: Free Press; 1983.
- Campbell R, Starkey F, Holliday J, Audrey S, Bloor M, Parry-Langdon N, et al. An informal school-based peer-led intervention for smoking prevention in adolescence (ASSIST): a cluster randomised trial. Lancet 2008;371:1595-602. https://doi.org/10.1016/S0140-6736(08)60692-3.
- Prestwich A, Sniehotta FF, Whittington C, Dombrowski SU, Rogers L, Michie S. Does theory influence the effectiveness of health behavior interventions? Meta-analysis. Health Psychol 2014;33:465-74. https://doi.org/10.1037/a0032853.
- Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol 2000;55:68-7. https://doi.org/10.1037/0003-066x.55.1.68.
- Deci EL, Ryan RM. The ‘what’ and ‘why’ of goal pursuits: human needs and the self-determination of behavior. Psychol Inq 2000;11:227-68. https://doi.org/10.1207/S15327965PLI1104_01.
- Teixeira PJ, Carraça EV, Markland D, Silva MN, Ryan RM. Exercise, physical activity, and self-determination theory: a systematic review. Int J Behav Nutr Phys Act 2012;9. https://doi.org/10.1186/1479-5868-9-78.
- Sebire SJ, Jago R, Fox KR, Edwards MJ, Thompson JL. Testing a self-determination theory model of children’s physical activity motivation: a cross-sectional study. Int J Behav Nutr Phys Act 2013;10. https://doi.org/10.1186/1479-5868-10-111.
- Fortier MS, Duda JL, Guerin E, Teixeira PJ. Promoting physical activity: development and testing of self-determination theory-based interventions. Int J Behav Nutr Phys Act 2012;9. https://doi.org/10.1186/1479-5868-9-20.
- Sebire SJ, Edwards MJ, Fox KR, Davies B, Banfield K, Wood L, et al. Delivery and receipt of a self-determination theory-based extra-curricular physical activity intervention: exploring theoretical fidelity in action 3:30. J Sport Exerc Psychol 2016;38:381-95. https://doi.org/10.1123/jsep.2015-0217.
- Gillison FB, Rouse P, Standage M, Sebire SJ, Ryan RM. A meta-analysis of techniques to promote motivation for health behaviour change from a self-determination theory perspective. Health Psychol Rev 2019;13:110-30. https://doi.org/10.1080/17437199.2018.1534071.
- Standage M, Duda JL, Ntoumanis N. A test of self-determination theory in school physical education. Br J Educ Psychol 2005;75:411-33. https://doi.org/10.1348/000709904X22359.
- Sebire SJ, Standage M, Vansteenkiste M. Predicting objectively assessed physical activity from the content and regulation of exercise goals: evidence for a mediational model. J Sport Exerc Psychol 2011;33:175-97. https://doi.org/10.1123/jsep.33.2.175.
- Emm-Collison LG, Jago R, Salway R, Thompson JL, Sebire SJ. Longitudinal associations between parents’ motivations to exercise and their moderate-to-vigorous physical activity. Psychol Sport Exerc 2019;43:343-9. https://doi.org/10.1016/j.psychsport.2019.04.007.
- Emm-Collison LG, Sebire SJ, Salway R, Thompson JL, Jago R. Multidimensional motivation for exercise: a latent profile and transition analysis. Psychol Sport Exerc 2020;47. https://doi.org/10.1016/j.psychsport.2019.101619.
- Sebire SJ, Standage M, Vansteenkiste M. Examining intrinsic versus extrinsic exercise goals: cognitive, affective, and behavioral outcomes. J Sport Exerc Psychol 2009;31:189-210. https://doi.org/10.1123/jsep.31.2.189.
- Sebire SJ, Jago R, Banfield K, Edwards MJ, Campbell R, Kipping R, et al. Results of a feasibility cluster randomised controlled trial of a peer-led school-based intervention to increase the physical activity of adolescent girls (PLAN-A). Int J Behav Nutr Phys Act 2018;15. https://doi.org/10.1186/s12966-018-0682-4.
- Sebire S, Banfield K, Campbell R, Edjwards MJ, Kipping R, Kadir B, et al. A peer-led physical activity intervention in schools for adolescent girls: a feasibility RCT. Public Health Res 2019;7. https://doi.org/10.3310/phr07160.
- Sebire SJ, Edwards MJ, Campbell R, Jago R, Kipping RR, Banfield K, et al. Protocol for a feasibility randomised controlled trial of a peer-led school-based intervention to increase the physical activity of adolescent girls (PLAN-A). Pilot Feasibility Stud 2016;2. https://doi.org/10.1186/s40814-016-0110-y.
- Sutherland R, Campbell E, Lubans DR, Morgan PJ, Okely AD, Nathan N, et al. ‘Physical Activity 4 Everyone’ school-based intervention to prevent decline in adolescent physical activity levels: 12 month (mid-intervention) report on a cluster randomised trial. Br J Sports Med 2016;50:488-95. https://doi.org/10.1136/bjsports-2014-094523.
- Sebire SJ, Banfield K, Jago R, Edwards MJ, Campbell R, Kipping R, et al. A process evaluation of the PLAN-A intervention (Peer-Led physical Activity iNtervention for Adolescent girls). BMC Public Health 2019;19. https://doi.org/10.1186/s12889-019-7545-z.
- Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ 2008;337. https://doi.org/10.1136/bmj.a1655.
- Marsh HW. Self Description Questionnaire (SDQ) II: A Theoretical and Empirical Basis for the Measurement of Multiple Dimensions of Adolescent Self-Concept. A Test Manual and Research Monograph. Penrith, NSW: Faculty of Education, University of Western Sydney; 1992.
- Eldridge SM, Chan CL, Campbell MJ, Bond CM, Hopewell S, Thabane L, et al. CONSORT 2010 statement: extension to randomised pilot and feasibility trials. BMJ 2016;355. https://doi.org/10.1136/bmj.i5239.
- Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care 2007;19:349-57. https://doi.org/10.1093/intqhc/mzm042.
- Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014;348. https://doi.org/10.1136/bmj.g1687.
- Husereau D, Drummond M, Petrou S, Carswell C, Moher D, Greenberg D, et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) – explanation and elaboration: a report of the ISPOR Health Economic Evaluation Publication Guidelines Good Reporting Practices Task Force. Value Health 2013;16:231-50. https://doi.org/10.1016/j.jval.2013.02.002.
- Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap) – a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 2009;42:377-81. https://doi.org/10.1016/j.jbi.2008.08.010.
- Boyce W, Torsheim T, Currie C, Zambon A. The family affluence scale as a measure of national wealth: validation of an adolescent self-report measure. Soc Indic Res 2006;78:473-87. https://doi.org/10.1007/s11205-005-1607-6.
- Currie C, Molcho M, Boyce W, Holstein B, Torsheim T, Richter M. Researching health inequalities in adolescents: the development of the Health Behaviour in School-Aged Children (HBSC) family affluence scale. Soc Sci Med 2008;66:1429-36. https://doi.org/10.1016/j.socscimed.2007.11.024.
- Welk GJ, Schaben JA, Morrow JR. Reliability of accelerometry-based activity monitors: a generalizability study. Med Sci Sports Exerc 2004;36:1637-45.
- Evenson KR, Catellier DJ, Gill K, Ondrak KS, McMurray RG. Calibration of two objective measures of physical activity for children. J Sports Sci 2008;26:1557-65. https://doi.org/10.1080/02640410802334196.
- Trost SG, Loprinzi PD, Moore R, Pfeiffer KA. Comparison of accelerometer cut points for predicting activity intensity in youth. Med Sci Sports Exerc 2011;43:1360-8. https://doi.org/10.1249/MSS.0b013e318206476e.
- Markland D, Tobin V. A modification of the Behavioral Regulation in Exercise Questionnaire to include an assessment of amotivation. J Sport Exerc Psychol 2004;26:191-6. https://doi.org/10.1123/jsep.26.2.191.
- McAuley E, Duncan T, Tammen VV. Psychometric properties of the Intrinsic Motivation Inventory in a competitive sport setting: a confirmatory factor analysis. Res Q Exerc Sport 1989;60:48-5. https://doi.org/10.1080/02701367.1989.10607413.
- Bartholomew JB, Loukas A, Jowers EM, Allua S. Validation of the Physical Activity Self-Efficacy Scale: testing measurement invariance between Hispanic and Caucasian children. J Phys Act Health 2006;3:70-8. https://doi.org/10.1123/jpah.3.1.70.
- Cazuza de Farias J, da Silva Lopes A, Siequeira Reis R, do Nasciemento JV, Borgatto AF, Hallall PC. Development and validation of a questionnaire measuring factors associated with physical activity in adolescents. Braz J Mother Infant Health 2011;11:301-12. https://doi.org/10.1590/S1519-38292011000300011.
- Ling J, Robbins LB, Resnicow K, Bakhoya M. Social support and peer norms scales for physical activity in adolescents. Am J Health Behav 2014;38:881-9. https://doi.org/10.5993/AJHB.38.6.10.
- Harvey J, Emm-Collison L, Sebire S. ‘I feel proper self-conscious all the time’: a qualitative study of adolescent girls’ views of menstruation and physical activity. [Version 1; peer review: 1 approved with reservations, 1 not approved.]. Wellcome Open Res 2020;5. https://doi.org/10.12688/wellcomeopenres.16391.1.
- Macneill SJ, Jago R. PLAN A: A Cluster Randomised Trial of a Peer-Led Physical Activity INtervention for Adolescent Girls. Bristol: University of Bristol; 2020.
- Jago R, Tibbitts B, Porter A, Sanderson E, Bird E, Powell JE, et al. A revised teaching assistant-led extracurricular physical activity programme for 8- to 10-year-olds: the Action 3:30R feasibility cluster RCT. Public Health Res 2019;7. https://doi.org/10.3310/phr07190.
- Jones NR, Jones A, van Sluijs EM, Panter J, Harrison F, Griffin SJ. School environments and physical activity: the development and testing of an audit tool. Health Place 2010;16:776-83. https://doi.org/10.1016/j.healthplace.2010.04.002.
- Lounsbery MA, McKenzie TL, Morrow JR, Holt KA, Budnar RG. School physical activity policy assessment. J Phys Act Health 2013;10:496-503. https://doi.org/10.1123/jpah.10.4.496.
- Jago R, Tibbitts B, Sanderson E, Bird EL, Porter A, Metcalfe C, et al. Action 3:30R: Results of a cluster randomised feasibility study of a revised teaching assistant-led extracurricular physical activity intervention for 8 to 10 year olds. Int J Environ Res Public Health 2019;16. https://doi.org/10.3390/ijerph16010131.
- Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol 2013;13. https://doi.org/10.1186/1471-2288-13-117.
- Innerd AL, Azevedo LB, Batterham AM. The effect of a curriculum-based physical activity intervention on accelerometer-assessed physical activity in schoolchildren: a non-randomised mixed methods controlled before-and-after study. PLOS ONE 2019;14. https://doi.org/10.1371/journal.pone.0225997.
- National Association of Schoolmasters Union of Women Teachers: The Teachers’ Union . Directed Time (England) 2021. www.nasuwt.org.uk/advice/conditions-of-service/directed-time/directed-time-england.html (accessed 22 May 2020).
- TES Global Ltd . Salary Scales Teacher 2020. www.tes.com/sites/default/files/main_teacherpayscale_01b.pdf (accessed 22 May 2020).
- EuroQol Research Foundation . EQ-5D-Y (Youth): About 2009. https://euroqol.org/eq-5d-instruments/eq-5d-y-about/ (accessed 22 May 2020).
- Wille N, Badia X, Bonsel G, Burstrom K, Cavrini G, Devlin N, et al. Development of the EQ-5D-Y: a child-friendly version of the EQ-5D. Quality Life Res 2010;19:875-86. https://doi.org/10.1007/s11136-010-9648-y.
- Stevens K. Valuation of the Child Health Utility 9D Index. PharmacoEconomics 2012;30:729-47. https://doi.org/10.2165/11599120-000000000-00000.
- Ratcliffe J, Huynh E, Chen G, Stevens K, Swait J, Brazier J, et al. Valuing the Child Health Utility 9D: using profile case best worst scaling methods to develop a new adolescent specific scoring algorithm. Soc Sci Med 2016;157:48-59. https://doi.org/10.1016/j.socscimed.2016.03.042.
- UNISON . National Joint Council for Local Government Services 2018. www.unison.org.uk/content/uploads/2018/08/New-NJC-Pay-Spine-2018-2019.pdf (accessed 22 May 2020).
- Child Public Health . KIDSCREEN – Health Related Quality of Life Questionnaire for Children and Young People and Their Parents 2011. www.kidscreen.org/english/ (accessed 22 May 2020).
- Chen G, Stevens K, Rowen D, Ratcliffe J. From KIDSCREEN-10 to CHU9D: creating a unique mapping algorithm for application in economic evaluation. Health Qual Life Outcomes 2014;12. https://doi.org/10.1186/s12955-014-0134-z.
- Harrington DM, Davies MJ, Bodicoat D, Charles JM, Chudasama YV, Gorely T, et al. A school-based intervention (‘Girls Active’) to increase physical activity levels among 11- to 14-year-old girls: cluster RCT. Public Health Res 2019;7. https://doi.org/10.3310/phr07050.
- Corder K, Sharp SJ, Jong ST, Foubister C, Brown HE, Wells EK, et al. Effectiveness and cost-effectiveness of the GoActive intervention to increase physical activity among UK adolescents: a cluster randomised controlled trial. PLOS Med 2020;17. https://doi.org/10.1371/journal.pmed.1003210.
- Fenwick E, Briggs A. Cost-effectiveness acceptability curves in the dock: case not proven?. Med Decis Making 2007;27:93-5. https://doi.org/10.1177/0272989X07300071.
- Mauskopf JA, Paul JE, Grant DM, Stergachis A. The role of cost-consequence analysis in healthcare decision-making. PharmacoEconomics 1998;13:277-88. https://doi.org/10.2165/00019053-199813030-00002.
- Howie EK, Straker LM. Rates of attrition, non-compliance and missingness in randomized controlled trials of child physical activity interventions using accelerometers: a brief methodological review. J Sci Med Sport 2016;19:830-6. https://doi.org/10.1016/j.jsams.2015.12.520.
- Ravens-Sieberer U, Gosch A, Rajmil L, Erhart M, Bruil J, Duer W, et al. KIDSCREEN-52 quality-of-life measure for children and adolescents. Expert Rev Pharmacoecon Outcomes Res 2005;5:353-64. https://doi.org/10.1586/14737167.5.3.353.
- Kandiyali RHW, Jago R. PLAN-A: A Cluster Randomised Trial of a Peer-led Physical Activity INtervention for Adolescent Girls: Health Economic Analysis Plan. Bristol: University of Bristol; 2020.
- European Parliament and Council of the European Union . Regulation (EU) 2016 679 of the European Parliament and of the Council of 27 April 2016 on the Protection of Natural Persons With Regard to the Processing of Personal Data and on the Free Movement of Such Data, and Repealing Directive 95 46 EC (General Data Protection Regulation) n.d.
- National Statistics . Health Survey for England 2015 Physical Activity in Children 2016.
- Aadland E, Nilsen AKO, Ylvisåker E, Johannessen K, Anderssen SA. Reproducibility of objectively measured physical activity: reconsideration needed. J Sports Sci 2020;38:1132-9. https://doi.org/10.1080/02640414.2020.1743054.
- Baranowski T, Mâsse LC, Ragan B, Welk G. How many days was that? We’re still not sure, but we’re asking the question better!. Med Sci Sports Exerc 2008;40:S544-9. https://doi.org/10.1249/MSS.0b013e31817c6651.
- Parkin S, McKeganey N. The rise and rise of peer education approaches. Drug-Educ Prev Polic 2000;7:293-310. https://doi.org/10.1080/09687630050109961.
- Ding D, Lawson KD, Kolbe-Alexander TL, Finkelstein EA, Katzmarzyk PT, van Mechelen W, et al. The economic burden of physical inactivity: a global analysis of major non-communicable diseases. Lancet 2016;388:1311-24. https://doi.org/10.1016/S0140-6736(16)30383-X.
- Jago R, Edwards MJ, Sebire SJ, Tomkinson K, Bird EL, Banfield K, et al. Effect and cost of an after-school dance programme on the physical activity of 11-12 year old girls: The Bristol Girls Dance Project, a school-based cluster randomised controlled trial. Int J Behav Nutr Phys Act 2015;12. https://doi.org/10.1186/s12966-015-0289-y.
- Charles JM, Harrington DM, Davies MJ, Edwardson CL, Gorely T, Bodicoat DH, et al. Micro-costing and a cost-consequence analysis of the ‘Girls Active’ programme: a cluster randomised controlled trial. PLOS ONE 2019;14. https://doi.org/10.1371/journal.pone.0221276.
- Sutherland R, Reeves P, Campbell E, Lubans DR, Morgan PJ, Nathan N, et al. Cost effectiveness of a multi-component school-based physical activity intervention targeting adolescents: the ‘Physical Activity 4 Everyone’ cluster randomized trial. Int J Behav Nutr Phys Act 2016;13. https://doi.org/10.1186/s12966-016-0418-2.
- Rodriguez-Ayllon M, Cadenas-Sánchez C, Estévez-López F, Muñoz NE, Mora-Gonzalez J, Migueles JH, et al. Role of physical activity and sedentary behavior in the mental health of preschoolers, children and adolescents: a systematic review and meta-analysis. Sports Med 2019;49:1383-410. https://doi.org/10.1007/s40279-019-01099-5.
- Canaway A, Frew E, Lancashire E, Pallan M, Hemming K, Adab P. Economic evaluation of a childhood obesity prevention programme for children: results from the WAVES cluster randomised controlled trial conducted in schools. PLOS ONE 2019;14. https://doi.org/10.1371/journal.pone.0219500.
- Eminson K, Canaway A, Adab P, Lancashire E, Pallan M, Frew E. How does age affect the relationship between weight and health utility during the middle years of childhood?. Qual Life Res 2018;27:1455-62. https://doi.org/10.1007/s11136-018-1790-y.
- Breheny K, Passmore S, Adab P, Martin J, Hemming K, Lancashire ER, et al. Effectiveness and cost-effectiveness of The Daily Mile on childhood weight outcomes and wellbeing: a cluster randomised controlled trial. Int J Obes 2020;44:812-22. https://doi.org/10.1038/s41366-019-0511-0.
- Wyatt K, Lloyd J, Creanor S, Green C, Dean SG, Hillsdon M, et al. Cluster randomised controlled trial and economic and process evaluation to determine the effectiveness and cost-effectiveness of a novel intervention [Healthy Lifestyles Programme (HeLP)] to prevent obesity in school children. Public Health Res 2018;6. https://doi.org/10.3310/phr06010.
- Vijay SGc, Suhrcke M, Atkin AJ, van Sluijs E, Turner D. Cost-effectiveness of physical activity interventions in adolescents: model development and illustration using two exemplar interventions. BMJ Open 2019;9. https://doi.org/10.1136/bmjopen-2018-027566.
- Harrington DM, Davies MJ, Bodicoat DH, Charles JM, Chudasama YV, Gorely T, et al. Effectiveness of the ‘Girls Active’ school-based physical activity programme: a cluster randomised controlled trial. Int J Behav Nutr Phys Act 2018;15. https://doi.org/10.1186/s12966-018-0664-6.
- Dumith SC, Gigante DP, Domingues MR, Kohl HW. Physical activity change during adolescence: a systematic review and a pooled analysis. Int J Epidemiol 2011;40:685-98. https://doi.org/10.1093/ije/dyq272.
- Escriva-Boulley G, Tessier D, Ntoumanis N, Sarrazin P. Need-supportive professional development in elementary school physical education: effects of a cluster-randomized control trial on teachers’ motivating style and student physical activity. Sport Exerc Perform 2018;7:218-34. https://doi.org/10.1037/spy0000119.
- Ha AS, Lonsdale C, Ng JYY, Lubans DR. A school-based rope skipping program for adolescents: results of a randomized trial. Prev Med 2017;101:188-94. https://doi.org/10.1016/j.ypmed.2017.06.001.
- Owen KB, Smith J, Lubans DR, Ng JY, Lonsdale C. Self-determined motivation and physical activity in children and adolescents: a systematic review and meta-analysis. Prev Med 2014;67:270-9. https://doi.org/10.1016/j.ypmed.2014.07.033.
- Ha AS, Lonsdale C, Lubans DR, Ng JYY. Increasing students’ activity in physical education: results of the self-determined exercise and learning for fitness trial. Med Sci Sports Exerc 2020;52:696-704. https://doi.org/10.1249/MSS.0000000000002172.
- Robbins LB, Wen F, Ling J. Mediators of physical activity behavior change in the ‘Girls on the Move’ intervention. Nurs Res 2019;68:257-66. https://doi.org/10.1097/NNR.0000000000000359.
- Demetriou Y, Bachner J. A school-based intervention based on self-determination theory to promote girls’ physical activity: study protocol of the CReActivity cluster randomised controlled trial. BMC Public Health 2019;19. https://doi.org/10.1186/s12889-019-6817-y.
- Lonsdale C, Lester A, Owen KB, White RL, Peralta L, Kirwan M, et al. An internet-supported school physical activity intervention in low socioeconomic status communities: results from the Activity and Motivation in Physical Education (AMPED) cluster randomised controlled trial. Br J Sports Med 2019;53:341-7. https://doi.org/10.1136/bjsports-2017-097904.
- Lubans DR, Lonsdale C, Cohen K, Eather N, Beauchamp MR, Morgan PJ, et al. Framework for the design and delivery of organized physical activity sessions for children and adolescents: rationale and description of the ‘SAAFE’ teaching principles. Int J Behav Nutr Phys Act 2017;14. https://doi.org/10.1186/s12966-017-0479-x.
- Ntoumanis N, Ng JYY, Prestwich A, Quested E, Hancox JE, Thogersen-Ntoumani C, et al. A meta-analysis of self-determination theory-informed intervention studies in the health domain: effects on motivation, health behavior, physical, and psychological health. Health Psychol Rev 2020;15:214-44. https://doi.org/10.1080/17437199.2020.1718529.
- Jago R, Sebire SJ, Cooper AR, Haase AM, Powell J, Davis L, et al. Bristol girls dance project feasibility trial: outcome and process evaluation results. Int J Behav Nutr Phys Act 2012;9. https://doi.org/10.1186/1479-5868-9-83.
- Carlin A, Murphy MH, Nevill A, Gallagher AM. Effects of a peer-led Walking In ScHools intervention (the WISH study) on physical activity levels of adolescent girls: a cluster randomised pilot study. Trials 2018;19. https://doi.org/10.1186/s13063-017-2415-4.
- Corder K, Sharp SJ, Foubister C, Brown HE, Jong ST, Wells EK, et al. Effectiveness of the GoActive intervention to increase physical activity in adolescents aged 13-14 years: a cluster randomised controlled trial. Lancet 2019;394. https://doi.org/10.1016/S0140-6736(19)32831-4.
- Owen MB, Kerner C, Taylor SL, Noonan RJ, Newson L, Kosteli MC, et al. The feasibility of a novel school peer-led mentoring model to improve the physical activity levels and sedentary time of adolescent girls: the Girls Peer Activity (G-PACT) Project. Children 2018;5. https://doi.org/10.3390/children5060067.
- Salway R, Sebire SJ, Tibbitts B, Sanderson E, Kandiyali R, Willis K, et al. Physical activity and psychosocial characteristics of the peer supporters in the PLAN-A Study – a latent class analysis. Int J Environ Res Public Health 2020;17. https://doi.org/10.3390/ijerph17217980.
- van Woudenberg TJ, Bevelander KE, Burk WJ, Smit CR, Buijs L, Buijzen M. A randomized controlled trial testing a social network intervention to promote physical activity among adolescents. BMC Public Health 2018;18. https://doi.org/10.1186/s12889-018-5451-4.
- Borgatti SP. Identifying sets of key players in a social network. Comput Math Organ Theor 2006;12:21-34. https://doi.org/10.1007/s10588-006-7084-x.
- van Woudenberg TJ, Simoski B, Fernandes de Mello Araújo E, Bevelander KE, Burk WJ, Smit CR, et al. Identifying influence agents that promote physical activity through the simulation of social network interventions: agent-based modeling study. J Med Internet Res 2019;21. https://doi.org/10.2196/12914.
- Zingora T, Stark TH, Flache A. Who is most influential? Adolescents’ intergroup attitudes and peer influence within a social network. Group Process Interg 2020;23:684-709. https://doi.org/10.1177/1368430219869460.
- Dobbie F, Purves R, McKell J, Dougall N, Campbell R, White J, et al. Implementation of a peer-led school based smoking prevention programme: a mixed methods process evaluation. BMC Public Health 2019;19. https://doi.org/10.1186/s12889-019-7112-7.
- Stone AA, Shiffman S. Ecological momentary assessment (EMA) in behavorial medicine. Ann Behav Med 1994;16:199-202. https://doi.org/10.1093/abm/16.3.199.
- Degroote L, DeSmet A, De Bourdeaudhuij I, Van Dyck D, Crombez G. Content validity and methodological considerations in ecological momentary assessment studies on physical activity and sedentary behaviour: a systematic review. Int J Behav Nutr Phys Act 2020;17. https://doi.org/10.1186/s12966-020-00932-9.
- Liao Y, Skelton K, Dunton G, Bruening M. A systematic review of methods and procedures used in ecological momentary assessments of diet and physical activity research in youth: an adapted STROBE Checklist for Reporting EMA Studies (CREMAS). J Med Internet Res 2016;18. https://doi.org/10.2196/jmir.4954.
- May M, Junghaenel DU, Ono M, Stone AA, Schneider S. Ecological momentary assessment methodology in chronic pain research: a systematic review. J Pain 2018;19:699-716. https://doi.org/10.1016/j.jpain.2018.01.006.
- LeBlanc AG, Janssen I. Difference between self-reported and accelerometer measured moderate-to-vigorous physical activity in youth. Pediatr Exerc Sci 2010;22:523-34. https://doi.org/10.1123/pes.22.4.523.
- Dyrstad SM, Hansen BH, Holme IM, Anderssen SA. Comparison of self-reported versus accelerometer-measured physical activity. Med Sci Sports Exerc 2014;46:99-106. https://doi.org/10.1249/MSS.0b013e3182a0595f.
- Pedišić Ž, Bauman A. Accelerometer-based measures in physical activity surveillance: current practices and issues. Br J Sports Med 2015;49:219-23. https://doi.org/10.1136/bjsports-2013-093407.
- Quante M, Kaplan ER, Rueschman M, Cailler M, Buxton OM, Redline S. Practical considerations in using accelerometers to assess physical activity, sedentary behavior, and sleep. Sleep Health 2015;1:275-84. https://doi.org/10.1016/j.sleh.2015.09.002.
- Pew Research Center . Teens, Social Media &Amp; Technology Overview 2015 2015. www.pewresearch.org/internet/2015/04/09/teens-social-media-technology-2015/ (accessed 20 November 2020).
- Hirvonen MK, Purcell C, Elliott L, Bailey JV, Simpson SA, McDaid L, et al. Peer-to-peer sharing of sexual health social media messages in a school-based intervention: opportunities and challenges identified in the STASH feasibility trial. J Med Internet Res 2021;23. https://doi.org/10.2196/20898.
- Beets MW, Weaver RG, Ioannidis JPA, Geraci M, Brazendale K, Decker L, et al. Identification and evaluation of risk of generalizability biases in pilot versus efficacy/effectiveness trials: a systematic review and meta-analysis. Int J Behav Nutr Phys Act 2020;17. https://doi.org/10.1186/s12966-020-0918-y.
- Estabrooks PA, Gyurcsik NC. Evaluating the impact of behavioral interventions that target physical activity: issues of generalizability and public health. Psychol Sport Exerc 2003;4:41-55. https://doi.org/10.1016/S1469-0292(02)00016-X.
- Rutter H, Savona N, Glonti K, Bibby J, Cummins S, Finegood DT, et al. The need for a complex systems model of evidence for public health. Lancet 2017;390:2602-4. https://doi.org/10.1016/S0140-6736(17)31267-9.
- Daly-Smith A, Quarmby T, Archbold VSJ, Corrigan N, Wilson D, Resaland GK, et al. Using a multi-stakeholder experience-based design process to co-develop the Creating Active Schools Framework. Int J Behav Nutr Phys Act 2020;17. https://doi.org/10.1186/s12966-020-0917-z.
- Adams J, Mytton O, White M, Monsivais P. Why are some population interventions for diet and obesity more equitable and effective than others? The role of individual agency. PLOS Med 2016;13. https://doi.org/10.1371/journal.pmed.1001990.
- Lewallen TC, Hunt H, Potts-Datema W, Zaza S, Giles W. The whole school, whole community, whole child model: a new approach for improving educational attainment and healthy development for students. J Sch Health 2015;85:729-39. https://doi.org/10.1111/josh.12310.
- Campbell MK, Piaggio G, Elbourne DR, Altman DG. CONSORT 2010 statement: extension to cluster randomised trials. BMJ 2012;345. https://doi.org/10.1136/bmj.e5661.
Appendix 1 Deductive codes for qualitative analysis
| Code | Informant group | Description |
|---|---|---|
| Recruitment/initial involvement |
Trainer Peer supporter School contact Non-peer supporter |
How the participant(s) became involved, thoughts on the recruitment process and reasons for involvement |
| Training the trainers | Trainer | Thoughts on the logistics of the training (i.e. venue, length and resources) and the content |
| Peer supporter training logistics |
Trainer Peer supporter School contact |
Views on the training venue, timings, length and catering for the training |
| Peer supporter training content |
Trainer Peer supporter School contact |
What was and was not enjoyed, activities or elements of the training that did and did not work, and any improvements to the content or adaptations made to activities |
| Delivering the peer supporter training | Trainers | Experience of delivering the training to the girls, how prepared they felt and difficulties they had |
| Impact of PLAN-A (on the peer supporter, non-peer supporters and others) |
Trainer Peer supporter School contact Non-peer supporter |
Evidence of how the training helped the girls become peer supporters, and how the training or experience of being a peer supporter has had an impact on them. The impact of PLAN-A on other Year 9 girls or the wider school. The impact of data collection |
| Views on trainers | Peer supporters | What the trainers were like and their delivery style |
| Support for peer supporters |
Peer supporters School contact |
Whether or not the peer supporters helped each other, whether or not they needed help and how the trial can encourage them to peer support |
| Needs-support |
Trainer Peer supporters |
Evidence of trainers providing autonomy support through positive feedback, offering choice, setting out clear expectations and being empathetic. It also includes evidence of genuine interest in the girls’ lives and nurturing individual interests |
| School attitude | School contact | How the school responded to being part of PLAN-A and its attitude towards all elements of the project, including data collection, peer supporter training and process evaluation. Were there any barriers to implementing PLAN-A? |
| Evidence of peer supporting |
Trainers Peer supporters School contacts Non-peer supporter |
Any evidence that a peer supporter provided support, attempted to support or did nothing to peer support |
| Problems/issues experienced during PLAN-A |
Trainers Peer supporters School contacts |
Issues peer supporter had with being a peer supporter (e.g. bullying) or general problems with PLAN-A in school |
| PLAN-A sustainability |
Peers supporters School contacts |
How can the impact of PLAN-A be sustained? How can we ensure success? What is appealing about PLAN-A that would encourage others to take part? |
| Data collection |
School contacts Non-peer supporter |
Logistics and experiences of data collection, and improvements |
| General attitudes towards physical activity |
Peer supporters Non-peer supporter |
The views and experiences of physical activity among Year 9 girls |
Appendix 2 Mean and difference in mean counts per minute on weekdays, weekends and average
| Trial arm | Value | Mean (SD)/p-value |
|---|---|---|
| Weekdays | ||
| Intervention (n) | 603 | 354.55 (119.24) |
| Control (n) | 616 | 382.13 (178.36) |
| Difference in means (95% CI)a | –22.23 (–44.43 to –0.05) | 0.05 |
| Difference in means (95% CI)b | –26.27 (–45.29 to –7.25) | 0.007 |
| Weekends | ||
| Intervention (n) | 347 | 376.29 (364.58) |
| Control (n) | 386 | 352.60 (364.61) |
| Difference in means (95% CI)a | –24.22 (–111.77 to 63.34) | 0.588 |
| Difference in means (95% CI)b | –16.74 (–96.86 to 63.38) | 0.682 |
| Average across all valid days | ||
| Intervention (n) | 603 | 357.06 (126.57) |
| Control (n) | 616 | 379.15 (198.85) |
| Difference in means (95% CI)a | –20.41 (–41.57 to 0.75) | 0.059 |
| Difference in means (95% CI)b | –21.54 (–40.79 to –2.29) | 0.028 |
Appendix 3 Weekday moderate to vigorous physical activity in peer supporters and non-peer supporters in intervention schools only
| Weekday MVPA | Peer supporters | Non-peer supporters | ||
|---|---|---|---|---|
| Number | Mean (SD) | Number | Mean (SD) | |
| T0 | 163 | 53.62 (19.43) | 530 | 50.23 (20.73) |
| T1 | 149 | 45.21 (18.78) | 454 | 45.19 (18.34) |
| Change in MVPA: T1 – T0 | 138 | –9.30 (17.12) | 430 | –5.05 (16.69) |
| Adjusted difference in T1 MVPA between peer supporter and non-peer supporter (95% CI)a | –2.25 (–5.27 to 0.22) | p-value = 0.071 | ||
Appendix 4 Mapped Child Health Utility, nine dimensions, scores (unadjusted, all available data)
| CHU-9D score | Baseline | Follow-up | ||
|---|---|---|---|---|
| Control arm (N = 800) | Intervention arm (N = 758) | Control arm (N = 800) | Intervention (N = 758) | |
| Number of participants with data available (%) | 788 (98.5) | 738 (97.4) | 683 (85.4) | 673 (88.8) |
| Mean | 0.832 | 0.832 | 0.807 | 0.810 |
| SD | 0.097 | 0.097 | 0.096 | 0.097 |
| 5th percentile | 0.660 | 0.657 | 0.634 | 0.635 |
| 95th percentile | 0.980 | 0.971 | 0.948 | 0.957 |
| Minimum | 0.566 | 0.566 | 0.566 | 0.566 |
| Maximum | 1.000 | 1.000 | 1.000 | 1.000 |
Appendix 5 Trainers’ evaluation of the training arrangements (2-day and top-up day training)
| Question | Evaluation score, mean (SD) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| School ID, trainer ID | All schools | ||||||||||
| 1, A and D | 2, C and E | 4, B and F | 5, D and G | 7, E and F | 10, A and B | 14, C and E | 15, D and G | 16, A and C | 17, C and E | ||
| 2-day training | |||||||||||
| Transport to and from the venue (for pupils) | 2.50 (0.71) | 4.00a | 4.00a | 4.00 (0.00) | b | b | b | 2.50 (0.71) | 1.00a | b | 3.00 (1.12) |
| Suitability of the training space | 3.00 (0.00) | 3.50 (0.71) | 3.50 (0.71) | 2.00 (0.00) | 1.50 (0.71) | 2.00 (0.00) | 2.50 (0.71) | 2.50 (0.71) | 4.00 (0.00) | 3.50 (0.71) | 2.80 (0.89) |
| Quality of the facilities (e.g. toilets, kitchen, social spaces) | 2.00 (0.00) | 3.50 (0.71) | 3.50 (0.71) | 1.50 (0.71) | 3.50 (0.71) | 1.00 (0.00) | 2.00 (0.00) | 2.50 (0.71) | 2.50 (0.71) | 3.50 (0.71) | 2.55 (1.00) |
| Location (i.e. distance from school) | 3.00 (0.00) | 4.00a | 4.00 (0.00) | 4.00 (0.00) | 3.50 (0.71) | b | 2.50 (0.71) | 3.00 (0.00) | 2.50 (0.71) | 3.50 (0.71) | 3.29 (0.69) |
| Training manual | 4.00 (0.00) | 4.00 (0.00) | 4.00 (0.00) | 4.00 (0.00) | 3.50 (0.71) | 4.00 (0.00) | 4.00 (0.00) | 4.00 (0.00) | 4.00 (0.00) | 4.00 (0.00) | 3.95 (0.22) |
| Resources to support the training | 4.00 (0.00) | 4.00 (0.00) | 4.00 (0.00) | 4.00 (0.00) | 4.00 (0.00) | 4.00 (0.00) | 4.00 (0.00) | 4.00 (0.00) | 4.00a | 4.00 (0.00) | 4.00 (0.00) |
| Arrangements for refreshments | 2.50 (0.71) | 3.50 (0.71) | 3.00 (0.00) | 2.00 (1.41) | 4.00 (0.00) | 3.00 (0.00) | 3.50 (0.71) | 3.00 (0.00) | 3.00 (0.00) | 1.00 (0.00) | 2.85 (0.93) |
| Quality of refreshments | 2.00 (0.00) | 3.50 (0.71) | 3.00 (0.00) | 1.00 (0.00) | 4.00 (0.00) | 3.00 (0.00) | 3.50 (0.71) | 3.00 (0.00) | 1.50 (0.71) | 0.00 (0.00) | 2.45 (1.28) |
| Top-up day training | |||||||||||
| Transport to and from the venue (for pupils) | 3.50 (0.71) | 3.00a | 3.50 (0.71) | 3.00 (0.00) | b | c | 3.00a | b | 2.00a | 3.00a | 2.80 (1.14) |
| Suitability of the training space | 3.50 (0.71) | 3.00 (0.00) | 3.50 (0.71) | 1.50 (0.71) | 2.50 (0.71) | c | 2.00 (0.00) | 3.00 (0.00) | 3.00 (0.00) | 2.00 (0.00) | 2.67 (0.77) |
| Quality of the facilities (e.g. toilets, kitchen, social spaces) | 2.50 (0.71) | 0.50 (0.71) | 3.00 (0.00) | 0.50 (0.71) | 2.00 (0.00) | c | 2.00 (0.00) | 2.50 (0.71) | 3.00 (0.00) | 1.00 (0.00) | 1.89 (1.02) |
| Location (i.e. distance from school) | 3.50 (0.71) | 2.50 (0.71) | 3.50 (0.71) | 3.50 (0.71) | b | c | 2.50 (0.71) | 2.00a | 3.50 (0.71) | 1.50 (0.71) | 2.87 (0.92) |
| Training manual | 4.00 (0.00) | 4.00 (0.00) | 3.50 (0.71) | 4.00 (0.00) | 4.00 (0.00) | c | 3.50 (0.71) | 4.00 (0.00) | 4.00 (0.00) | 4.00 (0.00) | 3.89 (0.32) |
| Resources to support the training | 4.00 (0.00) | 4.00 (0.00) | 4.00 (0.00) | 4.00 (0.00) | 4.00 (0.00) | c | 3.50 (0.71) | 4.00 (0.00) | 4.00 (0.00) | 4.00 (0.00) | 3.94 (0.24) |
| Arrangements for refreshments | 3.50 (0.71) | 2.00 (0.00) | 3.00 (0.00) | 0.00 (0.00) | 3.00 (0.00) | c | 3.50 (0.71) | 4.00 (0.00) | 3.50 (0.71) | 3.50 (0.71) | 2.89 (1.23) |
| Quality of refreshments | 2.50 (0.71) | 2.00 (0.00) | 3.00 (0.00) | 0.00 (0.00) | 3.00 (0.00) | c | 3.00 (1.41) | 4.00 (0.00) | 3.50 (0.71) | 3.50 (0.71) | 2.72 (1.23) |
Appendix 6 Trainers’ evaluation of the level of achievement of the training objectives (2-day and top-up day training)
| Question | Evaluation score, mean (SD) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| School ID, trainer ID | All schools | ||||||||||
| 1, A and D | 2, C and E | 4, B and F | 5, D and G | 7, E and F | 10, A and B | 14, C and E | 15, D and G | 16, A and C | 17, C and E | ||
| 2-day training | |||||||||||
| Increasing PSs’ knowledge about physical activity | 3.00 (0.00) | 2.50 (0.71) | 3.00 (0.00) | 3.00 (0.00) | 2.50 (0.71) | 2.50 (0.71) | 3.00 (0.00) | 2.00 (0.00) | 3.00 (0.00) | 2.00 (0.00) | 2.65 (0.49) |
| Enhancing PSs’ interpersonal skills | 3.00 (0.00) | 2.00 (0.00) | 2.00 (0.00) | 3.00 (0.00) | 2.00 (0.00) | 2.00 (0.00) | 3.00 (0.00) | 2.00 (0.00) | 2.00 (0.00) | 0.50 (0.71) | 2.15 (0.75) |
| Enhancing PSs’ communication skills | 3.00 (0.00) | 2.50 (0.71) | 2.50 (0.71) | 3.00 (0.00) | 2.50 (0.71) | 1.50 (0.71) | 3.00 (0.00) | 2.00 (0.00) | 1.50 (0.71) | 1.00 (0.00) | 2.25 (0.79) |
| Enhancing PSs’ confidence to instigate informal, health-promoting conversations with peers | 2.50 (0.71) | 2.50 (0.71) | 2.00 (0.00) | 3.00 (0.00) | 3.00 (0.00) | 2.00 (0.00) | 3.00 (0.00) | 2.00 (0.00) | 2.00 (0.00) | 1.00 (0.00) | 2.30 (0.66) |
| How much did the PSs understand their role? | 3.00 (0.00) | 2.00 (0.00) | 3.00 (0.00) | 3.00 (0.00) | 2.00 (0.00) | 2.50 (0.71) | 3.00 (0.00) | 2.00 (0.00) | 2.50 (0.71) | 0.50 (0.71) | 2.35 (0.81) |
| Top-up day training | |||||||||||
| Increasing PSs’ knowledge about physical activity | 2.50 (0.71) | 2.50 (0.71) | 2.50 (0.71) | 3.00 (0.00) | 2.00 (0.00) | b | 3.00 (0.00) | 2.00 (0.00) | 2.00 (0.00) | 1.50 (0.71) | 2.33 (0.59) |
| Enhancing PSs’ interpersonal skills | 3.00 (0.00) | 2.50 (0.71) | 2.00 (0.00) | 3.00 (0.00) | 2.00 (0.00) | b | 2.00 (0.00) | 2.00 (0.00) | 1.50 (0.71) | 2.00 (0.00) | 2.22 (0.55) |
| Enhancing PSs’ communication skills | 2.50 (0.71) | 2.50 (0.71) | 2.00 (0.00) | 3.00 (0.00) | 2.00 (0.00) | b | 2.00 (0.00) | 2.00a | 2.00a | 1.50 (0.71) | 2.19 (0.54) |
| Enhancing PSs’ confidence to instigate informal, health-promoting conversations with peers | 2.50 (0.71) | 2.50 (0.71) | 2.00a | 3.00 (0.00) | 2.00 (0.00) | b | 2.50 (0.71) | 2.50 (0.71) | 2.00 (0.00) | 2.00 (0.00) | 2.35 (0.49) |
| How much did the PSs understand their role? | 3.00 (0.00) | 2.50 (0.71) | 2.00 (0.00) | 3.00 (0.00) | 2.00 (0.00) | b | 2.50 (0.71) | 2.50 (0.71) | 2.50 (0.71) | 1.00 (0.00) | 2.33 (0.69) |
Appendix 7 Trainers’ evaluation of peer supporters’ response to the training (2-day and top-up day training)
| Question | Evaluation score, mean (SD) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| School ID, trainer ID | All schools | ||||||||||
| 1, A and D | 2, C and E | 4, B and F | 5, D and G | 7, E and F | 10, A and B | 14, C and E | 15, D and G | 16, A and C | 17, C and E | ||
| 2-day training | |||||||||||
| How involved were they? | 3.00 (0.00) | 3.00 (0.00) | 3.00 (0.00) | 2.50 (0.71) | 2.00 (0.00) | 2.00 (0.00) | 3.00 (0.00) | 2.00 (0.00) | 3.00 (0.00) | 2.00 (0.00) | 2.55 (0.51) |
| How engaged were they? | 3.00 (0.00) | 2.50 (0.71) | 2.50 (0.71) | 3.00 (0.00) | 1.50 (0.71) | 1.50 (0.71) | 3.00 (0.00) | 2.00 (0.00) | 3.00 (0.00) | 1.00 (0.00) | 2.30 (0.80) |
| How much did you think they enjoyed themselves? | 3.00 (0.00) | 2.00 (0.00) | 2.50 (0.71) | 2.00 (0.00) | 2.00 (0.00) | 2.00 (0.00) | 3.00 (0.00) | 2.50 (0.71) | 2.50 (0.71) | 0.00 (0.00) | 2.15 (0.88) |
| What was their overall level of interest? | 3.00 (0.00) | 2.00 (0.00) | 2.00 (0.00) | 2.50 (0.71) | 2.00 (0.00) | 1.50 (0.71) | 3.00 (0.00) | 2.00 (0.00) | 3.00 (0.00) | 0.00 (0.00) | 2.10 (0.91) |
| Question | 1, A and D | 2, C and E | 4, B and F | 5, D and G | 7, D and F | 10, B and C | 14, C and F | 15, C and G | 16, A and C | 17, C and E | All schools, mean (SD) |
| Top-up day training | |||||||||||
| How involved were they? | 3.00 (0.00) | 3.00 (0.00) | 3.00 (0.00) | 3.00 (0.00) | 1.50 (0.71) | b | 3.00 (0.00) | 2.50 (0.71) | 2.50 (0.71) | 2.00 (0.00) | 2.61 (0.61) |
| How engaged were they? | 3.00 (0.00) | 3.00 (0.00) | 2.50 (0.71) | 3.00 (0.00) | 1.00 (0.00) | b | 3.00 (0.00) | 2.00 (0.00) | 2.50 (0.71) | 1.50 (0.71) | 2.39 (0.78) |
| How much did you think they enjoyed themselves? | 3.00 (0.00) | 3.00 (0.00) | 2.50 (0.71) | 3.00 (0.00) | 1.50 (0.71) | b | 2.50 (0.71) | 2.00a | 2.50 (0.71) | 2.00 (0.00) | 2.47 (0.62) |
| What was their overall level of interest? | 3.00 (0.00) | 3.00 (0.00) | 2.00 (0.00) | 3.00 (0.00) | 1.50 (0.71) | b | 2.00 (0.00) | 2.00 (0.00) | 2.50 (0.71) | 1.00 (0.00) | 2.22 (0.73) |
Appendix 8 Observed versus allocated time for training activities on all 3 training days
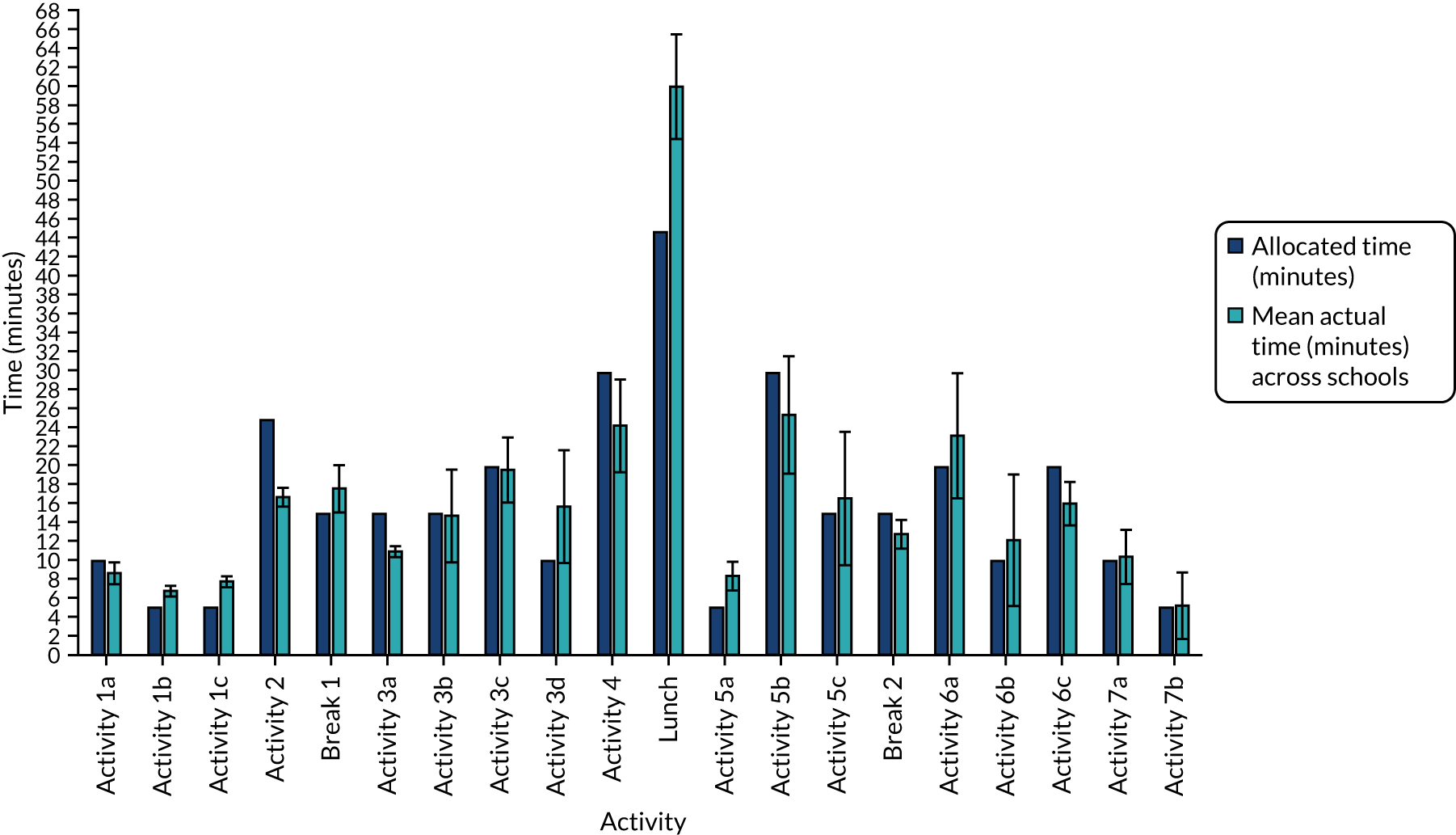
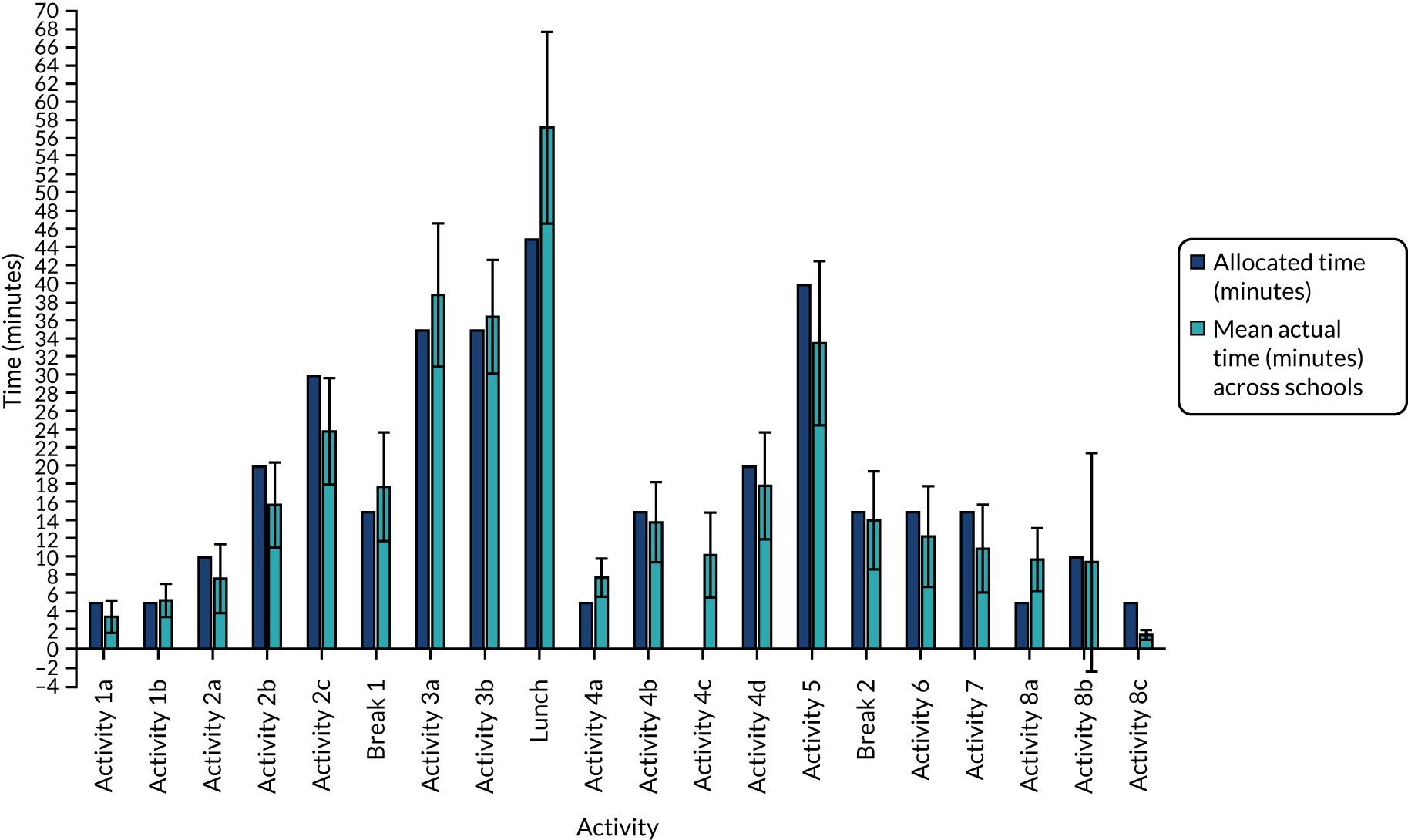
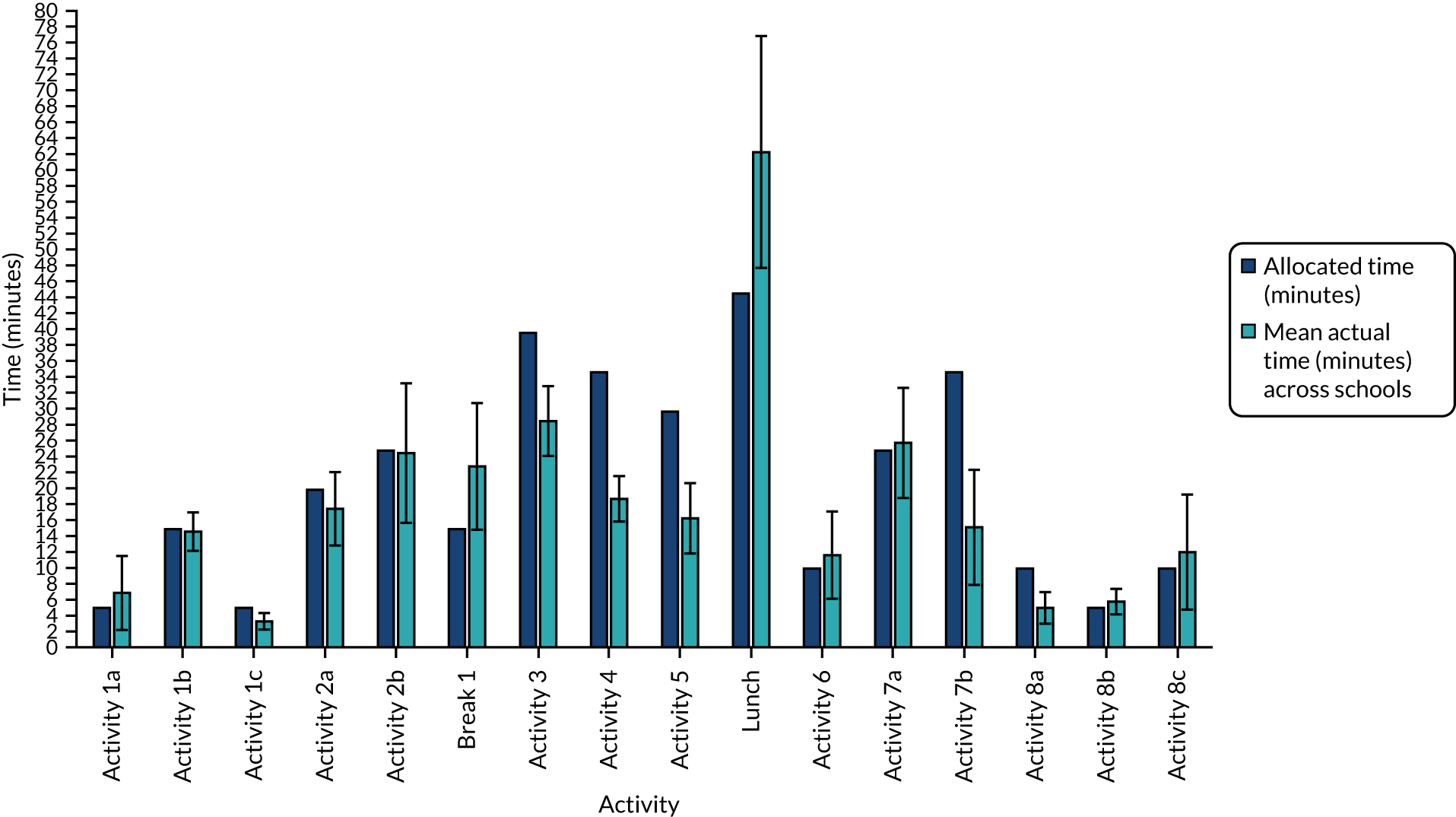
Appendix 9 Types and reach of peer-supporting activities attempted by peer supporters in the first 5 weeks following the 2-day training
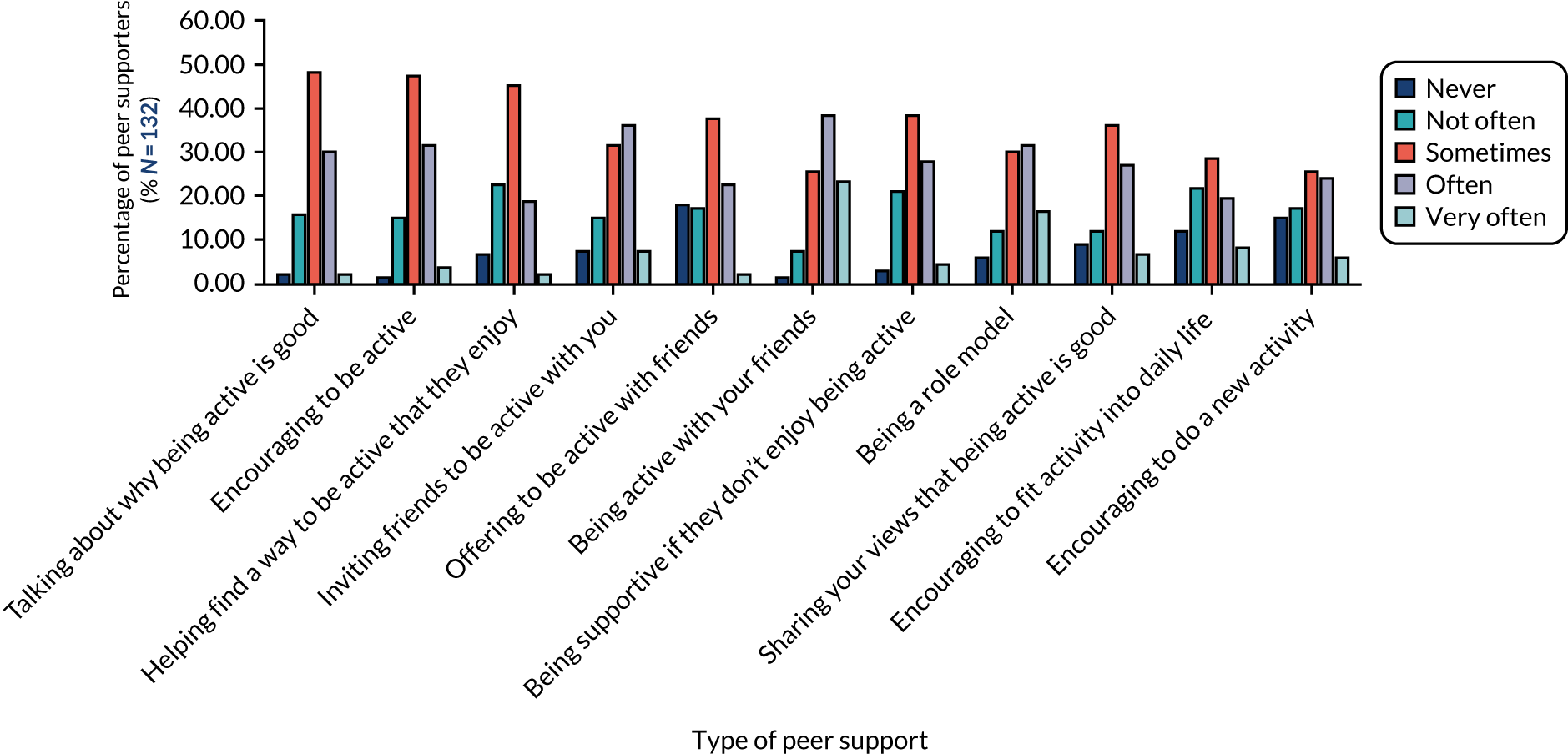
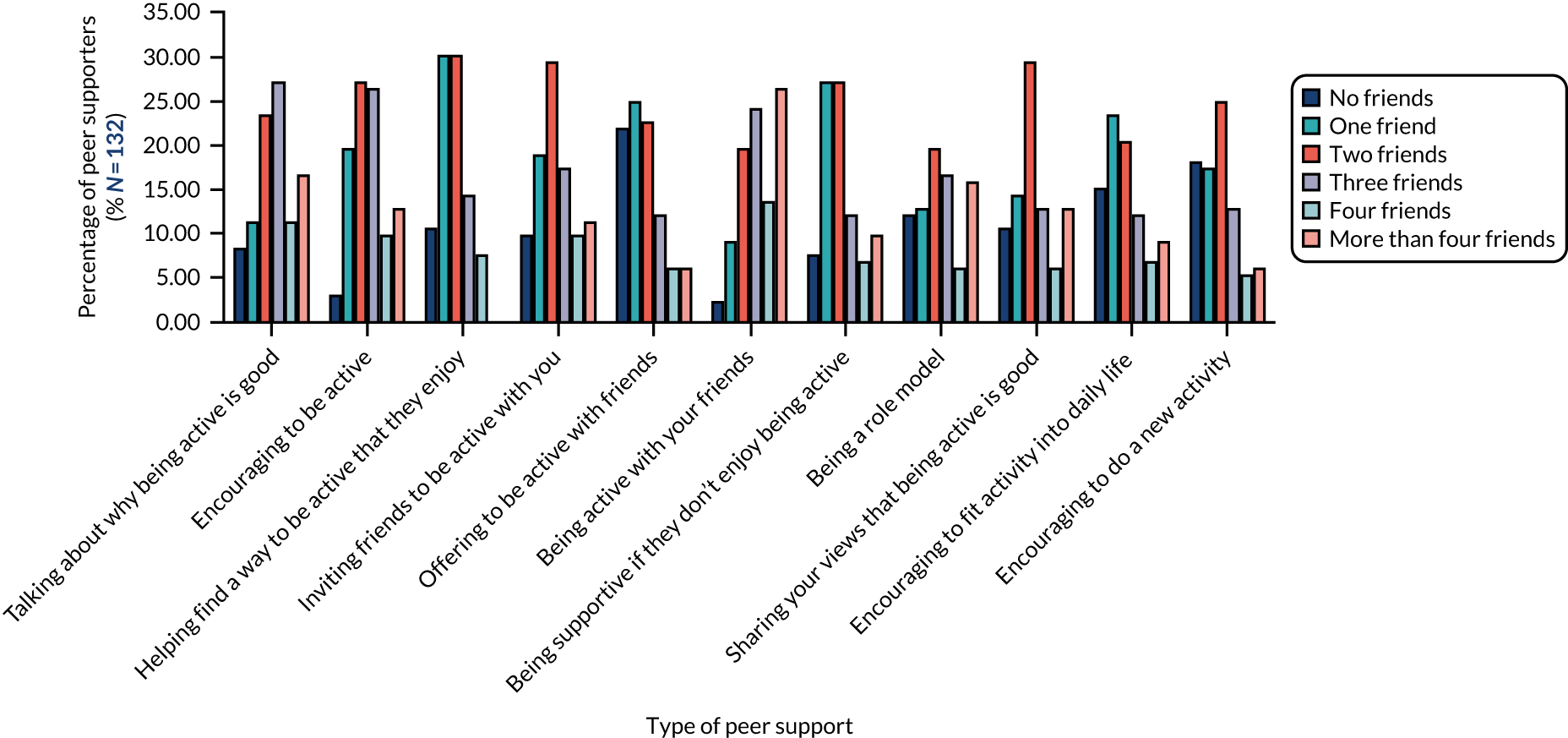
Appendix 10 School policy on physical education provision and attitude towards physical activity
| Item | Intervention school ID (number of pupils in school/Year 9) | Total (%) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 (809/164) | 2 (973/176) | 4 (995/166) | 5 (841/164) | 7 (1557/251) | 10 (1285/224) | 14 (920/152) | 15 (878/146) | 16 (918/125) | 17 (945/170) | ||
| Written policy requiring PE programme to follow specific PE standards/guidelines? | ✓ | ✗ | ✓ | ✗ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 8 (80) |
| If ‘no’, informal policy? | ✗ | ✓ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | – |
| Written policy requiring pupils to have a specific amount of PE? | ✗ | ✓ | ✗ | ✓ | ✓ | ✓ | ✗ | ✗ | ✓ | ✓ | 6 (60) |
| If ‘no’, informal policy? | ✗ | ✗ | ✓ | ✗ | ✗ | ✗ | ✗ | ✓ | ✗ | ✗ | – |
| Policy that encourages students to walk/cycle to school? | ✗ | ✗ | ✓ | ✗ | ✗ | ✓ | ✗ | ✗ | ✗ | ✗ | 2 (20) |
| Does your school offer cycle training [e.g. Bikeability (The Bikeability Trust, Cambridge UK)]? | ✓ | ✓ | ✗ | ✗ | ✓ | ✗ | ✗ | ✓ | ✓ | ✗ | 5 (50) |
| Policy requiring all staff to receive training on the promotion of physical activity? | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | 0 (0) |
| Encouraging staff to be active (written policy)? | ✗ | ✓ | ✗ | ✓ | ✓ | ✓ | ✗ | ✓ | ✗ | ✗ | 5 (50) |
| Provide facilities supporting staff to be active? | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✓ | ✓ | 9 (90) |
| Budget allocation for PE equipment/supplies? | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 10 (100) |
| If ‘yes’, on average, how much? | £2000 | £3000 | ✓ | ✓ | ✓ | ✓ | ✓ | £3500 | £1066 | ✗ | – |
| How involved is the PE teacher with PE budget decisions? | B | A | A | B | B | A | A | B | A | A | A |
| Scorea | 6 | 8 | ✗ | 6 | 9 | 10 | 6 | 6 | 9 | 8 | 7.50 (1.51) |
| Item | Control school ID (number of pupils in school/Year 9) | Total (%) | |||||||||
| 3 (1209/179) | 6 (778/139) | 8 (1484/247) | 9 (759/155) | 11 (1685/224) | 12 (759/178) | 13 (1323/299) | 18 (815/175) | 19 (1093/198) | 20 (978/130) | ||
| Written policy requiring PE programme to follow specific PE standards/guidelines? | ✓ | ✓ | ✓ | ✓ | ✓ | Do not know | ✓ | ✓ | ✗ | Do not know | 6 (60) |
| If ‘no’, informal policy? | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✓ | ✗ | – |
| Written policy requiring pupils to have a specific amount of PE? | ✓ | ✗ | ✓ | ✓ | ✓ | ✗ | ✓ | ✓ | ✗ | ✗ | 6 (60) |
| If ‘no’, informal policy? | ✗ | ✗ | ✗ | ✗ | ✗ | ✓ | ✗ | ✗ | ✗ | ✗ | – |
| Policy that encourages students to walk/cycle to school? | Do not know | ✓ | ✓ | ✗ | ✓ | ✗ | Do not know | ✗ | ✗ | ✓ | 4 (40) |
| Does your school offer cycle training (e.g. Bikeability)? | ✓ | ✗ | ✗ | ✓ | Do not know | ✗ | ✓ | ✓ | ✗ | ✗ | 4 (40) |
| Policy requiring all staff to receive training on the promotion of physical activity? | Do not know | ✗ | ✗ | ✗ | Do not know | ✗ | ✗ | ✗ | ✗ | ✗ | 0 (0) |
| Encouraging staff to be active (written policy)? | ✓ | ✓ | ✓ | ✗ | ✓ | ✗ | Do not know | ✓ | ✗ | ✓ | 6 (60) |
| Provide facilities supporting staff to be active? | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 10 (100) |
| Budget allocation for PE equipment/supplies? | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 10 (100) |
| If ‘yes’, on average, how much? | £3000 | £5500 | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | £6940 | £600 | – |
| How involved is the PE teacher with PE budget decisions? | A | A | A | A | B | A | A | A | B | C | A |
| Scorea | 10 | 8 | 10 | 7 | 9 | 4 | 9 | 10 | 3 | 4 | 7.40 (2.62) |
Appendix 11 Physical activity throughout the wider curriculum
| Item | Intervention school ID (number of pupils in school/Year 9) | Total (%) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 (809/164) | 2 (973/176) | 4 (995/166) | 5 (841/164) | 7 (1557/251) | 10 (1285/224) | 14 (920/152) | 15 (878/146) | 16 (918/125) | 17 (945/170) | ||
| Physical activity use in non-PE KS3 subjects? | ✗ | Do not know | Do not know | ✗ | ✓ | ✗ | ✓ | ✗ | ✗ | ✓ | 3 (30) |
| If yes, what subjects? | ✗ | ✗ | ✗ | ✗ | Science and PSHE | ✗ | Biology and PSHE | ✗ | ✗ | Science and Drama | – |
| Teachers provide regular physical activity breaks throughout the day? | ✓Individual teachers | ✗ | ✓Individual teachers | Do not know | ✓School wide | ✗ | ✗ | ✗ | ✗ | Do not know | 3 (30) |
| Teachers encouraged to promote physical activity with their students? | Do not know | ✗ | ✗ | ✗ | ✓ | ✓ | ✓ | ✗ | ✓ | ✓ | 5 (50) |
| Frequency that students are withheld from PE to fulfil academic requirements? | B | B | C | B | – | B | C | A | C | B | B |
| Frequency that PE delivery is compromised for competing demands for PE space? | B | B | C | B | C | A | C | B | B | B | B |
| School rules about when students can access certain playgrounds/fields/equipment during breaks? | ✓ Year 11: sports hall, field (seasonal) | ✗ | ✓ open to all: field (seasonal), playground (all year) | ✓ available to all: equipment, lunch time clubs | ✓ open to all: AstroTurf (AstroTurf, Dalton, GA, USA), tennis courts (seasonal) | ✓ seasonal access to field | ✓ open to set year groups and at set times: main field; aged ≥ 16 years: gym | ✓open to set year groups and at set times: different yards | ✗ | ✓ Year 7: small playground; open to set years, genders and times: sports hall | 7 (70) |
| Other comments about how physical activity is thought of or prioritised in school | Core PE: Years 7–11, 2.5 hours per week. Value physical activity a lot, especially at stressful times (for mental health) | ✗ | It’s very strong during extracurricular | Core PE: KS3 two lessons per week (one activity and one fitness), KS4 1 hour per week (competitive or leisure) | Very well supported with whole school | Valued and celebrated | One of our 10 core aims. Working with local primary school to offer weekly PE sessions | ✗ | ✗ | Sport and PE are well respected and promoted at the school | – |
| Scorea | 3 | 2 | 5 | 2 | 5 | 2 | 6 | 1 | 3 | 3 | 3.20 (1.62) |
| Item | Control school ID (number of pupils in school/Year 9) | Total (%) | |||||||||
| 3 (1209/179) | 6 (778/139) | 8 (1484/247) | 9 (759/155) | 11 (1685/224) | 12 (759/178) | 13 (1323/299) | 18 (815/175) | 19 (1093/198) | 20 (978/130) | ||
| Physical activity use in non-PE KS3 subjects? | ✓ | ✓ | ✓ | ✗ | ✓ | X | ✓ | Do not know | ✗ | ✗ | 5 (50) |
| If yes, what subjects? | Drama and Science | Drama and PSHE | PSHE and Biology | ✗ | Biology – sport science project | ✗ | Drama, Science, English and PSHE | ✗ | ✗ | ✗ | – |
| Teachers provide regular physical activity breaks throughout day? | Do not know | ✗ | ✓ Individual teachers | ✗ | ✗ | ✗ | Do not know | ✓ Individual teachers | ✗ | ✗ | 2 (20) |
| Teachers encouraged to promote physical activity with their students? | ✓ | Do not know | ✓ | Do not know | ✓ | ✗ | ✓ | ✓ | ✓ | ✗ | 6 (60) |
| Frequency that students are withheld from PE to fulfil academic requirements? | B | C | B | C | B | C | B | C | B | B | B |
| Frequency that PE delivery is compromised for competing demands for PE space? | A | C | A | C | B | B | B | C | A | A | B |
| School rules about when students can access certain playgrounds/fields/equipment during breaks? | ✗ | ✓ field (seasonal) and courts (all year) | ✗ | ✓ Year 11: AstroTurf (Year 7 allowed after May half-term) | ✓ open/available to all: AstroTurf/courts (weather dependent) and equipment | ✓ weather dependent. Year 7: lower playground | ✗ | ✓ all times | ✓ open to set year groups at set times: sports hall; open to all: playground | ✓ open to set year groups at set times: sports hall. No ‘large’ balls in courtyard | 7 (70) |
| Other comments about how physical activity is thought of or prioritised in school | Held in extremely high regard. Valued and supported by a strong SLT | High priority in terms. Extracurriculars highly regarded | Held in high regard. Promoted and encouraged | ✗ | ✗ | Waiting for development of site for space allowing more physical activity/PE (currently only have a 3G pitch) | Representative sports are encouraged (have fewer PE hours). Is valued | ✗ | Exams take priority. Students are often pulled from PE to do extra Maths and English | Low priority for school | – |
| Scorea | 3 | 5 | 6 | 4 | 4 | 3 | 4 | 6 | 2 | 1 | 3.80 (1.62) |
Appendix 12 School physical activity provision scores
| School ID (number of pupils in school/Year 9) | Score | Mean (SD) quality of facility provisione | School physical activity suitability scoref | |||
|---|---|---|---|---|---|---|
| Cycling provisiona | Walking provisionb | Sports and play facility provisionc | Design of school groundsd | |||
| 1 (809/164) | 29 | 13 | 53 | 15 | 4.89 (0.33) | 97 |
| 2 (973/176) | 35 | 18 | 40 | 13 | 4.57 (0.79) | 88 |
| 3 (1209/179) | 26 | 19 | 47 | 12 | 3.70 (0.82) | 85 |
| 4 (995/166) | 32 | 18 | 39 | 11 | 3.88 (0.64) | 82 |
| 5 (841/164) | 29 | 15 | 37 | 15 | 3.50 (0.76) | 81 |
| 6 (778/139) | 28 | 13 | 58 | 15 | 4.18 (0.75) | 101 |
| 7 (1557/251) | 17 | 17 | 63 | 15 | 4.17 (0.58) | 95 |
| 8 (1484/247) | 27 | 14 | 67 | 16 | 4.25 (0.45) | 110 |
| 9 (759/155) | 44 | 25 | 46 | 11 | 4.00 (1.00) | 101 |
| 10 (1285/224) | 33 | 23 | 49 | 15 | 4.22 (0.83) | 97 |
| 11 (1685/224) | 24 | 17 | 43 | 11 | 4.38 (0.52) | 78 |
| 12 (759/178) | 18 | 13 | 32 | 10 | 4.17 (0.75) | 60 |
| 13 (1323/299) | ||||||
| Site A | 29 | 18 | 34 | 11 | 3.25 (0.89) | 74 |
| Site B | 29 | 22 | 25 | 15 | 3.00 (1.26) | 69 |
| 14 (920/152) | 27 | 23 | 32 | 13 | 3.57 (0.98) | 74 |
| 15 (878/146) | 17 | 14 | 37 | 13 | 4.29 (1.11) | 69 |
| 16 (918/125) | 23 | 17 | 42 | 14 | 4.13 (0.99) | 72 |
| 17 (945/170) | 18 | 11 | 30 | 13 | 3.29 (0.49) | 67 |
| 18 (815/175) | 33 | 28 | 41 | 15 | 3.56 (0.53) | 79 |
| 19 (1093/198) | 24 | 18 | 42 | 12 | 3.56 (1.13) | 61 |
| 20 (978/130) | 41 | 23 | 35 | 9 | 3.38 (0.52) | 89 |
| Trial arm | ||||||
| Control | 29.36 (7.54) | 19.09 (4.95) | 42.73 (11.92) | 12.45 (2.38) | 3.77 (0.46) | 84.55 (15.00) |
| Intervention | 26.00 (6.83) | 16.90 (3.93) | 42.20 (10.10) | 13.70 (1.34) | 4.05 (0.50) | 81.90 (12.61) |
Appendix 13 Termly physical activity provision changes, by school
| Intervention school ID | Physical activity provision change | Control school ID | Physical activity provision change |
|---|---|---|---|
| 1 | No participation in other research projects. Participated in a series of sessions with a professional club promoting girls’ rugby between T0 and T1. More team sport was added to PE provision in Year 10. Extracurricular physical activity opportunities remained similar between T0 and T1 | 3 | No involvement in other research projects. Annual involvement in the This Girl Can campaign (Sport England) each February. Between T0 and T1, PE provision now includes inspiring mass fitness sessions (e.g. HIIT to music) and contemporary fitness class activities such as Body Pump |
| 2 | No participation in other research projects or local initiatives. PE provision between Year 9 and Year 10 unchanged. After-school club options have greatly reduced for Year 10 girls compared with Year 9 girls | 6 | No participation in other research projects or local initiatives. PE provision focus shifted from games and sports to being more health based. Participation in football and netball extracurricular clubs has increased in Year 10 girls |
| 4 | No participation in other research projects or local initiatives. PE provision between Year 9 and Year 10 unchanged. Extracurricular clubs stayed similar in Year 10 to those in Year 9 | 8 | No participation in other research projects or local initiatives. PE provision stayed the same between Year 9 and Year 10. The range of extracurricular clubs decreased slightly in Year 10 from Year 9 |
| 5 | No participation in other research projects or local initiatives. PE provision dropped to one lesson per week in Year 10 from two in Year 9. No change in after-school provision | 9 | No participation in other research projects or local initiatives. PE provision stayed the same between Year 9 and Year 10. No real difference between after-school provision in Year 10 and Year 9 |
| 7 | No participation in other research projects or local initiatives. In Year 10, girls had a greater variety of activities to pick from and had autonomy over which they could take part in. Termly extracurricular activity on offer was similar across the year | 11 | No participation in other research projects or local initiatives. Activities in the PE curriculum have changed slightly, but have not increased/decreased. No change between Year 10 and Year 9 extracurricular clubs |
| 10 | No participation in other research projects or local initiatives. No change in PE provision between T0 and T1. Slight reduction in club range for extracurricular provision | 12 | No participation in other research projects or local initiatives. Reduced hours of compulsory PE in Year 10 compared with those in Year 9. Slightly reduced number of extracurricular clubs in Year 10 from Year 9 |
| 14 | No participation in other research projects or local initiatives. Weekly PE provision increased by 2 hours, although this included theoretical work. Increased offering of lunchtime/extracurricular opportunities, but girls must pay for these | 13 | No participation in other research projects or local initiatives. PE provision has halved from 2 hours in Year 9 to 1 hour in Year 10. Extracurricular options largely the same. Split site means that half of the girls have access to a fitness suite; the others have to walk between sites to access it (approximately 10 minutes walk) |
| 15 | No participation in other research projects or local initiatives. Boxercise was added for Year 10 for PE provision. Extracurricular clubs differ depending on the season, but no real change between T0 and T1 | 18 | No participation in other research projects. School took part in the Healthy Lifestyle Champions programme (Youth Sport Trust, Loughborough, UK), with two girls providing physical activity opportunities for other students in the school. PE provision focus was tailored to the year group and shifted towards more focus on fitness, teamwork and motivation |
| 16 | No participation in other research projects. Took part in This Girl Can campaign, which provided access to local leisure facilities between T0 and T1. Girls football was added to the PE curriculum. No real changes to after-school clubs between T0 and T1 | 19 | No participation in other research projects or local initiatives. PE curriculum changed between Year 9 and Year 10 for girls, with a greater focus on fitness, teamwork and motivation and less of a focus on competitive sport. More extracurricular clubs have been added at break times and after school for Year 10 girls. Badminton lunchtime provision was increased. Other projects of note include Badminton Leaders, Sports Leaders and Netball Leaders |
| 17 | No participation in other research projects or local initiatives. PE provision between T0 and T1 remained the same. Three extracurricular options removed (two for staff-related reasons), but two others added | 20 | No involvement in other research projects or community initiatives. No change to PE provision between T0 and T1. Extracurricular activity data not provided |
Appendix 14 Psychosocial variable intercorrelations
| Autonomous motivation physical activity composite | Controlled motivation physical activity composite | Autonomy need satisfaction in physical activity | Competence need satisfaction in physical activity | Relatedness need satisfaction in physical activity | Physical activity self-efficacy | Peer support for physical activity | Peer norms: prevalence of physical activity | Peer norms: importance of physical activity | Peer norms: acceptance of physical activity | |
|---|---|---|---|---|---|---|---|---|---|---|
| T0 intercorrelations | ||||||||||
| Autonomous motivation physical activity composite | 1 | |||||||||
| Controlled motivation physical activity composite | 0.336 | 1 | ||||||||
| Autonomy need satisfaction in physical activity | 0.648 | 0.099 | 1 | |||||||
| Competence need satisfaction in physical activity | 0.652 | 0.043 | 0.63 | 1 | ||||||
| Relatedness need satisfaction in physical activity | 0.439 | –0.024 | 0.556 | 0.455 | 1 | |||||
| Physical activity self-efficacy | 0.546 | 0.010 | 0.543 | 0.583 | 0.511 | 1 | ||||
| Peer support for physical activity | 0.427 | 0.086 | 0.374 | 0.411 | 0.436 | 0.496 | 1 | |||
| Peer norms: prevalence of physical activity | 0.345 | 0.027 | 0.309 | 0.344 | 0.370 | 0.420 | 0.459 | 1 | ||
| Peer norms: importance of physical activity | 0.333 | 0.116 | 0.242 | 0.290 | 0.275 | 0.306 | 0.332 | 0.318 | 1 | |
| Peer norms: acceptance of physical activity | 0.2274 | 0.138 | 0.182 | 0.186 | 0.246 | 0.279 | 0.502 | 0.336 | 0.333 | 1 |
| T1 intercorrelations | ||||||||||
| Autonomous motivation physical activity composite | 1 | |||||||||
| Controlled motivation physical activity composite | 0.423 | 1 | ||||||||
| Autonomy need satisfaction in physical activity | 0.683 | 0.216 | 1 | |||||||
| Competence need satisfaction in physical activity | 0.622 | 0.126 | 0.577 | 1 | ||||||
| Relatedness need satisfaction in physical activity | 0.457 | 0.048 | 0.524 | 0.452 | 1 | |||||
| Physical activity self-efficacy | 0.621 | 0.186 | 0.575 | 0.559 | 0.484 | 1 | ||||
| Peer support for physical activity | 0.441 | 0.190 | 0.420 | 0.420 | 0.405 | 0.552 | 1 | |||
| Peer norms: prevalence of physical activity | 0.423 | 0.165 | 0.354 | 0.311 | 0.330 | 0.462 | 0.468 | 1 | ||
| Peer norms: importance of physical activity | 0.348 | 0.184 | 0.291 | 0.250 | 0.276 | 0.324 | 0.325 | 0.334 | 1 | |
| Peer norms: acceptance of physical activity | 0.288 | 0.229 | 0.219 | 0.229 | 0.230 | 0.337 | 0.530 | 0.336 | 0.327 | 1 |
| Psychosocial variable | Correlation: T0 with T1 |
|---|---|
| Autonomous motivation physical activity composite | 0.622 |
| Controlled motivation physical activity composite | 0.472 |
| Autonomy need satisfaction in physical activity | 0.471 |
| Competence need satisfaction in physical activity | 0.676 |
| Relatedness need satisfaction in physical activity | 0.500 |
| Physical activity self-efficacy | 0.551 |
| Peer support for physical activity | 0.466 |
| Peer norms: prevalence of physical activity | 0.416 |
| Peer norms: importance of physical activity | 0.331 |
| Peer norms: acceptance of physical activity | 0.296 |
Appendix 15 Regression models of associations between psychological variables and weekday moderate to vigorous physical activity
| Model | Coefficient | 95% CI | p-value |
|---|---|---|---|
| Model 1: primary analysisa model, additionally adjusted for autonomous motivation, controlled motivation and amotivation | |||
| Autonomous motivation | 0.86 | –0.57 to 2.29 | 0.239 |
| Controlled motivation | –0.29 | –1.45 to 0.86 | 0.618 |
| Amotivation | 0.02 | –1.14 to 1.19 | 0.967 |
| Model 2: primary analysisa model, additionally adjusted for autonomy need satisfaction, competence need satisfaction and relatedness need satisfaction | |||
| Autonomy need satisfaction | –0.34 | –1.22 to 0.09 | 0.456 |
| Competence need satisfaction | 0.01 | –0.74 to 0.76 | 0.977 |
| Relatedness need satisfaction | 0.12 | –0.50 to 0.74 | 0.700 |
| Model 3: primary analysisa model, additionally adjusted for intrinsic motivation, identified motivation, introjected motivation, external motivation and amotivation | |||
| Intrinsic motivation | 1.35 | 0.03 to 2.67 | 0.045 |
| Identified motivation | –1.44 | –3.08 to 0.21 | 0.086 |
| Introjected motivation | –0.42 | –1.45 to 0.61 | 0.421 |
| External motivation | 0.61 | –0.65 to 1.78 | 0.309 |
| Amotivation | 0.70 | –0.75 to 2.15 | 0.344 |
| Model 4: primary analysisa model, additionally adjusted for physical activity self-efficacy, physical activity social support, prevalence norms, importance norms and acceptance norms | |||
| Physical activity self-efficacy | 0.61 | –1.81 to 3.02 | 0.622 |
| Peer support for physical activity | 0.66 | –1.15 to 2.47 | 0.475 |
| Peer norms: prevalence of physical activity | –0.50 | –2.14 to 1.14 | 0.553 |
| Peer norms: importance of physical activity | 0.10 | –1.04 to 1.24 | 0.863 |
| Peer norms: acceptance of physical activity | –1.24 | –2.68 to 0.20 | 0.091 |
List of abbreviations
- ACME
- average causal mediated effect
- ASSIST
- A Stop Smoking In Schools Trial
- BRTC
- Bristol Randomised Trials Collaboration
- CEAC
- cost-effectiveness acceptability curve
- CEP
- cost-effectiveness plane
- CHU-9D
- Child Health Utility Instrument, nine dimensions
- CI
- confidence interval
- CMO
- Chief Medical Officer
- CONSORT
- Consolidated Standards of Reporting Trials
- COREQ
- Consolidated Criteria for Reporting Qualitative Research
- CPM
- counts per minute
- DOI
- diffusion of innovations
- EMA
- ecological momentary assessment
- EQ-5D
- EuroQol 5-Dimensions
- EQ-5D-Y
- EuroQol 5-Dimensions, Youth version
- ES
- external stakeholder
- GDPR
- General Data Protection Regulation
- HIIT
- high-intensity interval training
- HRQoL
- health-related quality of life
- ICER
- incremental cost-effectiveness ratio
- ID
- identification number
- IMD
- Index of Multiple Deprivation
- IQR
- interquartile range
- ITT
- intention to treat
- LAG
- Local Advisory Group
- MICE
- multiple imputation by chained equations
- MVPA
- moderate to vigorous physical activity
- NIHR
- National Institute for Health Research
- NPS
- non-peer supporter
- Ofsted
- Office for Standards in Education, Children’s Services and Skills
- PE
- physical education
- PLAN-A
- Peer-led physical Activity iNtervention for Adolescent girls
- PS
- peer supporter
- PSHE
- Personal, Social, Health and Economic Education
- QALY
- quality-adjusted life-year
- REDCap
- Research Electronic Data Capture
- SC
- school contact
- SD
- standard deviation
- SDT
- self-determination theory
- SEP
- socioeconomic position
- SLT
- senior leadership team
- SNA
- social network analysis
- T0
- time 0
- T1
- time 1
- TIDieR
- Template for Intervention Description and Replication
- TMG
- Trial Management Group
- TSC
- Trial Steering Committee
- UKCRC
- United Kingdom Clinical Research Collaboration
- VAS
- visual analogue scale
Notes
Supplementary material can be found on the NIHR Journals Library report page (https://doi.org/10.3310/ZJQW2587).
Supplementary material has been provided by the authors to support the report and any files provided at submission will have been seen by peer reviewers, but not extensively reviewed. Any supplementary material provided at a later stage in the process may not have been peer reviewed.